
Positive Effects of Vitamin D Supplementation in Patients Hospitalized for COVID-19: A Randomized, Double-Blind, Placebo-Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology
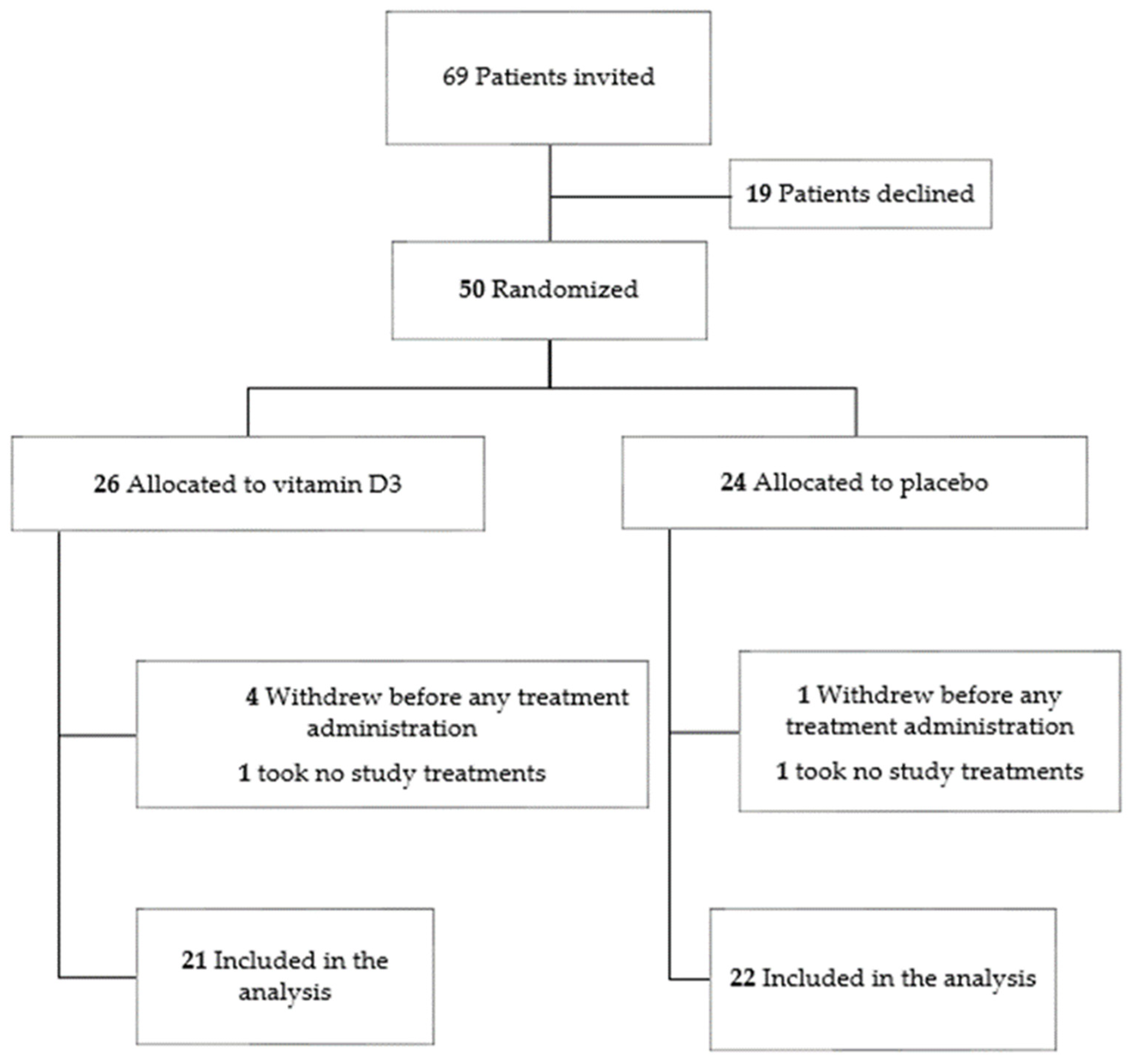
2.2. Study Population
2.3. Study Intervention
2.4. Study Endpoints
2.5. Laboratory Tests
2.6. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Safety Assessment
3.3. Measurements of Calcifediol
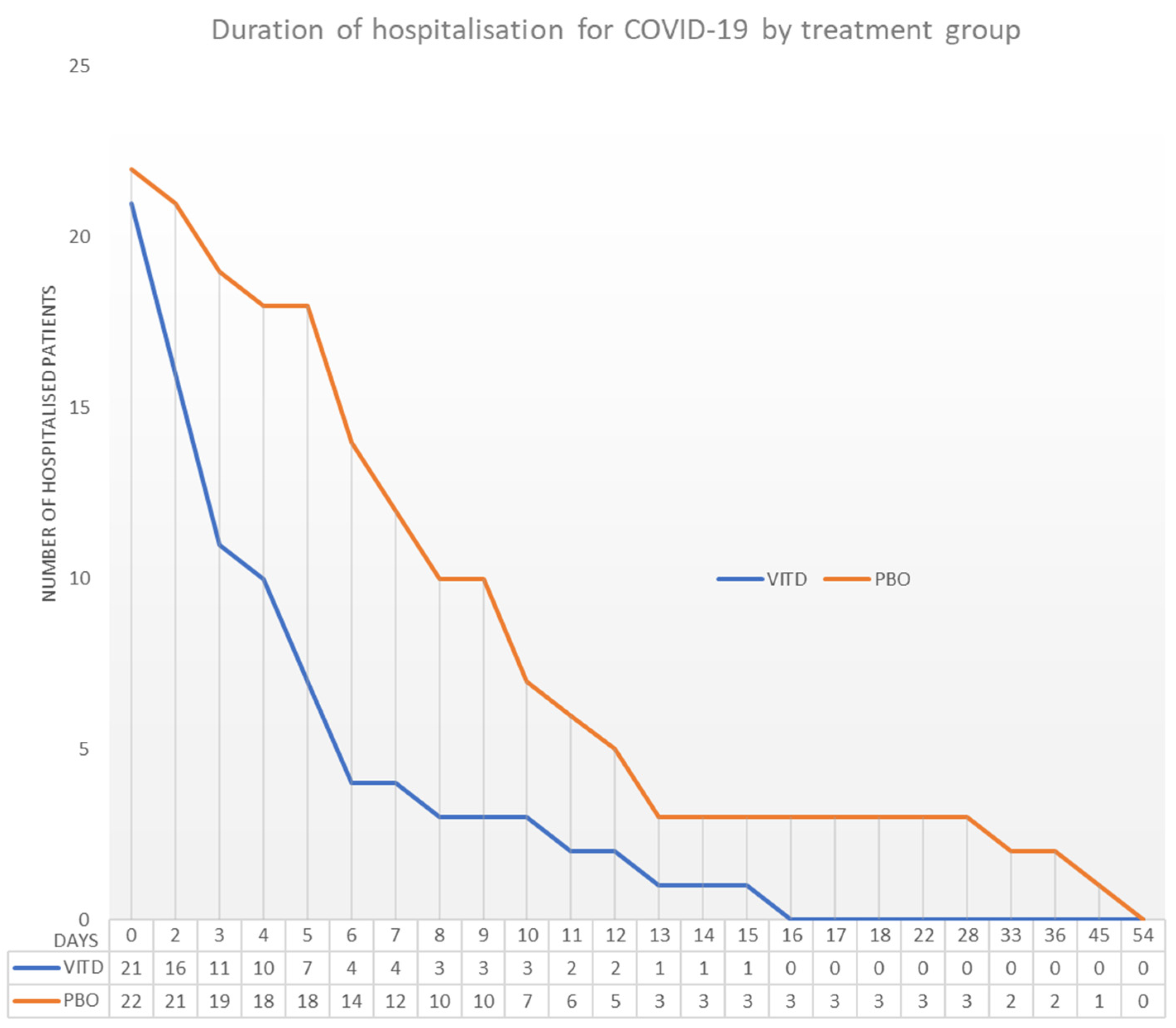
3.4. Clinical Outcomes
3.5. WHO Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.A.; Bearden, A.; Striker, R. Vitamin D and the anti-viral state. J. Clin. Virol. 2011, 50, 194–200. [Google Scholar] [CrossRef]
- Greiller, C.L.; Martineau, A.R. Modulation of the immune response to respiratory viruses by vitamin D. Nutrients 2015, 7, 4240–4270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coussens, A.K. The role of UV radiation and vitamin D in the seasonality and outcomes of infectious disease. Photochem. Photobiol. Sci. 2017, 16, 314–338. [Google Scholar] [CrossRef]
- Lang, P.O.; Aspinall, R. Vitamin D Status and the Host Resistance to Infections: What It Is Currently (Not) Understood. Clin. Ther. 2017, 39, 930–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruber-Bzura, B.M. Vitamin D and Influenza-Prevention or Therapy? Int. J. Mol. Sci. 2018, 19, 2419. [Google Scholar] [CrossRef] [Green Version]
- Rondanelli, M.; Miccono, A.; Lamburghini, S.; Avanzato, I.; Riva, A.; Allegrini, P.; Faliva, M.A.; Peroni, G.; Nichetti, M.; Perna, S. Self-Care for Common Colds: The Pivotal Role of Vitamin D, Vitamin C, Zinc, and Echinacea in Three Main Immune Interactive Clusters (Physical Barriers, Innate and Adaptive Immunity) Involved during an Episode of Common Colds-Practical Advice on Dosages and on the Time to Take These Nutrients/Botanicals in order to Prevent or Treat Common Colds. Evid.-Based Complement. Altern. Med. ECAM 2018, 2018, 5813095. [Google Scholar] [CrossRef] [Green Version]
- Gombart, A.F.; Pierre, A.; Maggini, S. A Review of Micronutrients and the Immune System-Working in Harmony to Reduce the Risk of Infection. Nutrients 2020, 12, 236. [Google Scholar] [CrossRef] [Green Version]
- Jolliffe, D.A.; Camargo Jr, C.A.; Sluyter, J.D.; Aglipay, M.; Aloia, J.F.; Ganmaa, D.; Bergman, P.; Bischoff-Ferrari, H.A.; Borzutzky, A.; Damsgaard, C.T.; et al. Vitamin D supplementation to prevent acute respiratory infections: A systematic review and meta-analysis of aggregate data from randomised controlled trials. Lancet Diabetes Endocrinol. 2021, 9, 276–292. [Google Scholar] [CrossRef]
- Hewison, M. Vitamin D and immune function: An overview. Proc. Nutr. Soc. 2012, 71, 50–61. [Google Scholar] [CrossRef] [Green Version]
- Wei, R.; Christakos, S. Mechanisms Underlying the Regulation of Innate and Adaptive Immunity by Vitamin D. Nutrients 2015, 7, 8251–8260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabbri, A.; Infante, M.; Ricordi, C. Editorial—Vitamin D status: A key modulator of innate immunity and natural defense from acute viral respiratory infections. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 4048–4052. [Google Scholar] [CrossRef] [PubMed]
- Teymoori-Rad, M.; Marashi, S.M. Vitamin D and COVID-19: From potential therapeutic effects to unanswered questions. Rev. Med. Virol. 2021, 31, e2159. [Google Scholar] [CrossRef]
- Dijkman, R.; Jebbink, M.F.; Deijs, M.; Milewska, A.; Pyrc, K.; Buelow, E.; van der Bijl, A.; van der Hoek, L. Replication-dependent downregulation of cellular angiotensin-converting enzyme 2 protein expression by human coronavirus NL63. J. Gen. Virol. 2012, 93, 1924–1929. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Griffiths, C.J.; Martineau, A.R. Vitamin D in the prevention of acute respiratory infection: Systematic review of clinical studies. J. Steroid Biochem. Mol. Biol. 2013, 136, 321–329. [Google Scholar] [CrossRef]
- Hansdottir, S.; Monick, M.M.; Hinde, S.L.; Lovan, N.; Look, D.C.; Hunninghake, G.W. Respiratory epithelial cells convert inactive vitamin D to its active form: Potential effects on host defense. J. Immunol. Baltim. Md. 1950 2008, 181, 7090–7099. [Google Scholar] [CrossRef] [Green Version]
- Olliver, M.; Spelmink, L.; Hiew, J.; Meyer-Hoffert, U.; Henriques-Normark, B.; Bergman, P. Immunomodulatory effects of vitamin D on innate and adaptive immune responses to Streptococcus pneumoniae. J. Infect Dis. 2013, 208, 1474–1481. [Google Scholar] [CrossRef] [Green Version]
- Golpour, A.; Bereswill, S.; Heimesaat, M.M. Antimicrobial and Immune-Modulatory Effects of Vitamin D Provide Promising Antibiotics-Independent Approaches to Tackle Bacterial Infections—Lessons Learnt from a Literature Survey. Eur. J. Microbiol. Immunol. 2019, 9, 80–87. [Google Scholar] [CrossRef]
- Moromizato, T.; Litonjua, A.A.; Braun, A.B.; Gibbons, F.K.; Giovannucci, E.; Christopher, K.B. Association of low serum 25-hydroxyvitamin D levels and sepsis in the critically ill. Crit. Care Med. 2014, 42, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Thickett, D.R.; Moromizato, T.; Litonjua, A.A.; Amrein, K.; Quraishi, S.A.; Lee-Sarwar, K.A.; Mogensen, K.M.; Purtle, S.W.; Gibbons, F.K.; Camargo, C.A.; et al. Association between prehospital vitamin D status and incident acute respiratory failure in critically ill patients: A retrospective cohort study. BMJ Open Respir. Res. 2015, 2, e000074. [Google Scholar] [CrossRef] [Green Version]
- Higgins, D.M.; Wischmeyer, P.E.; Queensland, K.M.; Sillau, S.H.; Sufit, A.J.; Heyland, D.K. Relationship of vitamin D deficiency to clinical outcomes in critically ill patients. JPEN J. Parenter. Enter. Nutr. 2012, 36, 713–720. [Google Scholar] [CrossRef]
- Nair, P.; Lee, P.; Reynolds, C.; Nguyen, N.D.; Myburgh, J.; Eisman, J.A.; Center, J.R. Significant perturbation of vitamin D-parathyroid-calcium axis and adverse clinical outcomes in critically ill patients. Intensive Care Med. 2013, 39, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Braun, A.B.; Gibbons, F.K.; Litonjua, A.A.; Giovannucci, E.; Christopher, K.B. Low serum 25-hydroxyvitamin D at critical care initiation is associated with increased mortality. Crit. Care Med. 2012, 40, 63–72. [Google Scholar] [CrossRef]
- Quraishi, S.A.; Litonjua, A.A.; Moromizato, T.; Gibbons, F.K.; Camargo, C.A., Jr.; Giovannucci, E.; Christopher, K.B. Association between prehospital vitamin D status and hospital-acquired Clostridium difficile infections. JPEN J. Parenter. Enter. Nutr. 2015, 39, 47–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, N.; Zhao, Z.; Koyama, T.; Janz, D.R.; Wang, C.Y.; May, A.K.; Bernard, G.R.; Ware, L.B. Vitamin D deficiency and risk of acute lung injury in severe sepsis and severe trauma: A case-control study. Ann. Intensive Care 2014, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Amrein, K.; Schnedl, C.; Holl, A.; Riedl, R.; Christopher, K.B.; Pachler, C.; Purkart, T.U.; Waltensdorfer, A.; Münch, A.; Warnkross, H.; et al. Effect of high-dose vitamin D3 on hospital length of stay in critically ill patients with vitamin D deficiency: The VITdAL-ICU randomized clinical trial. JAMA 2014, 312, 1520–1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNally, J.D.; Menon, K.; Chakraborty, P.; Fisher, L.; Williams, K.A.; Al-Dirbashi, O.Y.; Doherty, D.R. The association of vitamin D status with pediatric critical illness. Pediatrics 2012, 130, 429–436. [Google Scholar] [CrossRef] [Green Version]
- Kempker, J.A.; West, K.G.; Kempker, R.R.; Siwamogsatham, O.; Alvarez, J.A.; Tangpricha, V.; Ziegler, T.R.; Martin, G.S. Vitamin D status and the risk for hospital-acquired infections in critically ill adults: A prospective cohort study. PLoS ONE 2015, 10, e0122136. [Google Scholar] [CrossRef]
- Kaufman, H.W.; Niles, J.K.; Kroll, M.H.; Bi, C.; Holick, M.F. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS ONE 2020, 15, e0239252. [Google Scholar] [CrossRef]
- Angelidi, A.M.; Belanger, M.J.; Lorinsky, M.K.; Karamanis, D.; Chamorro-Pareja, N.; Ognibene, J.; Palaiodimos, L.; Mantzoros, C.S. Vitamin D Status Is Associated With In-Hospital Mortality and Mechanical Ventilation: A Cohort of COVID-19 Hospitalized Patients. Mayo Clin. Proc. 2021, 96, 875–886. [Google Scholar] [CrossRef]
- Meltzer, D.O.; Best, T.J.; Zhang, H.; Vokes, T.; Arora, V.; Solway, J. Association of Vitamin D Status and Other Clinical Characteristics With COVID-19 Test Results. JAMA Netw. Open 2020, 3, e2019722. [Google Scholar] [CrossRef] [PubMed]
- Han, J.E.; Jones, J.L.; Tangpricha, V.; Brown, M.A.; Hao, L.; Hebbar, G.; Lee, M.J.; Liu, S.; Brown, L.A.S.; Ziegler, T.R.; et al. High Dose Vitamin D Administration in Ventilated Intensive Care Unit Patients: A Pilot Double Blind Randomized Controlled Trial. J. Clin. Transl. Endocrinol. 2016, 4, 59–65. [Google Scholar] [CrossRef] [Green Version]
- Castillo, M.E.; Costa, L.M.E.; Barrios, J.M.V.; Díaz, J.F.A.; Miranda, J.L.; Bouillon, R.; Gomez, J.M.Q. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalier, E.; Faché, W.; Souberbielle, J.C. A Randomised, Double-Blinded, Placebo-Controlled, Parallel Study of Vitamin D3 Supplementation with Different Schemes Based on Multiples of 25,000 IU Doses. Int. J. Endocrinol. 2013, 2013, 327265. [Google Scholar] [CrossRef]
- Schleck, M.L.; Souberbielle, J.C.; Jandrain, B.; Da Silva, S.; De Niet, S.; Vanderbist, F.; Scheen, A.; Cavalier, E. A Randomized, Double-Blind, Parallel Study to Evaluate the Dose-Response of Three Different Vitamin D Treatment Schemes on the 25-Hydroxyvitamin D Serum Concentration in Patients with Vitamin D Deficiency. Nutrients 2015, 7, 5413–5422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Niet, S.; Coffiner, M.; Da Silva, S.; Jandrain, B.; Souberbielle, J.C.; Cavalier, E. A Randomized Study to Compare a Monthly to a Daily Administration of Vitamin D3 Supplementation. Nutrients 2018, 10, 659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Working Group on the Clinical Characterisation and Management of COVID-19 infection. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef]
- Diagnostic Testing for SARS-CoV-2. Available online: https://www.who.int/publications-detail-redirect/diagnostic-testing-for-sars-cov-2 (accessed on 30 May 2022).
- Wise, S.A.; Camara, J.E.; Sempos, C.T.; Lukas, P.; Le Goff, C.; Peeters, S.; Burdette, C.Q.; Nalin, F.; Hahm, G.; Durazo-Arvizu, R.A.; et al. Vitamin D Standardization Program (VDSP) intralaboratory study for the assessment of 25-hydroxyvitamin D assay variability and bias. J. Steroid Biochem. Mol. Biol. 2021, 212, 105917. [Google Scholar] [CrossRef]
- Cavalier, E.; Fraser, C.G.; Bhattoa, H.P.; Heijboer, A.C.; Makris, K.; Ulmer, C.Z.; Vesper, H.W.; Vasikaran, S.; Lukas, P.; Delanaye, P.; et al. Analytical Performance Specifications for 25-Hydroxyvitamin D Examinations. Nutrients 2021, 13, 431. [Google Scholar] [CrossRef] [PubMed]
- Cavalier, E.; Lukas, P.; Bekaert, A.C.; Peeters, S.; Le Goff, C.; Yayo, E.; Delanaye, P.; Souberbielle, J.C. Analytical and clinical evaluation of the new Fujirebio Lumipulse®G non-competitive assay for 25(OH)-vitamin D and three immunoassays for 25(OH)D in healthy subjects, osteoporotic patients, third trimester pregnant women, healthy African subjects, hemodialyzed and intensive care patients. Clin. Chem. Lab. Med. 2016, 54, 1347–1355. [Google Scholar] [CrossRef]
- Cavalier, E.; Lukas, P.; Crine, Y.; Peeters, S.; Carlisi, A.; Le Goff, C.; Gadisseur, R.; Delanaye, P.; Souberbielle, J.C. Evaluation of automated immunoassays for 25(OH)-vitamin D determination in different critical populations before and after standardization of the assays. Clin. Chim. Acta Int. J. Clin. Chem. 2014, 431, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Murai, I.H.; Fernandes, A.L.; Sales, L.P.; Pinto, A.J.; Goessler, K.F.; Duran, C.S.; Silva, C.B.; Franco, A.S.; Macedo, M.B.; Dalmolin, H.H.; et al. Effect of a Single High Dose of Vitamin D3 on Hospital Length of Stay in Patients With Moderate to Severe COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Cannata-Andía, J.B.; Díaz-Sottolano, A.; Fernández, P.; Palomo-Antequera, C.; Herrero-Puente, P.; Mouzo, R.; Carrillo-López, N.; Panizo, S.; Ibañez, G.H.; Cusumano, C.A.; et al. A single-oral bolus of 100,000 IU of cholecalciferol at hospital admission did not improve outcomes in the COVID-19 disease: The COVID-VIT-D-a randomised multicentre international clinical trial. BMC Med. 2022, 20, 83. [Google Scholar] [CrossRef] [PubMed]
- Milani, G.P.; Simonetti, G.D.; Edefonti, V.; Lava, S.A.; Agostoni, C.; Curti, M.; Stettbacher, A.; Bianchetti, M.G.; Muggli, F. Seasonal variability of the vitamin D effect on physical fitness in adolescents. Sci. Rep. 2021, 11, 182. [Google Scholar] [CrossRef]
- Dopico, X.C.; Evangelou, M.; Ferreira, R.C.; Guo, H.; Pekalski, M.L.; Smyth, D.J.; Cooper, N.; Burren, O.S.; Fulford, A.J.; Hennig, B.J.; et al. Widespread seasonal gene expression reveals annual differences in human immunity and physiology. Nat. Commun. 2015, 6, 7000. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Day 1, 2, 3, 4, 8, 15, 22, 29 and 36 | |
| Group 1: Placebo group | 1 ampoule of placebo + standard of care treatment |
| Group 2: Vitamin D group | 1 ampoule of vitamin D 25,000 IU + standard of care treatment |
| Placebo Group n = 22 | Vitamin D Group n = 21 | p Value | ||
|---|---|---|---|---|
| Age (years) | ||||
| Mean ± SD | 68.73 ± 10.97 | 63.24 ± 14.46 | 0.167 | |
| min–max | 41.00–88.00 | 36.00–98.00 | ||
| Gender | ||||
| Male | n (%) | 10 (45%) | 13 (62%) | 0.364 |
| Female | n (%) | 12 (54%) | 8 (38%) | |
| Weight (kg) | ||||
| Mean ± SD | 79.46 ± 17.54 | 75.85 ± 12.03 | 0.728 | |
| min–max | 47.70–106.00 | 63.00–108.00 | ||
| BMI (kg/m2) | ||||
| Mean ± SD | 28.92 ± 6.92 | 26.52 ± 3.24 | 0.133 | |
| min–max | 19.11–44.89 | 21.30–32.97 | ||
| Calcifediol concentration at screening (ng/mL) | n | 22 | 21 | |
| Mean ± SD | 16.87 ± 9.48 | 17.87 ± 10.15 | 0.741 | |
| min–max | 4.80–43.60 | 5.00–44.60 | ||
| Vaccinal Status | ||||
| Not vaccinated | n (%) | 20 (91%) | 17 (81%) | 0.169 |
| 1 Dose | n (%) | 2 (9.1%) | 1 (5%) | |
| 2 Doses | n (%) | 0 (0.0%) | 3 (14%) | |
| Cardiac Pathology | ||||
| Yes | n (%) | 9 (42%) | 7 (33%) | |
| Hepatic Failure | ||||
| Yes | n (%) | 0 (0.0%) | 2 (9.5%) | |
| Renal Failure | ||||
| Yes | n (%) | 4 (18%) | 4 (19%) | |
| Diabetes | ||||
| Yes | n (%) | 8 (36%) | 8 (38%) | |
| Arterial Hypertension | ||||
| Yes | n (%) | 13 (59%) | 11 (52%) | |
| Chronic lung disease | ||||
| Yes | n (%) | 9 (42%) | 5 (24%) |
| Placebo Group n = 22 | Vitamin D Group n = 21 | p Value | ||
|---|---|---|---|---|
| Hospital length of stay (Days) | ||||
| Median | 8.0 | 4.0 | 0.003 | |
| Q1–Q3 | 6.0–12.0 | 3.0–6.0 | ||
| Proportion of patients hospitalized | ||||
| At Day 7 | n (%) | 12 (54) | 4 (19.) | 0.016 |
| At Day 14 | n (%) | 3 (14) | 1 (4.8)) | 0.262 |
| At Day 21 | n (%) | 3 (14) | 0 (0.0) | 0.125 |
| At Day 28 | n (%) | 3 (14) | 0 (0.0) | 0.125 |
| At Day 36 | n (%) | 2 (9.1%) | 0 (0.0) | 0.256 |
| Admission in intensive care unit | n (%) | 5 (23) | 2 (9.5) | 0.412 |
| Intensive Care Unit length of stay (Days) | Mean ± SD | 12.4 ± 14.3 | 4.0 ± 4.2 | 0.472 |
| min–max | 3.0–36.0 | 1.0–7.0 | ||
| Proportion of patients requiring supplemental oxygen, non-invasive ventilation or high-flow oxygen devices, invasive mechanical ventilation | n (%) | 19 (86) | 13 (62) | 0.054 |
| Duration of supplemental conventional oxygen (Days) | ||||
| Median | 7.0 | 4.0 | 0.012 | |
| Q1–Q3 | 5.0–11.0 | 0.0–6.0 | ||
| Duration of non-invasive ventilation or high-flow nasal oxygen, invasive mechanical ventilation or additional organ support (Days) | Mean ± SD | 1.3 ± 4.2 | 0.3 ± 1.3 | 0.306 |
| min–max | 0.0–16.0 | 0.0–16.0 | ||
| Time until absence of fever for more than 48 h without antipyretics (Days) | Mean ± SD | 14.1 ± 13.1 | 7.7 ± 4.7 | 0.059 |
| min–max | 0.0–52.0 | 2.0–18.0 | ||
| Mortality All causes | n (%) | 3 (14) | 4 (19) | 0.286 |
| Mortality related to COVID-19 | n (%) | 3 (12) | 1 (4.8) | 0.129 |
| Placebo Group n = 22 | Vitamin D Group n = 21 | p Value | ||
|---|---|---|---|---|
| Ordinal Scale for clinical improvement by severity * at baseline (Day 1) | 0.512 | |||
| No infection | n (%) | 0 (0.0) | 0 (0.0) | |
| Mild | n (%) | 0 (0.0) | 0 (0.0) | |
| Moderate | n (%) | 21 (95) | 20 (95) | |
| Severe | n (%) | 1 (4.5) | 1 (4.8) | |
| Death | n (%) | 0 (0.0) | 0 (0.0) | |
| Ordinal Scale for clinical improvement by severity * at Day 7 | 0.005 | |||
| No infection | n (%) | 0 (0.0) | 0 (0.0) | |
| Mild | n (%) | 4 (18) | 15 (71) | |
| Moderate | n (%) | 14 (63) | 4 (19) | |
| Severe | n (%) | 3 (13) | 1 (4.8) | |
| Death | n (%) | 1 (4.5) | 1 (4.8) | |
| Ordinal Scale for clinical improvement by severity * at Day 15 | 0.549 | |||
| No infection | n (%) | 0 (0.0) | 0 (0.0) | |
| Mild | n (%) | 15 (68) | 18 (85) | |
| Moderate | n (%) | 4 (18) | 1 (4.8) | |
| Severe | n (%) | 1 (4.5) | 1 (4.8) | |
| Death | n (%) | 1 (4.5) | 1 (4.8) | |
| Ordinal Scale for clinical improvement by severity * at Day 22 | 0.543 | |||
| No infection | n (%) | 0 (0.0) | 0 (0.0) | |
| Mild | n (%) | 17 (77) | 19 (90) | |
| Moderate | n (%) | 1 (4.5) | 0 (0.0) | |
| Severe | n (%) | 2 (9.1) | 0 (0.0) | |
| Death | n (%) | 2 (9.1) | 2 (9.5) | |
| Ordinal Scale for clinical improvement by severity * at Day 29 | 0.543 | |||
| No infection | n (%) | 0 (0.0) | 0 (0.0) | |
| Mild | n (%) | 17 (77) | 19 (90) | |
| Moderate | n (%) | 1 (4.5) | 0 (0.0) | |
| Severe | n (%) | 2 (9.1) | 0 (0.0) | |
| Death | n (%) | 2 (9.1) | 2 (9.5) | |
| Ordinal Scale for clinical improvement by severity * at Day 36 | 0.318 | |||
| No infection | n (%) | 0 (0.0) | 0 (0.0) | |
| Mild | n (%) | 17 (77.) | 19 (90) | |
| Moderate | n (%) | 2 (9.1) | 0 (0.0) | |
| Severe | n (%) | 0 (0.0) | 0 (0.0) | |
| Death | n (%) | 3 (14) | 2 (9.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Niet, S.; Trémège, M.; Coffiner, M.; Rousseau, A.-F.; Calmes, D.; Frix, A.-N.; Gester, F.; Delvaux, M.; Dive, A.-F.; Guglielmi, E.; et al. Positive Effects of Vitamin D Supplementation in Patients Hospitalized for COVID-19: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2022, 14, 3048. https://doi.org/10.3390/nu14153048
De Niet S, Trémège M, Coffiner M, Rousseau A-F, Calmes D, Frix A-N, Gester F, Delvaux M, Dive A-F, Guglielmi E, et al. Positive Effects of Vitamin D Supplementation in Patients Hospitalized for COVID-19: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients. 2022; 14(15):3048. https://doi.org/10.3390/nu14153048
Chicago/Turabian StyleDe Niet, Sophie, Mickaël Trémège, Monte Coffiner, Anne-Francoise Rousseau, Doriane Calmes, Anne-Noelle Frix, Fanny Gester, Muriel Delvaux, Anne-Francoise Dive, Elora Guglielmi, and et al. 2022. "Positive Effects of Vitamin D Supplementation in Patients Hospitalized for COVID-19: A Randomized, Double-Blind, Placebo-Controlled Trial" Nutrients 14, no. 15: 3048. https://doi.org/10.3390/nu14153048
APA StyleDe Niet, S., Trémège, M., Coffiner, M., Rousseau, A. -F., Calmes, D., Frix, A. -N., Gester, F., Delvaux, M., Dive, A. -F., Guglielmi, E., Henket, M., Staderoli, A., Maesen, D., Louis, R., Guiot, J., & Cavalier, E. (2022). Positive Effects of Vitamin D Supplementation in Patients Hospitalized for COVID-19: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients, 14(15), 3048. https://doi.org/10.3390/nu14153048