
Iron Deficiency in Adolescent and Young Adult German Athletes—A Retrospective Study

Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Participants
2.2. Blood Collection and Preparation
2.3. Anthropometric Data
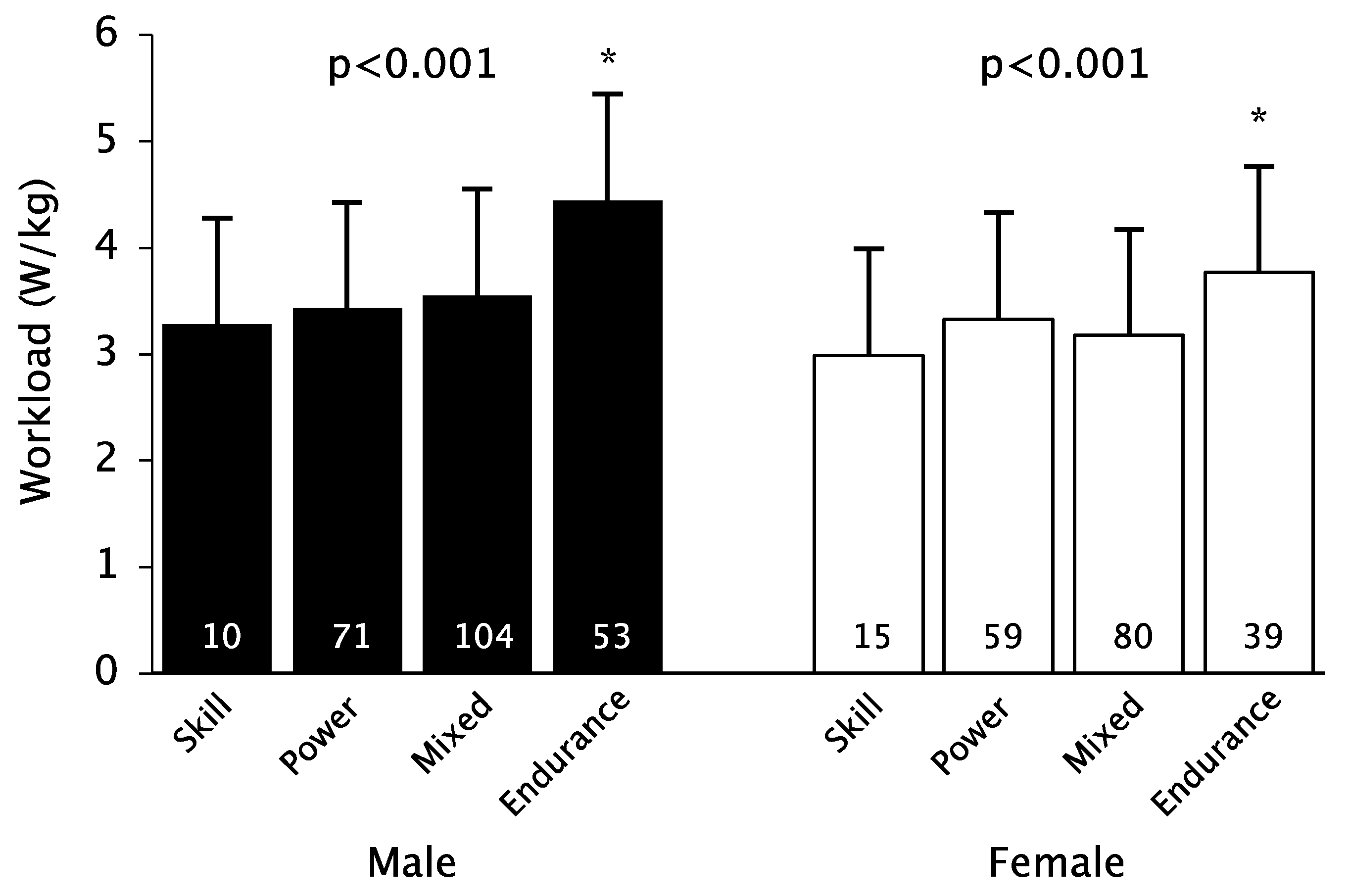
2.4. Ergometry
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limitations
- Athletes should eat an iron-rich diet taking into account vegetarian and vegan diets.
- Athletes should be monitored for iron levels at least once a year, and adolescent competitive athletes and women, in particular, should be monitored and treated more intensively.
- In case of insufficient dietary iron intake and iron deficiency, drug therapy should be taken into account (for points 2 and 3 age, type of sport, and performance status must be considered; for example, the indication of iron supplementation in a female middle-distance runner prior to international competition would be much more generous).
- An uncontrolled iron substitution should not take place.
6. Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lieu, P.T.; Heiskala, M.; Peterson, P.A.; Yang, Y. The roles of iron in health and disease. Mol. Asp. Med. 2001, 22, 1–87. [Google Scholar] [CrossRef]
- Mettler, S. Ferrum—Ein Mineralstoff im Sport. Schweiz. Z. Für Sportmed. Und Sport. 2004, 52, 105–114. [Google Scholar]
- Burden, R.J.; Morton, K.; Richards, T.; Whyte, G.P.; Pedlar, C.R. Is iron treatment beneficial in, iron-deficient but non-anaemic (IDNA) endurance athletes? A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Conrad, M.E.; Umbreit, J.N. Pathways of iron absorption. Blood.Cells Mol. Dis. 2002, 29, 336–355. [Google Scholar] [CrossRef] [PubMed]
- Peters, H.P.F.; De Vries, W.R.; Vanberge-Henegouwen, G.P.; Akkermans, L.M.A. Potential benefits and hazards of physical activity and exercise on the gastrointestinal tract. Gut 2001, 48, 435–439. [Google Scholar] [CrossRef] [Green Version]
- Warner, D.C.; Schnepf, G.; Barrett, M.S.; Dian, D.; Swigonski, N.L. Prevalence, attitudes, and behaviors related to the use of nonsteroidal anti-inflammatory drugs (NSAIDs) in student athletes. J. Adolesc. Health 2002, 30, 150–153. [Google Scholar] [CrossRef]
- Friedmann, B. Sportleranämie. Dtsch. Z. Sportmed. 2001, 52, 262–263. [Google Scholar]
- Hallberg, L.; Hulthen, L. High serum ferritin is not identical to high iron stores. Am. J. Clin. Nutr. 2003, 78, 1225–1226. [Google Scholar] [CrossRef] [Green Version]
- Zoller, H.; Vogel, W. Iron supplementation in athletes-first do no harm. Nutrition 2004, 20, 615–619. [Google Scholar] [CrossRef]
- Stupnicki, R.; Malczewska, J.; Milde, K.; Hackney, A.C. Day to day variability in the transferring receptor/ferritin index in female athletes. Br. J. Sports Med. 2003, 37, 267–269. [Google Scholar] [CrossRef] [Green Version]
- Robinson, Y.; Cristancho, E.; Böning, D. Die Hypoferritinämie des Sportlers ist kein sicheres Indiz für Eisenmangel. Dtsch. Z. Sport. 2010, 61, 141–145. [Google Scholar]
- Malczewska, J.; Blach, W.; Stupnicki, R. The effects of physical exer-cise on the concentrations of ferritin and transferrin receptor in plas-ma of female judoists. Int. J. Sports. Med. 2000, 21, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Murray-Kolb, L.E.; Beard, J.L.; Joseph, L.J.; Davey, S.L.; Evans, W.J.; Campbell, W.W. Resistance training affects iron status in older men and women. Int. J. Sport. Nutr. Exerc. Metab. 2001, 11, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Birkeland, K.I.; Stray-Gundersen, J.; Hemmersbach, P.; Hallen, J.; Haug, E.; Bahr, R. Effect of rhEPO administration on serum levels of sTfRand cycling performance. Med. Sci. Sports. Exerc. 2000, 32, 1238–1243. [Google Scholar] [CrossRef]
- Clénin, G.; Cordes, M.; Huber, A.; Schumacher, Y.O.; Noack, P.; Scales, J.; Kriemler, S. Iron deficiency in sports—Definition, influence on performance and therapy. Swiss Med. Wkly. 2015, 145, w14196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Guideline: Daily Iron Supplementation in Infants and Children; Committee GR; World Health Organization (WHO): Switzerland, Geneva, 2016. [Google Scholar]
- Sekhar, D.L.; Murray-Kolb, L.E.; Kunselman, A.R.; Weisman, C.S.; Paul, I.M. Association between menarche and iron deficiency in non-anemic young women. PLoS ONE 2017, 12, e0177183. [Google Scholar] [CrossRef] [Green Version]
- Schleiffenbaum, B.; Viollier, E.; Wegmller, E.; Viollier, A.; Stettler, E. Unexpected high prevalence of metabolic disorders and chronic disease among young male draftees—The Swiss Army XXI experience. Swiss Med. Wkly. 2006, 18, 136, 175–184. [Google Scholar] [CrossRef]
- Sim, M.; Garvican-Lewis, L.A.; Cox, G.R.; Govus, A.; McKay, A.K.A.; Stellingwerff, T.; Peeling, P. Iron considerations for the athlete: A narrative review. Eur. J Appl. Physiol. 2019, 119, 1463–1478. [Google Scholar] [CrossRef]
- Koehler, K.; Braun, H.; Achtzehn, S.; Hildebrand, U.; Predel, H.G.; Mester, J.; Schänzer, W. Iron status in elite young athletes: Gender-dependent influences of diet and exercise. Eur. J. Appl. Physiol. 2012, 112, 513–523. [Google Scholar] [CrossRef]
- Castell, L.M.; Nieman, D.C.; Bermon, S.; Peeling, P. Exercise-Induced Illness and Inflammation: Can Immunonutrition and Iron Help? Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Pelliccia, A.; Adami, P.E.; Quattrini, F.; Squeo, M.R.; Caselli, S.; Verdile, L.; Maestrini, V.; Di Paolo, F.; Pisicchio, C.; Ciardo, R.; et al. Are Olympic athletes free from cardiovascular diseases? Systematic investigation in 2352 participants from Athens 2004 to Sochi 2014. Br. J. Sports Med. 2017, 51, 238–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwabara, A.M.; Tenforde, A.S.; Do, J.T.F.; Fredericson, M. Iron deficiency in athletes: A narrative review. PM&R 2022, 14, 620–642. [Google Scholar] [CrossRef]
- Hunt, J.R. Moving toward a plant-based diet: Are iron and zinc at risk? Nutr. Rev. 2002, 60, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Rogerson, D. Vegan diets: Practical advice for athletes and exercisers. J. Int. Soc. Sports Nutr. 2017, 14, 36. [Google Scholar] [CrossRef] [Green Version]
- Beard, J.L. Iron Requirements in Adolescent Females. J. Nutr. 2000, 130, 440S–442S. [Google Scholar] [CrossRef] [Green Version]
- Daily, J.P.; Stumbo, J.R. Female Athlete Triad. Prim. Care Clin. Off. Pract. 2018, 45, 615–624. [Google Scholar] [CrossRef]
- Beard, J.; Tobin, B. Iron status and exercise. Am. J. Clin. Nutr. 2000, 72, 594S–597S. [Google Scholar] [CrossRef] [Green Version]
- Phillips, F. Vegetarian nutrition. Nutr. Bull. 2005, 30, 132–167. [Google Scholar] [CrossRef]
- Stoffel, N.U.; Cercamondi, C.I.; Brittenham, G.; Zeder, C.; Geurts-Moespot, A.J.; Swinkels, D.W.; Moretti, D.; Zimmermann, M.B. Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: Two open-label, randomised controlled trials. Lancet Haematol. 2017, 4, e524–e533. [Google Scholar] [CrossRef]
- Schaap, C.; Hendriks, J.C.; Kortman, G.A.; Klaver, S.M.; Kroot, J.J.; Laarakkers, C.M.; Wiegerinck, E.T.; Tjalsma, H.; Janssen, M.C.; Swinkels, D.W. Diurnal Rhythm rather than Dietary Iron Mediates Daily Hepcidin Variations. Clin. Chem. 2013, 59, 527–535. [Google Scholar] [CrossRef]
- Harris, S.S. The Effect of Calcium Consumption on Iron Absorption and Iron Status. Nutr. Clin. Care 2002, 5, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Vadhan-Raj, S.; Strauss, W.; Ford, D.; Bernard, K.; Boccia, R.; Li, J.; Allen, L.F. Efficacy and safety of IV ferumoxytol for adults with iron deficiency anemia previously unresponsive to or unable to tolerate oral iron. Am. J. Hematol. 2014, 89, 7–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDougall, I.C. Evolution of IV iron compounds over the last century. J. Ren. Care 2009, 35, 8–13. [Google Scholar] [CrossRef]
- The Prohibited List|World Anti-Doping Agency. Available online: https://www.wada-ama.org/en/prohibited-list?q=intravenous%20infusions (accessed on 9 September 2022).
- Klingshirn, L.A.; Pate, R.R.; Bourque, S.P.; Davis, J.M.; Sargent, R.G. Effect of iron supplementation on endurance capacity in iron-depleted female runners. Med. Sci. Sports Exerc. 1992, 24, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Fogelholm, M.; Jaakkola, L.; Lampisjärvi, T. Effects of Iron Supplementation in Female Athletes with Low Serum Ferritin Concentration. Endoscopy 1992, 13, 158–162. [Google Scholar] [CrossRef]
- Garvican, L.A.; Saunders, P.U.; Cardoso, T.; Macdougall, I.C.; Lobigs, L.M.; Fazakerley, R.; Fallon, K.E.; Anderson, B.; Anson, J.M.; Thompson, K.G.; et al. Intravenous Iron Supplementation in Distance Runners with Low or Suboptimal Ferritin. Med. Sci. Sports Exerc. 2014, 46, 376–385. [Google Scholar] [CrossRef]
- Brutsaert, T.D.; Hernandez-Cordero, S.; Rivera, J.; Viola, T.; Hughes, G.; Haas, J.D. Iron supplementation improves progressive fatigue resistance during dynamic knee extensor exercise in iron-depleted, nonanemic women. Am. J. Clin. Nutr. 2003, 77, 441–448. [Google Scholar] [CrossRef] [Green Version]
- Rubeor, A.; Goojha, C.; Manning, J.; White, J. Does Iron Supplementation Improve Performance in Iron-Deficient Nonanemic Athletes? Sports Health A Multidiscip. Approach 2018, 10, 400–405. [Google Scholar] [CrossRef]


{kind=link}
| Age | n | Normal Ferritin Levels | Prelalent | Latent | Anemia | |
|---|---|---|---|---|---|---|
| up to 14 | male | 33 | 27 (81.8%) | 4 (12.1%) | 2 (6.1%) | 0 |
| female | 37 | 28 (75.7%) | 3 (8.1%) | 5 (13.5%) | 1 (2.7%) | |
| 14–18 | male | 198 | 169 (85.4%) | 14 (7.1%) | 14 (7.1%) | 1 (0.5%) |
| female | 159 | 97 (61.0%) | 30 (18.9%) | 31 (19.5%) | 1 (0.6%) | |
| over 18 | male | 108 | 106 (98.1%) | 0 | 1 (0.9%) | 1 (0.9%) |
| female | 94 | 61 (64.9%) | 18 (19.1%) | 11 (11.7%) | 4 (4.3%) | |
| overall | male | 339 | 302 (89.1%) | 18 (5.3%) | 17 (5.0%) | 2 (0.6%) |
| female | 290 | 186 (64.1%) | 51 (17.6%) | 47 (16.2%) | 6 (2.1%) |
| Sport Types | n | Normal Ferritin Levels | Prelalent | Latent | Anemia | |
|---|---|---|---|---|---|---|
| Skill | male | 13 | 12 (92.3%) | 1 (7.7%) | 0 | 0 |
| female | 17 | 10 (58.8%) | 1 (5.9%) | 5 (29.4%) | 1 (5.9%) | |
| Power | male | 108 | 93 (86.1%) | 6 (5.6%) | 9 (8.3%) | 0 |
| female | 106 | 75 (70.8%) | 14 (13.2%) | 16 (15.1%) | 1 (0.9%) | |
| Mixed | male | 144 | 128 (88.9%) | 8 (5.6%) | 6 (4.2%) | 2 (1.4%) |
| female | 111 | 69 (62.2%) | 26 (23.4%) | 13 (11.7%) | 3 (2.7%) | |
| Endurance | male | 74 | 69 (93.2%) | 3 (4.1%) | 2 (2.7%) | 0 |
| female | 56 | 32 (57.1%) | 10 (17.9%) | 13 (23.2%) | 1 (1.8%) |
| Normal Ferritin Levels | Iron Deficiency | ||||||
|---|---|---|---|---|---|---|---|
| n | n | p | g | ||||
| Age (years) | male | 15.6 ± 1.4 | 196 | 15.1 ± 1.3 | 35 | 0.028 | 0.41 |
| female | 15.5 ± 1.6 | 125 | 15.6 ± 1.4 | 71 | 0.620 | - | |
| Height (cm) | male | 178.6 ± 10.8 | 166 | 174.0 ± 11.0 | 33 | 0.038 | 0.43 |
| female | 168.8 ± 7.0 | 99 | 169.9 ± 8.8 | 65 | 0.382 | - | |
| Weight (kg) | male | 67.7 ± 13.6 | 166 | 63.6 ± 13.8 | 33 | 0.044 | 0.37 |
| female | 61.1 ± 10.2 | 99 | 59.9 ± 9.2 | 65 | 0.420 | - | |
| BMI-SDS | male | −0.05 ± 0.77 | 166 | −0.14 ± 0.78 | 33 | 0.564 | - |
| female | 0.01± 0.87 | 99 | −0.25 ± 0.77 | 65 | 0.047 | 0.32 | |
| Body fat (%) | male | 9.6 ± 5.3 | 160 | 9.2 ± 4.7 | 30 | 0.769 | - |
| female | 18.7 ± 7.0 | 99 | 17.9 ± 5.2 | 64 | 0.860 | - | |
| Workload (W/kg) | male | 3.8 ± 0.8 | 138 | 3.7 ± 0.6 | 27 | 0.741 | - |
| female | 3.3 ± 0.5 | 82 | 3.3 ± 0.7 | 56 | 0.588 | - | |
| Heart rate (bpm) | male | 191.3 ± 11.0 | 138 | 193.2 ± 8.5 | 27 | 0.646 | - |
| female | 189.4 ± 9.5 | 82 | 188.7 ± 8.0 | 56 | 0.643 | - | |
| RRsys (mmHg) | male | 197.1 ± 25.0 | 138 | 191.8 ± 25.4 | 27 | 0.321 | - |
| female | 183.5 ± 20.6 | 82 | 190.1 ± 22.0 | 56 | 0.073 | - | |
| RRdia (mmHg) | male | 79.3 ± 9.8 | 138 | 80.8 ± 8.4 | 27 | 0.467 | - |
| female | 79.1 ± 9.1 | 82 | 79.3 ± 8.3 | 56 | 0.927 | - | |
| Lactate (mmol/L) | male | 8.90 ± 2.67 | 12 | 9.97 | 1 | - | - |
| female | 9.14 ± 2.04 | 7 | 7.14 ± 1.28 | 2 | 0.143 | - | |
| Hämoglobin | male | 14.88 ± 0.94 | 196 | 14.31 ± 0.91 | 35 | 0.001 | 0.61 |
| female | 13.39 ± 0.85 | 125 | 12.97 ± 0.95 | 71 | 0.002 | 0.48 | |
| Hämatokrit | male | 43.2 ± 2.7 | 196 | 42.0 ± 2.9 | 35 | 0.021 | 0.42 |
| female | 39.5 ± 2.5 | 125 | 38.8 ± 2.5 | 71 | 0.044 | 0.30 | |
| MCH | male | 29.4 ± 1.3 | 196 | 28.3 ± 1.1 | 35 | <0.001 | 0.85 |
| female | 29.3 ± 1.4 | 125 | 28.5 ± 1.7 | 71 | 0.002 | 0.49 | |
| MCHC | male | 34.5 ± 0.9 | 196 | 34.2 ± 1.0 | 35 | 0.078 | - |
| female | 34.0 ± 0.9 | 125 | 33.5 ± 1.0 | 71 | 0.002 | 0.52 | |
| MCV | male | 84.9 ± 3.3 | 196 | 83.0 ± 2.6 | 35 | 0.003 | 0.59 |
| female | 86.3 ± 3.1 | 125 | 84.9 ± 3.6 | 71 | 0.011 | 0.40 | |
| Ferritin | male | 64.9 ± 32.2 | 196 | 21.1 ± 6.3 | 35 | <0.001 | 1.47 |
| female | 56.6 ±46.3 | 125 | 17.8 ± 6.6 | 71 | <0.001 | 1.04 | |
| Eisen | male | 106.4 ± 40.1 | 196 | 83.2 ± 29.5 | 35 | 0.002 | 0.57 |
| female | 101.2 ± 38.8 | 125 | 80.8 ± 50.1 | 71 | <0.001 | 0.47 | |
| Transferrin | male | 274.7 ± 32.9 | 196 | 302.0 ± 32.9 | 35 | <0.001 | −0.83 |
| female | 281.3 ± 35.5 | 125 | 320.0 ± 46.5 | 71 | <0.001 | −0.97 | |
| Lösl. Rezeptor | male | 3.40 ± 0.43 | 18 | 3.66 ± 0.82 | 35 | 0.127 | - |
| female | 3.14 ± 0.89 | 32 | 3.52 ± 1.15 | 71 | 0.028 | −0.35 | |
| Trans.Sättigung | male | 28.1 ± 12.2 | 196 | 19.8 ± 7.4 | 35 | <0.001 | 0.71 |
| female | 25.8 ± 9.9 | 125 | 18.1 ± 10.1 | 71 | <0.001 | 0.77 | |
| Normal Ferritin Levels | Iron Deficiency | ||||||
|---|---|---|---|---|---|---|---|
| n | n | p | g | ||||
| Age | male | 21.7 ± 3.0 | 106 | 18.7 ± 0.1 | 2 | - | |
| female | 21.7 ± 3.4 | 61 | 21.6 ± 3.5 | 33 | 0.632 | - | |
| Height | male | 182.7 ± 9.4 | 81 | 164.0 | 1 | - | |
| female | 174.8 ± 9.6 | 42 | 170.0 ± 12.5 | 25 | 0.068 | - | |
| Weight | male | 78.6 ± 14.7 | 81 | 53.4 | 1 | - | |
| female | 66.8 ± 11.0 | 42 | 64.2 ± 11.7 | 25 | 0.364 | - | |
| BMI | male | 23.4 ± 3.0 | 81 | 19.9 | 1 | - | |
| female | 21.8 ± 2.7 | 42 | 22.2 ± 2.8 | 25 | 0.555 | - | |
| Body fat (%) | male | 10.8 ± 5.0 | 69 | 22.5 | 1 | - | |
| female | 16.7 ± 5.2 | 42 | 18.0 ± 4.4 | 22 | 0.331 | - | |
| Workload (W/kg) | male | 3.5 ± 0.8 | 72 | 3.7 | 1 | - | |
| female | 3.5± 0.5 | 34 | 3.2 ± 0.8 | 21 | 0.101 | - | |
| Heart rate (bpm) | male | 182.8 ± 13.4 | 72 | 181.0 | 1 | - | - |
| female | 183.4 ± 11.1 | 34 | 183.6 ± 10.9 | 21 | 0.943 | - | |
| RRsys (mmHg) | male | 203.3 ± 22.4 | 72 | 206 | 1 | - | - |
| female | 199.1 ± 20.9 | 34 | 189.0 ± 30.0 | 21 | 0.135 | - | |
| RRdia (mmHg) | male | 81.7 ± 9.1 | 72 | 91.0 | 1 | - | - |
| female | 83.7 ± 7.4 | 34 | 82.0 ± 8.9 | 21 | 0.470 | - | |
| Lactate (mmol/L) | male | 8.99 ± 2.90 | 37 | - | - | - | |
| female | 9.50 ± 2.40 | 17 | 9.28 ± 2.25 | 8 | 0.835 | - | |
| Hämoglobin | male | 15.25 ± 0.96 | 106 | 12.80 ± 0.42 | 2 | - | - |
| female | 13.72 ± 0.90 | 61 | 12.88 ± 0.88 | 33 | <0.001 | 0.93 | |
| Hämatokrit | male | 44.4 ± 2.5 | 106 | 38.1 ± 0.2 | 2 | - | - |
| female | 40.2 ± 2.4 | 61 | 38.9 ± 2.6 | 33 | 0.016 | 0.52 | |
| MCH | male | 29.6 ± 1.3 | 106 | 30.5 ± 0.7 | 2 | - | - |
| female | 30.0 ± 1.3 | 61 | 28.3 ± 2.1 | 33 | <0.001 | 1.05 | |
| MCHC | male | 34.3 ± 0.9 | 106 | 33.5 ± 0.7 | 2 | - | - |
| female | 34.1 ± 0.9 | 61 | 33.2 ± 0.9 | 33 | <0.001 | 1.04 | |
| MCV | male | 86.3 ± 3.0 | 106 | 89.5 ± 0.7 | 2 | - | - |
| female | 88.1 ± 3.2 | 61 | 85.3 ± 4.4 | 33 | 0.005 | 0.76 | |
| Ferritin | male | 115.8 ± 51.1 | 106 | 29.1 ± 16.6 | 2 | - | - |
| female | 84.5 ± 68.0 | 61 | 19.0 ± 8.9 | 33 | <0.001 | 1.18 | |
| Eisen | male | 110.2 ± 41.9 | 106 | 86.5 ± 50.2 | 2 | - | - |
| female | 117.3 ± 49.0 | 61 | 97.6 ± 55.2 | 33 | 0.078 | - | |
| Transferrin | male | 259.4 ± 32.2 | 106 | 257.0 ± 33.9 | 2 | - | - |
| female | 269.8 ± 40.5 | 61 | 328.3 ± 64.9 | 33 | <0.001 | −1.15 | |
| Lösl. Rezeptor | male | - | 3.30 | 1 | - | - | |
| female | 2.20 ± 0.36 | 7 | 3.24 ± 1.19 | 32 | 0.006 | −0.93 | |
| Trans.Sättigung | male | 30.2 ± 11.2 | 106 | 25.0 ± 17.1 | 2 | - | - |
| female | 31.6 ± 14.3 | 61 | 21.7 ± 12.4 | 33 | 0.001 | 0.72 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roy, R.; Kück, M.; Radziwolek, L.; Kerling, A. Iron Deficiency in Adolescent and Young Adult German Athletes—A Retrospective Study. Nutrients 2022, 14, 4511. https://doi.org/10.3390/nu14214511
Roy R, Kück M, Radziwolek L, Kerling A. Iron Deficiency in Adolescent and Young Adult German Athletes—A Retrospective Study. Nutrients. 2022; 14(21):4511. https://doi.org/10.3390/nu14214511
Chicago/Turabian StyleRoy, Rubina, Momme Kück, Lukas Radziwolek, and Arno Kerling. 2022. "Iron Deficiency in Adolescent and Young Adult German Athletes—A Retrospective Study" Nutrients 14, no. 21: 4511. https://doi.org/10.3390/nu14214511
APA StyleRoy, R., Kück, M., Radziwolek, L., & Kerling, A. (2022). Iron Deficiency in Adolescent and Young Adult German Athletes—A Retrospective Study. Nutrients, 14(21), 4511. https://doi.org/10.3390/nu14214511