
Postoperative Dehydration Is Associated with Frailty and Decreased Survival in Older Patients with Hip Fracture


Abstract
:1. Introduction
2. Materials and Methods
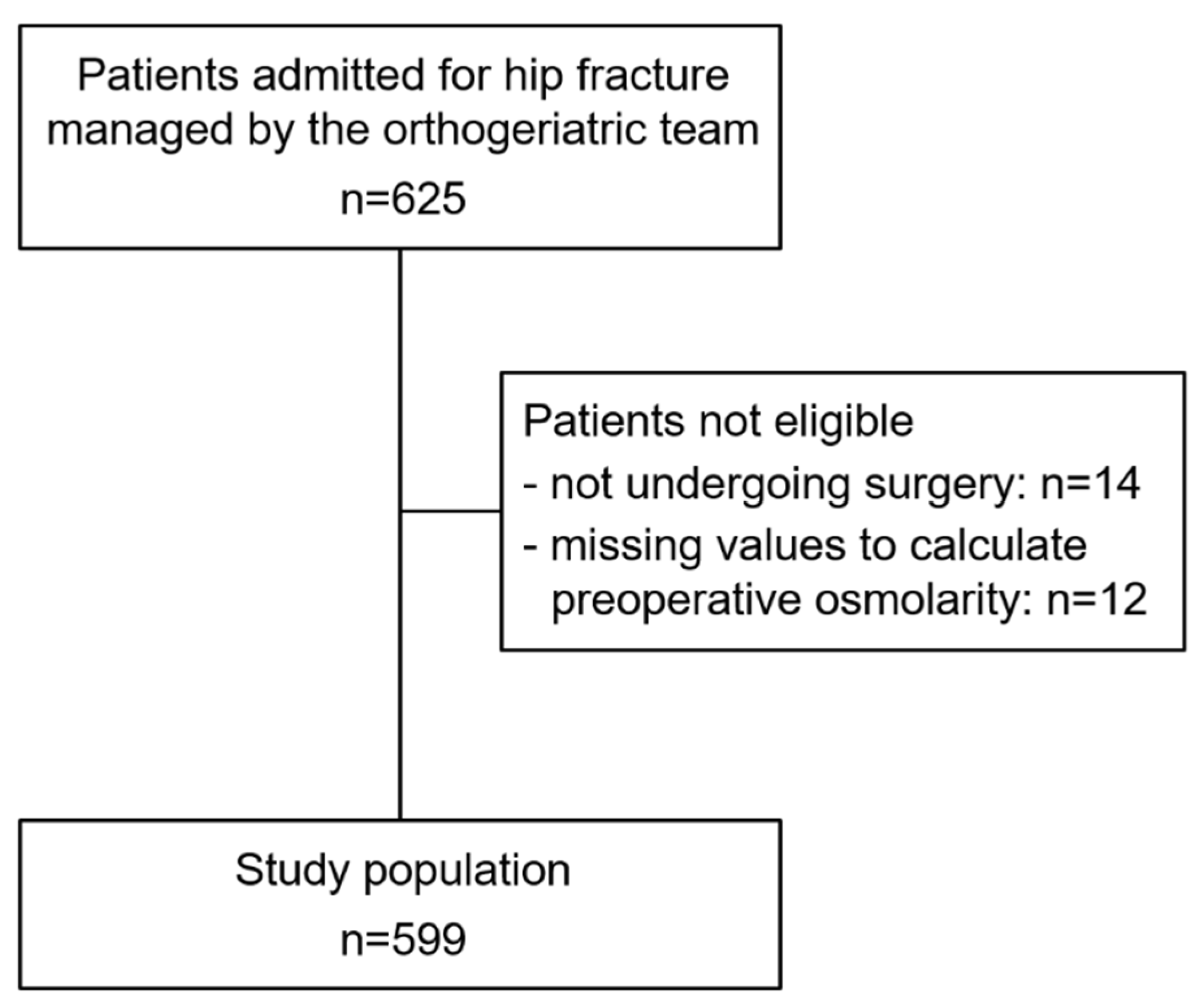
2.1. Study Design, Setting and Population
2.2. Study Variables
2.3. Study End-Points
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khan, M.A.; Hossain, F.S.; Dashti, Z.; Muthukumar, N. Causes and predictors of early re-admission after surgery for a fracture of the hip. J. Bone Jt. Surg. 2012, 94, 690–697. [Google Scholar] [CrossRef]
- Sheehan, K.J.; Guerrero, E.M.; Tainter, D.; Dial, B.; Milton-Cole, R.; Blair, J.A.; Alexander, J.; Swamy, P.; Kuramoto, L.; Guy, P.; et al. Prognostic factors of in-hospital complications after hip fracture surgery: A scoping review. Osteoporos. Int. 2019, 30, 1339–1351. [Google Scholar] [CrossRef]
- Sheehan, K.J.; Williamson, L.; Alexander, J.; Filliter, C.; Sobolev, B.; Guy, P.; Bearne, L.M.; Sackley, C. Prognostic factors of functional outcome after hip fracture surgery: A systematic review. Age Ageing 2018, 47, 661–670. [Google Scholar] [CrossRef] [Green Version]
- Ekman, L.; Johnson, P.; Hahn, R.G. Signs of dehydration after hip fracture surgery: An observational descriptive study. Medicina 2020, 56, 361. [Google Scholar] [CrossRef]
- Hahn, R.G. Renal injury during hip fracture surgery: An exploratory study. Anaesthesiol. Intensive Ther. 2015, 47, 284–290. [Google Scholar] [CrossRef] [Green Version]
- Ylienvaara, S.; Elisson, O.; Berg, K.; Zdolsek, J.H.; Krook, H.; Hahn, R.G. Preoperative urine-specific weight and the incidence of complications after hip fracture surgery. A prospective, observational study. Eur. J. Anaesthesiol. 2014, 31, 85–90. [Google Scholar] [CrossRef]
- Adunsky, A.; Mizrahi, E.H.; Kaplan, A.; Purits, E.; Waitzman, A.; Arad, M. Elevated blood urea, independent of glomerular filtration rate (GFR), confers increased risk of adverse functional outcome in elderly hip fracture patients. Arch. Gerontol. Geriatr. 2011, 53, e174–e178. [Google Scholar] [CrossRef]
- Docherty, N.G.; Delles, C.; D’Haese, P.; Layton, A.T.; Martínez-Salgado, C.; Vervaet, B.A.; López-Hernández, F.J. Haemodynamic frailty—A risk factor for acute kidney injury in the elderly. Ageing Res. Rev. 2021, 70, 101408. [Google Scholar] [CrossRef]
- Xu, B.Y.; Yan, S.; Low, L.L.; Vasanwala, F.F.; Low, S.G. Predictors of poor functional outcomes and mortality in patients with hip fracture: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 568. [Google Scholar] [CrossRef]
- Collin, C.; Bimou, C.; Mabit, C.; Tchalla, A.; Charissoux, J.L.; Marcheix, P.S. Orthogeriatric assessment of patients over 75 years of age with a proximal femur fracture: Predictors of 6-month mortality. Orthop. Traumatol. Surg. Res. 2020, 106, 1441–1447. [Google Scholar] [CrossRef]
- Pilotto, A.; Custodero, C.; Maggi, S.; Polidori, M.C.; Veronese, N.; Ferrucci, L. A multidimensional approach to frailty in older people. Ageing Res. Rev. 2020, 60, 101047. [Google Scholar] [CrossRef]
- Pioli, G.; Bendini, C.; Pignedoli, P.; Giusti, A.; Marsh, D. Orthogeriatric co-management—managing frailty as well as fragility. Injury 2018, 49, 1398–1402. [Google Scholar] [CrossRef]
- Katsoulis, M.; Benetou, V.; Karapetyan, T.; Feskanich, D.; Grodstein, F.; Pettersson-Kymmer, U.; Eriksson, S.; Wilsgaard, T.; Jørgensen, L.; Ahmed, L.A.; et al. Excess mortality after hip fracture in elderly persons from Europe and the USA: The CHANCES project. J. Intern. Med. 2017, 281, 300–310. [Google Scholar] [CrossRef]
- Van Heghe, A.; Mordant, G.; Dupont, J.; Dejaeger, M.; Laurent, M.R.; Gielen, E. Effects of orthogeriatric care models on outcomes of hip fracture patients: A systematic review and meta-analysis. Calcif. Tissue Int. 2022, 110, 162–184. [Google Scholar] [CrossRef] [PubMed]
- Kusen, J.Q.; Schafroth, B.; Poblete, B.; van der Vet, P.C.R.; Link, B.C.; Wijdicks, F.J.G.; Babst, R.H.; Beeres, F.J.P. The implementation of a Geriatric Fracture Centre for hip fractures to reduce mortality and morbidity: An observational study. Arch. Orthop. Trauma Surg. 2019, 139, 1705–1712. [Google Scholar] [CrossRef]
- Prestmo, A.; Hagen, G.; Sletvold, O.; Helbostad, J.L.; Thingstad, P.; Taraldsen, K.; Lydersen, S.; Halsteinli, V.; Saltnes, T.; Lamb, S.E.; et al. Comprehensive geriatric care for patients with hip fractures: A prospective, randomised, controlled trial. Lancet 2015, 385, 1623–1633. [Google Scholar] [CrossRef] [Green Version]
- Salvador-Marín, J.; Ferrández-Martínez, F.J.; Lawton, C.D.; Orozco-Beltrán, D.; Martínez-López, J.F.; Kelly, B.T.; Marzo-Campos, J.C. Efficacy of a multidisciplinary care protocol for the treatment of operated hip fracture patients. Sci. Rep. 2021, 11, 24082. [Google Scholar] [CrossRef]
- Khajuria, A.; Krahn, J. Osmolality revisited—Deriving and validating the best formula for calculated osmolality. Clin. Biochem. 2005, 38, 514–519. [Google Scholar] [CrossRef]
- Hooper, L.; Abdelhamid, A.; Ali, A.; Bunn, D.K.; Jennings, A.; John, W.G.; Kerry, S.; Lindner, G.; Pfortmueller, C.A.; Sjöstrand, F.; et al. Diagnostic accuracy of calculated serum osmolarity to predict dehydration in older people: Adding value to pathology laboratory reports. BMJ Open 2015, 5, e008846. [Google Scholar] [CrossRef] [Green Version]
- Munk, T.; Bech, C.B.; Klausen, T.W.; Rønholt, F.; Suetta, C.; Knudsen, A.W. Accuracy of the calculated serum osmolarity to screen for hyperosmolar dehydration in older hospitalised medical patients. Clin. Nutr. 2021, 43, 415–419. [Google Scholar] [CrossRef]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2019, 38, 10–47. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Warnier, R.M.; van Rossum, E.; van Velthuijsen, E.; Mulder, W.J.; Schols, J.M.; Kempen, G.I. Validity, Reliability and feasibility of tools to identify frail older patients in inpatient hospital care: A systematic review. J. Nutr. Health Aging 2016, 20, 218–230. [Google Scholar] [CrossRef]
- Pilotto, A.; Ferrucci, L.; Franceschi, M.; D’Ambrosio, L.P.; Scarcelli, C.; Cascavilla, L.; Paris, F.; Placentino, G.; Seripa, D.; Dallapiccola, B.; et al. Development and validation of a multidimensional prognostic index for one-year mortality from comprehensive geriatric assessment in hospitalized older patients. Rejuvenation Res. 2008, 11, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Budzynski, J.; Tojek, K.; Czerniak, B.; Banaszkiewicz, Z. Scores of nutritional risk and parameters of nutritional status assessment as predictors of in-hospital mortality and readmissions in the general hospital population. Clin. Nutr. 2016, 35, 1464–1471. [Google Scholar] [CrossRef] [PubMed]
- Kusen, J.Q.; van der Vet, P.C.R.; Wijdicks, F.J.G.; Link, B.C.; Poblete, B.; van der Velde, D.; Babst, R.; Beeres, F.J.P. Does preoperative hemodynamic preconditioning improve morbidity and mortality after traumatic hip fracture in geriatric patients? A retrospective cohort study. Arch. Orthop. Trauma Surg. 2021, 141, 1491–1497. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Abdelhamid, A.; Attreed, N.J.; Campbell, W.W.; Channell, A.M.; Chassagne, P.; Culp, K.R.; Fletcher, S.J.; Fortes, M.B.; Fuller, N.; et al. Clinical symptoms, signs and tests for identification of impending and current water-loss dehydration in older people. Cochrane Database Syst. Rev. 2015, 2015, Cd009647. [Google Scholar] [CrossRef] [Green Version]
- Löffel, L.M.; Engel, D.A.; Beilstein, C.M.; Hahn, R.G.; Furrer, M.A.; Wuethrich, P.Y. Dehydration before major urological surgery and the perioperative pattern of plasma creatinine: A prospective cohort series. J. Clin. Med. 2021, 10, 5817. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Bunn, D.K.; Downing, A.; Jimoh, F.O.; Groves, J.; Free, C.; Cowap, V.; Potter, J.F.; Hunter, P.R.; Shepstone, L. Which Frail Older People Are Dehydrated? The UK DRIE Study. J. Gerontology. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1341–1347. [Google Scholar] [CrossRef] [Green Version]
- Lancaster, K.J.; Smiciklas-Wright, H.; Heller, D.A.; Ahern, F.M.; Jensen, G. Dehydration in black and white older adults using diuretics. Ann. Epidemiol. 2003, 13, 525–529. [Google Scholar] [CrossRef]
- Zanetti, M.; Marzaro, G.; De Colle, P.; Toigo, G.; Bianchini, D.; Nastri, M.; Suriano, C.; Barazzoni, R.; Sanson, G. Predictors of short- and long-term mortality among acutely admitted older patients: Role of inflammation and frailty. Aging Clin. Exp. Res. 2021, 34, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Van Pottelbergh, G.; Den Elzen, W.P.; Degryse, J.; Gussekloo, J. Prediction of mortality and functional decline by changes in eGFR in the very elderly: The Leiden 85-plus study. BMC Geriatr. 2013, 13, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | n | All | no-HD | HD | p-Value |
|---|---|---|---|---|---|
| Age (years) | 599 | 84.0; 79.0–90.0 | 85.0; 78.0–90.0 | 84.0; 80.0–90.0 | 0.621 |
| Age > 85 years | 599 | 267 (44.6%) | 214 (44.9%) | 53 (43.4%) | 0.778 |
| Sex (male) | 599 | 151 (25.2%) | 121 (25.4%) | 30 (24.6%) | 0.860 |
| Living in a nursing home | 598 | 114 (19.1%) | 98 (20.5%) | 16 (13.2%) | 0.067 |
| Body Mass Index (kg/m2) | 598 | 23.1; 20.9–25.7 | 22.7; 20.8–25.0 | 24.5; 22.2–28.4 | <0.001 |
| Multidimensional Prognostic Index | 596 | 0.50; 0.37–0.63 | 0.50; 0.36–0.63 | 0.50; 0.38–0.63 | 0.335 |
| Main comorbid conditions | 599 | ||||
| Arterial hypertension | 599 | 361 (60.3%) | 269 (56.4%) | 92 (75.4%) | <0.001 |
| Chronic heart failure | 599 | 95 (15.9%) | 68 (14.3%) | 27 (22.1%) | 0.034 |
| Chronic kidney disease | 599 | 76 (12.7%) | 45 (9.4%) | 31 (25.4%) | <0.001 |
| Cognitive impairment (severe) | 597 | 143 (23.9%) | 119 (24.9%) | 24 (20.0%) | 0.256 |
| COPD | 599 | 61 (10.2%) | 49 (10.3%) | 12 (9.8%) | 0.887 |
| Diabetes mellitus | 599 | 122 (20.4%) | 88 (18.4%) | 34 (27.9%) | 0.021 |
| Hypertensive heart disease | 599 | 124 (20.7%) | 92 (19.3%) | 32 (26.2%) | 0.091 |
| Ischemic heart disease | 599 | 112 (18.7%) | 86 (18.0%) | 26 (21.3%) | 0.407 |
| Valvular heart disease | 599 | 74 (12.4%) | 60 (12.6%) | 14 (11.5%) | 0.741 |
| Relevant home therapy | 599 | ||||
| Number of medications | 599 | 4.0; 2.0–6.0 | 4.0; 2.0–6.0 | 5.0; 2.0–7.0 | 0.021 |
| Polipharmacy (>4 drugs) | 599 | 266 (44.4%) | 199 (41.7%) | 67 (54.9%) | 0.009 |
| Diuretics | 599 | 190 (31.7%) | 130 (27.3%) | 60 (49.2%) | <0.001 |
| Anti hypertensives | 599 | 347 (57.9%) | 260 (54.5%) | 87 (71.3%) | 0.001 |
| Neuroleptics/benzodiazepines | 599 | 231 (38.6%) | 189 (39.6%) | 42 (34.4%) | 0.293 |
| Steroids | 599 | 19 (3.2%) | 14 (2.9%) | 5 (4.1%) | 0.513 |
| Preoperative laboratory blood tests | 599 | ||||
| eGFR (mL/min/1.73 m2) | 599 | 71.6; 54.9–89.3 | 75.7; 60.2–93.0 | 53.9; 38.0–70.6 | <0.001 |
| Urea (mmol/L) | 599 | 7.3; 5.8–9.9 | 6.8; 5.3–8.7 | 11.2; 8.5–13.5 | <0.001 |
| Sodium (mmol/L) | 599 | 138.0; 136.0–140.0 | 137.0; 135.0–139.0 | 140.0; 138.0–141.0 | <0.001 |
| Potassium (mmol/L) | 599 | 4.0; 3.7–4.3 | 4.0; 3.7–4.3 | 4.2; 3.9–4.6 | <0.001 |
| Fasting glucose (mmol/L) | 599 | 7.1; 6.3–8.3 | 7.0; 6.2–8.1 | 7.9; 6.6–9.7 | <0.001 |
| Serum osmolarity (mmol/L) | 599 | 295.0; 290.5–299.3 | 293.1; 289.6–296.4 | 303.7; 302.0–305.6 | <0.001 |
| Hemoglobin (g/dL) | 599 | 11.9; 10.6–13.2 | 12.0; 10.7–13.3 | 11.4; 10.3–12.9 | 0.007 |
| Total protein (g/dL) | 514 | 6.2; 5.8–6.6 | 6.2; 5.8–6.6 | 6.1; 5.8–6.5 | 0.489 |
| Albumin (g/dL) | 538 | 3.5; 3.2–3.7 | 3.5; 3.2–3.7 | 3.5; 3.3–3.7 | 0.401 |
| C-reactive protein (mg/L) | 562 | 19.9; 6.5–63.2 | 19.4; 6.2–62.2 | 21.0; 7.1–78.0 | 0.126 |
| Lymphocytes (cells × 103/mL) | 522 | 1.1; 0.8–1.5 | 1.1; 0.8–1.5 | 1.1; 0.8–1.4 | 0.247 |
| Glasgow Prognostic Score = 2 | 516 | 186 (31.1%) | 152 (37.0%) | 34 (32.4%) | 0.381 |
| Variable | n | no-HD | HD | p-Value |
|---|---|---|---|---|
| Age > 85 years | 595 | 206 (41.5%) | 58 (58.6%) | 0.002 |
| Sex (male) | 595 | 119 (24.0%) | 30 (30.3%) | 0.186 |
| Surgery after two or more days | 595 | 128 (25.8%) | 40 (40.4%) | 0.003 |
| Type of surgery | 595 | 0.953 | ||
| Osteosyntesis | 294 (59.3%) | 59 (59.6%) | ||
| Arthroplasty | 202 (40.7%) | 40 (40.4%) | ||
| Blood transfusions | 590 | 207 (42.0%) | 52 (53.6%) | 0.035 |
| Postoperative complications | ||||
| Blood glucose imbalance | 590 | 5 (1.0%) | 1 (1.0%) | 1.000 |
| Delirium | 590 | 54 (11.0%) | 14 (14.4%) | 0.327 |
| Electrolyte imbalance | 590 | 101 (20.5%) | 29 (29.9%) | 0.041 |
| Heart failure exacerbation | 590 | 37 (7.5%) | 15 (15.5%) | 0.011 |
| Pneumonia | 590 | 11 (2.2%) | 8 (8.2%) | 0.002 |
| Pressure ulcers | 595 | 0 (0.0%) | 2 (2.1%) | 0.027 |
| Respiratory failure | 590 | 22 (4.5%) | 9 (9.3%) | 0.052 |
| Sepsis | 590 | 3 (0.6%) | 0 (0.0%) | 1.000 |
| Surgical wound infection | 590 | 0 (0.0%) | 0 (0.0%) | n.c. |
| Urinary tract infections | 590 | 19 (3.9%) | 5 (5.2%) | 0.572 |
| Variables | B | SE (95% CI) | β | p-Value |
|---|---|---|---|---|
| Postoperative HD | 0.083 | 0.021 (0.042–0.125) | 0.171 | <0.001 |
| Glasgow Prognostic Score | 0.050 | 0.017 (0.017–0.082) | 0.130 | 0.003 |
| Multidimensional prognostic index | −0.051 | 0.019 (−0.088–−0.013) | −0.117 | 0.008 |
| Sex (male) | 0.044 | 0.018 (0.008–0.080) | 0.103 | 0.018 |
| Dependent Variable | Predictor | Unadjusted Risk a χ2; p-Value | Adjusted Risk b HR (95% CI); p-Value |
|---|---|---|---|
| 30-day mortality | Postoperative HD | 6.510; 0.011 | n.s. |
| MPI-severe risk | 4.840 (1.896–12.360); 0.001 | ||
| GPS-poor prognosis | 4.298 (1.539–12.000); 0.005 | ||
| 60-day mortaility | Postoperative HD | 15.429; <0.001 | 3.084 (1.624–5.854); 0.001 |
| MPI-severe risk | 3.322 (1.760–6.272); 0.001 | ||
| GPS-poor prognosis | 3.312 (1.720–6.377); <0.001 | ||
| Sex | 2.269 (1.188–4.333); 0.013 | ||
| 90-days mortality | Postoperative HD | 17.015; <0.001 | 3.155 (1.723–5.775); <0.001 |
| MPI-severe risk | 3.267 (1.795–5.945); <0.001 | ||
| GPS-poor prognosis | 2.997 (1.632–5.503); <0.001 | ||
| Sex | 2.529 (1.384–4.623); 0.003 | ||
| 180-days mortality | Postoperative HD | 12.339; <0.001 | 2.392 (1.429–4.002); 0.001 |
| MPI-severe risk | 3.646 (2.244–5.926); <0.001 | ||
| GPS-poor prognosis | 2.689 (1.652–4.379); <0.001 | ||
| Sex | 2.016 (1.212–3.356); 0.007 | ||
| 365-days mortality | Postoperative HD | 5.522; 0.019 | 1.655 (1.056–2.594); 0.028 |
| MPI-severe risk | 3.502 (2.365–5.186); <0.001 | ||
| GPS-poor prognosis | 1.818 (1.234–2.678); 0.002 | ||
| Sex | 2.159 (1.437–3.244); <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanetti, M.; De Colle, P.; Omiciuolo, C.; Ratti, C.; Gortan Cappellari, G.; Barazzoni, R.; Murena, L.; Sanson, G. Postoperative Dehydration Is Associated with Frailty and Decreased Survival in Older Patients with Hip Fracture. Nutrients 2022, 14, 820. https://doi.org/10.3390/nu14040820
Zanetti M, De Colle P, Omiciuolo C, Ratti C, Gortan Cappellari G, Barazzoni R, Murena L, Sanson G. Postoperative Dehydration Is Associated with Frailty and Decreased Survival in Older Patients with Hip Fracture. Nutrients. 2022; 14(4):820. https://doi.org/10.3390/nu14040820
Chicago/Turabian StyleZanetti, Michela, Paolo De Colle, Cinzia Omiciuolo, Chiara Ratti, Gianluca Gortan Cappellari, Rocco Barazzoni, Luigi Murena, and Gianfranco Sanson. 2022. "Postoperative Dehydration Is Associated with Frailty and Decreased Survival in Older Patients with Hip Fracture" Nutrients 14, no. 4: 820. https://doi.org/10.3390/nu14040820
APA StyleZanetti, M., De Colle, P., Omiciuolo, C., Ratti, C., Gortan Cappellari, G., Barazzoni, R., Murena, L., & Sanson, G. (2022). Postoperative Dehydration Is Associated with Frailty and Decreased Survival in Older Patients with Hip Fracture. Nutrients, 14(4), 820. https://doi.org/10.3390/nu14040820