
Creatine Enhances the Effects of Cluster-Set Resistance Training on Lower-Limb Body Composition and Strength in Resistance-Trained Men: A Pilot Study

 ,
,  ,
,  ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
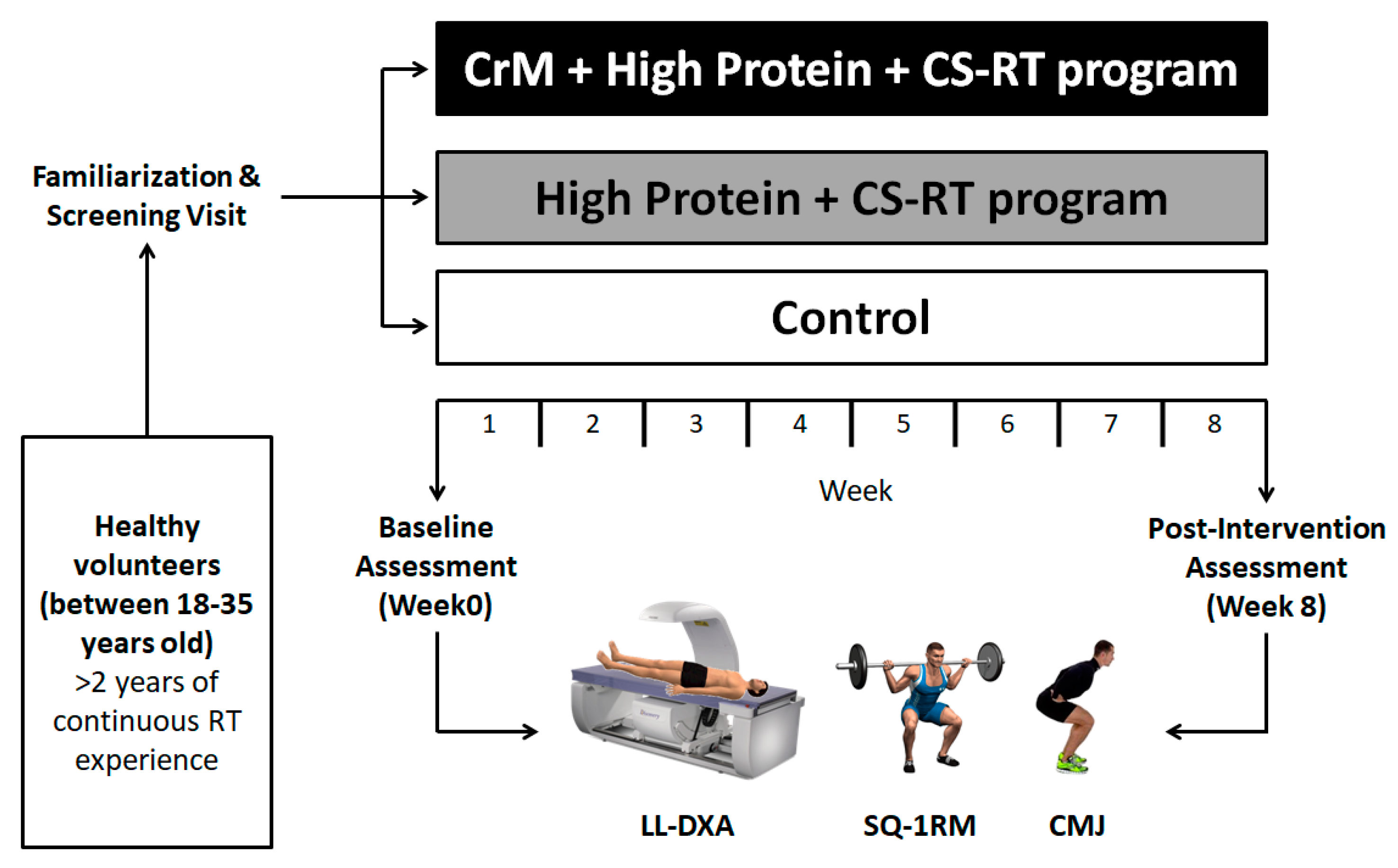
2.1. Trial Design
2.2. Participants
2.3. Intervention Procedures
2.3.1. Anthropometry
2.3.2. Exercise Protocol
2.3.3. Dietary Intervention
2.4. Outcomes
2.4.1. Primary Outcome Measures
2.4.2. Secondary Outcome Measures
Muscle Strength (Repetition Maximum Test)
Muscle Power (Countermovement Jump Test)
2.5. Sample Size
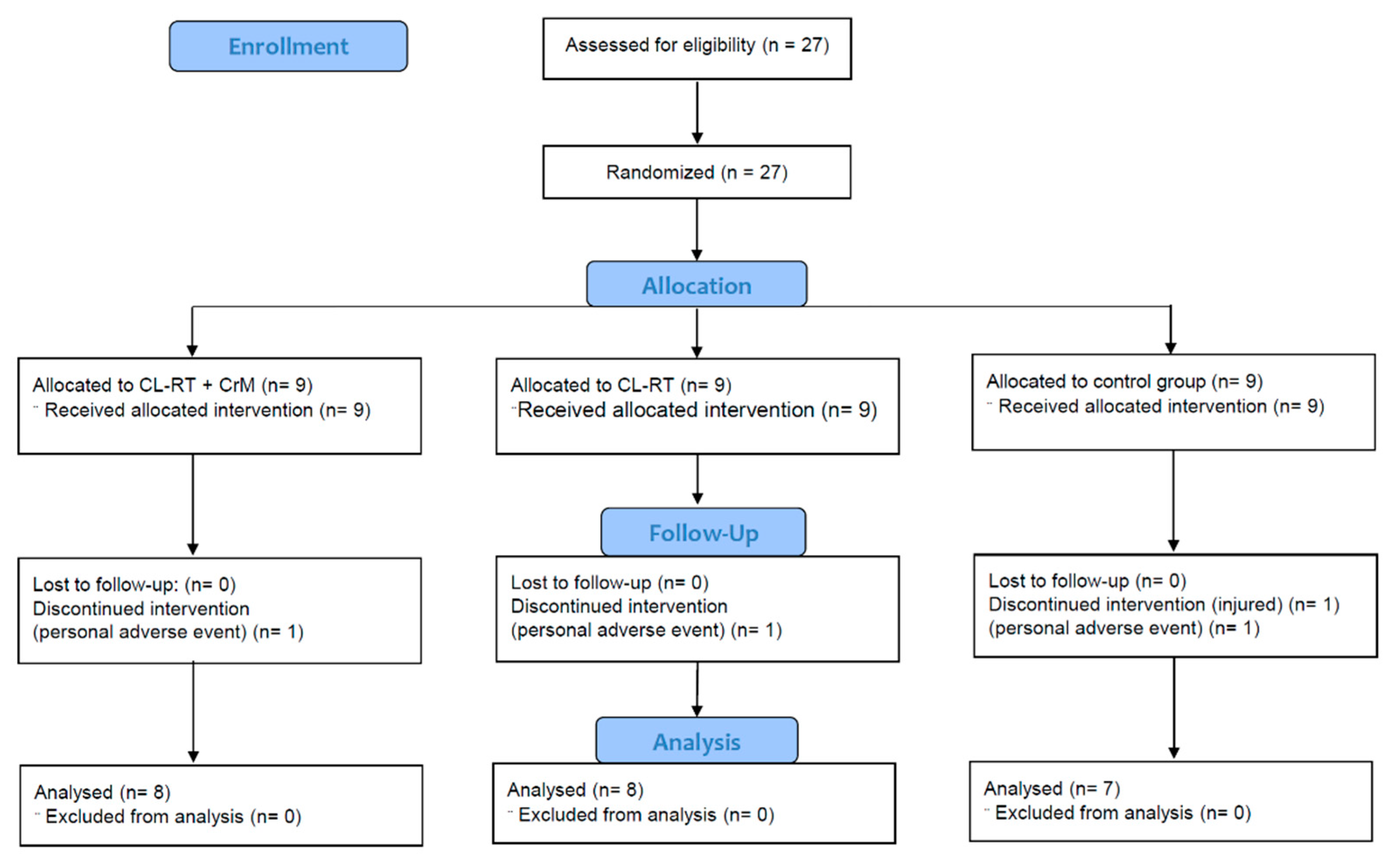
2.6. Randomization
2.7. Statistical Analysis
3. Results
3.1. Baseline Data
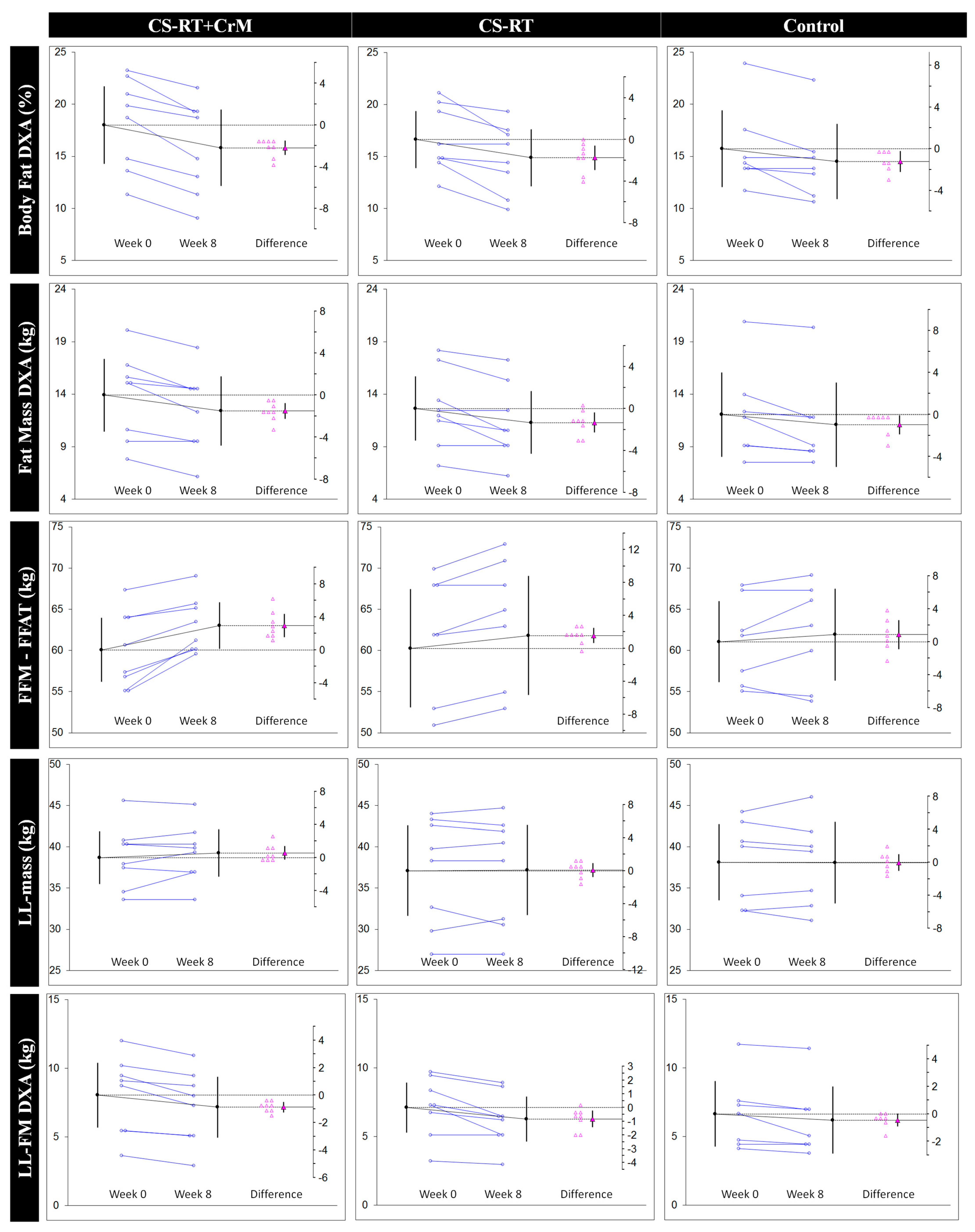
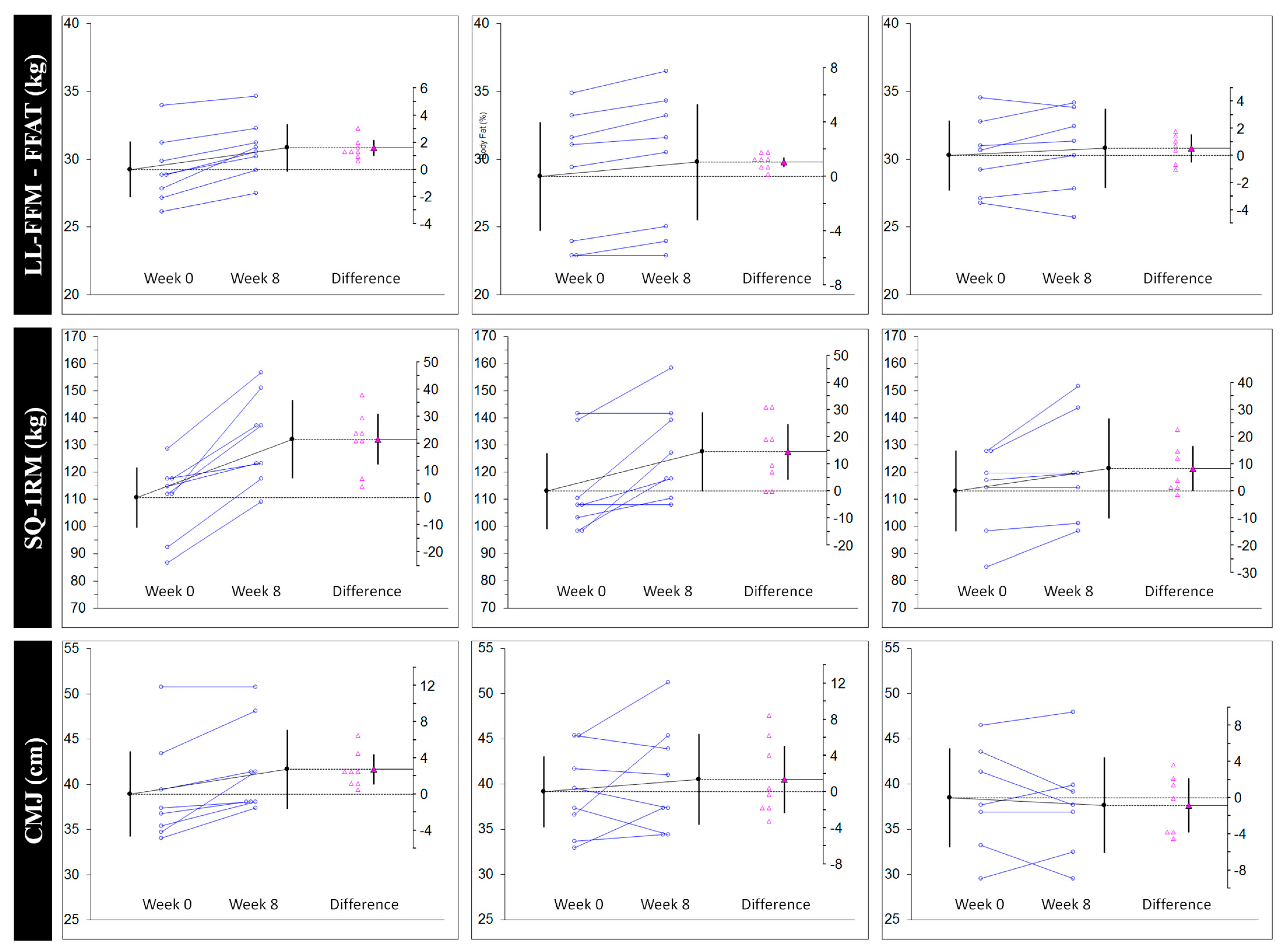
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sundberg, C.W.; Fitts, R.H. Bioenergetic basis of skeletal muscle fatigue. Curr. Opin. Physiol. 2019, 10, 118–127. [Google Scholar] [CrossRef]
- Hunter, S.K. Performance fatigability: Mechanisms and task specificity. Cold Spring Harb. Perspect. Med. 2018, 8. [Google Scholar] [CrossRef] [Green Version]
- Sundberg, C.W.; Hunter, S.K.; Trappe, S.W.; Smith, C.S.; Fitts, R.H. Effects of elevated H(+) and Pi on the contractile mechanics of skeletal muscle fibres from young and old men: Implications for muscle fatigue in humans. J. Physiol. 2018, 596, 3993–4015. [Google Scholar] [CrossRef] [Green Version]
- Davies, R.C.; Eston, R.G.; Fulford, J.; Rowlands, A.V.; Jones, A.M. Muscle damage alters the metabolic response to dynamic exercise in humans: A 31P-MRS study. J. Appl. Physiol. 2011, 111, 782–790. [Google Scholar] [CrossRef] [Green Version]
- Jarvis, K.; Woodward, M.; Debold, E.P.; Walcott, S. Acidosis affects muscle contraction by slowing the rates myosin attaches to and detaches from actin. J. Muscle Res. Cell Motil. 2018, 39, 135–147. [Google Scholar] [CrossRef]
- Allen, D.G.; Trajanovska, S. The multiple roles of phosphate in muscle fatigue. Front. Physiol. 2012, 3, 463. [Google Scholar] [CrossRef] [Green Version]
- Bonilla, D.A.; Moreno, Y. Molecular and metabolic insights of creatine supplementation on resistance training. Rev. Colomb. Química 2015, 44, 11–18. [Google Scholar] [CrossRef]
- Bonilla, D.A.; Kreider, R.B.; Stout, J.R.; Forero, D.A.; Kerksick, C.M.; Roberts, M.D.; Rawson, E.S. Metabolic basis of creatine in health and disease: A Bioinformatics-assisted review. Nutrients 2021, 13, 1238. [Google Scholar] [CrossRef] [PubMed]
- Wallimann, T. The extended, dynamic mitochondrial reticulum in skeletal muscle and the creatine kinase (CK)/phosphocreatine (PCr) shuttle are working hand in hand for optimal energy provision. J. Muscle Res. Cell Motil. 2015, 36, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Wallimann, T.; Tokarska-Schlattner, M.; Schlattner, U. The creatine kinase system and pleiotropic effects of creatine. Amino Acids 2011, 40, 1271–1296. [Google Scholar] [CrossRef] [Green Version]
- Schlattner, U.; Kay, L.; Tokarska-Schlattner, M. Mitochondrial proteolipid complexes of creatine kinase. In Membrane Protein Complexes: Structure and Function; Springer: Berlin, Germany, 2018; pp. 365–408. [Google Scholar]
- Kreider, R.B.; Kalman, D.S.; Antonio, J.; Ziegenfuss, T.N.; Wildman, R.; Collins, R.; Candow, D.G.; Kleiner, S.M.; Almada, A.L.; Lopez, H.L. International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. J. Int. Soc. Sports Nutr. 2017, 14. [Google Scholar] [CrossRef]
- Antonio, J.; Candow, D.G.; Forbes, S.C.; Gualano, B.; Jagim, A.R.; Kreider, R.B.; Rawson, E.S.; Smith-Ryan, A.E.; VanDusseldorp, T.A.; Willoughby, D.S.; et al. Common questions and misconceptions about creatine supplementation: What does the scientific evidence really show? J. Int. Soc. Sports Nutr. 2021, 18, 13. [Google Scholar] [CrossRef] [PubMed]
- Wax, B.; Kerksick, C.M.; Jagim, A.R.; Mayo, J.J.; Lyons, B.C.; Kreider, R.B. Creatine for exercise and sports performance, with recovery considerations for healthy populations. Nutrients 2021, 13, 1915. [Google Scholar] [CrossRef] [PubMed]
- Forbes, S.C.; Candow, D.G.; Ostojic, S.M.; Roberts, M.D.; Chilibeck, P.D. Meta-analysis examining the importance of creatine ingestion strategies on lean tissue mass and strength in older adults. Nutrients 2021, 13, 1912. [Google Scholar] [CrossRef]
- Kreider, R.B.; Stout, J.R. Creatine in health and disease. Nutrients 2021, 13, 447. [Google Scholar] [CrossRef] [PubMed]
- Harmon, K.K.; Stout, J.R.; Fukuda, D.H.; Pabian, P.S.; Rawson, E.S.; Stock, M.S. The Application of creatine supplementation in medical rehabilitation. Nutrients 2021, 13, 1825. [Google Scholar] [CrossRef]
- Li, B.; Yang, L. Creatine in T Cell antitumor immunity and cancer immunotherapy. Nutrients 2021, 13, 1633. [Google Scholar] [CrossRef] [PubMed]
- Wallimann, T.; Hall, C.H.T.; Colgan, S.P.; Glover, L.E. Creatine supplementation for patients with inflammatory bowl diseases: A scientific rationale for a clinical trial. Nutrients 2021, 13, 1429. [Google Scholar] [CrossRef]
- Balestrino, M. Role of creatine in the heart: Health and disease. Nutrients 2021, 13, 1215. [Google Scholar] [CrossRef] [PubMed]
- Muccini, A.M.; Tran, N.T.; de Guingand, D.L.; Philip, M.; Della Gatta, P.A.; Galinsky, R.; Sherman, L.S.; Kelleher, M.A.; Palmer, K.R.; Berry, M.J.; et al. Creatine metabolism in female reproduction, pregnancy and newborn health. Nutrients 2021, 13, 490. [Google Scholar] [CrossRef]
- Stricker, P.R.; Faigenbaum, A.D.; McCambridge, T.M. Resistance training for children and adolescents. Pediatrics 2020, 145. [Google Scholar] [CrossRef]
- Talar, K.; Hernández-Belmonte, A.; Vetrovsky, T.; Steffl, M.; Kałamacka, E.; Courel-Ibáñez, J. Benefits of Resistance training in early and late stages of frailty and sarcopenia: A systematic review and meta-analysis of randomized controlled studies. J. Clin. Med. 2021, 10, 1630. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.W. Periodized resistance training for enhancing skeletal muscle hypertrophy and strength: A mini-review. Front. Physiol. 2019, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, D.A.; Benítez-Porres, J.; Romance, R.; Medina, I.; Petro, J.L.; Schoenfeld, B.J.; García-Sillero, M.; Kreider, R.B.; Vargas-Molina, S. Effects of a non-linear resistance training program on biochemical and physiological health parameters in elderly. Med. Sci. Sports Exerc. 2020, 52, 749. [Google Scholar] [CrossRef]
- Vargas-Molina, S.; Romance, R.; Schoenfeld, B.J.; García, M.; Petro, J.L.; Bonilla, D.A.; Kreider, R.B.; Martín-Rivera, F.; Benítez-Porres, J. Effects of cluster training on body composition and strength in resistance-trained men. Isokinet. Exerc. Sci. 2020, 28, 391–399. [Google Scholar] [CrossRef]
- Garcia-Ramos, A.; Gonzalez-Hernandez, J.M.; Banos-Pelegrin, E.; Castano-Zambudio, A.; Capelo-Ramirez, F.; Boullosa, D.; Haff, G.G.; Jimenez-Reyes, P. Mechanical and metabolic responses to traditional and cluster set configurations in the bench press exercise. J. Strength Cond. Res. 2020, 34, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Morales-Artacho, A.J.; Padial, P.; Garcia-Ramos, A.; Perez-Castilla, A.; Feriche, B. Influence of a cluster set configuration on the adaptations to short-term power training. J. Strength Cond. Res. 2018, 32, 930–937. [Google Scholar] [CrossRef]
- Tufano, J.J.; Halaj, M.; Kampmiller, T.; Novosad, A.; Buzgo, G. Cluster sets vs. traditional sets: Levelling out the playing field using a power-based threshold. PLoS ONE 2018, 13, e0208035. [Google Scholar] [CrossRef]
- Latella, C.; Teo, W.-P.; Drinkwater, E.J.; Kendall, K.; Haff, G.G. The acute neuromuscular responses to cluster set resistance training: A systematic review and meta-analysis. Sports Med. 2019, 49, 1861–1877. [Google Scholar] [CrossRef] [Green Version]
- Marshall, J.; Bishop, C.; Turner, A.; Haff, G.G. Optimal training sequences to develop lower body force, velocity, power, and jump height: A systematic review with meta-analysis. Sports Med. 2021, 51, 1245–1271. [Google Scholar] [CrossRef]
- Arazi, H.; Khoshnoud, A.; Asadi, A.; Tufano, J.J. The effect of resistance training set configuration on strength and muscular performance adaptations in male powerlifters. Sci. Rep. 2021, 11, 7844. [Google Scholar] [CrossRef]
- Jukic, I.; Van Hooren, B.; Ramos, A.G.; Helms, E.R.; McGuigan, M.R.; Tufano, J.J. The effects of set structure manipulation on chronic adaptations to resistance training: A systematic review and meta-analysis. Sports Med. 2021, 51, 1061–1086. [Google Scholar] [CrossRef]
- Willardson, J.M. A Brief Review: Factors affecting the length of the rest interval between resistance exercise sets. J. Strength Cond. Res. 2006, 20. [Google Scholar] [CrossRef]
- Harris, R.C.; Edwards, R.H.; Hultman, E.; Nordesjo, L.O.; Nylind, B.; Sahlin, K. The time course of phosphorylcreatine resynthesis during recovery of the quadriceps muscle in man. Pflugers Arch. 1976, 367, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Hansen, K.T.; Cronin, J.B.; Newton, M.J. The effect of cluster loading on force, velocity, and power during ballistic jump squat training. Int. J. Sports Physiol. Perform. 2011, 6, 455–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iglesias-Soler, E.; Carballeira, E.; Sanchez-Otero, T.; Mayo, X.; Fernandez-del-Olmo, M. Performance of maximum number of repetitions with cluster-set configuration. Int. J. Sports Physiol. Perform. 2014, 9, 637–642. [Google Scholar] [CrossRef]
- Moreno, S.D.; Brown, L.E.; Coburn, J.W.; Judelson, D.A. Effect of cluster sets on plyometric jump power. J. Strength Cond. Res. 2014, 28, 2424–2428. [Google Scholar] [CrossRef] [PubMed]
- Asadi, A.; Ramirez-Campillo, R. Effects of cluster vs. traditional plyometric training sets on maximal-intensity exercise performance. Medicina 2016, 52, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. Pilot Feasibility Stud. 2016, 2. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Postgrad. Med. 2002, 48, 206–208. [Google Scholar]
- Vargas-Molina, S.; Petro, J.L.; Romance, R.; Kreider, R.B.; Schoenfeld, B.J.; Bonilla, D.A.; Benitez-Porres, J. Effects of a ketogenic diet on body composition and strength in trained women. J. Int. Soc. Sports Nutr. 2020, 17, 19. [Google Scholar] [CrossRef] [Green Version]
- Rozenek, R.; Ward, P.; Long, S.; Garhammer, J. Effects of high-calorie supplements on body composition and muscular strength following resistance training. J. Sports Med. Phys. Fit. 2002, 42, 340–347. [Google Scholar]
- Campbell, B.; Kreider, R.B.; Ziegenfuss, T.; La Bounty, P.; Roberts, M.; Burke, D.; Landis, J.; Lopez, H.; Antonio, J. International Society of Sports Nutrition position stand: Protein and exercise. J. Int. Soc. Sports Nutr. 2007, 4. [Google Scholar] [CrossRef] [Green Version]
- Heymsfield, S.B.; Gallagher, D.; Kotler, D.P.; Wang, Z.; Allison, D.B.; Heshka, S. Body-size dependence of resting energy expenditure can be attributed to nonenergetic homogeneity of fat-free mass. Am. J. Physiol. Endocrinol. Metab. 2002, 282, E132–E138. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Dankel, S.J.; Loenneke, J.P. Body fat loss automatically reduces lean mass by changing the fat-free component of adipose tissue. Obesity 2019, 27, 357–358. [Google Scholar] [CrossRef]
- Abe, T.; Loenneke, J.P.; Thiebaud, R.S.; Fujita, E.; Akamine, T. The impact of DXA-derived fat-free adipose tissue on the prevalence of low muscle mass in older adults. Eur. J. Clin. Nutr. 2018, 73, 757–762. [Google Scholar] [CrossRef] [PubMed]
- McGuigan, M. Administration, scoring, and interpretation of selected tests. In Essentials of Strength Training and Conditioning; Haff, G., Triplett, N., Eds.; Human Kinetics: Champaign, IL, USA, 2016; pp. 265–266. [Google Scholar]
- Caulfield, S.; Berninger, D. Exercise technique for free weight and machine training. In Essentials of Strength Training and Conditioning—National Strength and Conditioning Association; Haff, G., Triplett, T., Eds.; Human Kinetics: Champaign, IL, USA, 2016; Volume 4, p. 735. [Google Scholar]
- Morris, N.S.; Rosenbloom, D.A. Defining and understanding pilot and other feasibility studies. Am. J. Nurs. 2017, 117, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, J.A. Qualitative Descriptors of strength of association and effect size. J. Soc. Serv. Res. 1996, 21, 37–59. [Google Scholar] [CrossRef]
- Cannataro, R.; Cione, E.; Gallelli, L.; Marzullo, N.; Bonilla, D.A. Acute effects of supervised making weight on health markers, hormones and body composition in muay thai fighters. Sports 2020, 8, 137. [Google Scholar] [CrossRef]
- Cumming, G. Understanding the New Statistics; Effect Sizes, Confidence Intervals, and Meta-Analysis, 1st ed.; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Johannsmeyer, S.; Candow, D.G.; Brahms, C.M.; Michel, D.; Zello, G.A. Effect of creatine supplementation and drop-set resistance training in untrained aging adults. Exp. Gerontol. 2016, 83, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, D.A.; Pérez-Idárraga, A.; Odriozola-Martínez, A.; Kreider, R.B. The 4R’s framework of nutritional strategies for post-exercise recovery: A review with emphasis on new generation of carbohydrates. Int. J. Environ. Res. Public Health 2020, 18, 103. [Google Scholar] [CrossRef]
- Dias, R.K.N.; Penna, E.M.; Noronha, A.S.N.; de Azevedo, A.B.C.; Barbalho, M.; Gentil, P.V.; Coswig, V.S. Cluster-sets resistance training induce similar functional and strength improvements than the traditional method in postmenopausal and elderly women. Exp. Gerontol. 2020, 138. [Google Scholar] [CrossRef]
- Lanhers, C.; Pereira, B.; Naughton, G.; Trousselard, M.; Lesage, F.-X.; Dutheil, F. Creatine supplementation and lower limb strength performance: A systematic review and meta-analyses. Sports Med. 2015, 45, 1285–1294. [Google Scholar] [CrossRef]
- Latella, C.; Peddle-McIntyre, C.; Marcotte, L.; Steele, J.; Kendall, K.; Fairman, C.M. Strengthening the case for cluster set resistance training in aged and clinical settings: Emerging evidence, proposed benefits and suggestions. Sports Med. 2021. [Google Scholar] [CrossRef]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.i.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-related loss of muscle mass and function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef]
- Newman, A.; Suetta, C.; Frandsen, U.; Alegre, L.M.; Prescott, E.; Hansen, S.K.; Kamper, R.S.; Haddock, B.; Aagaard, P.; Alcazar, J. Age-and sex-specific changes in lower-limb muscle power throughout the lifespan. J. Gerontol. Ser. A 2020, 75, 1369–1378. [Google Scholar] [CrossRef]
- Morris, R.; Lewis, A. Falls and Cancer. Clin. Oncol. 2020, 32, 569–578. [Google Scholar] [CrossRef]
- Alway, S.E.; Lee, S.Y.; Ro, H.J.; Chung, S.G.; Kang, S.H.; Seo, K.M.; Kim, D.-K. Low skeletal muscle mass in the lower limbs is independently associated to knee osteoarthritis. PLoS ONE 2016, 11. [Google Scholar] [CrossRef]
- Marini, A.C.B.; Pimentel, G.D. Creatine supplementation plus neuromuscular electrical stimulation improves lower-limb muscle strength and quality of life in hemodialysis men. Einstein Sao Paolo 2020, 18. [Google Scholar] [CrossRef]
- Post, A.; Schutten, J.C.; Kremer, D.; van der Veen, Y.; Groothof, D.; Sotomayor, C.G.; Koops, C.A.; de Blaauw, P.; Kema, I.P.; Westerhuis, R.; et al. Creatine homeostasis and protein energy wasting in hemodialysis patients. J. Transl. Med. 2021, 19. [Google Scholar] [CrossRef] [PubMed]
- Jäger, R.; Kerksick, C.M.; Campbell, B.I.; Cribb, P.J.; Wells, S.D.; Skwiat, T.M.; Purpura, M.; Ziegenfuss, T.N.; Ferrando, A.A.; Arent, S.M.; et al. International Society of Sports Nutrition Position Stand: Protein and exercise. J. Int. Soc. Sports Nutr. 2017, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helms, E.R.; Aragon, A.A.; Fitschen, P.J. Evidence-based recommendations for natural bodybuilding contest preparation: Nutrition and supplementation. J. Int. Soc. Sports Nutr. 2014, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etikan, I.; Babtope, O. A basic approach in sampling methodology and sample size calculation. MedLife Clin. 2019, 1, 1006. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Exercises | Sets per Exercise | Reps per Set | Clusters per Set | Intra-Set Rest (s) | Inter-Set Rest (s) |
|---|---|---|---|---|---|---|
| CS-RT+CrM | Squat, deadlift, and leg press * | 3 | 12 | 4 × 3RM | 20 | 180 |
| CS-RT | 3 | 12 | 4 × 3RM | 20 | 180 | |
| Control | Followed their habitual diet and training programs (no recorded) | |||||
| Variable | CS-RT+CrM (n = 8) (SD) | 95% CI (min, max) | CS-RT (n = 8) (SD) | 95% CI (min, max) | Control (n = 7) (SD) | 95% CI (min, max) |
|---|---|---|---|---|---|---|
| Body mass (kg) | 76.41 (6.72) | 70.79, 82.03 | 75.09 (11.69) | 65.31, 84.86 | 75.22 (8.83) | 67.04, 83.39 |
| Stature (cm) | 179.41 (5.07) | 175.16, 183.65 | 173.31 (7.72) | 166.85, 179.77 | 176.45 (7.47) | 169.54, 183.36 |
| BMI (kg∙m−2) | 23.89 (1.71) | 22.45, 25.32 | 25.02 (2.73) | 22.73, 27.31 | 24.25 (2.51) | 22.82, 25.68 |
| Body fatDXA (%) | 18.00 (4.45) | 14.27, 21.73 | 16.63 (3.27) | 13.89, 19.36 | 15.72 (3.99) | 12.02, 19.41 |
| FMDXA (kg) | 13.89 (4.15) | 10.42, 17.37 | 12.62 (3.65) | 9.56, 15.67 | 12.04 (4.32) | 8.04, 16.05 |
| FFATtotal (kg) | 2.45 (0.73) | 1.84, 3.06 | 2.22 (0.64) | 1.68, 2.76 | 2.12 (0.76) | 1.42, 2.83 |
| FFMDXA (kg) | 62.51 (4.69) | 58.59, 66.43 | 62.47 (8.98) | 54.95, 69.98 | 63.17 (5.69) | 57.90, 68.44 |
| FFMDXA minus FFATtotal (kg) | 60.06 (4.63) | 56.18, 63.93 | 60.24 (8.58) | 53.06, 67.42 | 61.04 (5.32) | 56.12, 65.96 |
| LL-mass (kg) | 38.70 (3.83) | 35.49, 41.90 | 37.10 (6.55) | 31.6, 42.58 | 38.10 (4.97) | 33.50, 42.71 |
| LL-FMDXA (kg) | 8.03 (2.83) | 5.67, 10.40 | 7.11 (2.17) | 5.30, 8.93 | 6.66 (2.58) | 4.27, 9.05 |
| LL-FFAT (kg) | 1.41 (0.49) | 1.00, 1.83 | 1.25 (0.38) | 0.93, 1.57 | 1.17 (0.45) | 0.75, 1.59 |
| LL-FFMDXA (kg) | 30.66 (2.42) | 28.63, 32.69 | 29.98 (5.01) | 25.78, 34.18 | 31.44 (3.01) | 28.65, 34.23 |
| LL-FFM minus LL-FFAT (kg) | 29.24 (2.45) | 27.19, 31.29 | 28.72 (4.79) | 24.71, 32.74 | 30.27 (2.77) | 27.70, 32.84 |
| SQ-1RM (kg) | 110.62 (13.36) | 99.45, 121.79 | 113.00 (16.82) | 98.93, 127.06 | 113.00 (16.02) | 98.18, 127.81 |
| CMJ (cm) | 38.92 (5.64) | 34.20, 43.64 | 39.14 (4.69) | 35.21, 43.06 | 38.47 (5.91) | 33.00, 43.95 |
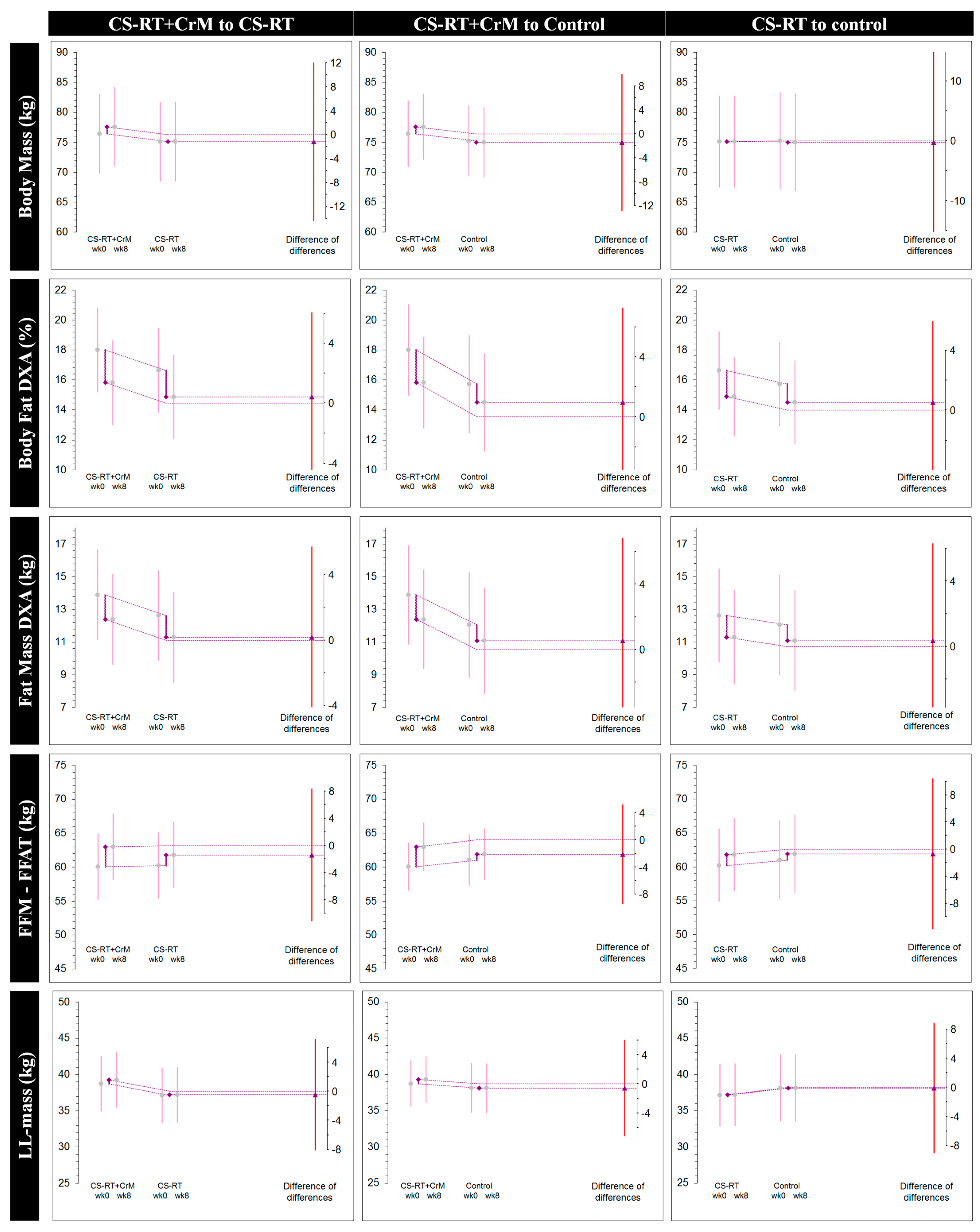
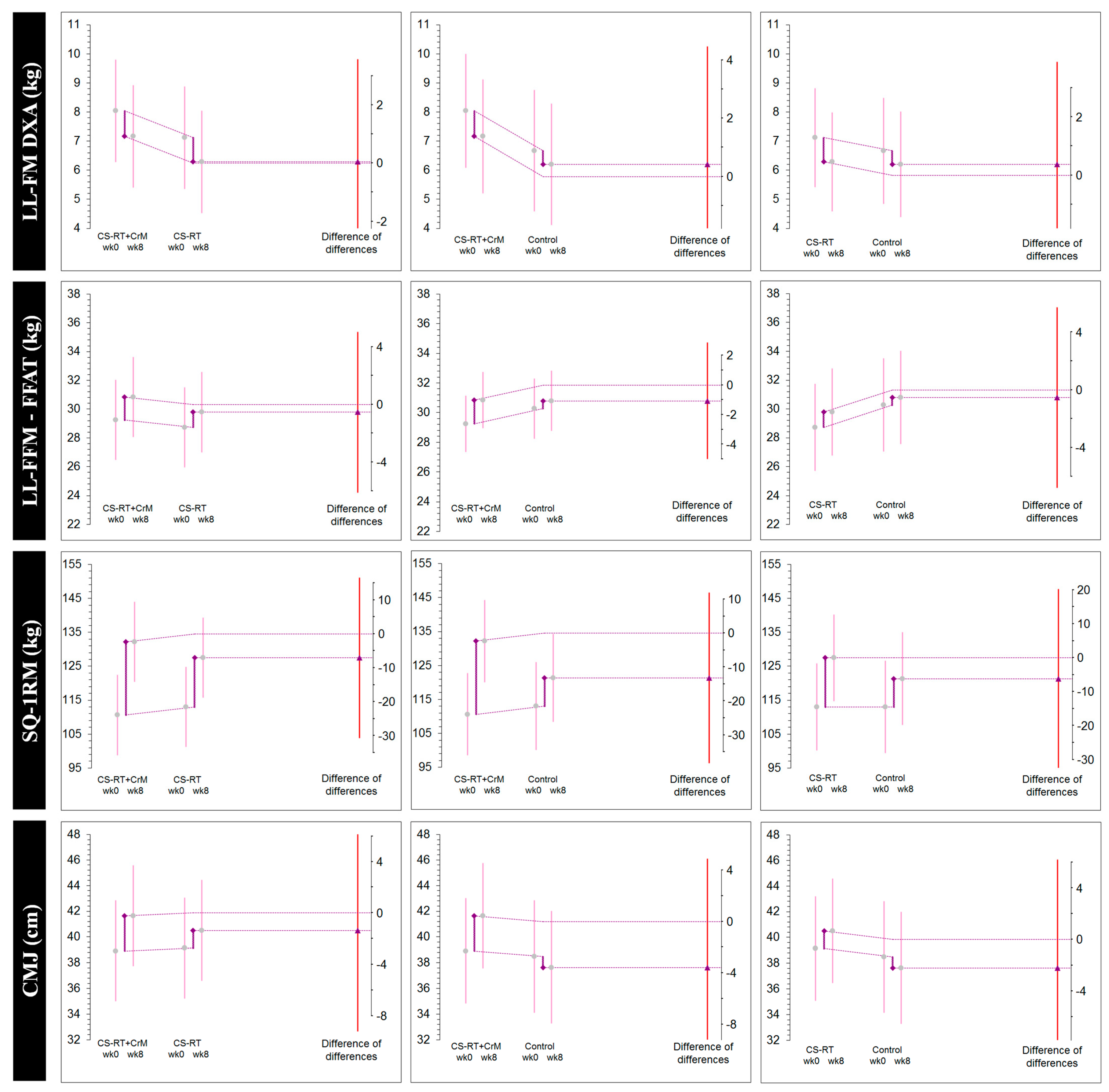
| Variable | Group | Week 0 (SD) | Week 8 (SD) | Δ (SD) [95% CI] | dunb δ [95% CI] |
|---|---|---|---|---|---|
| Body mass (kg) | CS-RT+CrM | 76.41 (6.72) | 77.59 (4.89) | 1.18 (2.33) [–0.76, 3.13] | 0.17 [–0.09, 0.48] |
| CS-RT | 75.09 (11.69) | 75.11 (11.34) | 0.01 (1.17) [–0.96, 1.00] | 0.00 [–0.06, 0.07] | |
| Control | 75.22 (8.83) | 74.96 (9.52) | –0.25 (2.16) [–2.25, 1.74] | –0.02 [–0.20, 0.14] | |
| Body fatDXA (%) | CS-RT+CrM | 18.00 (4.45) | 15.81 (4.37) | –2.18 (0.82) [–2.88, –1.49] * | –0.44 [–0.77, –0.20] |
| CS-RT | 16.63 (3.27) | 14.87 (3.28) | –1.75 (1.41) [–2.94, –0.56] * | –0.47 [–0.93, –0.11] | |
| Control | 15.72 (3.99) | 14.49 (3.91) | –1.22 (1.08) [–2.23, –0.22] * | –0.27 [–0.57, –0.03] | |
| FMDXA (kg) | CS-RT+CrM | 13.89 (4.15) | 12.39 (3.92) | –1.50 (0.88) [–2.24, –0.76] * | –0.33 [–0.61, –0.12] |
| CS-RT | 12.62 (3.65) | 11.30 (3.56) | –1.32 (1.12) [–2.26, –0.37] * | –0.36 [–0.64, –0.07] | |
| Control | 12.04 (4.32) | 11.08 (4.35) | –0.96 (0.97) [–1.86, –0.06] * | –0.19 [–0.42, –0.01] | |
| FFMDXA minus FFATtotal (kg) | CS-RT+CrM | 60.06 (4.63) | 63.01 (3.35) | 2.95 (1.68) [1.54, 4.35] * | 0.64 [0.24, 1.19] |
| CS-RT | 60.24 (8.58) | 61.81 (8.62) | 1.57 (1.09) [0.65, 2.48] * | 0.16 [0.05, 0.30] | |
| Control | 61.04 (5.32) | 61.92 (6.04) | 0.87 (1.91) [–0.89, 2.64] | 0.13 [–0.11, 0.41] | |
| LL-mass (kg) | CS-RT+CrM | 38.70 (3.83) | 39.26 (3.44) | 0.55 (0.99) [–0.27, 1.38] | 0.13 [–0.05, 0.35] |
| CS-RT | 37.10 (6.55) | 37.17 (6.53) | 0.07 (1.00) [–0.76, 0.91] | 0.01 [–0.09, 0.11] | |
| Control | 38.10 (4.97) | 38.09 (5.34) | –0.01 (1.08) [–1.01, 0.99] | –0.002 [–0.15, 0.15] | |
| LL-FMDXA (kg) | CS-RT+CrM | 8.03 (2.83) | 7.16 (2.65) | –0.87 (0.44) [–1.24, –0.51] * | –0.28 [–0.51, –0.11] |
| CS-RT | 7.11 (2.17) | 6.28 (1.96) | –0.83 (0.72) [–1.44, –0.22] * | –0.35 [–0.71, –0.07] | |
| Control | 6.66 (2.58) | 6.20 (2.64) | –0.45 (0.50) [–0.92, 0.006] * | –0.15 [–0.34, 0.002] | |
| LL-FFM minus LL-FFAT (kg) | CS-RT+CrM | 29.24 (2.45) | 30.83 (2.09) | 1.59 (0.70) [1.00, 2.18] * | 0.62 [0.27, 1.11] |
| CS-RT | 28.72 (4.79) | 29.78 (5.10) | 1.05 (0.43) [0.69, 1.41] * | 0.18 [0.08, 0.33] | |
| Control | 30.27 (2.77) | 30.79 (3.15) | 0.52 (1.12) [–0.51, 1.56] | 0.15 [–0.12, 0.46] | |
| SQ-1RM (kg) | CS-RT+CrM | 110.62 (13.36) | 132.16 (17.27) | 21.53 (11.19) [12.17, 30.89] * | 1.23 [0.50, 2.25] |
| CS-RT | 113.00 (16.82) | 127.50 (17.48) | 14.50 (12.27) [4.24, 24.75] * | 0.75 [0.17, 1.48] | |
| Control | 113.00 (16.02) | 121.31 (19.87) | 8.31 (9.02) [–0.03, 16.66] | 0.40 [–0.001, 0.89] | |
| CMJ (cm) | CS-RT+CrM | 38.92 (5.64) | 41.65 (5.23) | 2.72 (1.99) [1.06, 4.39] * | 0.44 [0.13, 0.85] |
| CS-RT | 39.14 (4.69) | 40.50 (6.01) | 1.36 (4.42) [–2.34, 5.06] | 0.22 [–0.33, 0.82] | |
| Control | 38.47 (5.91) | 37.63 (5.71) | –0.84 (3.23) [–3.82, 2.14] | –0.12 [–0.55, 0.28] |
| DID for CS-RT+CrM (Δ1) and CS-RT (Δ2) | DID for CS-RT+CrM (Δ1) and Control (Δ3) | DID for CS-RT (Δ2) and Control (Δ3) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Mean (Δ2–Δ1) | DID | 95% CI | p | Mean (Δ3–Δ1) | DID | 95% CI | p | Mean (Δ3–Δ2) | DID | 95% CI | p |
| Body mass (kg) | 0.01–1.18 | −1.16 | −14.41, 12.08 | 0.858 | −0.25–1.18 | −1.44 | −12.86, 9.97 | 0.797 | −0.25–0.01 | −0.27 | −16.09, 15.53 | 0.972 |
| Body fatDXA (%) | −1.75–−2.18 | 0.43 | −5.20, 6.07 | 0.876 | −1.22–−2.18 | 0.96 | −5.37, 7.29 | 0.758 | −1.22–−1.75 | 0.52 | −4.90, 5.95 | 0.843 |
| FMDXA (kg) | −1.32–−1.50 | 0.18 | −5.36, 5.73 | 0.947 | −0.96–−1.50 | 0.53 | −5.75, 6.83 | 0.862 | −0.96–−1.32 | 0.35 | −5.60, 6.31 | 0.903 |
| FFMDXA minus FFAT total (kg) | 1.57–2.95 | −1.38 | −11.12, 8.34 | 0.774 | 0.87–2.95 | −2.07 | −9.41, 5.25 | 0.566 | 0.87–1.57 | −0.69 | −11.84, 10.44 | 0.899 |
| LL-mass (kg) | 0.07–0.55 | −0.48 | −8.15, 7.18 | 0.898 | −0.01–0.55 | −0.57 | −7.21, 6.06 | 0.861 | −0.01–0.07 | −0.087 | −9.03, 8.86 | 0.984 |
| LL-FMDXA (kg) | −0.83–−0.87 | 0.04 | −3.47 3.56 | 0.980 | −0.45–−0.87 | 0.41 | −3.62, 4.46 | 0.833 | −0.45–−0.83 | 0.37 | −3.14, 3.89 | 0.828 |
| LL-FFM minus LL-FFAT (kg) | 1.05–1.59 | −0.53 | −6.12, 5.04 | 0.845 | 0.52–−1.59 | −1.06 | −5.01, 2.88 | 0.583 | 0.52–1.05 | −0.53 | −6.78, 5.72 | 0.863 |
| SQ-1RM (kg) | 14.50–21.53 | −7.03 | −30.68, 16.60 | 0.547 | 8.31–21.53 | −13.22 | −38.34, 11.89 | 0.289 | 8.31–14.50 | −6.18 | −32.63, 20.25 | 0.635 |
| CMJ (cm) | 1.36–2.72 | −1.36 | −9.21, 6.48 | 0.724 | −0.84–2.72 | −3.56 | −12.02, 4.88 | 0.394 | −0.84–1.36 | −2.203 | −10.62, 6.21 | 0.595 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonilla, D.A.; Kreider, R.B.; Petro, J.L.; Romance, R.; García-Sillero, M.; Benítez-Porres, J.; Vargas-Molina, S. Creatine Enhances the Effects of Cluster-Set Resistance Training on Lower-Limb Body Composition and Strength in Resistance-Trained Men: A Pilot Study. Nutrients 2021, 13, 2303. https://doi.org/10.3390/nu13072303
Bonilla DA, Kreider RB, Petro JL, Romance R, García-Sillero M, Benítez-Porres J, Vargas-Molina S. Creatine Enhances the Effects of Cluster-Set Resistance Training on Lower-Limb Body Composition and Strength in Resistance-Trained Men: A Pilot Study. Nutrients. 2021; 13(7):2303. https://doi.org/10.3390/nu13072303
Chicago/Turabian StyleBonilla, Diego A., Richard B. Kreider, Jorge L. Petro, Ramón Romance, Manuel García-Sillero, Javier Benítez-Porres, and Salvador Vargas-Molina. 2021. "Creatine Enhances the Effects of Cluster-Set Resistance Training on Lower-Limb Body Composition and Strength in Resistance-Trained Men: A Pilot Study" Nutrients 13, no. 7: 2303. https://doi.org/10.3390/nu13072303
APA StyleBonilla, D. A., Kreider, R. B., Petro, J. L., Romance, R., García-Sillero, M., Benítez-Porres, J., & Vargas-Molina, S. (2021). Creatine Enhances the Effects of Cluster-Set Resistance Training on Lower-Limb Body Composition and Strength in Resistance-Trained Men: A Pilot Study. Nutrients, 13(7), 2303. https://doi.org/10.3390/nu13072303