
Alleviation of Pain, PAIN Interference, and Oxidative Stress by a Novel Combination of Hemp Oil, Calamari Oil, and Broccoli: A Randomized, Double-Blind, Placebo-Controlled Trial

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Investigational Product
2.3. Anthropometrics
2.4. Oxidative Stress
2.5. Self-Reported Pain
2.6. Statistics
3. Results
3.1. Subject Demographics
3.2. Tolerance Assessment
3.3. Pain Intensity
3.4. Pain Interference
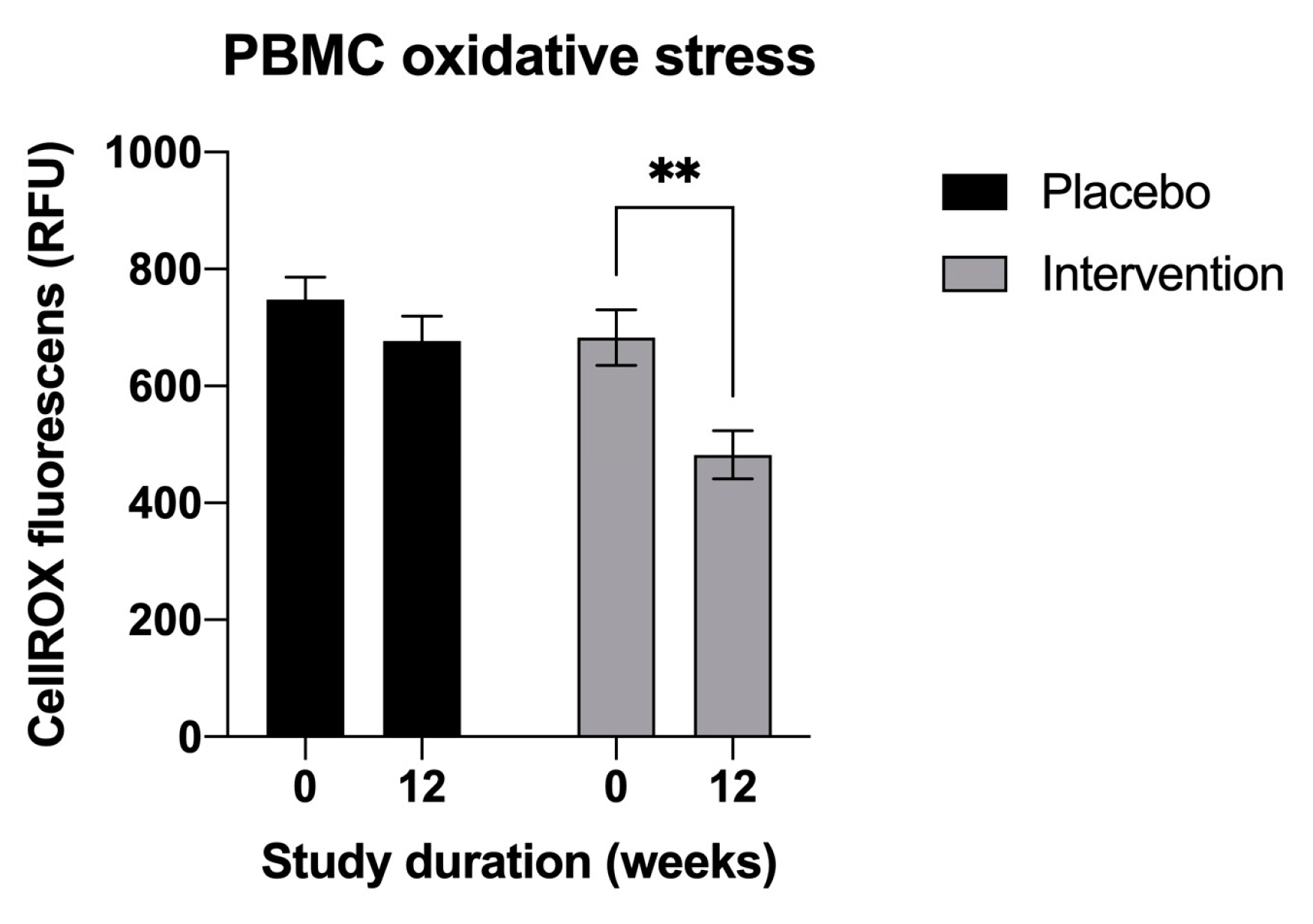
3.5. Biomarkers of Oxidative Stress
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pizzo, P.A.; Clark, N.M. Alleviating Suffering 101—Pain Relief in the United States. N. Engl. J. Med. 2012, 366, 197–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahlhamer, J.; Lucas, J.; Zelaya, C.; Nahin, R.; Mackey, S.; DeBar, L.; Kerns, R.; Von Korff, M.; Porter, L.; Helmick, C. Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults—United States, 2016. Morb. Mortal. Wkly. Rep. 2018, 67, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Volcheck, M.M.; Graham, S.M.; Fleming, K.C.; Mohabbat, A.B.; Luedtke, C.A. Central Sensitization, Chronic Pain, and Oth-er Symptoms: Better Understanding, Better Management. Cleve. Clin. J. Med. 2023, 90, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Nadeau, S.E.; Wu, J.K.; Lawhern, R.A. Opioids and Chronic Pain: An Analytic Review of the Clinical Evidence. Front. Pain Res. 2021, 2, 721357. [Google Scholar] [CrossRef] [PubMed]
- Blanco, C.; Wiley, T.R.A.; Lloyd, J.J.; Lopez, M.F.; Volkow, N.D. America’s Opioid Crisis: The Need for an Integrated Public Health Approach. Transl. Psychiatry 2020, 10, 167. [Google Scholar] [CrossRef]
- Darnall, B.D.; Scheman, J.; Davin, S.; Burns, J.W.; Murphy, J.L.; Wilson, A.C.; Kerns, R.D.; Mackey, S.C. Pain Psychology: A Global Needs Assessment and National Call to Action. Pain Med. 2016, 17, 250–263. [Google Scholar] [CrossRef] [Green Version]
- McCubbin, T.; Kempe, K.L.; Beck, A. Complementary and Alternative Medicine in an Integrated Health Care Delivery System: Users of Chiropractic, Acupuncture, and Massage Services. Perm. J. 2017, 21, 16–172. [Google Scholar] [CrossRef] [Green Version]
- LeFebvre, R.; Peterson, D.; Haas, M. Evidence-Based Practice and Chiropractic Care. J. Evid.-Based Complement. Altern. Med. 2012, 18, 75–79. [Google Scholar] [CrossRef] [Green Version]
- Coulter, I.D.; Crawford, C.; Vernon, H.; Hurwitz, E.L.; Khorsan, R.; Booth, M.S.; Herman, P.M. Manipulation and Mobiliza-tion for Treating Chronic Nonspecific Neck Pain: A Systematic Review and Meta-Analysis for an Appropriateness Panel. Pain Physician 2019, 22, E55–E70. [Google Scholar] [CrossRef]
- Masaracchio, M.; Kirker, K.; States, R.; Hanney, W.J.; Liu, X.; Kolber, M. Thoracic Spine Manipulation for the Management of Mechanical Neck Pain: A Systematic Review and Meta-Analysis. PLoS ONE 2019, 14, e0211877. [Google Scholar] [CrossRef] [Green Version]
- Fleming, S.; Rabago, D.P.; Mundt, M.P.; Fleming, M.F. CAM Therapies among Primary Care Patients Using Opioid Thera-py for Chronic Pain. BMC Complement. Altern. Med. 2007, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, A.; Townsend, C.B.; Ilyas, A.M. Medical Cannabis in Hand Surgery: A Review of the Current Evidence. J. Hand Surg. Am. 2023, 48, 292–300. [Google Scholar] [CrossRef] [PubMed]
- De Gregori, M.; Muscoli, C.; Schatman, M.E.; Stallone, T.; Intelligente, F.; Rondanelli, M.; Franceschi, F.; Arranz, L.I.; Lorente-Cebrián, S.; Salamone, M.; et al. Combining Pain Therapy with Lifestyle: The Role of Personalized Nutrition and Nutritional Supplements According to the SIMPAR Feed Your Destiny Approach. J. Pain Res. 2016, 9, 1179–1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odonkor, C.A.; AlFarra, T.; Adekoya, P.; Orhurhu, V.; Rodríguez, T.; Sottosanti, E.; Kaye, A.D. Dorsal Column Stimulation and Cannabinoids in the Treatment of Chronic Nociceptive and Neuropathic Pain: A Review of the Clinical and Pre-Clinical Data. Curr. Pain Headache Rep. 2022, 26, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Galán-Arriero, I.; Serrano-Muñoz, D.; Gómez-Soriano, J.; Goicoechea, C.; Taylor, J.; Velasco, A.; Ávila-Martín, G. The Role of Omega-3 and Omega-9 Fatty Acids for the Treatment of Neuropathic Pain after Neurotrauma. Biochim. Biophys. Acta Biomembr. 2017, 1859, 1629–1635. [Google Scholar] [CrossRef]
- Santín-Márquez, R.; Alarcón-Aguilar, A.; López-Diazguerrero, N.E.; Chondrogianni, N.; Königsberg, M. Sulforaphane—Role in Aging and Neurodegeneration. GeroScience 2019, 41, 655–670. [Google Scholar] [CrossRef]
- Komarnytsky, S.; Rathinasabapathy, T.; Wagner, C.; Metzger, B.; Carlisle, C.; Panda, C.; Le Brun-Blashka, S.; Troup, J.P.; Varadharaj, S. Endocannabinoid System and Its Regulation by Polyunsaturated Fatty Acids and Full Spectrum Hemp Oils. Int. J. Mol. Sci. 2021, 22, 5479. [Google Scholar] [CrossRef]
- Biswas, S.K. Does the Interdependence between Oxidative Stress and Inflammation Explain the Antioxidant Paradox? Oxid. Med. Cell. Longev. 2016, 2016, 5698931. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.-M.; An, J. Cytokines, Inflammation, and Pain. Int. Anesthesiol. Clin. 2007, 45, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.Z.; Wang, Y.; Cicuttini, F.M.; Hughes, H.J.; Chou, L.; Urquhart, D.M.; Ong, P.X.; Hussain, S.M. Association Between Inflammatory Biomarkers and Nonspecific Low Back Pain: A Systematic Review. Clin. J. Pain 2020, 36, 379–389. [Google Scholar] [CrossRef]
- Menzel, A.; Samouda, H.; Dohet, F.; Loap, S.; Ellulu, M.S.; Bohn, T. Common and Novel Markers for Measuring Inflamma-tion and Oxidative Stress Ex Vivo in Research and Clinical Practice-Which to Use Regarding Disease Outcomes? Antioxidants 2021, 10, 414. [Google Scholar] [CrossRef]
- Bothwell, L.E.; Avorn, J.; Khan, N.F.; Kesselheim, A.S. Adaptive Design Clinical Trials: A Review of the Literature and ClinicalTrials. Gov. BMJ Open 2018, 8, e018320. [Google Scholar] [CrossRef] [PubMed]
- Cook, T.; DeMets, D.L. Review of Draft FDA Adaptive Design Guidance. J. Biopharm. Stat. 2010, 20, 1132–1142. [Google Scholar] [CrossRef] [PubMed]
- Chow, S.-C.; Corey, R. Benefits, Challenges and Obstacles of Adaptive Clinical Trial Designs. Orphanet J. Rare Dis. 2011, 6, 79. [Google Scholar] [CrossRef] [Green Version]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A Classification of Chronic Pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fillingim, R.B. Individual Differences in Pain: Understanding the Mosaic That Makes Pain Personal. Pain 2017, 158 (Suppl. S1), S11–S18. [Google Scholar] [CrossRef] [Green Version]
- Dziura, J.D.; Post, L.A.; Zhao, Q.; Fu, Z.; Peduzzi, P. Strategies for Dealing with Missing Data in Clinical Trials: From De-sign to Analysis. Yale J. Biol. Med. 2013, 86, 343–358. [Google Scholar]
- Broglio, K. Randomization in Clinical Trials: Permuted Blocks and Stratification. JAMA 2018, 319, 2223–2224. [Google Scholar] [CrossRef]
- McEntegart, D.J. The Pursuit of Balance Using Stratified and Dynamic Randomization Techniques: An Overview. Drug-Form. J. 2003, 37, 293–308. [Google Scholar] [CrossRef]
- Lohr, K.N.; Zebrack, B.J. Using Patient-Reported Outcomes in Clinical Practice: Challenges and Opportunities. Qual. Life Res. 2009, 18, 99–107. [Google Scholar] [CrossRef]
- Tan, G.; Jensen, M.P.; Thornby, J.I.; Shanti, B.F. Validation of the Brief Pain Inventory for Chronic Nonmalignant Pain. J. Pain 2004, 5, 133–137. [Google Scholar] [CrossRef] [PubMed]
- van der Meij, B.S.; Langius, J.A.E.; Spreeuwenberg, M.D.; Slootmaker, S.M.; Paul, M.A.; Smit, E.F.; van Leeuwen, P.A.M. Oral Nutritional Supplements Containing N-3 Polyunsaturated Fatty Acids Affect Quality of Life and Functional Status in Lung Cancer Patients during Multimodality Treatment: An RCT. Eur. J. Clin. Nutr. 2012, 66, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S.; Warren, S.; Magee, D. Intention to Treat Analysis, Compliance, Drop-Outs and How to Deal with Missing Data in Clinical Research: A Review. Phys. Ther. Rev. 2009, 14, 36–49. [Google Scholar] [CrossRef]
- Gariballa, S.; Forster, S. Dietary Supplementation and Quality of Life of Older Patients: A Randomized, Double-Blind, Pla-cebo-Controlled Trial. J. Am. Geriatr. Soc. 2007, 55, 2030–2034. [Google Scholar] [CrossRef] [PubMed]
- Voscopoulos, C.; Lema, M. When Does Acute Pain Become Chronic? Br. J. Anaesth. 2010, 105 (Suppl. S1), i69–i85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Hecke, O.; Torrance, N.; Smith, B.H. Chronic Pain Epidemiology—Where Do Lifestyle Factors Fit In? Br. J. Pain 2013, 7, 209–217. [Google Scholar] [CrossRef] [Green Version]
- Komarnytsky, S.; Retchin, S.; Vong, C.I.; Lila, M.A. Gains and Losses of Agricultural Food Production: Implications for the Twenty-First Century. Annu. Rev. Food Sci. Technol. 2022, 13, 239–261. [Google Scholar] [CrossRef]
- Johnson, M.A.; Cosgrove, C.D. Complementary and Alternative Medicine for Chronic Musculoskeletal Pain. Fed. Pract. 2015, 32, 31–36. [Google Scholar]
- Bhattacharya, D.; Whiteside, H.; Tang, E.; Kantilal, K.; Loke, Y.; Atkins, B.; Hill, C. A Review of Trial and Real-world Data Applying Elements of a Realist Approach to Identify Behavioural Mechanisms Supporting Practitioners to Taper Opioids. Br. J. Clin. Pharmacol. 2022, 88, 4019–4042. [Google Scholar] [CrossRef]
- Takai, Y.; Yamamoto-Mitani, N.; Abe, Y.; Suzuki, M. Literature Review of Pain Management for People with Chronic Pain. Jpn. J. Nurs. Sci. 2015, 12, 167–183. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Peirce-Sandner, S.; Baron, R.; Bellamy, N.; Burke, L.B.; Chappell, A.; Chartier, K.; Cleeland, C.S.; Costello, A.; et al. Research Design Considerations for Confirmatory Chronic Pain Clinical Trials: IMMPACT Recommen-dations. Pain 2010, 149, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Lopez, H.L.; Cesareo, K.R.; Raub, B.; Kedia, A.W.; Sandrock, J.E.; Kerksick, C.M.; Ziegenfuss, T.N. Effects of Hemp Extract on Markers of Wellness, Stress Resilience, Recovery and Clinical Biomarkers of Safety in Overweight, But Otherwise Healthy Subjects. J. Diet. Suppl. 2020, 17, 561–586. [Google Scholar] [CrossRef] [PubMed]
- Narouze, S. Antinociception Mechanisms of Action of Cannabinoid-Based Medicine: An Overview for Anesthesiologists and Pain Physicians. Reg. Anesth. Pain Med. 2021, 46, 240–250. [Google Scholar] [CrossRef]
- Rajesh, M.; Pan, H.; Mukhopadhyay, P.; Bátkai, S.; Osei-Hyiaman, D.; Haskó, G.; Liaudet, L.; Gao, B.; Pacher, P. Canna-binoid-2 Receptor Agonist HU-308 Protects against Hepatic Ischemia/Reperfusion Injury by Attenuating Oxidative Stress, Inflammatory Response, and Apoptosis. J. Leukoc. Biol. 2007, 82, 1382–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, L.; Vang, D.; Nguyen, J.; Benson, B.; Lei, J.; Gupta, K. Cannabinoid Receptor-Specific Mechanisms to Alleviate Pain in Sickle Cell Anemia via Inhibition of Mast Cell Activation and Neurogenic Inflammation. Haematologica 2016, 101, 566–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McPartland, J.M.; Giuffrida, A.; King, J.; Skinner, E.; Scotter, J.; Musty, R.E. Cannabimimetic Effects of Osteopathic Manipu-lative Treatment. J. Am. Osteopath. Assoc. 2005, 105, 283–291. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Measures | Placebo (n = 13) | Intervention (n = 12) |
|---|---|---|
| Age (years) | 55.1 ± 11.3 | 55.2 ± 10.7 |
| Gender (female/male, %) | 9/4 (69.2%) | 9/3 (75.0%) |
| Hight, cm | 165.36 ± 6.54 | 161.92 ± 4.72 |
| Weight, kg | 84.59 ± 20.74 | 77.57 ± 10.22 |
| BMI, kg/m2 | 31.39 ± 9.76 | 29.73 ± 4.87 |
| Systolic BP, mmHg | 132.72 ± 3.03 | 125.47 ± 25.50 |
| Diastolic BP, mmHg | 91.11 ± 17.01 | 80.60 ± 11.43 |
| Pain duration (years) | 13.9 ± 8.6 | 14.8 ± 9.5 |
| Pain level (NPRS-11, pts) | 5.3 ± 0.6 | 5.8 ± 0.5 |
| Pain interference (BPI, pts) | 5.5 ± 1.9 | 5.0 ± 0.5 |
| ROS in PMBC | 747.7 (±102.1) | 682.45 (±106.4) |
| BPI | Placebo (n = 13) M (SD) | Intervention (n = 12) M (SD) | ||||
|---|---|---|---|---|---|---|
| Week 0 | Week 6 | Week 12 | Week 0 | Week 6 | Week 12 | |
| General Activity | 5.7 (±2.7) | 3.4 (±2.5) | 3.2 (±2.8) | 3.8 (±2.3) | 2.5 (±2.2) | 1.8 (±2.0) |
| Mood | 5.0 (±2.7) | 3.5 (±2.8) | 3.5 (±2.9) | 3.3 (±2.3) | 2.8 (±2.9) | 1.3 (±1.6) |
| Walking Ability | 4.7 (±3.2) | 2.2 (±2.4) | 2.6 (±2.1) | 2.7 (±2.7) | 2.0 (±2.5 | 1.9 (±1.8) |
| Normal Work | 6.3 (±2.3) | 3.3 (±2.4) | 3.3 (±2.4) | 3.2 (±2.3) | 2.0 (±1.9) | 1.9 (±2.0) |
| Sleep | 5.5 (±2.5) | 2.5 (±2.6) | 3.6 (±2.3) | 4.1 (±2.5) | 1.9 (±2.3) | 0.5 (±2.0) |
| Enjoyment of Life | 5.9 (±2.8) | 3.9 (±2.8) | 3.8 (±3.1) | 4.3 (±2.7) | 2.2 (±2.3) | 2 (±2.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlisle, C.; Polley, K.; Panda, C.; Barron, K.; Hamrock, M.; Dominique, A.; Metzger, B.; Le Brun-Blashka, S.; Komarnytsky, S. Alleviation of Pain, PAIN Interference, and Oxidative Stress by a Novel Combination of Hemp Oil, Calamari Oil, and Broccoli: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2023, 15, 2654. https://doi.org/10.3390/nu15122654
Carlisle C, Polley K, Panda C, Barron K, Hamrock M, Dominique A, Metzger B, Le Brun-Blashka S, Komarnytsky S. Alleviation of Pain, PAIN Interference, and Oxidative Stress by a Novel Combination of Hemp Oil, Calamari Oil, and Broccoli: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients. 2023; 15(12):2654. https://doi.org/10.3390/nu15122654
Chicago/Turabian StyleCarlisle, Carolina, Kristine Polley, Chinmayee Panda, Keri Barron, Meghan Hamrock, Ashley Dominique, Brandon Metzger, Sara Le Brun-Blashka, and Slavko Komarnytsky. 2023. "Alleviation of Pain, PAIN Interference, and Oxidative Stress by a Novel Combination of Hemp Oil, Calamari Oil, and Broccoli: A Randomized, Double-Blind, Placebo-Controlled Trial" Nutrients 15, no. 12: 2654. https://doi.org/10.3390/nu15122654
APA StyleCarlisle, C., Polley, K., Panda, C., Barron, K., Hamrock, M., Dominique, A., Metzger, B., Le Brun-Blashka, S., & Komarnytsky, S. (2023). Alleviation of Pain, PAIN Interference, and Oxidative Stress by a Novel Combination of Hemp Oil, Calamari Oil, and Broccoli: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients, 15(12), 2654. https://doi.org/10.3390/nu15122654