
The Association between Dietary Patterns and Pre-Pregnancy BMI with Gestational Weight Gain: The “Born in Shenyang” Cohort

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Exposures: Maternal Diet
2.3. Outcomes: Gestational Weight Gain
2.4. Covariates
2.5. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Dietary Patterns
3.3. Dietary Patterns and Risk of EGWG
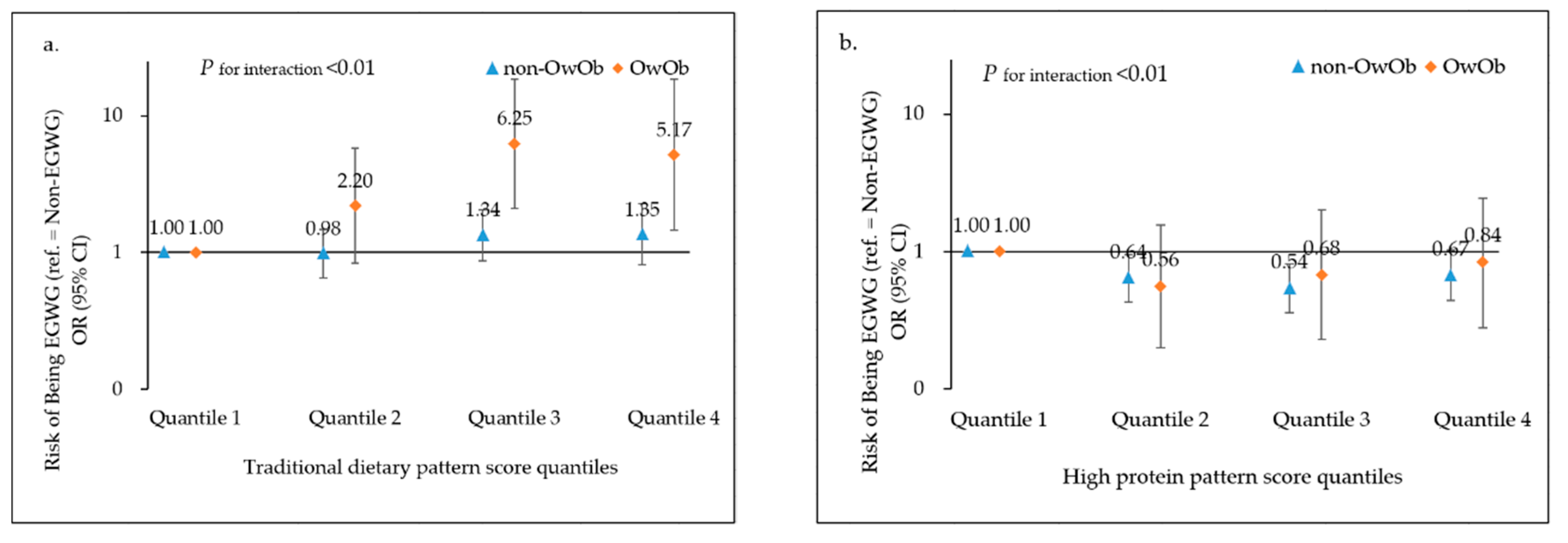
3.4. Dietary Patterns in Relation to EGWG, Stratified by Pre-Pregnancy Weight Status
3.5. Dietary Patterns in Relation to GWG Rate
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Santos, S.; Voerman, E.; Amiano, P.; Barros, H.; Beilin, L.J.; Bergstrom, A.; Charles, M.A.; Chatzi, L.; Chevrier, C.; Chrousos, G.P.; et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: An individual participant data meta-analysis of European, North American and Australian cohorts. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 984–995. [Google Scholar] [CrossRef]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of Gestational Weight Gain With Maternal and Infant Outcomes A Systematic Review and Meta-analysis. JAMA J. Am. Med. Assoc. 2017, 317, 2207–2225. [Google Scholar] [CrossRef] [PubMed]
- Mamun, A.A.; Mannan, M.; Doi, S.A.R. Gestational weight gain in relation to offspring obesity over the life course: A systematic review and bias- adjusted meta- analysis. Obes. Rev. 2014, 15, 338–347. [Google Scholar] [CrossRef]
- Xiao, L.L.; Ding, G.D.; Vinturache, A.; Xu, J.; Ding, Y.F.; Guo, J.L.; Huang, L.P.; Yin, X.L.; Qiao, J.; Thureraja, I.; et al. Associations of maternal pre-pregnancy body mass index and gestational weight gain with birth outcomes in Shanghai, China. Sci. Rep. 2017, 7, 41073. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Cheng, H.; Wang, C. The effect of pre-pregnancy body mass index, gestational weight gain in pregnancy process and outcome. Curr. Adv. Obstet. Gynecol. 2017, 26, 756–759. [Google Scholar]
- Hu, Y.; Wu, Q.; Han, L.Y.; Zou, Y.Q.; Hong, D.; Liu, J.; Zhu, Y.Y.; Zhu, Q.M.; Chen, D.Q.; Qi, L.; et al. Association between maternal gestational weight gain and preterm birth according to body mass index and maternal age in Quzhou, China. Sci. Rep. 2020, 10, 15863. [Google Scholar] [CrossRef] [PubMed]
- Itani, L.; Radwan, H.; Hashim, M.; Hasan, H.; Obaid, R.S.; Al Ghazal, H.; Al Hilali, M.; Rayess, R.; Mohamed, H.J.J.; Hamadeh, R.; et al. Dietary patterns and their associations with gestational weight gain in the United Arab Emirates: Results from the MISC cohort. Nutr. J. 2020, 19, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Augustin, H.; Winkvist, A.; Barebring, L. Poor Dietary Quality Is Associated with Low Adherence to Gestational Weight Gain Recommendations among Women in Sweden. Nutrients 2020, 12, 317. [Google Scholar] [CrossRef] [Green Version]
- Shin, D.; Lee, K.W.; Song, W.O. Dietary Patterns During Pregnancy are Associated with Gestational Weight Gain. Matern. Child Health J. 2016, 20, 2527–2538. [Google Scholar] [CrossRef]
- Pathirathna, M.L.; Sekijima, K.; Sadakata, M.; Fujiwara, N.; Muramatsu, Y.; Wimalasiri, K.M.S. Impact of Second Trimester Maternal Dietary Intake on Gestational Weight Gain and Neonatal Birth Weight. Nutrients 2017, 9, 627. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.X.; Wang, M.L.; Tobias, D.K.; Rich-Edwards, J.W.; Darling, A.M.; Abioye, A.I.; Noor, R.A.; Madzorera, I.; Fawzi, W.W. Dietary diversity and diet quality with gestational weight gain and adverse birth outcomes, results from a prospective pregnancy cohort study in urban Tanzania. Matern. Child Nutr. 2022, 18, e13300. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, A.; Barchitta, M.; Favara, G.; La Rosa, M.C.; La Mastra, C.; San Lio, R.M.; Agodi, A. Maternal Dietary Patterns Are Associated with Pre-Pregnancy Body Mass Index and Gestational Weight Gain: Results from the “Mamma & Bambino” Cohort. Nutrients 2019, 11, 1308. [Google Scholar]
- Cano-Ibanez, N.; Martinez-Galiano, J.M.; Luque-Fernandez, M.A.; Martin-Pelaez, S.; Bueno-Cavanillas, A.; Delgado-Rodriguez, M. Maternal Dietary Patterns during Pregnancy and Their Association with Gestational Weight Gain and Nutrient Adequacy. Int. J. Environ. Res. Public Health 2020, 17, 7908. [Google Scholar] [CrossRef]
- Wrottesley, S.V.; Pisa, P.T.; Norris, S.A. The Influence of Maternal Dietary Patterns on Body Mass Index and Gestational Weight Gain in Urban Black South African Women. Nutrients 2017, 9, 732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angali, K.A.; Shahri, P.; Borazjani, F. Maternal dietary pattern in early pregnancy is associated with gestational weight gain and hyperglycemia: A cohort study in South West of Iran. Diabetes Metab. Syndr. 2020, 14, 1711–1717. [Google Scholar] [CrossRef] [PubMed]
- Han, A.X.; Sun, T.H.; Ming, J.; Chai, L.; Liao, X.W. Are the Chinese Moving toward a Healthy Diet? Evidence from Macro Data from 1961 to 2017. Int. J. Environ. Res. Public Health 2020, 17, 5294. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.L.; Powles, J.; Mozaffarian, D.; Global Burden Dis Nutr Chronic, D. Dietary quality among men and women in 187 countries in 1990 and 2010: A systematic assessment. Lancet Glob. Health 2015, 3, E132–E142. [Google Scholar] [CrossRef] [Green Version]
- Wei, X.L.; He, J.R.; Lin, Y.; Lu, M.S.; Zhou, Q.L.; Li, S.H.; Lu, J.H.; Yuan, M.Y.; Chen, N.N.; Zhang, L.F.; et al. The influence of maternal dietary patterns on gestational weight gain: A large prospective cohort study in China. Nutrition 2019, 59, 90–95. [Google Scholar] [CrossRef]
- Li, Y.; Zhou, X.; Zhang, Y.; Zhong, C.; Huang, L.; Chen, X.; Chen, R.; Wu, J.; Li, Q.; Sun, G.; et al. Association of Maternal Dietary Patterns With Birth Weight and the Mediation of Gestational Weight Gain: A Prospective Birth Cohort. Front. Nutr. 2021, 8, 782011. [Google Scholar] [CrossRef]
- Dubois, L.; Diasparra, M.; Bedard, B.; Colapinto, C.K.; Fontaine-Bisson, B.; Tremblay, R.E.; Fraser, W.D. Adequacy of nutritional intake during pregnancy in relation to prepregnancy BMI: Results from the 3D Cohort Study. Br. J. Nutr. 2018, 120, 335–344. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.J.; Aris, I.M.; Oken, E.; Ma, Y.N.; Ding, N.; Gao, M.; Wei, X.T.; Wen, D.L. Association of Total and Trimester-Specific Gestational Weight Gain Rate with Early Infancy Weight Status: A Prospective Birth Cohort Study in China. Nutrients 2019, 11, 280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute of Nutrition and Food Safety; China Centers for Disease Control. China Food Composition, 2nd ed.; Peking University Medical Press: Beijing, China, 2009; pp. 1–452. [Google Scholar]
- Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines. Weight Gain During Pregnancy: Reexamining the Guidelines; National Academies Press (US): Washington, DC, USA, 2009; p. S-2. [Google Scholar]
- WHO. Physical Status: The Use and Interpretation of Anthropometry. Report of a WHO Expert Committee; WHO: Geneva, Switzerland, 1995; pp. 1–452.
- Xiang, M.; Konishi, M.; Hu, H.H.; Takahashi, M.; Fan, W.B.; Nishimaki, M.; Ando, K.; Kim, H.K.; Tabata, H.; Arao, T.; et al. Reliability and Validity of a Chinese-Translated Version of a Pregnancy Physical Activity Questionnaire. Matern. Child Health J. 2016, 20, 1940–1947. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.S.; Lay, S.; Yu, H.N.; Shen, S.R. Dietary Guidelines for Chinese Residents (2016): Comments and comparisons. J. Zhejiang Univ. Sci. B 2016, 17, 649–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.H.; Xia, Y.; Chang, Q.; Gao, S.Y.; Zhao, Y.H. Dietary patterns and associations between air pollution and gestational diabetes mellitus. Environ. Int. 2021, 147, 106347. [Google Scholar]
- Suliga, E.; Rokita, W.; Adamczyk-Gruszka, O.; Pazera, G.; Ciesla, E.; Gluszek, S. Factors associated with gestational weight gain: A cross-sectional survey. BMC Pregnancy Childbirth 2018, 18, 465. [Google Scholar] [CrossRef]
- Knudsen, V.K.; Heitmann, B.L.; Halldorsson, T.I.; Sorensen, T.I.A.; Olsen, S.F. Maternal dietary glycaemic load during pregnancy and gestational weight gain, birth weight and postpartum weight retention: A study within the Danish National Birth Cohort. Br. J. Nutr. 2013, 109, 1471–1478. [Google Scholar] [CrossRef] [Green Version]
- Tielemans, M.J.; Garcia, A.H.; Santos, A.P.; Bramer, W.M.; Luksa, N.; Luvizotto, M.J.; Moreira, E.; Topi, G.; de Jonge, E.A.L.; Visser, T.L.; et al. Macronutrient composition and gestational weight gain: A systematic review. Am. J. Clin. Nutr. 2016, 103, 83–99. [Google Scholar] [CrossRef] [Green Version]
- Mikkelsen, P.B.; Toubro, S.; Astrup, A. Effect of fat-reduced diets on 24-h energy expenditure: Comparisons between animal protein, vegetable protein, and carbohydrate. Am. J. Clin. Nutr. 2000, 72, 1135–1141. [Google Scholar] [CrossRef] [Green Version]
- Maslova, E.; Halldorsson, T.I.; Astrup, A.; Olsen, S.F. Dietary protein-to-carbohydrate ratio and added sugar as determinants of excessive gestational weight gain: A prospective cohort study. BMJ Open 2015, 5, e005839. [Google Scholar] [CrossRef] [Green Version]
- Jones, S.; Luo, S.; Dorton, H.M.; Yunker, A.G.; Angelo, B.; Defendis, A.; Monterosso, J.R.; Page, K.A. Obesity and Dietary Added Sugar Interact to Affect Postprandial GLP-1 and Its Relationship to Striatal Responses to Food Cues and Feeding Behavior. Front. Endocrinol. 2021, 12, 638504. [Google Scholar] [CrossRef]
- Cakir, M.; Sari, R.; Tosun, O.; Karayalcin, U. Cortisol levels during an oral glucose tolerance test in lean and obese women. Endocr. Res. 2005, 31, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Crozier, S.R.; Robinson, S.M.; Godfrey, K.M.; Cooper, C.; Inskip, H.M. Women’s Dietary Patterns Change Little from Before to During Pregnancy. J. Nutr. 2009, 139, 1956–1963. [Google Scholar] [CrossRef] [PubMed]
- Cuco, G.; Fernandez-Ballart, J.; Sala, J.; Viladrich, C.; Iranzo, R.; Vila, J.; Arija, V. Dietary patterns and associated lifestyles in preconception, pregnancy and postpartum. Eur. J. Clin. Nutr. 2006, 60, 364–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Gestational Weight Gain Status, n (%) | ||
|---|---|---|---|
| Non-EGWG | EGWG | p Value | |
| Age at enrollments (years) | 0.26 | ||
| <25 | 27 (5.5) | 33 (6.1) | |
| 25−29 | 220 (45.2) | 230 (42.7) | |
| 30−34 | 157 (32.2) | 201 (37.3) | |
| ≥35 | 83 (17.0) | 75 (13.9) | |
| Ethnicity | 0.04 | ||
| Han | 418 (85.8) | 437 (81.1) | |
| Minority | 69 (14.2) | 102 (18.9) | |
| Educational attainment | <0.01 | ||
| High school or below | 93 (19.1) | 148 (27.5) | |
| College or above | 394 (80.9) | 391 (72.5) | |
| Household income per year, CNY | 0.37 | ||
| <50,000 | 251 (51.5) | 293 (54.4) | |
| ≥50,000 | 236 (48.5) | 246 (45.6) | |
| Parity | 0.27 | ||
| Primipara | 370 (76.0) | 425 (78.9) | |
| Multipara | 117 (24.0) | 114 (21.2) | |
| Pre-pregnancy BMI category, kg/m2 | <0.01 | ||
| <18.5 | 86 (17.7) | 48 (8.9) | |
| 18.5–<25.0 | 339 (69.6) | 361 (67.0) | |
| ≥25.0 | 62 (12.7) | 130 (24.1) | |
| Smoking during or before pregnancy | 0.49 | ||
| No | 485 (99.6) | 535 (99.3) | |
| Yes | 2 (0.4) | 4 (0.7) | |
| Physical activity status during pregnancy, MET-hour/week | 0.94 | ||
| <100 | 125 (25.8) | 141 (26.2) | |
| 100−200 | 263 (54.0) | 293 (54.4) | |
| >200 | 99 (20.3) | 105 (19.5) | |
| Energy intake, kcal/day | 0.15 | ||
| <2100 | 305 (62.6) | 314 (58.2) | |
| ≥2100 | 182 (37.4) | 225 (41.7) | |
| Dietary Patterns | Food | Factor Loading Coefficient | Variance Explained (%) |
|---|---|---|---|
| Traditional pattern | 8.68 | ||
| Tubers | 0.67 | ||
| Vegetables | 0.61 | ||
| Fruits | 0.55 | ||
| Red meat | 0.54 | ||
| Rice | 0.42 | ||
| Sweet foods pattern | 6.39 | ||
| Sweet beverages | 0.73 | ||
| Pastry and candy | 0.65 | ||
| Shrimps, crabs and mussels | 0.42 | ||
| Fruits | 0.24 | ||
| High protein pattern | 6.14 | ||
| Fried foods | 0.73 | ||
| Beans and bean products | 0.69 | ||
| Dairy products | 0.32 | ||
| Fruits | 0.21 | ||
| Milk-nut--seafood pattern | 5.85 | ||
| Milk | 0.68 | ||
| Nuts | 0.49 | ||
| Shrimps, crabs and mussels | 0.39 | ||
| Fruits | 0.27 | ||
| Dairy products | 0.24 | ||
| Eggs and egg products | 0.22 | ||
| Pastry and candy | 0.20 | ||
| Sweet beverages | −0.24 |
| Characteristics | Dietary Pattern Scores, Mean (SD) | |||
|---|---|---|---|---|
| Traditional Pattern | Sweet Foods Pattern | High Protein Pattern | Milk-Nut-Sea Food Pattern | |
| Age, years | ||||
| <25 | 0.53 (1.89) | 0.27 (1.67) | 0.00 (1.80) | −0.32 (1.05) |
| 25−29 | 0.07 (1.89) | 0.01 (1.39) | 0.00 (1.26) | 0.06 (1.28) |
| 30−34 | −0.17 (1.74) | −0.01 (1.22) | 0.04 (1.29) | −0.06 (1.18) |
| ≥35 | −0.01 (2.10) | −0.12 (1.38) | −0.09 (1.25) | 0.09 (1.35) |
| P | 0.040 | 0.298 | 0.756 | 0.092 |
| Ethnicity | ||||
| Han | −0.01 (1.87) | 0.00 (1.35) | 0.02 (1.34) | 0.02 (1.27) |
| Minority | 0.07 (1.91) | 0.01 (1.34) | −0.11 (1.11) | −0.09 (1.13) |
| P | 0.598 | 0.944 | 0.208 | 0.312 |
| Educational attainment | ||||
| High school or below | 0.29 (1.92) | −0.14 (1.24) | −0.11 (1.21) | −0.06 (1.16) |
| College or above | −0.09 (1.86) | 0.04 (1.38) | 0.04 (1.33) | 0.02 (1.27) |
| P | 0.006 | 0.062 | 0.119 | 0.417 |
| Household income per year, CNY | ||||
| <50,000 | 0.08 (1.92) | −0.08 (1.21) | −0.06 (1.28) | −0.07 (1.19) |
| ≥50,000 | −0.09 (1.83) | 0.09 (1.49) | 0.06 (1.33) | 0.08 (1.30) |
| P | 0.151 | 0.041 | 0.149 | 0.068 |
| Parity | ||||
| 0 | 0.00 (1.86) | 0.02 (1.40) | 0.02 (1.32) | 0.03 (1.28) |
| ≥1 | −0.02 (1.95) | −0.08 (1.17) | −0.06 (1.25) | −0.12 (1.12) |
| P | 0.887 | 0.328 | 0.404 | 0.104 |
| Smoking status during pregnancy | ||||
| Yes | −0.75 (2.05) | 0.03 (1.96) | −0.43 (1.04) | −0.41 (0.75) |
| No | 0.00 (1.88) | −0.00 (1.35) | 0.00 (1.30) | 0.00 (1.25) |
| P | 0.327 | 0.950 | 0.417 | 0.415 |
| Pre-pregnancy BMI category, kg/m2 | ||||
| <18.5 | 0.00 (1.87) | −0.02 (1.17) | −0.05 (1.27) | −0.06 (1.27) |
| 18.5 to <25.0 | 0.02 (1.88) | 0.01 (1.42) | −0.01 (1.31) | 0.02 (1.24) |
| ≥25.0 | −0.08 (1.88) | −0.02 (1.22) | 0.07 (1.30) | −0.05 (1.26) |
| P | 0.778 | 0.944 | 0.669 | 0.674 |
| Physical Activity, MET-hour/week | ||||
| <100 | −0.02 (1.89) | 0.12 (1.70) | −0.01 (1.43) | −0.10 (1.38) |
| 100 to <200 | 0.02 (1.82) | −0.06 (1.13) | 0.05 (1.27) | 0.07 (1.20) |
| ≥200 | −0.02 (2.02) | 0.00 (1.38) | −0.13 (1.21) | −0.07 (1.19) |
| P | 0.944 | 0.205 | 0.218 | 0.129 |
| Energy intake, kcal/day | ||||
| <2100 | −0.86 (1.23) | −0.16 (1.10) | −0.25 (1.11) | −0.24 (1.07) |
| ≥2100 | 1.30 (1.94) | 0.24 (1.63) | 0.39 (1.47) | 0.37 (1.41) |
| P | <0.001 | <0.001 | <0.001 | <0.001 |
| Dietary Patterns | Risk of Being EGWG (ref. = Non-EGWG, n = 1026) | ||||
|---|---|---|---|---|---|
| Q1 Reference | Q2 OR (95%CI) | Q3 OR (95%CI) | Q4 OR (95%CI) | Pfor trend | |
| Traditional pattern | |||||
| Model 1 | 1.00 | 0.98 (0.69, 1.38) | 1.53 (1.08, 2.16) | 1.52 (1.07, 2.15) | <0.01 |
| Model 2 | 1.00 | 1.02 (0.71, 1.45) | 1.62 (1.13, 2.31) | 1.56 (1.08, 2.23) | <0.01 |
| Model 3 | 1.00 | 1.06 (0.74, 1.53) | 1.62 (1.10, 2.38) | 1.57 (0.99, 2.50) | 0.03 |
| Sweet foods pattern | |||||
| Model 1 | 1.00 | 0.70 (0.50, 1.00) | 0.95 (0.67, 1.34) | 0.85 (0.60, 1.21) | 0.81 |
| Model 2 | 1.00 | 0.72 (0.50, 1.02) | 1.04 (0.73, 1.50) | 0.92 (0.64, 1.32) | 1.00 |
| Model 3 | 1.00 | 0.70 (0.49, 0.99) | 1.05 (0.73, 1.51) | 0.95 (0.66, 1.37) | 0.86 |
| High protein pattern | |||||
| Model 1 | 1.00 | 0.70 (0.49, 0.99) | 0.61 (0.43, 0.86) | 0.78 (0.55, 1.10) | 0.23 |
| Model 2 | 1.00 | 0.70 (0.49, 0.99) | 0.57 (0.40, 0.82) | 0.69 (0.48, 1.00) | 0.12 |
| Model 3 | 1.00 | 0.68 (0.47, 0.97) | 0.56 (0.39, 0.81) | 0.71 (0.48, 1.03) | 0.16 |
| Milk–nut–seafood pattern | |||||
| Model 1 | 1.00 | 0.85 (0.60, 1.20) | 0.96 (0.68, 1.36) | 1.08 (0.76, 1.53) | 0.48 |
| Model 2 | 1.00 | 0.84 (0.59, 1.20) | 0.96 (0.68, 1.37) | 1.01 (0.71, 1.46) | 0.68 |
| Model 3 | 1.00 | 0.85 (0.59, 1.22) | 0.95 (0.66, 1.38) | 1.05 (0.71, 1.54) | 0.90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, J.; Gao, M.; Ma, Y.; Wan, N.; Liu, Y.; Liu, B.; Li, L.; Yu, Y.; Liu, Y.; Liu, B.; et al. The Association between Dietary Patterns and Pre-Pregnancy BMI with Gestational Weight Gain: The “Born in Shenyang” Cohort. Nutrients 2022, 14, 2551. https://doi.org/10.3390/nu14122551
Hu J, Gao M, Ma Y, Wan N, Liu Y, Liu B, Li L, Yu Y, Liu Y, Liu B, et al. The Association between Dietary Patterns and Pre-Pregnancy BMI with Gestational Weight Gain: The “Born in Shenyang” Cohort. Nutrients. 2022; 14(12):2551. https://doi.org/10.3390/nu14122551
Chicago/Turabian StyleHu, Jiajin, Ming Gao, Yanan Ma, Ningyu Wan, Yilin Liu, Borui Liu, Lin Li, Yang Yu, Yang Liu, Bohan Liu, and et al. 2022. "The Association between Dietary Patterns and Pre-Pregnancy BMI with Gestational Weight Gain: The “Born in Shenyang” Cohort" Nutrients 14, no. 12: 2551. https://doi.org/10.3390/nu14122551
APA StyleHu, J., Gao, M., Ma, Y., Wan, N., Liu, Y., Liu, B., Li, L., Yu, Y., Liu, Y., Liu, B., & Wen, D. (2022). The Association between Dietary Patterns and Pre-Pregnancy BMI with Gestational Weight Gain: The “Born in Shenyang” Cohort. Nutrients, 14(12), 2551. https://doi.org/10.3390/nu14122551