
NutriCatt Protocol Improves Body Composition and Clinical Outcomes in Elderly Patients Undergoing Colorectal Surgery in ERAS Program: A Retrospective Cohort Study

 ,
,  , , , , ,
, , , , , 

Abstract
:1. Introduction
- -
- to evaluate the effects of the NutriCatt protocol on the body composition of elderly (>75 years) patients undergoing colorectal surgery from the pre-admission phase, to admission and discharge.
- -
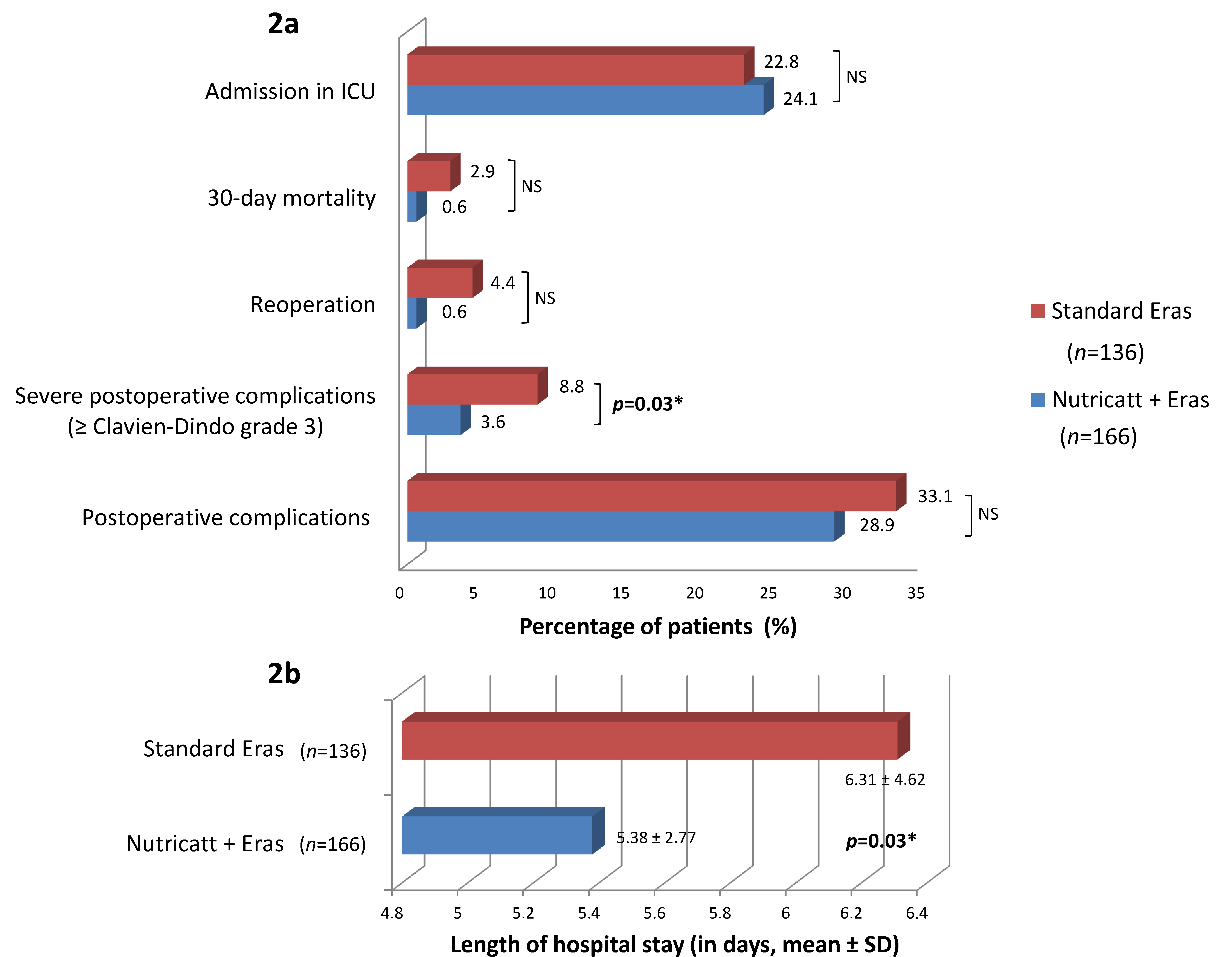
- to compare clinical outcomes such as postoperative complications, re-operation, 30-day mortality, admission to Intensive Care Unit (ICU), and LOS between elderly patients receiving or not the perioperative nutritional support (both within the ERAS program).
2. Materials and Methods
2.1. Study Design and Ethical Committee Approval
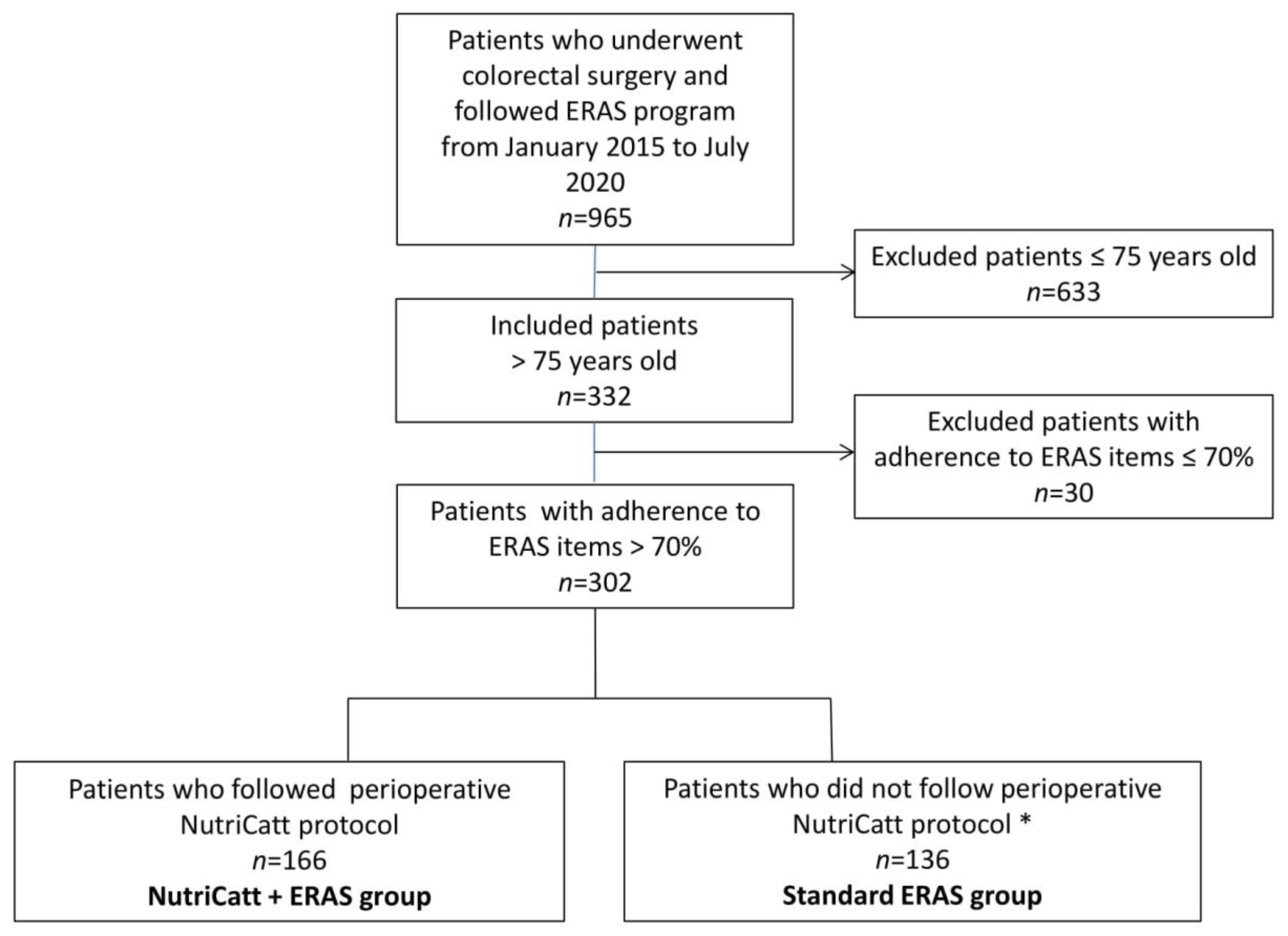
2.2. Patients
2.3. NutriCatt Nutritional Protocol
2.4. BIA Measurement Protocol
2.5. Discharge Criteria
2.6. Outcomes
- Within patients undergoing NutriCatt protocol: body composition changes between pre-admission, admission, and discharge including FFM (kg), phase angle (PhA; degree), resistance (Rz; Ohm), reactance (Xc; Ohm), BCM (kg), BCMI, and TBW (L);
- Between patients undergoing NutriCatt protocol + ERAS and those in standard ERAS:
- ○
- LOS defined as the number of days from surgery to discharge calculated from discharge letters;
- ○
- Number and type of postoperative complications according to Clavien–Dindo staging [20];
- ○
- Number of severe complications (Clavien–Dindo grade ≥ III);
- ○
- 30-day mortality defined as death occurring within 30 days of colorectal surgery;
- ○
- Number of re-operations;
- ○
- Number of admissions to Intensive Care Unit (ICU).
2.7. Data Collection and Statistical Analysis
3. Results
3.1. Patients Baseline Characteristics
3.2. Body Composition Changes between Pre-Admission, Admission, and Discharge in Patients following NutriCatt Protocol
3.3. Impact of NutriCatt Protocol on Outcomes of Hospitalization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flynn, D.E.; Mao, D.; Yerkovich, S.; Franz, R.; Iswariah, H.; Hughes, A.; Shaw, I.; Tam, D.; Chandrasegaram, M. Should We Resect Colorectal Cancer in Patients over the Age of 85? World J. Gastrointest. Oncol. 2021, 13, 185–196. [Google Scholar] [CrossRef]
- De van der Schueren, M.A.E.; de Vries, O.J.; Danner, S.A.; Kramer, M.H.; Muller, M. Prevalence and Determinants for Malnutrition in Geriatric Outpatients. Clin. Nutr. 2013, 32, 1007–1011. [Google Scholar] [CrossRef] [PubMed]
- Ennis, B.W.; Saffel-Shrier, S.; Verson, H. Diagnosing Malnutrition in the Elderly. Nurse Pract. 2001, 26, 52–65. [Google Scholar] [CrossRef] [PubMed]
- Argilés, J.M. Cancer-Associated Malnutrition. Eur. J. Oncol. Nurs. 2005, 9, S39–S50. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN Guidelines on Definitions and Terminology of Clinical Nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Mislang, A.R.; Di Donato, S.; Hubbard, J.; Krishna, L.; Mottino, G.; Bozzetti, F.; Biganzoli, L. Nutritional Management of Older Adults with Gastrointestinal Cancers: An International Society of Geriatric Oncology (SIOG) Review Paper. J. Geriatr. Oncol. 2018, 9, 382–392. [Google Scholar] [CrossRef] [Green Version]
- Barker, L.A.; Gout, B.S.; Crowe, T.C. Hospital Malnutrition: Prevalence, Identification and Impact on Patients and the Healthcare System. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef] [Green Version]
- Joseph, B.; Pandit, V.; Sadoun, M.; Zangbar, B.; Fain, M.J.; Friese, R.S.; Rhee, P. Frailty in Surgery. J. Trauma Acute Care Surg. 2014, 76, 1151–1156. [Google Scholar] [CrossRef]
- Kehlet, H. Multimodal Approach to Control Postoperative Pathophysiology and Rehabilitation. Br. J. Anaesth. 1997, 78, 606–617. [Google Scholar] [CrossRef]
- Stephen, A.E.; Berger, D.L. Shortened Length of Stay and Hospital Cost Reduction with Implementation of an Accelerated Clinical Care Pathway after Elective Colon Resection. Surgery 2003, 133, 277–282. [Google Scholar] [CrossRef]
- DiFronzo, L.A.; Yamin, N.; Patel, K.; O’Connell, T.X. Benefits of Early Feeding and Early Hospital Discharge in Elderly Patients Undergoing Open Colon Resection. J. Am. Coll. Surg. 2003, 197, 747–752. [Google Scholar] [CrossRef]
- Gustafsson, U.O.; Scott, M.J.; Schwenk, W.; Demartines, N.; Roulin, D.; Francis, N.; McNaught, C.E.; MacFie, J.; Liberman, A.S.; Soop, M.; et al. Guidelines for Perioperative Care in Elective Colonic Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations. Clin. Nutr. 2012, 31, 783–800. [Google Scholar] [CrossRef] [PubMed]
- Carli, F.; Scheede-Bergdahl, C. Prehabilitation to Enhance Perioperative Care. Anesthesiol. Clin. 2015, 33, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Rinninella, E.; Persiani, R.; D’Ugo, D.; Pennestrì, F.; Cicchetti, A.; Di Brino, E.; Cintoni, M.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. NutriCatt Protocol in the Enhanced Recovery After Surgery (ERAS) Program for Colorectal Surgery: The Nutritional Support Improves Clinical and Cost-Effectiveness Outcomes. Nutrition 2018, 50, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN Guidelines on Nutrition in Cancer Patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustafsson, U.O.; Hausel, J.; Thorell, A.; Ljungqvist, O.; Soop, M.; Nygren, J. Enhanced Recovery After Surgery Study Group Adherence to the Enhanced Recovery after Surgery Protocol and Outcomes after Colorectal Cancer Surgery. Arch. Surg. 2011, 146, 571–577. [Google Scholar] [CrossRef] [Green Version]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN Guideline: Clinical Nutrition in Surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NOAH, N. The STROBE Initiative STrengthening the Reporting of OBservational Studies in Epidemiology (STROBE). Epidemiol. Infect. 2008, 136, 865. [Google Scholar] [CrossRef] [Green Version]
- Pisarska, M.; Pędziwiatr, M.; Małczak, P.; Major, P.; Ochenduszko, S.; Zub-Pokrowiecka, A.; Kulawik, J.; Budzyński, A. Do We Really Need the Full Compliance with ERAS Protocol in Laparoscopic Colorectal Surgery? A Prospective Cohort Study. Int J. Surg. 2016, 36, 377–382. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo Classification of Surgical Complications: Five-Year Experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Guralnik, J.M.; Ferrucci, L.; Simonsick, E.M.; Salive, M.E.; Wallace, R.B. Lower-Extremity Function in Persons over the Age of 70 Years as a Predictor of Subsequent Disability. N. Engl. J. Med. 1995, 332, 556–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burd, N.A.; Gorissen, S.H.; van Loon, L.J.C. Anabolic Resistance of Muscle Protein Synthesis with Aging. Exerc. Sport Sci. Rev. 2013, 41, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Rinninella, E.; Silvestri, G.; Cintoni, M.; Perna, A.; Martorana, G.E.; De Lorenzo, A.; Rossini, P.M.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. Clinical Use of Bioelectrical Impedance Analysis in Patients Affected by Myotonic Dystrophy Type 1: A Cross-Sectional Study. Nutrition 2019, 67–68. [Google Scholar] [CrossRef]
- Ji, W.; Liu, X.; Zheng, K.; Yang, H.; Cui, J.; Li, W. Correlation of Phase Angle with Sarcopenia and Its Diagnostic Value in Elderly Men with Cancer. Nutrition 2021, 84, 111110. [Google Scholar] [CrossRef] [PubMed]
- Prognostic Effect of Weight Loss Prior to Chemotherapy in Cancer Patients. Eastern Cooperative Oncology Group—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/7424938/ (accessed on 17 March 2021).
- Baracos, V.E.; Martin, L.; Korc, M.; Guttridge, D.C.; Fearon, K.C.H. Cancer-Associated Cachexia. Nat. Rev. Dis Primers 2018, 4, 17105. [Google Scholar] [CrossRef]
- Gupta, D.; Lammersfeld, C.A.; Burrows, J.L.; Dahlk, S.L.; Vashi, P.G.; Grutsch, J.F.; Hoffman, S.; Lis, C.G. Bioelectrical Impedance Phase Angle in Clinical Practice: Implications for Prognosis in Advanced Colorectal Cancer. Am. J. Clin. Nutr. 2004, 80, 1634–1638. [Google Scholar] [CrossRef] [Green Version]
- Ardito, F.; Lai, Q.; Rinninella, E.; Mimmo, A.; Vellone, M.; Panettieri, E.; Adducci, E.; Cintoni, M.; Mele, M.C.; Gasbarrini, A.; et al. The Impact of Personalized Nutritional Support on Postoperative Outcome within the Enhanced Recovery after Surgery (ERAS) Program for Liver Resections: Results from the NutriCatt Protocol. Updates Surg. 2020, 72, 681–691. [Google Scholar] [CrossRef]
- Lirosi, M.C.; Tirelli, F.; Biondi, A.; Mele, M.C.; Larotonda, C.; Lorenzon, L.; D’Ugo, D.; Gasbarrini, A.; Persiani, R. Enhanced Recovery Program for Colorectal Surgery: A Focus on Elderly Patients Over 75 Years Old. J. Gastrointest. Surg. 2019, 23, 587–594. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a Combined Comorbidity Index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Sauvanet, A.; Mariette, C.; Thomas, P.; Lozac’H, P.; Segol, P.; Tiret, E.; Delpero, J.-R.; Collet, D.; Leborgne, J.; Pradère, B.; et al. Mortality and Morbidity after Resection for Adenocarcinoma of the Gastroesophageal Junction: Predictive Factors. J. Am. Coll. Surg. 2005, 201, 253–262. [Google Scholar] [CrossRef]
- Carey, M.S.; Victory, R.; Stitt, L.; Tsang, N. Factors That Influence Length of Stay for In-Patient Gynaecology Surgery: Is the Case Mix Group (CMG) or Type of Procedure More Important? J. Obstet. Gynaecol. Can. 2006, 28, 149–155. [Google Scholar] [CrossRef]
- Risk Factors for Surgical Site Infection after Elective Resection of the Colon and Rectum: A Single-Center Prospective Study of 2809 Consecutive Patients—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/11505063/ (accessed on 17 March 2021).
- Pawa, N.; Cathcart, P.L.; Arulampalam, T.H.A.; Tutton, M.G.; Motson, R.W. Enhanced Recovery Program Following Colorectal Resection in the Elderly Patient. World J. Surg. 2012, 36, 415–423. [Google Scholar] [CrossRef]
- Rumstadt, B.; Guenther, N.; Wendling, P.; Engemann, R.; Germer, C.T.; Schmid, M.; Kipfmueller, K.; Walz, M.K.; Schwenk, W. Multimodal Perioperative Rehabilitation for Colonic Surgery in the Elderly. World J. Surg. 2009, 33, 1757–1763. [Google Scholar] [CrossRef] [PubMed]
- Ong, E.S.; Alassas, M.; Dunn, K.B.; Rajput, A. Colorectal Cancer Surgery in the Elderly: Acceptable Morbidity? Am. J. Surg. 2008, 195, 344–348. [Google Scholar] [CrossRef]
- Devon, K.M.; Vergara-Fernandez, O.; Victor, J.C.; McLeod, R.S. Colorectal Cancer Surgery in Elderly Patients: Presentation, Treatment, and Outcomes. Dis. Colon Rectum 2009, 52, 1272–1277. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All (n = 302) | NutriCatt + ERAS (n = 166) | Standard ERAS (n = 136) | p-Value | |
|---|---|---|---|---|
| Age (years), mean ± SD | 80.47 ± 4.08 | 80.76 ± 4.05 | 80.12 ± 4.06 | 0.18 |
| Gender (n, %) | 0.28 | |||
| Male | 154 (51.0) | 80 | 74 | |
| Female | 148 (49.0) | 86 | 62 | |
| Diagnosis (n, %) | 0.12 | |||
| Adenocarcinoma | 273 (90.4) | 157 | 116 | |
| Adenoma | 10 (3.3) | 5 | 5 | |
| Diverticulitis | 3 (0.9) | 0 | 3 | |
| Other | 16 (5.3) | 4 | 12 | |
| Site of Surgery (n, %) | 0.39 | |||
| Right hemicolectomy | 119 (39.4) | 64 | 55 | |
| Left hemicolectomy | 57 (18.9) | 32 | 25 | |
| Rectal surgery | 102 (33.8) | 58 | 44 | |
| Other | 24 (7.9) | 12 | 12 | |
| TNM stage (n, %) | 0.32 | |||
| 0 | 18(5.9) | 14 | 4 | |
| I | 53(17.7) | 25 | 28 | |
| IIA | 64(21.2) | 40 | 24 | |
| IIB | 21(6.9) | 10 | 11 | |
| IIC | 2(0.6) | 2 | 0 | |
| IIIA | 5(1.7) | 3 | 2 | |
| IIIB | 58(19.2) | 31 | 27 | |
| IIIC | 10(3.3) | 6 | 4 | |
| IV | 13(4.3) | 6 | 7 | |
| NR | 58(19.2) | 29 | 29 | |
| NAD (n, %) | 0.55 | |||
| Yes | 35 (11.6) | 18 | 17 | |
| No | 267 (88.4) | 148 | 119 | |
| CCI, mean ± SD | 5.50 ± 2.46 | 5.71 ± 2.24 | 5.24 ± 2.69 | 0.10 |
| ASA Score (n, %) | 0.002 * | |||
| ≥3 | 101 (33.5) | 64 | 37 | |
| <3 | 201 (66.5) | 102 | 99 | |
| Time of surgical intervention (min), mean ± SD | 217.2 ± 76.9 | 211.28 ± 75.52 | 224.02 ± 78.45 | 0.15 |
| Type of surgery (n, %) | 0.04 * | |||
| Laparotomy | 9 (3.0) | 7 | 2 | |
| Laparoscopy | 254 (84.1) | 145 | 109 | |
| Robotic | 39 (12.9) | 14 | 25 |
| Media ± SD | n (%) | |
|---|---|---|
| Body weight (kg) | 66.8 ± 11.2 | |
| Height (cm) | 158.9 ± 9.6 | |
| BMI (kg/m2) | 26.5 ± 3.9 | |
| Wrist circumference (cm) | 17.0 ± 1.2 | |
| Arm circumference (cm) | 28.1 ± 3.2 | |
| Waist circumference (cm) | 93.5 ± 12.9 | |
| Hip circumference (cm) | 99.6 ± 8.2 | |
| NRS-2002 | ||
| 1 | 5 (3.0) | |
| 2 | 86 (52.5) | |
| 3 | 68 (41.5) | |
| 4 | 5 (3.0) | |
| Rz (Ohm) | 498.1 ± 82.8 | |
| Xc (Ohm) | 41.5 ± 8.8 | |
| Phase angle (°) | 4.7 ± 0.9 | |
| Total body water (L) | 37.1 ± 6.9 | |
| Total body water (%) | 55.9 ± 7.1 | |
| Body extracellular water (L) | 19.4 ± 3.7 | |
| Body extracellular water (%) | 52.5 ± 5.3 | |
| Fat-free mass (kg) | 49.2 ± 8.7 | |
| Fat-free mass (%) | 74.2 ± 8.9 | |
| BCM (kg) | 23.1 ± 5.7 | |
| BCMI | 9.1 ± 1.8 |
| Pre-Admission T0 | Admission T1 | Discharge T2 | p-Value (ANOVA) | T0–T1 | T1–T2 | T0–T2 | |
|---|---|---|---|---|---|---|---|
| Body weight (kg) | 66.4 ± 11.1 | 66.1 ± 10.9 | 65.7 ± 10.8 | 0.39 | |||
| BMI (kg/m2) | 26.5 ± 3.9 | 26.4 ± 4.1 | 26.2 ± 4.6 | 0.42 | |||
| Rz (Ohm) | 492.6 ± 83.1 | 495.1 ± 86.6 | 507.0 ± 90.7 | 0.56 | |||
| Xc (Ohm) | 39.4 ± 7.7 | 42.2 ± 9.7 | 54.7 ± 8.2 | 0.04 * | 0.04 * | ||
| Phase angle (°) | 4.61 ± 0.79 | 4.84 ± 0.85 | 5.85 ± 0.73 | 0.002 * | 0.001 * | 0.0002 * | |
| Total body water (L) | 36.9 ± 7.1 | 36.9 ± 6.8 | 36.5 ± 7.9 | 0.84 | |||
| Total body water (%) | 56.3 ± 7.5 | 56.6 ± 8.3 | 56.2 ± 9.0 | 0.77 | |||
| Extracellular water (L) | 19.7 ± 3.7 | 19.2 ± 3.6 | 19.6 ± 5.4 | 0.79 | |||
| Extracellular water (%) | 53.5 ± 4.9 | 52.2 ± 5.5 | 52.6 ± 7.4 | 0.91 | |||
| Fat-free mass (kg) | 48.9 ± 8.8 | 49.1 ± 8.5 | 47.8 ± 11.4 | 0.12 | |||
| Fat-free mass (%) | 74.5 ± 9.3 | 75.3 ± 9.8 | 72.5 ± 13.0 | 0.16 | |||
| BCM (kg) | 22.4 ± 5.6 | 23.2 ± 5.7 | 23.1 ± 5.8 | 0.03 * | 0.02 * | ||
| BCMI | 8.9 ± 1.8 | 9.3 ± 1.9 | 9.2 ± 1.9 | 0.04 * | 0.05 * |
| Severe Complications (n = 18) | LOS > 5 Days (n = 117) | |||
|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | |
| NutriCatt + ERAS vs. standard ERAS | 0.10 (0.01–0.56) | 0.009 * | 0.53 (0.19–1.43) | 0.21 |
| Age | 1.04 (0.88–1.22) | 0.59 | 0.97 (0.86–1.09) | 0.66 |
| Sex | 2.67 (0.65–10.89) | 0.17 | 0.97 (0.36–2.55) | 0.95 |
| CCI | 1.15 (0.86–1.54) | 0.35 | 0.96 (0.76–1.22) | 0.76 |
| ASA Score < 3 | 0.69 (0.13–3.65) | 0.64 | 0.33 (0.11–0.96) | 0.04 * |
| Type of surgery | ||||
| Laparotomy | Reference | Reference | ||
| Laparoscopy | 0.15 (0.01–2.19) | 0.16 | 0.13 (0.01–1.3) | 0.08 |
| Robotic | 0.38 (0.02–6.78) | 0.51 | 0.61 (0.05–8.18) | 0.71 |
| Tumor stage | ||||
| I | Reference | Reference | ||
| II | 0.63 (0.11–3.6) | 0.61 | 1.8 (0.53–6.10) | 0.34 |
| III | 0.72 (0.12–4.29) | 0.71 | 0.63 (0.18–2.15) | 0.46 |
| IV | 0.70 (0.06–8.37) | 0.78 | 0.69 (0.10–4.61) | 0.71 |
| Severe Complications | - | - | 3.08 (0.56–17.26) | 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rinninella, E.; Biondi, A.; Cintoni, M.; Raoul, P.; Scialanga, F.; Persichetti, E.; Pulcini, G.; Pezzuto, R.; Persiani, R.; D’Ugo, D.; et al. NutriCatt Protocol Improves Body Composition and Clinical Outcomes in Elderly Patients Undergoing Colorectal Surgery in ERAS Program: A Retrospective Cohort Study. Nutrients 2021, 13, 1781. https://doi.org/10.3390/nu13061781
Rinninella E, Biondi A, Cintoni M, Raoul P, Scialanga F, Persichetti E, Pulcini G, Pezzuto R, Persiani R, D’Ugo D, et al. NutriCatt Protocol Improves Body Composition and Clinical Outcomes in Elderly Patients Undergoing Colorectal Surgery in ERAS Program: A Retrospective Cohort Study. Nutrients. 2021; 13(6):1781. https://doi.org/10.3390/nu13061781
Chicago/Turabian StyleRinninella, Emanuele, Alberto Biondi, Marco Cintoni, Pauline Raoul, Francesca Scialanga, Eleonora Persichetti, Gabriele Pulcini, Roberto Pezzuto, Roberto Persiani, Domenico D’Ugo, and et al. 2021. "NutriCatt Protocol Improves Body Composition and Clinical Outcomes in Elderly Patients Undergoing Colorectal Surgery in ERAS Program: A Retrospective Cohort Study" Nutrients 13, no. 6: 1781. https://doi.org/10.3390/nu13061781
APA StyleRinninella, E., Biondi, A., Cintoni, M., Raoul, P., Scialanga, F., Persichetti, E., Pulcini, G., Pezzuto, R., Persiani, R., D’Ugo, D., Gasbarrini, A., & Mele, M. C. (2021). NutriCatt Protocol Improves Body Composition and Clinical Outcomes in Elderly Patients Undergoing Colorectal Surgery in ERAS Program: A Retrospective Cohort Study. Nutrients, 13(6), 1781. https://doi.org/10.3390/nu13061781