
US Consumer Identification of the Health Benefits of Dietary Fiber and Consideration of Fiber When Making Food Choices


Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey
2.2. Measures
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Questions Asked to Participants in the IRi Survey
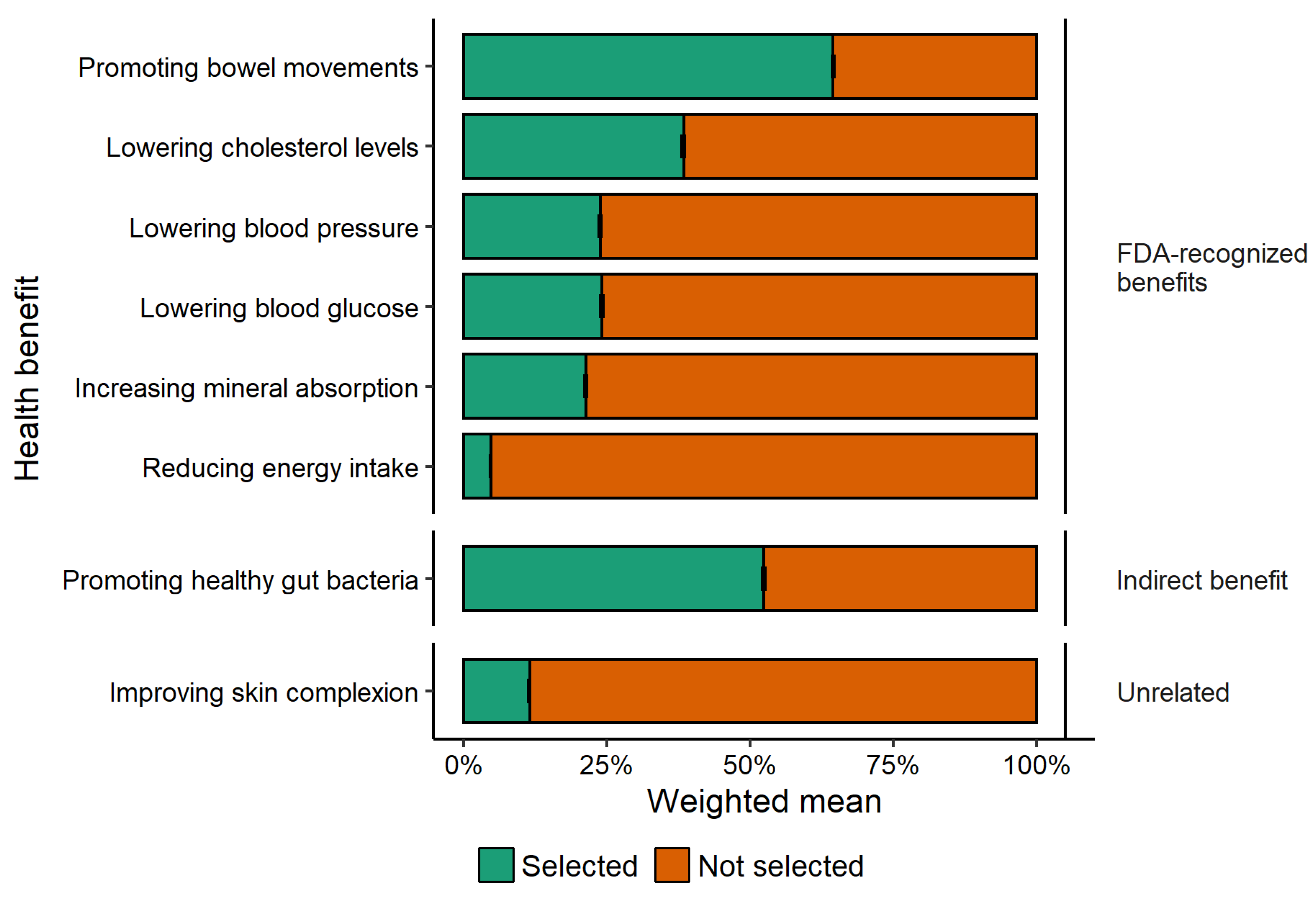
- Which of the following, if any, do you believe are health benefits that result from consuming dietary fiber? (Select all that apply)
- Lowering blood glucose
- Lowering cholesterol levels
- Lowering blood pressure
- Increasing frequency of bowel movements
- Increasing mineral absorption in the intestinal tract
- Reducing energy intake
- Maintaining healthy gut bacteria
- Improving skin complexion
- Which of the following nutrients, if any, do you consider when you are choosing what foods to buy or eat (or have you considered in the past when establishing dietary patterns that you currently follow)? (Select all that apply)
- Potassium
- Calcium
- Dietary fiber
- Vitamin D
- Calories
- Saturated fat
- Sodium
- Added sugar
References
- Murphy, S.L.; Kochanek, K.D.; Xu, J.; Arias, E. Mortality in the United States, 2020. NCHS Data Brief 2021, 1–8. [Google Scholar]
- US Burden of Disease Collaborators. The State of US Health, 1990–2016: Burden of Diseases, Injuries, and Risk Factors Among US States. JAMA 2018, 319, 1444–1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jardim, T.V.; Mozaffarian, D.; Abrahams-Gessel, S.; Sy, S.; Lee, Y.; Liu, J.; Huang, Y.; Rehm, C.; Wilde, P.; Micha, R.; et al. Cardiometabolic Disease Costs Associated with Suboptimal Diet in the United States: A Cost Analysis Based on a Microsimulation Model. PLoS Med. 2019, 16, e1002981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elbel, B.; Kersh, R.; Brescoll, V.L.; Dixon, L.B. Calorie Labeling And Food Choices: A First Look At The Effects On Low-Income People In New York City: Calorie Information on Menus Appears to Increase Awareness of Calorie Content, but Not Necessarily the Number of Calories People Purchase. Health Aff. 2009, 28, w1110–w1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petimar, J.; Moran, A.J.; Ramirez, M.; Block, J.P. A Natural Experiment to Evaluate the Nutritional Content of Restaurant Meal Purchases After Calorie Labeling. J. Acad. Nutr. Diet. 2020, 120, P2039–P2046. [Google Scholar] [CrossRef] [PubMed]
- Variyam, J.N. Do Nutrition Labels Improve Dietary Outcomes? Health Econ. 2008, 17, 695–708. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025; USDA: Washington, DC, USA, 2020; 395p.
- Post, R.E.; Mainous, A.G., 3rd; King, D.E.; Simpson, K.N. Dietary Fiber for the Treatment of Type 2 Diabetes Mellitus: A Meta-Analysis. J. Am. Board Fam. Med. 2012, 25, 16–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Qian, Y.; Pan, Y.; Li, P.; Yang, J.; Ye, X.; Xu, G. Association between Dietary Fiber Intake and Risk of Coronary Heart Disease: A Meta-Analysis. Clin. Nutr. 2015, 34, 603–611. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; The National Academies Press: Washington, DC, USA, 2005.
- Food and Drug Administration. Food Labeling: Revision of the Nutrition and Supplement Facts Labels. Fed. Regist. 2016, 81, 33741–33999. [Google Scholar]
- USDA; DHHS. Dietary Guidelines for Americans: Nutrition and Your Health; USDA: Washington, DC, USA, 1980.
- USDA. Agricultural Research Service Usual Nutrient Intake from Food and Beverages, by Gender and Age. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/wweianhanes-overview/ (accessed on 3 February 2022).
- Barrett, E.M.; Foster, S.I.; Beck, E.J. Whole Grain and High-Fibre Grain Foods: How Do Knowledge, Perceptions and Attitudes Affect Food Choice? Appetite 2020, 149, 104630. [Google Scholar] [CrossRef]
- Wardle, J.; Parmenter, K.; Waller, J. Nutrition Knowledge and Food Intake. Appetite 2000, 34, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Makki, K.; Deehan, E.C.; Walter, J.; Bäckhed, F. The Impact of Dietary Fiber on Gut Microbiota in Host Health and Disease. Cell Host Microbe 2018, 23, 705–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonnenburg, E.D.; Sonnenburg, J.L. Starving Our Microbial Self: The Deleterious Consequences of a Diet Deficient in Microbiota-Accessible Carbohydrates. Cell Metab. 2014, 20, 779–786. [Google Scholar] [CrossRef] [Green Version]
- Robertson, R. 9 Ways to Improve Your Gut Bacteria, Based on Science. Available online: https://www.healthline.com/nutrition/improve-gut-bacteria (accessed on 27 May 2022).
- Sonnenburg, J.; Sonnenburg, E. The Good Gut: Taking Control of Your Weight, Your Mood, and Your Long-Term Health; Penguin Publishing Group: New York, NY, USA, 2016; ISBN 9780143108085. [Google Scholar]
- James, S.D. Can You Change Your Gut Bacteria? Available online: https://www.webmd.com/digestive-disorders/news/20170531/can-you-change-your-gut-bacteria (accessed on 11 February 2022).
- How Your Gut Health Affects Your Whole Body. Available online: https://www.webmd.com/digestive-disorders/ss/slideshow-how-gut-health-affects-whole-body (accessed on 27 May 2022).
- Kellman, R. The Microbiome Diet: The Scientifically Proven Way to Restore Your Gut Health and Achieve Permanent Weight Loss; Da Capo Press: Boston, MA, USA, 2014; ISBN 9780738217659. [Google Scholar]
- Knight, R.; Buhler, B. Follow Your Gut: The Enormous Impact of Tiny Microbes; Simon and Schuster: New York, NY, USA, 2015; ISBN 9781476784748. [Google Scholar]
- Sonnenburg, J.; Sonnenburg, E. Gut Reactions: How Healthy Insides Can Improve Your Weight, Mood and Well-Being; Penguin Random House: New York, NY, USA, 2017. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; Citeseer: online publisher, 2021. [Google Scholar]
- Allaire, J. RStudio: Integrated Development Environment for R; Citeseer: Boston, MA, USA, 2012; Volume 770, pp. 165–171. Available online: https://www.r-project.org/conferences/useR-2011/abstracts/180111-allairejj.pdf (accessed on 14 January 2022).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: Berlin, Germany, 2016; ISBN 9783319242774. [Google Scholar]
- Wilke, C.O.; Wickham, H.; Wilke, M.C.O. Package ‘Cowplot’. Streamlined Plot Theme and Plot Annotations for ‘ggplot2’. 2019. Available online: https://mirror.lyrahosting.com/CRAN/web/packages/cowplot/cowplot.pdf (accessed on 6 March 2022).
- Ripley, B.; Venables, W.; Ripley, M.B. Package ‘Nnet.’ 2015. Available online: https://cran.microsoft.com/web/packages/nnet/nnet.pdf (accessed on 17 January 2022).
- Ripley, B.; Venables, B.; Bates, D.M.; Hornik, K.; Gebhardt, A.; Firth, D.; Ripley, M.B. Package ‘Mass’. Cran R 2013, 538, 113–120. [Google Scholar]
- Tighe, D. Grocery Shopping Responsibility Share in the United States by Gender 2018. 2020. Available online: https://www.statista.com/statistics/817500/grocery-shopping-responsibility-share-us-by-gender/ (accessed on 5 May 2022).
- Among, U.S. Couples, Women Do More Cooking and Grocery Shopping than Men. Available online: https://www.pewresearch.org/fact-tank/2019/09/24/among-u-s-couples-women-do-more-cooking-and-grocery-shopping-than-men/ (accessed on 5 May 2022).
- Mitova, T. 21+ Grocery Shopping Statistics for Every CUSTOMER in 2021. Available online: https://spendmenot.com/blog/grocery-shopping-statistics/ (accessed on 5 May 2022).
- Buckton, C.H.; Lean, M.E.J.; Combet, E. ’Language Is the Source of Misunderstandings’—Impact of Terminology on Public Perceptions of Health Promotion Messages. BMC Public Health 2015, 15, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, G.M.; Danaei, G.; Pelizzari, P.M.; Lin, J.K.; Cowan, M.J.; Stevens, G.A.; Farzadfar, F.; Khang, Y.-H.; Lu, Y.; Riley, L.M.; et al. The Age Associations of Blood Pressure, Cholesterol, and Glucose: Analysis of Health Examination Surveys from International Populations. Circulation 2012, 125, 2204–2211. [Google Scholar] [CrossRef]
- Lambert, M.; Chivers, P.; Farringdon, F. In Their Own Words: A Qualitative Study Exploring Influences on the Food Choices of University Students. Health Promot. J. Austr. 2019, 30, 66–75. [Google Scholar] [CrossRef] [Green Version]
- Zagorsky, J.L.; Smith, P.K. The Association between Socioeconomic Status and Adult Fast-Food Consumption in the U.S. Econ. Hum. Biol. 2017, 27, 12–25. [Google Scholar] [CrossRef]
- Kasi, P.M.; Shahjehan, F.; Cochuyt, J.J.; Li, Z.; Colibaseanu, D.T.; Merchea, A. Rising Proportion of Young Individuals with Rectal and Colon Cancer. Clin. Colorectal Cancer 2019, 18, e87–e95. [Google Scholar] [CrossRef] [Green Version]
- Dahm, C.C.; Keogh, R.H.; Spencer, E.A.; Greenwood, D.C.; Key, T.J.; Fentiman, I.S.; Shipley, M.J.; Brunner, E.J.; Cade, J.E.; Burley, V.J.; et al. Dietary Fiber and Colorectal Cancer Risk: A Nested Case-Control Study Using Food Diaries. J. Natl. Cancer Inst. 2010, 102, 614–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seninde, D.R.; Chambers, E., IV. A Comparison of the Percentage of “Yes” (Agree) Responses and Importance of Attributes (Constructs) Determined Using Check-All-That-Apply and Check-All-Statements (Yes/No) Question Formats in Five Countries. Foods 2020, 9, 1566. [Google Scholar] [CrossRef] [PubMed]
- Jaeger, S.R.; Beresford, M.K.; Paisley, A.G.; Antúnez, L.; Vidal, L.; Cadena, R.S.; Giménez, A.; Ares, G. Check-All-That-Apply (CATA) Questions for Sensory Product Characterization by Consumers: Investigations into the Number of Terms Used in CATA Questions. Food Qual. Prefer. 2015, 42, 154–164. [Google Scholar] [CrossRef]
- Geaney, F.; Fitzgerald, S.; Harrington, J.M.; Kelly, C.; Greiner, B.A.; Perry, I.J. Nutrition Knowledge, Diet Quality and Hypertension in a Working Population. Prev. Med. Rep. 2015, 2, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Cavaliere, A.; De Marchi, E.; Banterle, A. Investigation on the Role of Consumer Health Orientation in the Use of Food Labels. Public Health 2017, 147, 119–127. [Google Scholar] [CrossRef]
- Naughton, P.; McCarthy, S.N.; McCarthy, M.B. The Creation of a Healthy Eating Motivation Score and Its Association with Food Choice and Physical Activity in a Cross Sectional Sample of Irish Adults. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 74. [Google Scholar] [CrossRef] [Green Version]
- Arslain, K.; Gustafson, C.R.; Rose, D.J. Point-of-Decision Prompts Increase Dietary Fiber Content of Consumers’ Food Choices in an Online Grocery Shopping Simulation. Nutrients 2020, 12(11), 3487. [Google Scholar] [CrossRef]
- Arslain, K.; Gustafson, C.R.; Rose, D.J. The Effect of Health Prompts on Product Consideration, Attention to Information, and Choice in Large, Online Product Assortments: The Case of Fiber. Food Qual. Prefer. 2021, 94, 104329. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Category | Percentage (n) |
|---|---|
| Gender | |
| Female | 79.9% (33,582) |
| Male | 19.9% (8362) |
| Other | 0.2% (74) |
| Age | |
| 19–24 year | 0.9% (393) |
| 25–34 year | 8.6% (3601) |
| 35–44 year | 16.1% (6777) |
| 45–54 year | 18.1% (7621) |
| 55–64 year | 25.5% (10,719) |
| 65y and above | 30.7% (12,907) |
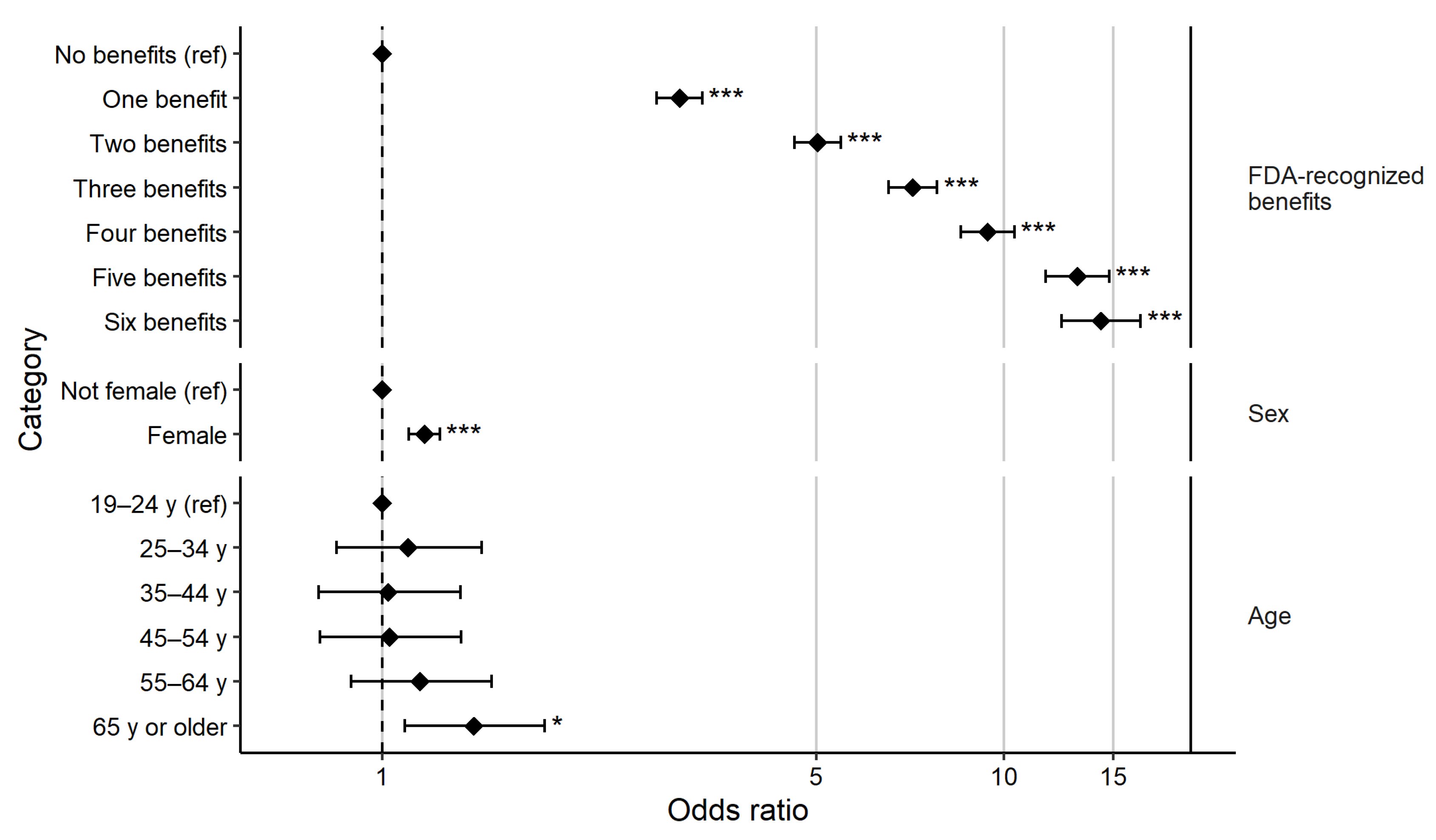
| Category | Prop. OR (95% CI) a |
|---|---|
| FEMALE (Ref.: Not female) | 1.178 (1.128, 1.230) |
| AGE (Ref.: 19–24 years) | |
| 25–34 years | 1.429 (1.183, 1.728) |
| 35–44 years | 1.668 (1.387, 2.008) |
| 45–54 years | 2.173 (1.808, 2.614) |
| 55–64 years | 2.508 (2.089, 3.014) |
| 65 years and above | 2.405 (2.005, 2.890) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gustafson, C.R.; Rose, D.J. US Consumer Identification of the Health Benefits of Dietary Fiber and Consideration of Fiber When Making Food Choices. Nutrients 2022, 14, 2341. https://doi.org/10.3390/nu14112341
Gustafson CR, Rose DJ. US Consumer Identification of the Health Benefits of Dietary Fiber and Consideration of Fiber When Making Food Choices. Nutrients. 2022; 14(11):2341. https://doi.org/10.3390/nu14112341
Chicago/Turabian StyleGustafson, Christopher R., and Devin J. Rose. 2022. "US Consumer Identification of the Health Benefits of Dietary Fiber and Consideration of Fiber When Making Food Choices" Nutrients 14, no. 11: 2341. https://doi.org/10.3390/nu14112341
APA StyleGustafson, C. R., & Rose, D. J. (2022). US Consumer Identification of the Health Benefits of Dietary Fiber and Consideration of Fiber When Making Food Choices. Nutrients, 14(11), 2341. https://doi.org/10.3390/nu14112341