
An Active Image-Based Mobile Food Record Is Feasible for Capturing Eating Occasions among Infants Ages 3–12 Months Old in Hawai‘i

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Participants
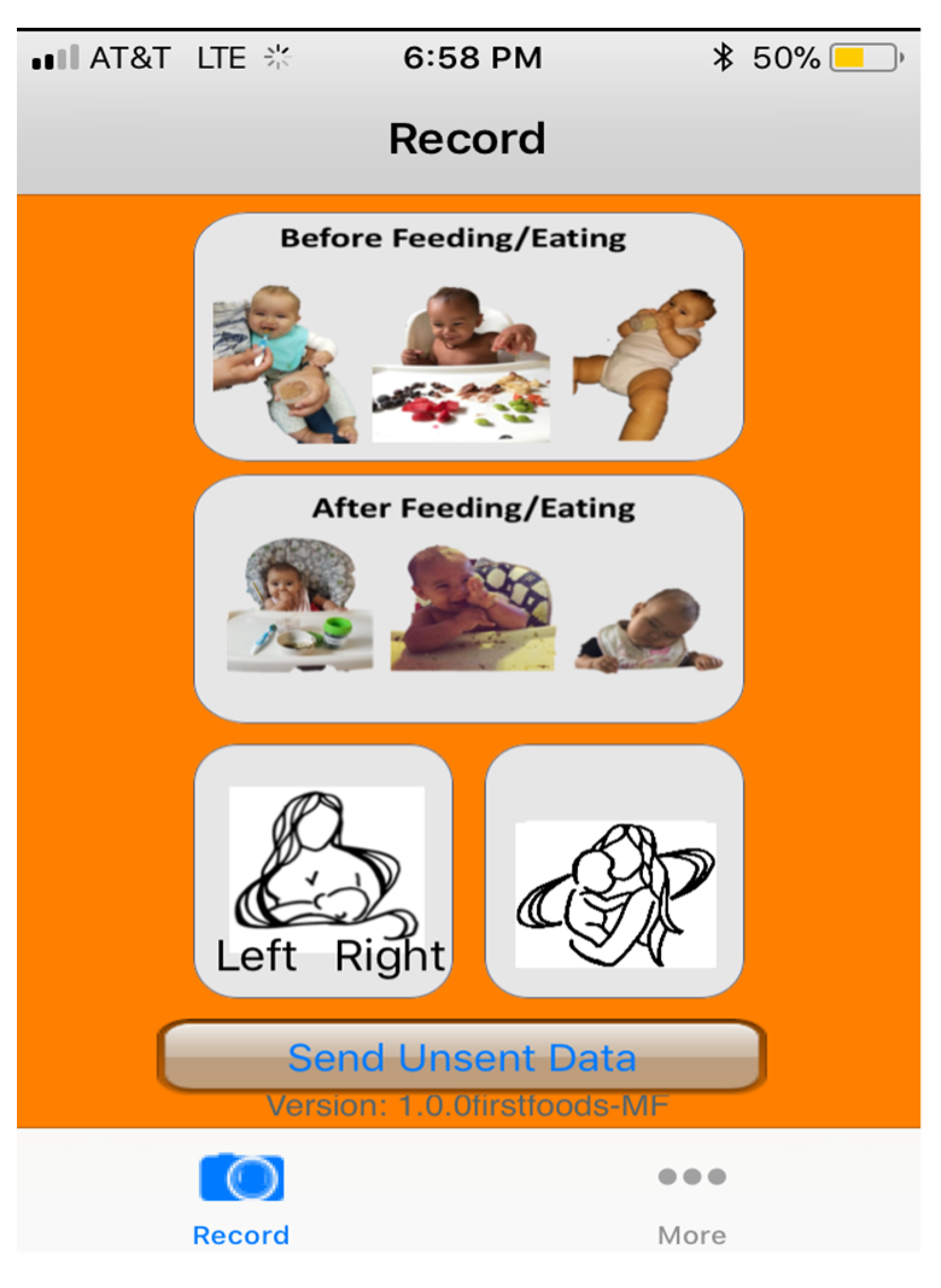
3.2. Mobile Food Record
3.3. Surrogate Reporter Feedback
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Questions |
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
References
- Mascarenhas, M.R.; Zemel, B.; Stallings, V.A. Nutritional assessment in pediatrics. Nutrition 1998, 14, 105–115. [Google Scholar] [CrossRef]
- Burrows, T.; Goldman, S.; Rollo, M. A systematic review of the validity of dietary assessment methods in children when compared with the method of doubly labelled water. Eur. J. Clin. Nutr. 2020, 74, 669–681. [Google Scholar] [CrossRef] [PubMed]
- Boushey, C.J.; Spoden, M.; Zhu, F.M.; Delp, E.J.; Kerr, D.A. New mobile methods for dietary assessment: Review of image-assisted and image-based dietary assessment methods. Proc. Nutr. Soc. 2017, 76, 283–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, F.; Mariappan, A.; Boushey, C.J.; Kerr, D.; Lutes, K.D.; Ebert, D.S.; Delp, E.J. Technology-assisted dietary assessment. Proc. SPIE Int. Soc. Opt. Eng. 2008, 6814, 681411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, F.; Bosch, M.; Woo, I.; Kim, S.; Boushey, C.J.; Ebert, D.S.; Delp, E.J. The use of mobile devices in aiding dietary assessment and evaluation. IEEE J. Sel. Top. Signal. Process. 2010, 4, 756–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Six, B.L.; Schap, T.E.; Zhu, F.M.; Mariappan, A.; Bosch, M.; Delp, E.J.; Ebert, D.S.; Kerr, D.A.; Boushey, C.J. Evidence-based development of a mobile telephone food record. J. Am. Diet. Assoc. 2010, 110, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, Z.; Bosch, M.; Khanna, N.; Kerr, D.A.; Boushey, C.J.; Zhu, F.; Delp, E.J. A mobile food record for integrated dietary assessment. In Proceedings of the 2nd International Workshop on Multimedia Assisted Dietary Management, Amsterdam, The Netherlands, 16 October 2016; pp. 53–62. [Google Scholar] [CrossRef] [Green Version]
- He, J.; Shao, Z.; Wright, J.; Kerr, D.; Boushey, C.; Zhu, F. Multi-task image-based dietary assessment for food recognition and portion size estimation. In Proceedings of the IEEE Conference on Multimedia Information Processing and Retrieval, Shenzhen, China, 6–8 August 2020; pp. 49–54. [Google Scholar] [CrossRef]
- Daugherty, B.L.; Schap, T.E.; Ettienne-Gittens, R.; Zhu, F.M.; Bosch, M.; Delp, E.J.; Ebert, D.S.; Kerr, D.A.; Boushey, C.J. Novel technologies for assessing dietary intake: Evaluating the usability of a mobile telephone food record among adults and adolescents. J. Med. Internet Res. 2012, 14, e58. [Google Scholar] [CrossRef]
- Aflague, T.F.; Boushey, C.J.; Guerrero, R.T.; Ahmad, Z.; Kerr, D.A.; Delp, E.J. Feasibility and use of the mobile food record for capturing eating occasions among children ages 3–10 years in Guam. Nutrients 2015, 7, 4403–4415. [Google Scholar] [CrossRef] [Green Version]
- Zhu, F.; Bosch, M.; Khanna, N.; Boushey, C.J.; Delp, E.J. Multiple hypotheses image segmentation and classification with application to dietary assessment. IEEE J. Biomed. Health Inform. 2015, 19, 377–388. [Google Scholar] [CrossRef] [Green Version]
- Boushey, C.J.; Spoden, M.; Delp, E.J.; Zhu, F.; Bosch, M.; Ahmad, Z.; Shvetsov, Y.B.; DeLany, J.P.; Kerr, D.A. Reported energy intake accuracy compared to doubly labeled water and usability of the mobile food record among community dwelling adults. Nutrients 2017, 9, 312. [Google Scholar] [CrossRef]
- Kerr, D.A.; Harray, A.J.; Pollard, C.M.; Dhaliwal, S.S.; Delp, E.J.; Howat, P.A.; Pickering, M.R.; Ahmad, Z.; Meng, X.; Pratt, I.S.; et al. The connecting health and technology study: A 6-month randomized controlled trial to improve nutrition behaviours using a mobile food record and text messaging support in young adults. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bathgate, K.E.; Sherriff, J.L.; Leonard, H.; Dhaliwal, S.S.; Delp, E.J.; Boushey, C.J.; Kerr, D.A. Feasibility of assessing diet with a mobile food record for adolescents and young adults with down syndrome. Nutrients 2017, 9, 273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pew Research Center. Mobile Fact Sheet. Available online: http://www.pewinternet.org/fact-sheet/mobile/ (accessed on 27 October 2021).
- Arain, M.; Campbell, M.J.; Cooper, C.L.; Lancaster, G.A. What is a pilot or feasibility study? A review of current practice and editorial policy. BMC Med. Res. Methodol. 2010, 10, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, U.; Venables, M.; Ohlund, I.; Lind, T. Active image-assisted food records in comparison to regular food records: A validation study against doubly labeled water in 12-month-old infants. Nutrients 2018, 10, 1904. [Google Scholar] [CrossRef] [Green Version]
- Fialkowski, M.K.; Ng-Osorio, J.; Kai, J.; Swafford, K.; Langfelder, G.; Young, C.G.; Chen, J.J.; Zhu, F.M.; Boushey, C.J. Type, timing, and diversity of complementary foods among native Hawaiian, Pacific Islander, and Filipino infants. Hawaii J. Health Soc. Welf. 2020, 79, 127–134. [Google Scholar]
- Xu, C.; Zhu, F.; Khanna, N.; Boushey, C.J.; Delp, E.J. Image enhancement and quality measures for dietary assessment using mobile devices. Proc. SPIE Int. Soc. Opt. Eng. 2012, 8296, 153–162. [Google Scholar] [CrossRef] [Green Version]
- Shoneye, C.L.; Dhaliwal, S.S.; Pollard, C.M.; Boushey, C.J.; Delp, E.J.; Harray, A.J.; Howat, P.A.; Hutchesson, M.J.; Rollo, M.E.; Zhu, F.; et al. Image-based dietary assessment and tailored feedback using mobile technology: Mediating behavior change in young adults. Nutrients 2019, 11, 435. [Google Scholar] [CrossRef] [Green Version]
- Bailey, R.L.; Stang, J.S.; Davis, T.A.; Naimi, T.S.; Schneeman, B.O.; Dewey, K.G.; Donovan, S.M.; Novotny, R.; Kleinman, R.E.; Taveras, E.M.; et al. Dietary and complementary feeding practices of US infants, 6 to 12 months: A narrative review of the federal nutrition monitoring data. J. Acad. Nutr. Diet. 2021; in press. [Google Scholar] [CrossRef]
- Scanlon, K.S.; Alexander, M.P.; Serdula, M.K.; Davis, M.K.; Bowman, B.A. Assessment of infant feeding: The validity of measuring milk intake. Nutr. Rev. 2002, 60, 235–251. [Google Scholar] [CrossRef]
- Rasmussen, K.M.; Felice, J.P.; O’Sullivan, E.J.; Garner, C.D.; Geraghty, S.R. The meaning of “Breastfeeding” is changing and so must our language about it. Breastfeed. Med. 2017, 12, 510–514. [Google Scholar] [CrossRef]
- Azad, M.B.; Vehling, L.; Chan, D.; Klopp, A.; Nickel, N.C.; McGavock, J.M.; Becker, A.B.; Mandhane, P.J.; Turvey, S.E.; Moraes, T.J.; et al. Infant feeding and weight gain: Separating breast milk from breastfeeding and formula from food. Pediatrics 2018, 142, e20181092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanigan, J.A.; Wells, J.C.; Lawson, M.S.; Lucas, A. Validation of food diary method for assessment of dietary energy and macronutrient intake in infants and children aged 6–24 months. Eur. J. Clin. Nutr. 2001, 55, 124–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The American College of Obstetricians and Gynecologists. FAQ: Breastfeeding Your Baby. Available online: https://www.acog.org/womens-health/faqs/breastfeeding-your-baby?utm_source=redirect&utm_medium=web&utm_campaign=otn#baby (accessed on 17 December 2020).
- Ghosh, R.; Mascie-Taylor, C.G.; Rosetta, L. Longitudinal study of the frequency and duration of breastfeeding in rural Bangladeshi women. Am. J. Hum. Biol. 2006, 18, 630–638. [Google Scholar] [CrossRef] [PubMed]
- da Costa, T.H.; Haisma, H.; Wells, J.C.; Mander, A.P.; Whitehead, R.G.; Bluck, L.J. How much human milk do infants consume? Data from 12 countries using a standardized stable isotope methodology. J. Nutr. 2010, 140, 2227–2232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, R.; He, J.; Shao, Z.; Yarlagadda, S.K.; Zhu, F. Visual aware hierarchy based food recognition. In International Conference on Pattern Recognition; Springer: Berlin/Heidelberg, Germany, 2021; pp. 571–598. [Google Scholar]
- Fang, S.; Shao, Z.; Kerr, D.A.; Boushey, C.J.; Zhu, F. An end-to-end image-based automatic food energy estimation technique based on learned energy distribution images: Protocol and methodology. Nutrients 2019, 11, 877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; He, Y.; Boushey, C.J.; Zhu, F.; Delp, E.J. Context based image analysis with application in dietary assessment and evaluation. Multimed. Tools Appl. 2018, 77, 19769–19794. [Google Scholar] [CrossRef]
- USDA Food and Nutrition Service. Pregnancy and Birth to 24 Months. Available online: https://www.fns.usda.gov/resource/pregnancy-and-birth-24-months (accessed on 24 May 2021).
- Raiten, D.J.; Raghavan, R.; Porter, A.; Obbagy, J.E.; Spahn, J.M. Executive summary: Evaluating the evidence base to support the inclusion of infants and children from birth to 24 mo of age in the Dietary Guidelines for Americans—“the B-24 Project”. Am. J. Clin. Nutr. 2014, 99, 663S–691S. [Google Scholar] [CrossRef] [Green Version]

| Characteristics | n (%) a |
|---|---|
| Age group | |
| 3–5 months | 14 (20) |
| 6–12 months | 56 (80) |
| Sex | |
| Boy | 38 (54) |
| Girl | 32 (46) |
| Ethnicity b | |
| Part-Native Hawaiian or Native Hawaiian | 50 (71) |
| Pacific Islander only c | 4 (6) |
| Part-Filipino or Filipino | 35 (50) |
| Currently receiving human milk | 40 (57) |
| Mode of Submission | ||||
|---|---|---|---|---|
| mFR | Text | |||
| Total Number of Images | 1114 | 66 | ||
| Before | After | Before | After | |
| Fiducial Marker | n (%) a | n (%) a | n (%) a | n (%) a |
| Absent | 165 (30) | 176 (32) | 42 (100) | 24 (100) |
| Partially Present | 65 (12) | 60 (11) | 0 (0) | 0 (0) |
| Present | 329 (59) | 319 (58) | 0 (0) | 0 (0) |
| Location of Fiducial Marker in Image | ||||
| Absent | 165 (30) | 176 (32) | 42 (100) | 24 (100) |
| Bottom-Left Corner | 198 (35) | 185 (33) | 0 (0) | 0 (0) |
| Bottom-Right Corner | 79 (14) | 70 (13) | 0 (0) | 0 (0) |
| Center Bottom | 97 (17) | 101 (18) | 0 (0) | 0 (0) |
| Center Top | 4 (1) | 6 (1) | 0 (0) | 0 (0) |
| Top-Left Corner | 9 (2) | 9 (2) | 0 (0) | 0 (0) |
| Top-Right Corner | 7 (1) | 8 (1) | 0 (0) | 0 (0) |
| Food and Beverage Visibility | ||||
| Forgot to Take an Image of Eating Occasion | 8 (1) | 36 (7) | 0 (0) | 0 (0) |
| Completely Visible | 414 (74) | 412 (74) | 36 (86) | 20 (83) |
| Partially Visible | 118 (21) | 99 (18) | 5 (12) | 4 (17) |
| Not Visible | 19 (3) | 8 (1) | 1 (2) | 0 (0) |
| Participant In Image | 30 (5) | 37 (7) | 5 (12) | 2 (8) |
| mFR Recording Day | ||||
|---|---|---|---|---|
| Variable | Thursday | Friday | Saturday | Sunday |
| Sample size (n) | 25 | 30 | 27 | 25 |
| Mean (SD) | Mean SD | Mean SD | Mean SD | |
| Number of breastfeeding events recorded | 4.9 (3.5) | 5 (3.6) | 5.6 (3.4) | 4.1 (3.1) |
| Duration of breastfeeding events in minutes | 7.0 (6.3) | 12.8 (11.8) | 17.5 (18.3) | 36.1 (48.4) |
| n (%) | n (%) | n (%) | n (%) | |
| Number of breastfeeding events <1 min | 20 (16) | 6 (4) | 18 (12) | 4 (4) |
| Number of breastfeeding events between 1 and 120 min | 102 (84) | 143 (95) | 132 (87) | 92 (89) |
| Number of breastfeeding events >120 min | 0 (0) | 1 (1) | 2 (1) | 7 (7) |
| Strongly Agree or Agree | Neither Agree or Disagree | Disagree or Strongly Disagree | |
|---|---|---|---|
| Questions | n (%) a | n (%) a | n (%) a |
| The mFR was easy to use | 66 (94) | 3 (4) | 1 (1) |
| The directions about how to use the mFR were easy to follow | 65 (93) | 3 (4) | 2 (3) |
| Knowing when to take an image of my child’s eating was easy | 65 (93) | 4 (6) | 1 (1) |
| Remembering to take an image before my child ate was easy | 50 (71) | 10 (14) | 10 (14) |
| Remembering to take an image after my child ate was easy | 45 (64) | 15 (21) | 10 (14) |
| Remembering to push the button before breastfeeding my child was easy b | 17 (25) | 10 (14) | 12 (17) |
| Remembering to push the button after breastfeeding my child was easy b | 11 (15) | 9 (13) | 19 (27) |
| I found it easy to include the fiducial marker in the picture of my child’s meals | 42 (60) | 13 (19) | 15 (22) |
| The mFR interfered with my daily activities | 2 (3) | 19 (27) | 49 (70) |
| Understanding the purpose of the mFR motivated me to use it c | 61 (87) | 7 (10) | 1 (1) |
| Overall, the mFR was a nuisance to use | 3 (4) | 19 (27) | 48 (69) |
| Overall, the mFR was enjoyable to use | 53 (76) | 16 (23) | 1 (1) |
| I would like to participate in another study using the mobile food record. | 58 (83) | 10 (14) | 2 (2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fialkowski, M.K.; Kai, J.; Young, C.; Langfelder, G.; Ng-Osorio, J.; Shao, Z.; Zhu, F.; Kerr, D.A.; Boushey, C.J. An Active Image-Based Mobile Food Record Is Feasible for Capturing Eating Occasions among Infants Ages 3–12 Months Old in Hawai‘i. Nutrients 2022, 14, 1075. https://doi.org/10.3390/nu14051075
Fialkowski MK, Kai J, Young C, Langfelder G, Ng-Osorio J, Shao Z, Zhu F, Kerr DA, Boushey CJ. An Active Image-Based Mobile Food Record Is Feasible for Capturing Eating Occasions among Infants Ages 3–12 Months Old in Hawai‘i. Nutrients. 2022; 14(5):1075. https://doi.org/10.3390/nu14051075
Chicago/Turabian StyleFialkowski, Marie K., Jessie Kai, Christina Young, Gemady Langfelder, Jacqueline Ng-Osorio, Zeman Shao, Fengqing Zhu, Deborah A. Kerr, and Carol J. Boushey. 2022. "An Active Image-Based Mobile Food Record Is Feasible for Capturing Eating Occasions among Infants Ages 3–12 Months Old in Hawai‘i" Nutrients 14, no. 5: 1075. https://doi.org/10.3390/nu14051075
APA StyleFialkowski, M. K., Kai, J., Young, C., Langfelder, G., Ng-Osorio, J., Shao, Z., Zhu, F., Kerr, D. A., & Boushey, C. J. (2022). An Active Image-Based Mobile Food Record Is Feasible for Capturing Eating Occasions among Infants Ages 3–12 Months Old in Hawai‘i. Nutrients, 14(5), 1075. https://doi.org/10.3390/nu14051075