
Update on Calcium and Phosphorus Requirements of Preterm Infants and Recommendations for Enteral Mineral Intake



Abstract
:1. Introduction
1.1. Definition of Bone Mineral Deficiency of Prematurity
1.2. Clinical Signs of BMDP in Preterm Infants
1.3. BMD in the First Years of Life
1.4. BMD at Child Age and in Adults
2. Materials and Methods
3. Results
3.1. Current Recommendations for Enteral Ca and P Intake in Preterm Infants
3.2. Physiology of Ca and P Requirements
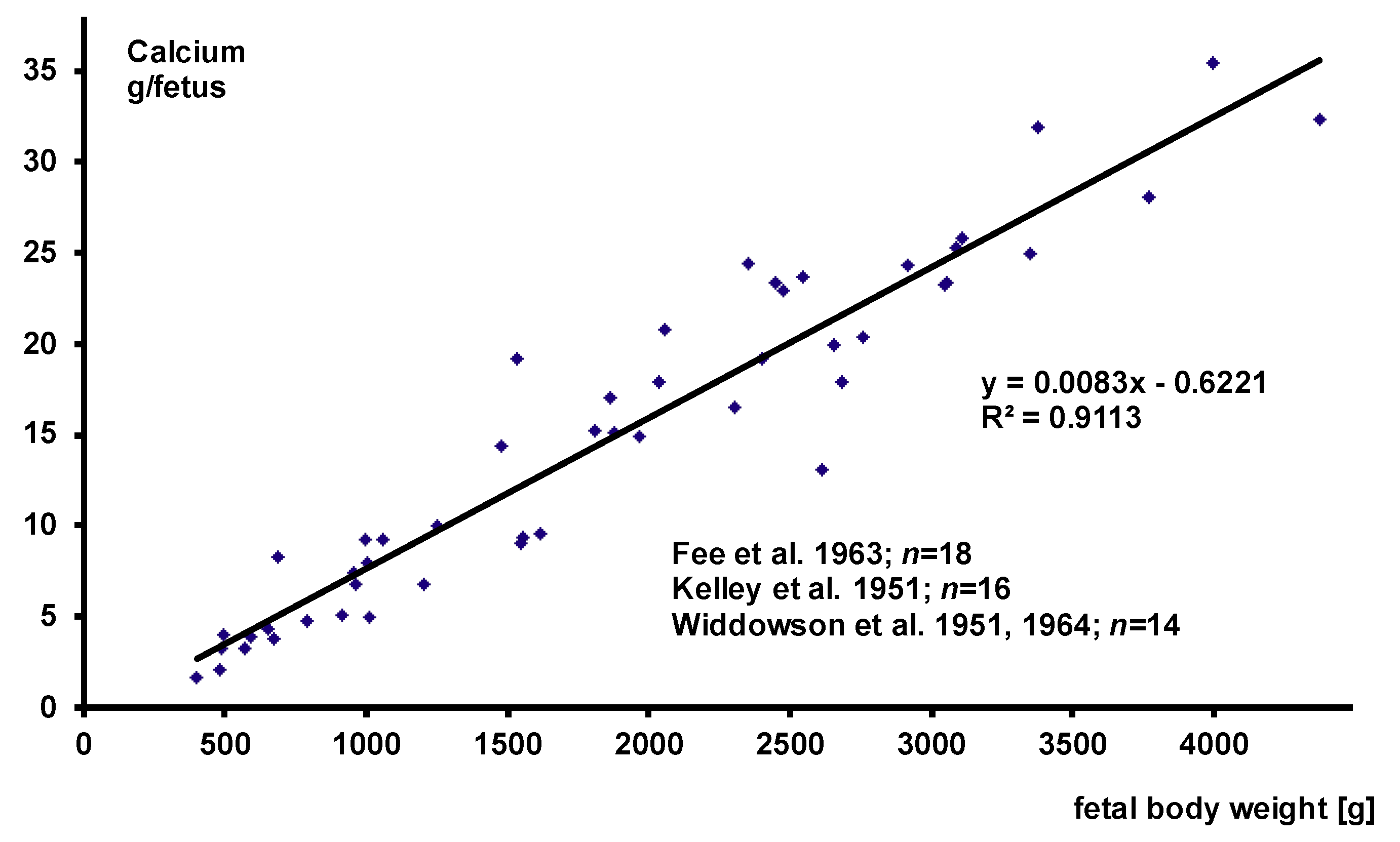
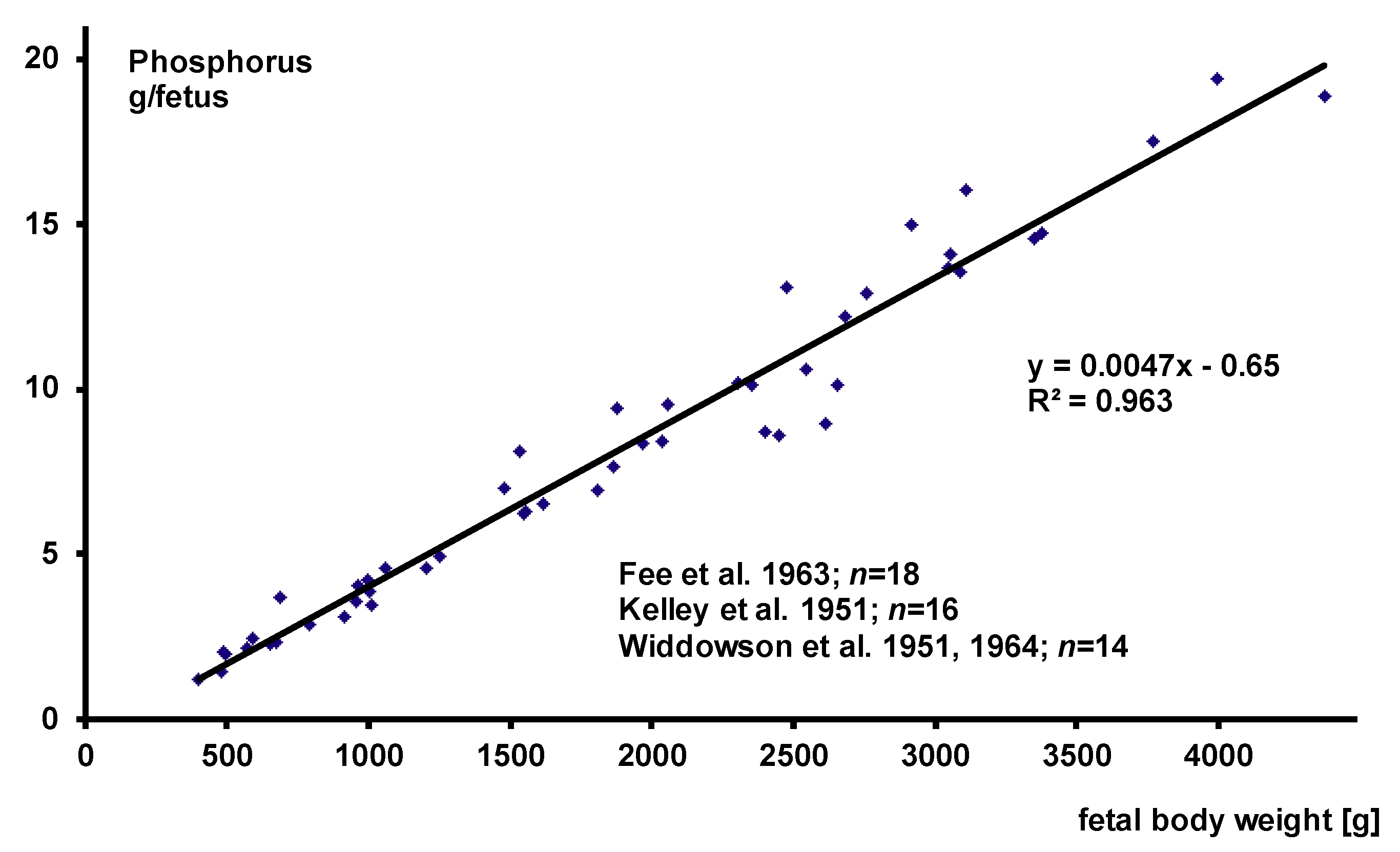
3.2.1. Fetal Body Composition
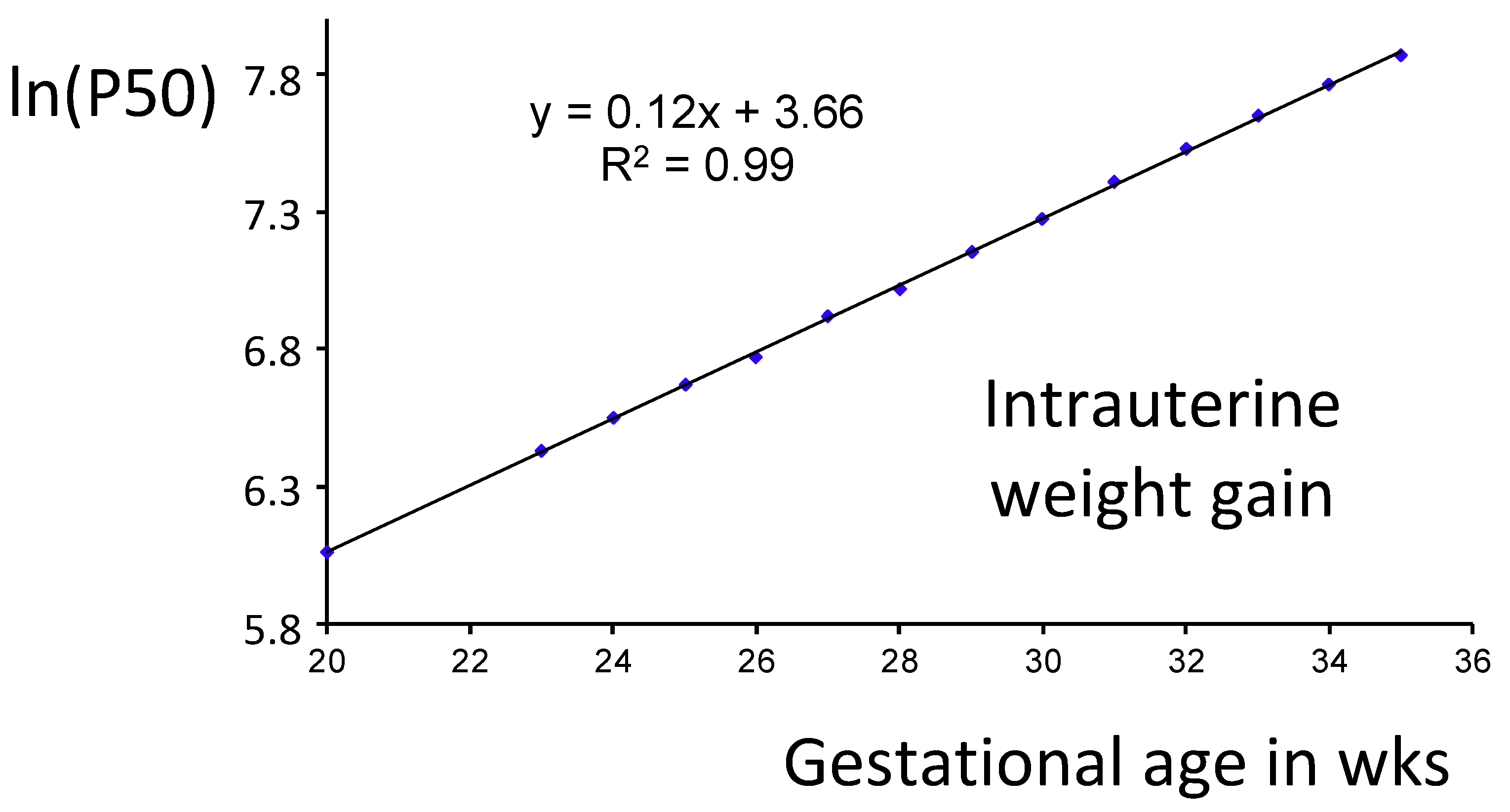
3.2.2. Fetal Weight Gain
3.2.3. Ca and P Absorption
3.2.4. Individualized Ca and P Supplementation
3.2.5. Caveats in Individualized Ca and P Supplementation
3.2.6. Risks of High Enteral Mineral Supplementation
4. Conclusions and Recommendations
4.1. Conclusions
- Ca and P requirements depend on weight gain.
- Current recommendations for enteral Ca and P intake fail to meet the requirements of preterm infants for two reasons:
- Given a target neonatal weight gain above 17 g/kg/day, the average intrauterine Ca and P accretion is systematically underestimated.
- The average enteral Ca bioavailability is systematically overestimated.
- Promotion of adequate nutrition with sufficient minerals (and vitamin D) may promote long-term bone health.
- Increasing the enteral intake recommendations for all infants (especially Ca intake) may improve average bone mineralization at the risk of a higher incidence of nephrocalcinosis.
4.2. Recommendations
- Individually adjusted additional enteral mineral supplementation to improve current mineral intake by formula/fortifier should be performed to prevent inadequately low infant BMC and to reduce the risk of nephrocalcinosis.
- Organic phosphate salts such as glycerophosphate or glucose phosphate should be preferred, because inorganic phosphate salts precipitate much more easily, especially when combined with calcium supplements, thus reducing the bioavailability of both Ca and P.
- Local individualized Ca and P supplementation strategies should be validated. This includes the idea of separating Ca and P supplement administrations to different times of the day.
- Future enteral Ca and P recommendation should be based on long-term bone health as well.
4.3. Research Direction for Future Studies
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Atkinson, A.J., Jr.; Tsang, R. Calcium, magnesium, phosphorus and vitamin D. In Nutrition of the Preterm Infant, 2nd ed.; Tsang, R., Uauy, R., Koletzko, B., Zlotkin, S., Eds.; Digital Educational Publishing, Inc.: Cincinnati, OH, USA, 2005; Volume 1, pp. 245–275. [Google Scholar]
- Agostoni, C.; Buonocore, G.; Carnielli, V.P.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellof, M.; Embleton, N.D.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral nutrient supply for preterm infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef]
- Abrams, S.A.; Committee on Nutrition. Calcium and vitamin d requirements of enterally fed preterm infants. Pediatrics 2013, 131, e1676–e1683. [Google Scholar] [CrossRef] [Green Version]
- Mimouni, F.B.; Mandel, D.; Lubetzky, R.; Senterre, T. Calcium, phosphorus, magnesium and vitamin D requirements of the preterm infant. World Rev. Nutr. Diet. 2014, 110, 140–151. [Google Scholar] [CrossRef]
- Klein, C.J. Nutrient requirements for preterm infant formulas. J. Nutr. 2002, 132, 1395S–1577S. [Google Scholar] [CrossRef]
- Hamilton, B. The calcium and phospuorus metabolism of prematurely born infants. Acta Paediatr. Scand. 1922, 2, 1–84. [Google Scholar] [CrossRef]
- Oppenheimer, S.J.; Snodgrass, G.J. Neonatal rickets. Histopathology and quantitative bone changes. Arch. Dis. Child. 1980, 55, 945–949. [Google Scholar] [CrossRef]
- Posner, A.S. Crystal chemistry of bone mineral. Physiol. Rev. 1969, 49, 760–792. [Google Scholar] [CrossRef]
- Chinoy, A.; Mughal, M.Z.; Padidela, R. Metabolic bone disease of prematurity: Causes, recognition, prevention, treatment and long-term consequences. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F560–F566. [Google Scholar] [CrossRef] [PubMed]
- Rustico, S.E.; Calabria, A.C.; Garber, S.J. Metabolic bone disease of prematurity. J. Clin. Transl. Endocrinol. 2014, 1, 85–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faienza, M.F.; D’Amato, E.; Natale, M.P.; Grano, M.; Chiarito, M.; Brunetti, G.; D’Amato, G. Metabolic bone disease of prematurity: Diagnosis and management. Front. Pediatr. 2019, 7, 143. [Google Scholar] [CrossRef]
- Bozzetti, V.; Tagliabue, P. Metabolic bone disease in preterm newborn: An update on nutritional issues. Ital. J. Pediatr. 2009, 35, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas, C.; Pohlandt, F.; Mihatsch, W.A.; Franz, A. Prävention von Knochenmineralmangel bei Frühgeborenen. Klin. Padiatr. 2012, 224, 80–87. [Google Scholar] [PubMed]
- Grahnen, H.; Sjolin, S.; Stenstrom, A. Mineralization defects of primary teeth in children born pre-term. Scand. J. Dent. Res. 1974, 82, 396–400. [Google Scholar] [CrossRef]
- Pimlott, J.F.; Howley, T.P.; Nikiforuk, G.; Fitzhardinge, P.M. Enamel defects in prematurely born, low birth-weight infants. Pediatr. Dent. 1985, 7, 218–223. [Google Scholar] [PubMed]
- Carroll, D.M.; Doria, A.S.; Paul, B.S. Clinical-radiological features of fractures in premature infants—A review. J. Perinat. Med. 2007, 35, 366–375. [Google Scholar] [CrossRef]
- Dabezies, E.J.; Warren, P.D. Fractures in very low birth weight infants with rickets. Clin. Orthop. Relat. Res. 1997, 335, 233–239. [Google Scholar] [CrossRef]
- Geggel, R.L.; Pereira, G.R.; Spackman, T.J. Fractured ribs: Unusual presentation of rickets in premature infants. J. Pediatr. 1978, 93, 680–682. [Google Scholar] [CrossRef]
- Pohlandt, F. Hypothesis: Myopia of prematurity is caused by postnatal bone mineral deficiency. Eur. J. Pediatr. 1994, 153, 234–236. [Google Scholar] [CrossRef]
- Pohlandt, F. Bone mineral deficiency as the main factor of dolichocephalic head flattening in very-low-birth-weight infants. Pediatr. Res. 1994, 35, 701–703. [Google Scholar] [CrossRef] [Green Version]
- Lyon, A.J.; McIntosh, N.; Wheeler, K.; Williams, J.E. Radiological rickets in extremely low birthweight infants. Pediatr. Radiol. 1987, 17, 56–58. [Google Scholar] [CrossRef]
- Koo, W.W.; Sherman, R.; Succop, P.; Krug-Wispe, S.; Tsang, R.C.; Steichen, J.J.; Crawford, A.H.; Oestreich, A.E. Fractures and rickets in very low birth weight infants: Conservative management and outcome. J. Pediatr. Orthop. 1989, 9, 326–330. [Google Scholar] [CrossRef]
- Fewtrell, M.S. Does early nutrition program later bone health in preterm infants? Am. J. Clin. Nutr. 2011, 94, 1870S–1873S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viswanathan, S.; Khasawneh, W.; McNelis, K.; Dykstra, C.; Amstadt, R.; Super, D.M.; Groh-Wargo, S.; Kumar, D. Metabolic bone disease: A continued challenge in extremely low birth weight infants. J. Parenter. Enteral. Nutr. 2014, 38, 982–990. [Google Scholar] [CrossRef]
- Smurthwaite, D.; Mughal, M.Z.; Wright, N.B.; Russell, S.; Emmerson, A.J. How common are radiologically apparent rib fractures in extremely low birth weight preterm infants? Arch. Dis. Child. 2009, 92, A45. [Google Scholar] [CrossRef]
- Mitchell, S.M.; Rogers, S.P.; Hicks, P.D.; Hawthorne, K.M.; Parker, B.R.; Abrams, S.A. High frequencies of elevated alkaline phosphatase activity and rickets exist in extremely low birth weight infants despite current nutritional support. BMC Pediatr. 2009, 9, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdallah, E.A.; Said, R.N.; Mosallam, D.S.; Moawad, E.M.; Kamal, N.M.; Fathallah, M.G. Serial serum alkaline phosphatase as an early biomarker for osteopenia of prematurity. Medicine 2016, 95, e4837. [Google Scholar] [CrossRef]
- Lapillonne, A.A.; Glorieux, F.H.; Salle, B.L.; Braillon, P.M.; Chambon, M.; Rigo, J.; Putet, G.; Senterre, J. Mineral balance and whole body bone mineral content in very low-birth-weight infants. Acta Paediatr. 1994, 405, 117–122. [Google Scholar] [CrossRef]
- Wauben, I.P.; Atkinson, S.A.; Grad, T.L.; Shah, J.K.; Paes, B. Moderate nutrient supplementation of mother’s milk for preterm infants supports adequate bone mass and short-term growth: A randomized, controlled trial. Am. J. Clin. Nutr. 1998, 67, 465–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieltain, C.; de Halleux, V.; Senterre, T.; Rigo, J. Prematurity and bone health. World Rev. Nutr. Diet. 2013, 106, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Bergner, E.M.; Shypailo, R.; Visuthranukul, C.; Hagan, J.; O’Donnell, A.R.; Hawthorne, K.M.; Abrams, S.A.; Hair, A.B. Growth, body composition, and neurodevelopmental outcomes at 2 years among preterm infants fed an exclusive human milk diet in the neonatal intensive care unit: A pilot study. Breastfeed. Med. 2020, 15, 304–311. [Google Scholar] [CrossRef]
- Mihatsch, W.; Dorronsoro Martín, I.; Barrios-Sabador, V.; Couce, M.L.; Martos-Moreno, G.Á.; Argente, J.; Quero, J.; Saenz de Pipaon, M. Bone mineral density, body composition, and metabolic health of very low birth weight infants fed in hospital following current macronutrient recommendations during the first 3 years of life. Nutrients 2021, 13, 1005. [Google Scholar] [CrossRef] [PubMed]
- Fewtrell, M.S.; Prentice, A.; Jones, S.C.; Bishop, N.J.; Stirling, D.; Buffenstein, R.; Lunt, M.; Cole, T.J.; Lucas, A. Bone mineralization and turnover in preterm infants at 8–12 years of age: The effect of early diet. J. Bone Miner. Res. 1999, 14, 810–820. [Google Scholar] [CrossRef] [PubMed]
- Abou Samra, H.; Stevens, D.; Binkley, T.; Specker, B. Determinants of bone mass and size in 7-year-old former term, late-preterm, and preterm boys. Osteoporos. Int. 2009, 20, 1903–1910. [Google Scholar] [CrossRef] [PubMed]
- Zamora, S.A.; Belli, D.C.; Rizzoli, R.; Slosman, D.O.; Bonjour, J.P. Lower femoral neck bone mineral density in prepubertal former preterm girls. Bone 2001, 29, 424–427. [Google Scholar] [CrossRef]
- Martinez-Mesa, J.; Restrepo-Mendez, M.C.; Gonzalez, D.A.; Wehrmeister, F.C.; Horta, B.L.; Domingues, M.R.; Menezes, A.M. Life-course evidence of birth weight effects on bone mass: Systematic review and meta-analysis. Osteoporos. Int. 2013, 24, 7–18. [Google Scholar] [CrossRef]
- Balasuriya, C.N.D.; Evensen, K.A.I.; Mosti, M.P.; Brubakk, A.M.; Jacobsen, G.W.; Indredavik, M.S.; Schei, B.; Stunes, A.K.; Syversen, U. Peak bone mass and bone microarchitecture in adults born with low birth weight preterm or at term: A cohort study. J. Clin. Endocrinol. Metab. 2017, 102, 2491–2500. [Google Scholar] [CrossRef] [Green Version]
- Buttazzoni, C.; Rosengren, B.; Tveit, M.; Landin, L.; Nilsson, J.A.; Karlsson, M. Preterm children born small for gestational age are at risk for low adult bone mass. Calcif. Tissue Int. 2016, 98, 105–113. [Google Scholar] [CrossRef]
- Hovi, P.; Andersson, S.; Jarvenpaa, A.L.; Eriksson, J.G.; Strang-Karlsson, S.; Kajantie, E.; Makitie, O. Decreased bone mineral density in adults born with very low birth weight: A cohort study. PLoS Med. 2009, 6, e1000135. [Google Scholar] [CrossRef] [Green Version]
- Xie, L.F.; Alos, N.; Cloutier, A.; Beland, C.; Dubois, J.; Nuyt, A.M.; Luu, T.M. The long-term impact of very preterm birth on adult bone mineral density. Bone Rep. 2019, 10, 100189. [Google Scholar] [CrossRef]
- Haikerwal, A.; Doyle, L.W.; Patton, G.; Garland, S.M.; Cheung, M.M.; Wark, J.D.; Cheong, J.L.Y. Bone health in young adult survivors born extremely preterm or extremely low birthweight in the post surfactant era. Bone 2021, 143, 115648. [Google Scholar] [CrossRef]
- Engan, M.; Vollsaeter, M.; Oymar, K.; Markestad, T.; Eide, G.E.; Halvorsen, T.; Juliusson, P.; Clemm, H. Comparison of physical activity and body composition in a cohort of children born extremely preterm or with extremely low birth weight to matched term-born controls: A follow-up study. BMJ Paediatr. Open 2019, 3, e000481. [Google Scholar] [CrossRef]
- Fee, B.A.; Weil, W.B., Jr. Body composition of infants of diabetic mothers by direct analysis. Ann. N. Y. Acad. Sci. 1963, 110, 869–897. [Google Scholar] [CrossRef]
- Kelly, H.J.; Soloan, R.E.; Hoffman, W.; Saunders, C. Accumulation of nitrogen and six minerals in the human fetus during gestation. Hum. Biol. 1951, 23, 61–74. [Google Scholar] [CrossRef]
- Widdowson, E.M.; Dickerson, J.W.T. Chemical compostion of the body. In Mineral Metabolism; Comar, C.L., Bronner, F., Eds.; Academic Press: New York, NY, USA, 1964; Volume 2, pp. 1–247. [Google Scholar]
- Ellis, K.J.; Shypailo, R.J.; Schanler, R.J. Body composition of the preterm infant. Ann. Hum. Biol. 1994, 21, 533–545. [Google Scholar] [CrossRef]
- Rigo, J.; De Curtis, M.; Picaud, J.C.; Nyamugabo, K.; Senterre, J. Whole body calcium content in term and preterm neonates. Eur. J. Pediatr. 1998, 157, 259–260. [Google Scholar]
- Voigt, M.; Schneider, K.T.; Jährig, K. Analysis of a 1992 birth sample in Germany. 1: New percentile values of the body weight of newborn infants. Geburtsh. Frauenheilkd. 1996, 56, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.R.; Himes, J.H.; Kaufman, R.B.; Mor, J.; Kogan, M. A United States National reference for fetal growth. Obstet. Gynecol. 1996, 87, 163–168. [Google Scholar] [CrossRef]
- Hay, W.W. Growth and development: Physiological aspects. In Encyclopedia of Human Nutrition, 4th ed.; Caballero, B., Ed.; Academic Press: Waltham, MA, USA, 2021; Volume 2, In press. [Google Scholar]
- Bronner, F.; Salle, B.L.; Putet, G.; Rigo, J.; Senterre, J. Net calcium absorption in premature infants: Results of 103 metabolic balance studies. Am. J. Clin. Nutr. 1992, 56, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Mize, C.E.; Uauy, R.; Waidelich, D.; Neylan, M.J.; Jacobs, J. Effect of phosphorus supply on mineral balance at high calcium intakes in very low birth weight infants. Am. J. Clin. Nutr. 1995, 62, 385–391. [Google Scholar] [CrossRef]
- Maas, C.; Pohlandt, F.; Mihatsch, W.A.; Franz, A.R. Prevention of bone mineral deficiency in premature infants: Review of the literature with focus on monitoring of urinary calcium and phosphate. Klin. Padiatr. 2012, 224, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Trotter, A.; Pohlandt, F. Calcium and phosphorus retention in extremely preterm infants supplemented individually. Acta Paediatr. 2002, 91, 680–683. [Google Scholar] [CrossRef] [PubMed]
- Carroll, W.F.; Fabres, J.; Nagy, T.R.; Frazier, M.; Roane, C.; Pohlandt, F.; Carlo, W.A.; Thome, U.H. Results of extremely-low-birth-weight infants randomized to receive extra enteral calcium supply. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 339–345. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, S.A.; Alston-Mills, B.; Lonnerdal, B.; Neville, M.C. Major minerals and ionic constituents of human and bovine milks. In Handbook of Milk Composition; Jensen, R.G., Ed.; Academic Press: San Diego, CA, USA, 1995; pp. 593–619. [Google Scholar]
- Narendra, A.; White, M.P.; Rolton, H.A.; Alloub, Z.I.; Wilkinson, G.; McColl, J.H.; Beattie, J. Nephrocalcinosis in preterm babies. Arch. Dis. Child. Fetal Neonatal Ed. 2001, 85, F207–F213. [Google Scholar] [CrossRef] [PubMed]
- Hein, G.; Richter, D.; Manz, F.; Weitzel, D.; Kalhoff, H. Development of nephrocalcinosis in very low birth weight infants. Pediatr. Nephrol. 2004, 19, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Schell-Feith, E.A.; Kist-van Holthe, J.E.; van der Heijden, A.J. Nephrocalcinosis in preterm neonates. Pediatr. Nephrol. 2010, 25, 221–230. [Google Scholar] [CrossRef] [Green Version]
- Hoppe, B.; Duran, I.; Martin, A.; Kribs, A.; Benz-Bohm, G.; Michalk, D.V.; Roth, B. Nephrocalcinosis in preterm infants: A single center experience. Pediatr. Nephrol. 2002, 17, 264–268. [Google Scholar] [CrossRef]
- Mihatsch, W.A.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; Desci, T.; Domellof, M.; Embleton, N.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition. Clin. Nutr. 2018, 37, 2303–2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pohlandt, F. Prevention of postnatal bone demineralization in very low-birth-weight infants by individually monitored supplementation with calcium and phosphorus. Pediatr. Res. 1994, 35, 125–129. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihatsch, W.; Thome, U.; Saenz de Pipaon, M. Update on Calcium and Phosphorus Requirements of Preterm Infants and Recommendations for Enteral Mineral Intake. Nutrients 2021, 13, 1470. https://doi.org/10.3390/nu13051470
Mihatsch W, Thome U, Saenz de Pipaon M. Update on Calcium and Phosphorus Requirements of Preterm Infants and Recommendations for Enteral Mineral Intake. Nutrients. 2021; 13(5):1470. https://doi.org/10.3390/nu13051470
Chicago/Turabian StyleMihatsch, Walter, Ulrich Thome, and Miguel Saenz de Pipaon. 2021. "Update on Calcium and Phosphorus Requirements of Preterm Infants and Recommendations for Enteral Mineral Intake" Nutrients 13, no. 5: 1470. https://doi.org/10.3390/nu13051470
APA StyleMihatsch, W., Thome, U., & Saenz de Pipaon, M. (2021). Update on Calcium and Phosphorus Requirements of Preterm Infants and Recommendations for Enteral Mineral Intake. Nutrients, 13(5), 1470. https://doi.org/10.3390/nu13051470