Efficacy of FODMAP Elimination and Subsequent Blinded Placebo-Controlled Provocations in a Randomised Controlled Study in Patients with Ulcerative Colitis in Remission and Symptoms of Irritable Bowel Syndrome: A Feasibility Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
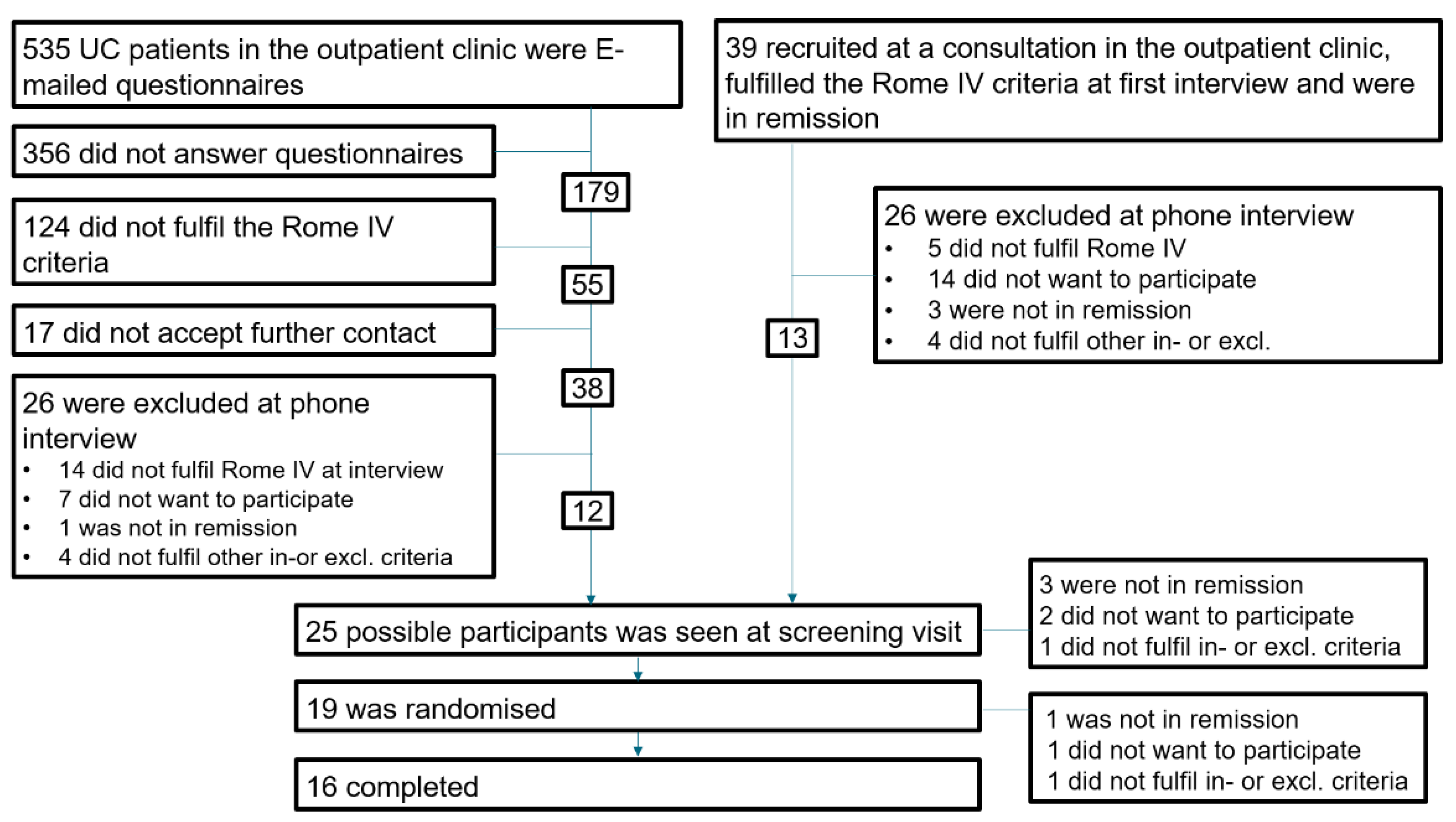
2.1. Participants
2.2. Measurements
2.3. Food Provocations
2.4. Questionnaires
2.5. Outcomes
2.6. Statistical Analysis and Bioinformatics
3. Results
3.1. Feasibility of Blinding and Adherence to Low FODMAP Diet
3.2. Primary Endpoint
3.3. Secondary Endpoints
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simrén, M.; Axelsson, J.; Gillberg, R.; Abrahamsson, H.; Svedlund, J.; Björnsson, E.S. Quality of Life in Inflammatory Bowel Disease in Remission: The Impact of IBS-like Symptoms and Associated Psychological Factors. Am. J. Gastroenterol. 2002, 97, 389–396. [Google Scholar] [CrossRef]
- Halpin, S.J.; Ford, A.C. Prevalence of Symptoms Meeting Criteria for Irritable Bowel Syndrome in Inflammatory Bowel Disease: Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2012, 107, 1474–1482. [Google Scholar] [CrossRef] [PubMed]
- Stanisic, V.; Quigley, E.M.M. The Overlap between IBS and IBD: What Is It and What Does It Mean? Expert Rev. Gastroenterol. Hepatol. 2014, 8, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Barbara, G.; Cremon, C.; Stanghellini, V. Inflammatory Bowel Disease and Irritable Bowel Syndrome: Similarities and Differences. Curr. Opin. Gastroenterol. 2014, 30, 352–358. [Google Scholar] [CrossRef]
- Mikocka-Walus, A.A.; Turnbull, D.A.; Andrews, J.M.; Moulding, N.T.; Holtmann, G.J. The Effect of Functional Gastrointestinal Disorders on Psychological Comorbidity and Quality of Life in Patients with Inflammatory Bowel Disease. Aliment. Pharmacol. Ther. 2008, 28, 475–483. [Google Scholar] [CrossRef]
- Keohane, J.; O’Mahony, C.; O’Mahony, L.; O’Mahony, S.; Quigley, E.M.; Shanahan, F. Irritable Bowel Syndrome-Type Symptoms in Patients with Inflammatory Bowel Disease: A Real Association or Reflection of Occult Inflammation? Am. J. Gastroenterol. 2010, 105, 1789–1794. [Google Scholar] [CrossRef]
- Gibson, P.R. Use of the Low-FODMAP Diet in Inflammatory Bowel Disease. J. Gastroenterol. Hepatol. 2017, 32 (Suppl. S1), 40–42. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, S.J.; Lomer, M.C.E.; Gibson, P.R. Short-Chain Carbohydrates and Functional Gastrointestinal Disorders. Am. J. Gastroenterol. 2013, 108, 707–717. [Google Scholar] [CrossRef]
- Altobelli, E.; Del Negro, V.; Angeletti, P.M.; Latella, G. Low-FODMAP Diet Improves Irritable Bowel Syndrome Symptoms: A Meta-Analysis. Nutrients 2017, 9, 940. [Google Scholar] [CrossRef]
- Krogsgaard, L.R.; Lyngesen, M.; Bytzer, P. Systematic Review: Quality of Trials on the Symptomatic Effects of the Low FODMAP Diet for Irritable Bowel Syndrome. Aliment. Pharmacol. Ther. 2017, 45, 1506–1513. [Google Scholar] [CrossRef] [Green Version]
- Halmos, E.P.; Power, V.A.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. A Diet Low in FODMAPs Reduces Symptoms of Irritable Bowel Syndrome. Gastroenterology 2014, 146, 67–75.e5. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, S.J.; Parker, F.C.; Muir, J.G.; Gibson, P.R. Dietary Triggers of Abdominal Symptoms in Patients with Irritable Bowel Syndrome: Randomized Placebo-Controlled Evidence. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2008, 6, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)-A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Chumpitazi, B.P.; Cope, J.L.; Hollister, E.B.; Tsai, C.M.; McMeans, A.R.; Luna, R.A.; Versalovic, J.; Shulman, R.J. Randomised Clinical Trial: Gut Microbiome Biomarkers Are Associated with Clinical Response to a Low FODMAP Diet in Children with the Irritable Bowel Syndrome. Aliment. Pharmacol. Ther. 2015, 42, 418–427. [Google Scholar] [CrossRef]
- Monash University. The Monash FODMAP Calculator. Available online: https://www.monashfodmapcalculator.com.au/ (accessed on 10 October 2021).
- Schroeder, K.W.; Tremaine, W.J.; Ilstrup, D.M. Coated Oral 5-Aminosalicylic Acid Therapy for Mildly to Moderately Active Ulcerative Colitis. A Randomized Study. N. Engl. J. Med. 1987, 317, 1625–1629. [Google Scholar] [CrossRef]
- Palsson, O.S.; Whitehead, W.E.; van Tilburg, M.A.L.; Chang, L.; Chey, W.; Crowell, M.D.; Keefer, L.; Lembo, A.J.; Parkman, H.P.; Rao, S.S.; et al. Rome IV Diagnostic Questionnaires and Tables for Investigators and Clinicians. Gastroenterology 2016, 150, 1481–1491. [Google Scholar] [CrossRef]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The Irritable Bowel Severity Scoring System: A Simple Method of Monitoring Irritable Bowel Syndrome and Its Progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Labus, J.S.; Bolus, R.; Chang, L.; Wiklund, I.; Naesdal, J.; Mayer, E.A.; Naliboff, B.D. The Visceral Sensitivity Index: Development and Validation of a Gastrointestinal Symptom-Specific Anxiety Scale. Aliment. Pharmacol. Ther. 2004, 20, 89–97. [Google Scholar] [CrossRef]
- Labus, J.S.; Mayer, E.A.; Chang, L.; Bolus, R.; Naliboff, B.D. The Central Role of Gastrointestinal-Specific Anxiety in Irritable Bowel Syndrome: Further Validation of the Visceral Sensitivity Index. Psychosom. Med. 2007, 69, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Svedlund, J.; Sjödin, I.; Dotevall, G. GSRS—A Clinical Rating Scale for Gastrointestinal Symptoms in Patients with Irritable Bowel Syndrome and Peptic Ulcer Disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Mangel, A.W.; Fehnel, S.E.; Drossman, D.A.; Mayer, E.A.; Talley, N.J. Primary Endpoints for Irritable Bowel Syndrome Trials: A Review of Performance of Endpoints. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2007, 5, 534–540. [Google Scholar] [CrossRef]
- Camilleri, M.; Chey, W.Y.; Mayer, E.A.; Northcutt, A.R.; Heath, A.; Dukes, G.E.; McSorley, D.; Mangel, A.M. A Randomized Controlled Clinical Trial of the Serotonin Type 3 Receptor Antagonist Alosetron in Women with Diarrhea-Predominant Irritable Bowel Syndrome. Arch. Intern. Med. 2001, 161, 1733–1740. [Google Scholar] [CrossRef] [PubMed]
- Mangel, A.W. Personal View: Adequate Relief as a Primary Endpoint in Irritable Bowel Syndrome. Aliment. Pharmacol. Ther. 2006, 23, 879–881. [Google Scholar] [CrossRef] [PubMed]
- De Vroege, L.; Hoedeman, R.; Nuyen, J.; Sijtsma, K.; van der Feltz-Cornelis, C.M. Validation of the PHQ-15 for Somatoform Disorder in the Occupational Health Care Setting. J. Occup. Rehabil. 2012, 22, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ware, J.E.J.; Sherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36). I. Conceptual Framework and Item Selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Bundgaard-Nielsen, C.; Hagstrøm, S.; Sørensen, S. Interpersonal Variations in Gut Microbiota Profiles Supersedes the Effects of Differing Fecal Storage Conditions. Sci. Rep. 2018, 8, 17367. [Google Scholar] [CrossRef]
- Team, R.C. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Charlesworth, J.E.G.; Petkovic, G.; Kelley, J.M.; Hunter, M.; Onakpoya, I.; Roberts, N.; Miller, F.G.; Howick, J. Effects of Placebos without Deception Compared with No Treatment: A Systematic Review and Meta-Analysis. J. Evid. Based. Med. 2017, 10, 97–107. [Google Scholar] [CrossRef] [Green Version]
- Jonefjäll, B.; Strid, H.; Ohman, L.; Svedlund, J.; Bergstedt, A.; Simren, M. Characterization of IBS-like Symptoms in Patients with Ulcerative Colitis in Clinical Remission. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc. 2013, 25, 756-e578. [Google Scholar] [CrossRef]
- Hustoft, T.N.; Hausken, T.; Ystad, S.O.; Valeur, J.; Brokstad, K.; Hatlebakk, J.G.; Lied, G.A. Effects of Varying Dietary Content of Fermentable Short-Chain Carbohydrates on Symptoms, Fecal Microenvironment, and Cytokine Profiles in Patients with Irritable Bowel Syndrome. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc. 2017, 29, e12969. [Google Scholar] [CrossRef] [PubMed]
- Cox, S.R.; Lindsay, J.O.; Fromentin, S.; Stagg, A.J.; McCarthy, N.E.; Galleron, N.; Ibraim, S.B.; Roume, H.; Levenez, F.; Pons, N.; et al. Effects of Low FODMAP Diet on Symptoms, Fecal Microbiome, and Markers of Inflammation in Patients with Quiescent Inflammatory Bowel Disease in a Randomized Trial. Gastroenterology 2020, 158, 176–188.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Megen, F.; Kahrs, G.E.; Hatlebakk, J.G. Effects of a FODMAP Restricted Diet in Irritable Bowel Symptoms in Patients with Inflammatory Bowel Diease. United Eur. Gastroenterol. J. 2014, 2, P0342. [Google Scholar]
- Sloan, T.J.; Jalanka, J.; Major, G.A.D.; Krishnasamy, S.; Pritchard, S.; Abdelrazig, S.; Korpela, K.; Singh, G.; Mulvenna, C.; Hoad, C.L.; et al. A Low FODMAP Diet Is Associated with Changes in the Microbiota and Reduction in Breath Hydrogen but Not Colonic Volume in Healthy Subjects. PLoS ONE 2018, 13, e0201410. [Google Scholar] [CrossRef] [Green Version]
- Spiegel, B.; Camilleri, M.; Bolus, R.; Andresen, V.; Chey, W.D.; Fehnel, S.; Mangel, A.; Talley, N.J.; Whitehead, W.E. Psychometric Evaluation of Patient-Reported Outcomes in Irritable Bowel Syndrome Randomized Controlled Trials: A Rome Foundation Report. Gastroenterology 2009, 137, 1943–1944. [Google Scholar] [CrossRef] [Green Version]
- Biesiekierski, J.R.; Peters, S.L.; Newnham, E.D.; Rosella, O.; Muir, J.G.; Gibson, P.R. No Effects of Gluten in Patients with Self-Reported Non-Celiac Gluten Sensitivity after Dietary Reduction of Fermentable, Poorly Absorbed, Short-Chain Carbohydrates. Gastroenterology 2013, 145, 320–323. [Google Scholar] [CrossRef]
- Patel, S.M.; Stason, W.B.; Legedza, A.; Ock, S.M.; Kaptchuk, T.J.; Conboy, L.; Canenguez, K.; Park, J.K.; Kelly, E.; Jacobson, E.; et al. The Placebo Effect in Irritable Bowel Syndrome Trials: A Meta-Analysis. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc. 2005, 17, 332–340. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Procedure | Screening | Visit 1 Baseline | Visit 2 | Visit 3 | Visit 4 Follow Up |
|---|---|---|---|---|---|
| Mayo Score | X | ||||
| Rome IV criteria | X | X | X | ||
| Dietician | X | ||||
| IBS-SSS | X | X | X | X | |
| SF-36 | X | X | X | X | |
| HADS | X | X | X | X | |
| GSRS | X | X | X | X | |
| VSI | X | X | X | X | |
| PHQ15 | X | X | X | X | |
| AR | X | X | X | X | |
| FODMAP frequency (daily in the week before) | X | X | X | ||
| Extra questions | X | X | X | ||
| Diet registration (3 days in the last week up to study start) | X | X | X | ||
| Symptom diary | X-------------------------------------------------------------------------X | ||||
| Calprotectin | X | X | X | X | |
| Blood sample | X | X | X | ||
| Body weight | X | X | X | X | |
| Demographics | Control Group | Low FODMAP Diet |
|---|---|---|
| n | 7 | 12 |
| m/w | 0/7 | 2/10 |
| Age (median (IQR)) | 47 (42; 48) | 38 (32; 50) |
| Caucasian | 7/7 | 12/12 |
| Weight (median (IQR)) kg | 85.0 (54.2; 93.7) | 72.4 (64.6; 87.2) |
| Debut year (median (IQR)) | 2010 (2009; 2012) | 2012 (2005; 2016) |
| Family members with CU (%) | 2 (29%) | 3 (25%) |
| Smoker (%) | 2 (29%) | 1 (8.3%) |
| Screening questionnaires | ||
| SCCAI (median (IQR)) | 3 (2; 5) | 4 (3; 5) |
| Endo Mayo score (median (IQR) | 1 (1; 1) | 1 (1; 2) |
| Missing (no endoscopy?) | 2 | 3 |
| Treatment | ||
| 5-ASA treatment (%) | 3 (43%) | 5 (42%) |
| Azathioprine (%) | 0 (0.0%) | 1 (8.3%) |
| Biologics (%) | 1 (14%) | 1 (8.3%) |
| Questionnaires at baseline, visits 2 and 3 | ||
| IBS-SSS score (median (IQR)) | 273 (248; 280) | 239 (208; 278) |
| Symptom score (average of 1 week) (median (IQR)) | 34.5 (28.5; 42.7) | 15.8 (11.5; 25.8) |
| Bristol Stool Score (average of 1 week), median (IQR)) | 4.0 (3.1; 5.0) | 5.0 (4.3; 5.2) |
| Stool frequency/day (average of 1 week) | 2.1 (1.6; 2.3) | 1.5 (1.1; 2.5) |
| GSRS score (median (IQR)) | 44 (36; 67) | 45 (36; 50) |
| SF-36 score (median (IQR)) | 75.6 (50.0; 84.7) | 76.1 (52.4; 82.1) |
| HADS score (median (IQR)) | 10 (5; 18) | 9 (4; 14) |
| VSI score (median (IQR)) | 55 (29; 63) | 54 (48; 65) |
| AR (% yes) | 6 (85.7%) | 3 (25.0%) |
| PHQ15 (median (IQR) | 12 (9; 19) | 11 (10; 16) |
| Daily FODMAP intake | ||
| GOS | 0.57 (0.54; 1.19) | 0.73 (0.61; 0.78) |
| Fructans | 4.87 (4.14; 5.57) | 4.67 (3.84;4.80) |
| Fructose | 1.23 (1.14; 2.14) | 3.15 (1.37; 30.83) |
| Lactose | 1.37 (0.70; 5.35) | 10.19 (7.04; 11.64) |
| Sorbitol | 0.36 (0.18; 2.04) | 0.38 (0.14; 1.63) |
| Mannitol | 0.03 (0.01; 0.08) | 0.06 (0.06; 0.11) |
| Low FODMAP Diet | Control Group | |||
|---|---|---|---|---|
| Provocation | After FODMAP | After Placebo | p | After 4 Weeks |
| Guessed the blinding status | 5 (56%) | 3 (33%) | >0.99 | - |
| Self-reported adherence to diet | 9 (100%) | 9 (100%) | - | - |
| Supplementary intake (median (IQR)) % | 86% (74; 95) | 93% (86; 100) | 0.40 | |
| Medication changes * | 1 (11%) | 0 (0.0%) | - | 0 (0.0%) |
| Secondary endpoints, Median (IQR) | ||||
| Weight: kg, % | −2.0 (−3.1; −0.9) | −1.0 (−2.3; −0.5) | 0.30 | 0.0 (−0.5; 0.2) |
| Change in Bristol Stool Scale score? | −0.3 (−1.0; 0.3) | −0.1 (−0.5; 0.0) | 0.30 | 0.3 (−0.2; 0.5) |
| Change in stool frequency/day | 0.0 (−0.9; 0.4) | −0.2 (−0.6; 0.0) | 0.20 | 0.3 (0.2; 0.5) |
| Change in GSRS score | −6 (−17; −3) | −7 (−11; −1) | 0.19 | −4 (−7; −0) |
| Change in SF-36 score | 3.2 (1.1; 7.5) | 2.2 (−3.5; 4.3) | 0.24 | −5.7 (−10.3; 0.3) |
| Change in HADS score | −2 (−6; −2) | 0 (−4; 0) | 0.03 | 0 (−2; 2) |
| Change in VSI score | 6 (3; 11) | −1 (−6; 7) | 0.29 | −3 (−4; 3) |
| Change in AR: No to Yes, % Yes to No, % | 3 (33%) 0 (0.0%) | 3 (33%) 0 (0.0%) | 1.00 | 0 (0.0) 3 (42.9) |
| Change in PHQ15 | −4 (−5; −2) | −4 (−4; −1) | 0.67 | 0 (−4; 2) |
| Change in FODMAPS in diet registration, % | ||||
| Index for all FODMAPs | −49% (−71; −37) | −74% (−78; −36) | 0.81 | 33% (2%; 49%) |
| Fructose | −38% (−49; −30) | −58% (−67.5; −20) | 1.00 | −13% (−29%; 37%) |
| Lactose | −96% (−99; −80) | −99% (−99; −94) | 1.00 | 166% (141%; 287%) |
| Sorbitol | −58% (−93; 147) | −91% (−100; 44) | 0.06 | −34% (−54%; 81%) |
| Mannitol | −22% (−67; −17) | −28% (−50; 9.1) | 1.00 | 200% (−10%; 325%) |
| Fructans | −32% (−47; −29) | −31% (−50; −31) | 0.81 | 0% (−26%; 23%) |
| GOS | −43% (−70; −23) | −40% (−52; −20) | 0.63 | −3% (−19%; 7%) |
| Change in FODMAPS in frequency registration, % | ||||
| Fructose | −30% (−73; 39) | −93% (−97; −90) | 0.06 | −15% (−52%; 166%) |
| Lactose | −100% (−100; −66) | −100% (−100; −57) | 0.58 | −7% (−28%; 96%) |
| Sorbitol | −83% (−92; −77) | −97% (−100; −80) | 0.69 | 20% (−25%; 196%) |
| Mannitol | −98% (−100; −37) | −100% (−100; −86) | 0.42 | −35% (−66%; 24%) |
| Fructans | −90% (−96; −56) | −89% (−93; −76) | 0.56 | 1% (−10%; 39%) |
| GOS | −83% (−98; −37) | −54% (−84; −13) | 0.69 | −1% (−33%; 5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melgaard, D.; Sørensen, J.; Riis, J.; Ovesen, T.S.; Leutscher, P.; Sørensen, S.; Knudsen, J.K.; Bundgaard-Nielsen, C.; Ejstrup, J.; Jensen, A.-M.; et al. Efficacy of FODMAP Elimination and Subsequent Blinded Placebo-Controlled Provocations in a Randomised Controlled Study in Patients with Ulcerative Colitis in Remission and Symptoms of Irritable Bowel Syndrome: A Feasibility Study. Nutrients 2022, 14, 1296. https://doi.org/10.3390/nu14061296
Melgaard D, Sørensen J, Riis J, Ovesen TS, Leutscher P, Sørensen S, Knudsen JK, Bundgaard-Nielsen C, Ejstrup J, Jensen A-M, et al. Efficacy of FODMAP Elimination and Subsequent Blinded Placebo-Controlled Provocations in a Randomised Controlled Study in Patients with Ulcerative Colitis in Remission and Symptoms of Irritable Bowel Syndrome: A Feasibility Study. Nutrients. 2022; 14(6):1296. https://doi.org/10.3390/nu14061296
Chicago/Turabian StyleMelgaard, Dorte, Jeanette Sørensen, Johannes Riis, Tine S. Ovesen, Peter Leutscher, Suzette Sørensen, Julie K. Knudsen, Caspar Bundgaard-Nielsen, Jeanette Ejstrup, Ann-Maria Jensen, and et al. 2022. "Efficacy of FODMAP Elimination and Subsequent Blinded Placebo-Controlled Provocations in a Randomised Controlled Study in Patients with Ulcerative Colitis in Remission and Symptoms of Irritable Bowel Syndrome: A Feasibility Study" Nutrients 14, no. 6: 1296. https://doi.org/10.3390/nu14061296
APA StyleMelgaard, D., Sørensen, J., Riis, J., Ovesen, T. S., Leutscher, P., Sørensen, S., Knudsen, J. K., Bundgaard-Nielsen, C., Ejstrup, J., Jensen, A. -M., Borre, M., & Krarup, A. L. (2022). Efficacy of FODMAP Elimination and Subsequent Blinded Placebo-Controlled Provocations in a Randomised Controlled Study in Patients with Ulcerative Colitis in Remission and Symptoms of Irritable Bowel Syndrome: A Feasibility Study. Nutrients, 14(6), 1296. https://doi.org/10.3390/nu14061296