
Caregiver Feeding Practices as Predictors for Child Dietary Intake in Low-Income, Appalachian Communities



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participant Eligibility Criteria
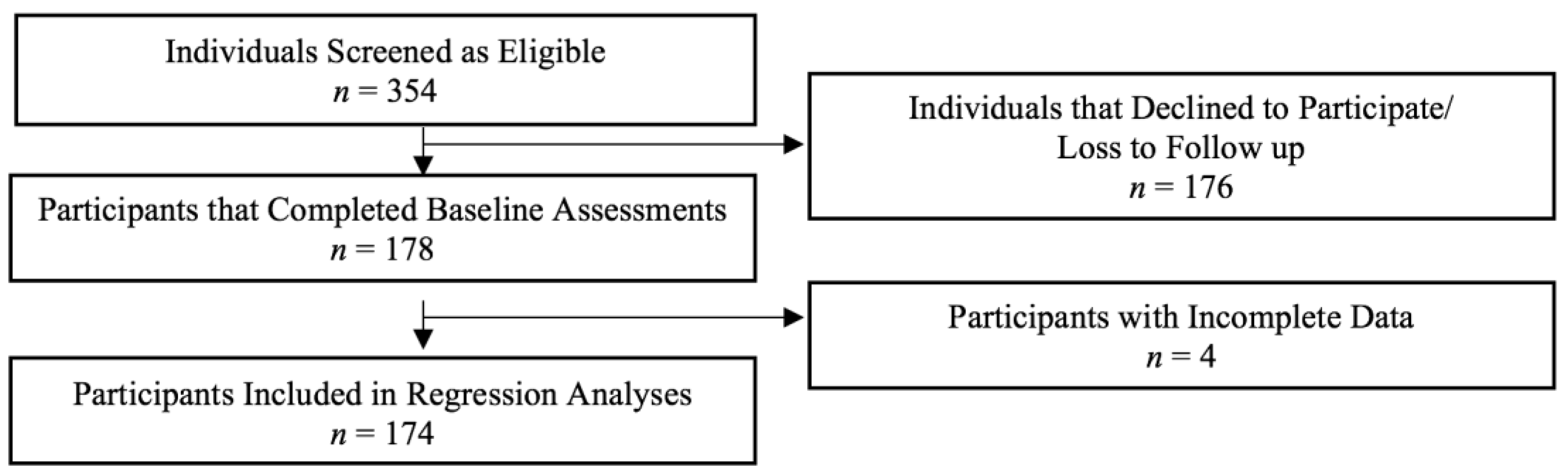
2.2. Recruitment and Data Collection
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Modeling, Caregiver Dietary Intake, and Home Food Availability
3.3. Caregiver Self-Reported Child and Caregiver Dietary Intake
3.4. Multiple Linear Regression Predicting Child Fruit Consumption
3.5. Multiple Linear Regression Predicting Child Vegetable Consumption
3.6. Multiple Linear Regression Predicting Child HS/HF Snack Food Consumption
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- US Department of Agriculture and US Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th ed.; 2020. Available online: DietaryGuidelines.gov (accessed on 7 August 2021).
- Krebs-Smith, S.M.; Guenther, P.M.; Subar, A.F.; Kirkpatrick, S.I.; Dodd, K.W. Americans Do Not Meet Federal Dietary Recommendations. J. Nutr. 2010, 140, 1832–1838. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Children Eating More Fruit, But Fruit and Vegetable Intake Still too Low. Available online: https://www.cdc.gov/nccdphp/dnpao/division-information/media-tools/dpk/vs-fruits-vegetables/index.html (accessed on 27 November 2018).
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. Dietary Guidelines for Americans 2015–2020, 8th ed.; USDA Publication: Washington, DC, USA, 2015; Volume 18. [CrossRef]
- Alsharairi, N.A.N.; Somerset, S.M. Associations between parenting styles and children’s fruit and vegetable intake. Ecol. Food Nutr. 2015, 54, 93–113. [Google Scholar] [CrossRef] [PubMed]
- Burnett, A.J.; Lamb, K.E.; McCann, J.; Worsley, A.; Lacy, K.E. Parenting styles and the dietary intake of pre-school children: A systematic review. Psychol. Health 2020, 35, 1326–1345. [Google Scholar] [CrossRef] [PubMed]
- Van der Horst, K.; Sleddens, E.F.C. Parenting styles and food-related parenting practices in relations to toddlers’ eating styles: A cluster analytics approach. PLoS ONE 2017, 12, e0178149. [Google Scholar] [CrossRef] [Green Version]
- Yee, A.Z.H.; Lwin, M.O.; Ho, S.S.; Kim, W. The influence of parental practices on child promotive and preventive food consumption behaviors: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14. [Google Scholar] [CrossRef]
- Draxten, M.; Fulkerson, J.A.; Friend, S.; Flattum, C.F.; Schow, R. Parental role modeling of fruits and vegetables at meals and snacks is associated with children’s adequate consumption. Appetite 2014, 78, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Modeling Theory: Some Traditions, Trends, and Disputes. In Recent Trends in Social Learning Theory; Elsevier: Amsterdam, The Netherlands, 1972; pp. 35–61. [Google Scholar] [CrossRef]
- Rolling, T.E.; Hong, M.Y. The effect of social cognitive theory-based interventions on dietary behaviors within children. J. Nutr. Health Food Sci. 2016, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Sleddens, E.F.C.; Kremers, S.P.J.; De Vries, N.K.; Thijs, C. Relationship between parental feeding styles and eating behaviours of Dutch children aged 6–7. Appetite 2010, 54, 30–36. [Google Scholar] [CrossRef]
- Goldman, R.L.; Radnitz, C.L.; McGrath, R.E. The role of family variables in fruit and vegetable consumption in pre-school children. J. Public Health Res. 2012, 1, 143–148. [Google Scholar] [CrossRef] [Green Version]
- Couch, S.C.; Glanz, K.; Zhou, C.; Sallis, J.F.; Saelens, B.E. Home Food Environment in Relation to Children’s Diet Quality and Weight Status. J. Acad. Nutr. Diet. 2014, 114, 1569–1579.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palfreyman, Z.; Haycraft, E.; Meyer, C. Development of the Parental Modelling of Eating Behaviours Scale (PARM): Links with food intake among children and their mothers. Matern. Child Nutr. 2014, 10, 617–629. [Google Scholar] [CrossRef] [Green Version]
- Vaughn, A.E.; Dearth-Wesley, T.; Tabak, R.G.; Bryant, M.; Ward, D.S. Development of a Comprehensive Assessment of Food Parenting Practices: The Home Self-Administered Tool for Environmental Assessment of Activity and Diet Family Food Practices Survey. J. Acad. Nutr. Diet. 2017, 117, 214–227. [Google Scholar] [CrossRef] [PubMed]
- Loth, K.A.; MacLehose, R.F.; Larson, N.; Berge, J.M.; Neumark-Sztainer, D. Food availability, modeling and restriction: How are these different aspects of the family eating environment related to adolescent dietary intake? Appetite 2016, 96, 80–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Østbye, T.; Krause, K.M.; Stroo, M.; Lovelady, C.A.; Evenson, K.R.; Peterson, B.L.; Bastian, L.A.; Swamy, G.K.; West, D.G.; Brouver, R.J.N.; et al. Parent-focused change to prevent obesity in preschoolers: Results from the KAN-DO study. Prev. Med. 2012, 55, 188–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blissett, J. Relationships between parenting style, feeding style and feeding practices and fruit and vegetable consumption in early childhood. Appetite 2011, 57, 826–831. [Google Scholar] [CrossRef] [PubMed]
- Carbert, N.S.; Brussoni, M.; Geller, J.; Masse, L.C. Moderating effects of family environment on overweight/obese adolescents’ dietary behaviors. Appetite 2019, 134, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Fleary, S.A.; Ettienne, R. The relationship between food parent practices, parental diet and their adolescents’ diet. Appetite 2019, 135, 79–85. [Google Scholar] [CrossRef]
- Coto, J.; Pulgaron, E.R.; Graziana, P.A.; Bagner, D.M.; Villa, M.; Malik, J.A.; Delamater, A.M. Parents and role models: Associations between parent and young children’s weight, dietary intake, and physical activity in a minority sample. Matern. Child Health J. 2019, 23, 943–950. [Google Scholar] [CrossRef]
- Melbye, E.L.; Hansen, H. Promotion and Prevention Focused Feeding Strategies: Exploring the Effects on Healthy and Unhealthy Child Eating. Biomed. Res Int. 2015, 2015, 306306. [Google Scholar] [CrossRef]
- Boots, S.B.; Tiggemann, M.; Corsini, N.; Mattiske, J. Managing young children’s snack food intake. The role of parenting style and feeding strategies. Appetite 2015, 92, 94–101. [Google Scholar] [CrossRef]
- Rasmussen, M.; Krølner, R.; Klepp, K.-I.; Lytle, L.; Brug, J.; Bere, E.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part I: Quantitative studies. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 22. [Google Scholar] [CrossRef] [Green Version]
- Marshall, J.; Thomas, L.; Lane, N.; Holmes, G.M.; Arcury, T.A.; Randolph, R.; Silberman, P.; Holding, W.; Villamil, L.; Thomas, S.; et al. Health Disparities in Appalachia: The First Report in a Series Exploring Health Issues in Appalachia; Appalachian Regional Commission: Washington, DC, USA, 2017.
- Beatty, K.; Hale, N.; Meit, M. Issue Brief: Health Disparities Related to Obesity in Appalachia—Practical Strategies and Recommendations for Communities. ETSU: Johnson City, TN, USA, 2019. [Google Scholar]
- Pollard, K.; Jacobsen, L.A. American Community Survey Chartbook; Appalachian Regional Commission: Washington, DC, USA, 2019; The Appalachian Region: A Data Overview from the 2013–2017.
- Hendryx, M.; Luo, J.; Borders, T. Health Disparities in Appalachia. Health Aff. 2017, 36, 2213. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.; United States Department of Agriculture. The Differences in Characteristics among Households with and without Obese Children: Findings from USDA’s FoodAPS. 2017. Available online: www.ers.usda.gov (accessed on 5 January 2018).
- Johnson, J.; Johnson, M. Urban-Rural Differences in Childhood and Adolescent Obesity in the United States: A Systematic Review and Meta-Analysis. Child. Obes. 2015, 11, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-H.; Jones, S.J.; Sun, H.; Probst, J.C.; Merchant, A.T.; Cavicchia, P. Diet, Physical Activity, and Sedentary Behaviors as Risk Factors for Childhood Obesity: An Urban and Rural Comparison. Child. Obes. 2012, 8, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Forshee, R.A.; Storey, M.L. Demographics, not beverage consumption, is associated with diet quality. Int. J. Food Sci. Nutr. 2006, 57, 494–511. [Google Scholar] [CrossRef]
- Jackson, J.; Smit, E.; Manore, M.; John, D.; Gunter, K. The Family-Home Nutrition Environment and Dietary Intake in Rural Children. Nutrients 2015, 7, 9707–9720. [Google Scholar] [CrossRef] [Green Version]
- Anderson Steeves, E.; Grier-Welch, A.; McIver, K.; Sweet, C.L.; Sneed, C.; Franck, K.; Burney, J. Process Evaluation of the Shop Smart Tennessee Intervention to Increase Access to and Demand for Healthier, Staple Food Items in Convenience Stores in Low-Income, Rural Appalachian Communities. Presented at the American Public Health Association Annual Meeting and Expo, Philadelphia, PA, USA, 2–6 November 2019.
- Hager, E.R.; Quigg, A.M.; Black, M.M.; Coleman, S.M.; Heeren, T.; Rose-Jacobs, R.; Cook, J.T.; de Cuba, S.A.E.; Casey, P.H.; Chilton, M.; et al. Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics 2010, 126. [Google Scholar] [CrossRef] [Green Version]
- Fulkerson, J.A.; Nelson, M.C.; Lytle, L.; Moe, S.; Heitzler, C.; Pasch, K.E. International Journal of Behavioral Nutrition and Physical Activity the validation of a home food inventory. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 55. [Google Scholar] [CrossRef] [Green Version]
- Thompson, F.E.; Midthune, D.; Kahle, L.; Dodd, K.W. Development and Evaluation of the National Cancer Institute’s Dietary Screener Questionnaire Scoring Algorithms. J. Nutr. 2017, 147, 1226–1233. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Surveillance of Fruit and Vegetable Intake Using the Behavioral Risk Factor Surveillance System. Available online: https://www.cdc.gov/brfss/pdf/fruits_vegetables.pdf (accessed on 29 January 2018).
- Sano, Y.; Routh, B.; Lanigan, J. Food parenting practices in rural poverty context. Appetite 2019, 135, 115–122. [Google Scholar] [CrossRef]
- Appleton, K.M.; Hemingway, A.; Saulais, L.; Dinnella, C.; Monteleone, E.; Depezay, L.; Morizet, D.; Perez-Cueto, F.J.A.; Bevan, A.; Hartwell, H. Increasing vegetable intakes: Rationale and systematic review of published interventions. Eur. J. Nutr. 2016, 55, 869–896. [Google Scholar] [CrossRef] [Green Version]
- Fischer, C.; Brug, J.; Tak, N.I.; Yngve, A.; te Velde, S.J. Differences in fruit and vegetable intake and their determinants among 11-year-old schoolchildren between 2003 and 2009. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 141. [Google Scholar] [CrossRef] [Green Version]
- Brug, J.; Tak, N.I.; te Velde, S.J.; Bere, E.; de Bourdeaudhuij, I. Taste preferences, liking and other factors related to fruit and vegetable intakes among schoolchildren: Results from observational studies. Br. J. Nutr. 2008, 99 (Suppl. S1), S7–S14. [Google Scholar] [CrossRef] [Green Version]
- Hendy, H.M.; Williams, K.E.; Camise, T.S.; Eckman, N.; Hedemann, A. The Parent Mealtime Action Scale (PMAS). Development and association with children’s diet and weight. Appetite 2009, 52, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L. Development of Food Preferences. Annu. Rev. Nutr. 1999, 19, 41–62. Available online: http://www.healthybeveragesinchildcare.org/Birch_1999_Development_of_food_preferences.pdf (accessed on 11 February 2018). [CrossRef] [PubMed] [Green Version]
- Ralston, J.; Brinsden, H.; Buse, K.; Candeias, V.; Caterson, I.; Hassell, T.; Kumanyika, S.; Nece, P.; Nishtar, S.; Patton, I.; et al. Time for a new obesity narrative. Lancet 2018, 392, 1384–1386. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O. Development of eating behaviors among children and adolescents. Pediatrics 1998, 101 (Suppl. S2), 539–549. Available online: http://www.ncbi.nlm.nih.gov/pubmed/12224660 (accessed on 7 January 2018).
- Dubois, L.; Girad, M. Accuracy of maternal reports of pre-schoolers’ weights and heights as estimates of BMI values. Int. J. Epi. 2007, 36, 132–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bland, J.M.; Altman, D.G. Statistical Notes: Cronbach’s Alpha. BMJ 1997, 314, 572. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Caregiver Age (±SD) | Child Age (±SD) |
| Mean Age in Years (±SD) | 35.6 ± 9.8 | 6.5 ± 2.7 |
| Caregiver % (n) | Child % (n) | |
| Female | 78 (138) | 54 (96) |
| Race | ||
| White | 97 (173) | 96 (171) |
| Not White a | 3 (5) | 4 (7) |
| Ethnicity, % not H/L b | 99 (176) | 98 (175) |
| Education | ||
| Less than HS c | 16 (28) | |
| HS c or GED | 53 (95) | |
| Some College | 20 (35) | |
| College Degree or higher | 11 (20) | |
| Marital Status | ||
| Never Married | 24 (43) | |
| Married | 47 (83) | |
| Separated | 8 (15) | |
| Divorced | 17 (31) | |
| Widowed | 3 (6) | |
| Income (in USD) d | ||
| $0–10,000 | 21 (38) | |
| $10,001–20,000 | 24 (43) | |
| $20,001–30,000 | 21 (37) | |
| $30,001–40,000 | 11 (19) | |
| $40,001–50,000 | 6 (11) | |
| $50,001–60,000 | 6 (11) | |
| $60,001+ | 7 (12) | |
| SNAP Participants e | 61 (109) | |
| WIC Participants f | 23 (41) | |
| Food Insecure Households | 59 (103) |
| Modeling (n = 178) | Mean (SD) |
| I try to eat healthy foods in front of my child, even if they are not my favorite a | 4.1 ± 0.94 |
| My child learns to eat healthy snacks from me a | 3.9 ± 0.93 |
| How often do you try not to eat unhealthy foods when your children are around? b | 3.2 ± 1.20 |
| How often do you drink soda (regular or diet) or other sweetened beverages at meals and snacks with your child? b,c | 2.6 ± 1.30 |
| I eat food I want my child to eat b | 4.2 ± 0.94 |
| Modeling Scale Total Score | 3.6 ± 0.63 |
| Home Food Availability Scores | Mean (SD) |
| Healthier Home Food Availability d (n = 174) | 20.3 ± 7.24 |
| Less Healthy Home Food Availability e (n = 178) | 10.1 ± 2.35 |
| Child Dietary Intake (n = 178) | Mean Score (SD) | Possible Range of Scores |
| Fruit a | 7.1 ± 1.78 | 0–8 (0 = never, 8 = 2+ times/day) |
| Vegetables b | 14.8 ± 4.70 | 0–24 (0 = never, 24 = 2+ times/day) |
| HS/HF snack foods c | 17.6 ± 6.33 | 0–32 (0 = never, 32 = 2+ times/day) |
| Caregiver Dietary Intake (n = 178) | Mean Times per Day (SD) | -- |
| Fruit d | 1.0 ± 1.09 | N/A |
| Vegetables e | 1.8 ± 1.16 | N/A |
| Variable (n = 174) | Beta | p-Value | 95% Confidence Interval |
|---|---|---|---|
| Modeling | 0.27 | 0.17 | −0.12 to 0.67 |
| Caregiver fruit consumption | 0.29 | 0.02 * | 0.04 to 0.54 |
| Healthier home food availability | 0.06 | 0.002 * | 0.02 to 0.09 |
| Child age b | −0.11 | 0.02 * | −0.21 to 0.02 |
| Child gender c | 0.25 | 0.32 | −0.25 to 0.76 |
| Household income d | −0.04 | 0.46 | −0.15 to 0.07 |
| Variable (n = 174) | Beta | p-Value | 95% Confidence Interval |
|---|---|---|---|
| Modeling | 1.02 | 0.04 * | 0.05 to 2.00 |
| Caregiver vegetable consumption | 1.56 | <0.001 * | 1.00 to 2.10 |
| Healthier home food availability | 0.09 | 0.05 * | 0.001 to 0.18 |
| Child age b | 0.03 | 0.79 | −0.20 to 0.27 |
| Child gender c | 1.50 | 0.02 * | 0.24 to 2.75 |
| Household income d | −0.13 | 0.36 | −0.39 to 0.14 |
| Variable (n = 178) | Beta | p-Value | 95% Confidence Interval |
|---|---|---|---|
| Modeling | −1.43 | 0.05 * | −2.85 to 0.00 |
| Less healthy home food availability | 0.59 | 0.003 * | 0.20 to 0.98 |
| Child age b | −0.02 | 0.90 | −0.37 to 0.32 |
| Child gender c | −1.12 | 0.23 | −3.00 to 0.75 |
| Household income d | −0.18 | 0.35 | −0.56 to 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McIver, M.B.; Colby, S.; Hansen-Petrik, M.; Anderson Steeves, E.T. Caregiver Feeding Practices as Predictors for Child Dietary Intake in Low-Income, Appalachian Communities. Nutrients 2021, 13, 2773. https://doi.org/10.3390/nu13082773
McIver MB, Colby S, Hansen-Petrik M, Anderson Steeves ET. Caregiver Feeding Practices as Predictors for Child Dietary Intake in Low-Income, Appalachian Communities. Nutrients. 2021; 13(8):2773. https://doi.org/10.3390/nu13082773
Chicago/Turabian StyleMcIver, Mikaela B., Sarah Colby, Melissa Hansen-Petrik, and Elizabeth T. Anderson Steeves. 2021. "Caregiver Feeding Practices as Predictors for Child Dietary Intake in Low-Income, Appalachian Communities" Nutrients 13, no. 8: 2773. https://doi.org/10.3390/nu13082773
APA StyleMcIver, M. B., Colby, S., Hansen-Petrik, M., & Anderson Steeves, E. T. (2021). Caregiver Feeding Practices as Predictors for Child Dietary Intake in Low-Income, Appalachian Communities. Nutrients, 13(8), 2773. https://doi.org/10.3390/nu13082773