

Mediterranean-Type Diet Adherence and Body Mass Index through 20 Years of Follow-Up: Results from the ATTICA Cohort Study (2002–2022)

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
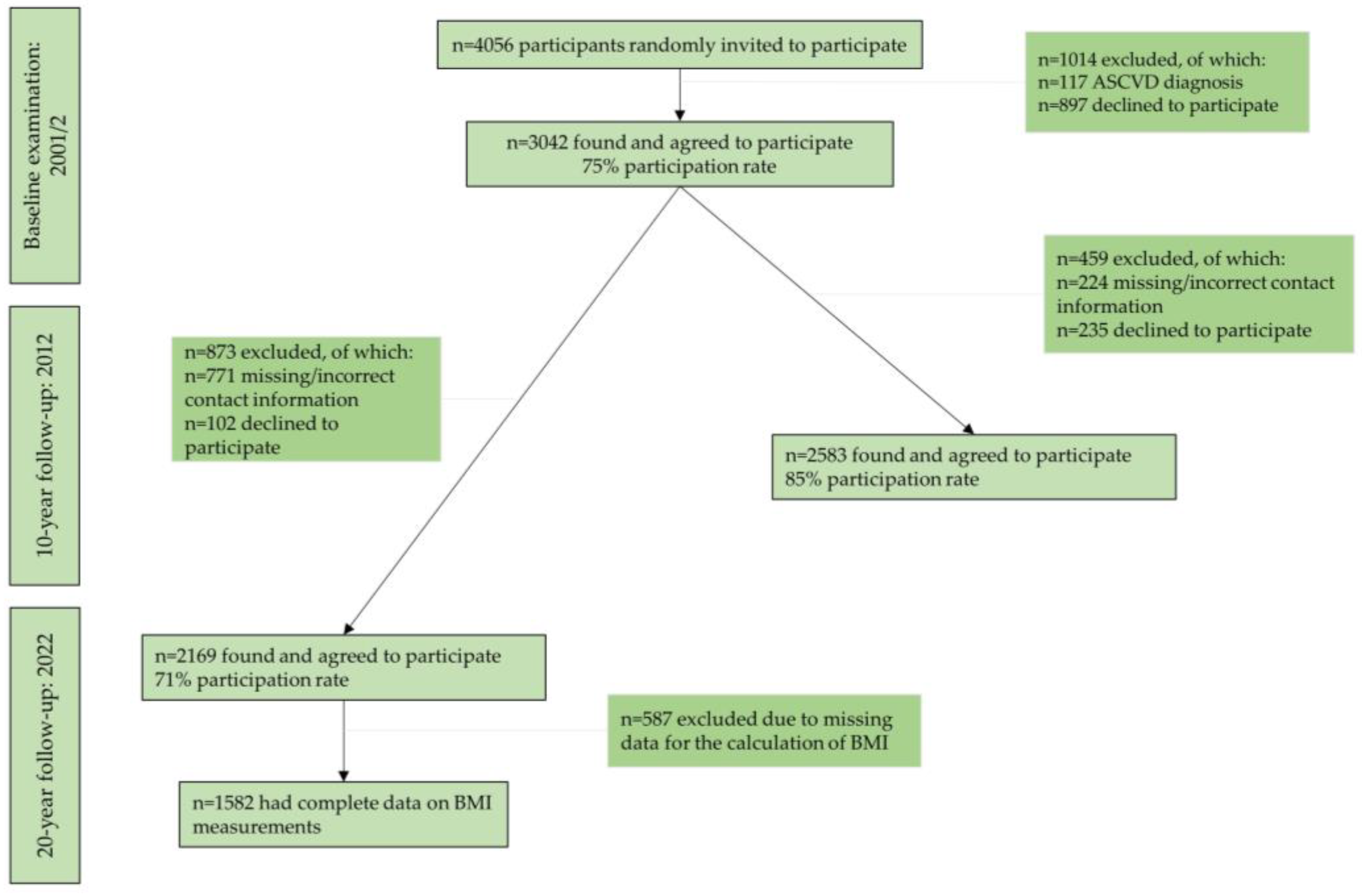
2.1. Study Design and Aims
2.2. Bioethics
2.3. Baseline and Follow-Up Assessment
2.3.1. Baseline Socio-Demographic Characteristics
2.3.2. Baseline Cardiometabolic Parameters
2.3.3. Baseline Clinical Characteristics
2.3.4. Baseline Lifestyle Characteristics
2.3.5. Dietary Habits
2.3.6. Body Weight Assessment
2.4. Study Sample
2.5. Statistical Analysis
3. Results
3.1. Participants’ Baseline Characteristics by Body Weight Trajectories (2002–2022)
3.2. Participants’ Dietary Habits by Body Weight Trajectories (2002–2022)
3.3. Dietary Habits and Body Mass Index during the 20-Year Follow-Up (2002–2022)
3.4. Dietary Habits and the Risk of Always Having Overweight/Obesity during the 20-Year Follow-Up (2002–2022)
4. Discussion
4.1. Main Findings
4.2. The Current State of the Research Field
4.3. The Mediterranean-Type Diet and Body Weight Management: The Underlying Mechanisms
4.4. Implications and Suggestions for Policy Measures
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Global Cardiovascular Risk Consortium; Magnussen, C.; Ojeda, F.M.; Leong, D.P.; Alegre-Diaz, J.; Amouyel, P.; Aviles-Santa, L.; De Bacquer, D.; Ballantyne, C.M.; Bernabé-Ortiz, A.; et al. Global Effect of Modifiable Risk Factors on Cardiovascular Disease and Mortality. N. Engl. J. Med. 2023, 389, 1273–1285. [Google Scholar] [CrossRef]
- Hassapidou, M.; Vlassopoulos, A.; Kalliostra, M.; Govers, E.; Mulrooney, H.; Ells, L.; Salas, X.R.; Muscogiuri, G.; Darleska, T.H.; Busetto, L.; et al. European Association for the Study of Obesity Position Statement on Medical Nutrition Therapy for the Management of Overweight and Obesity in Adults Developed in Collaboration with the European Federation of the Associations of Dietitians. Obes. Facts 2023, 16, 11–28. [Google Scholar] [CrossRef] [PubMed]
- Pati, S.; Irfan, W.; Jameel, A.; Ahmed, S.; Shahid, R.K. Obesity and Cancer: A Current Overview of Epidemiology, Pathogenesis, Outcomes, and Management. Cancers 2023, 15, 485. [Google Scholar] [CrossRef] [PubMed]
- Boutari, C.; Mantzoros, C.S. A 2022 Update on the Epidemiology of Obesity and a Call to Action: As Its Twin COVID-19 Pandemic Appears to Be Receding, the Obesity and Dysmetabolism Pandemic Continues to Rage On. Metabolism 2022, 133, 155217. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Veronese, N.; Di Bella, G.; Cusumano, C.; Parisi, A.; Tagliaferri, F.; Ciriminna, S.; Barbagallo, M. Mediterranean Diet in the Management and Prevention of Obesity. Exp. Gerontol. 2023, 174, 112121. [Google Scholar] [CrossRef]
- Godos, J.; Zappalà, G.; Bernardini, S.; Giambini, I.; Bes-Rastrollo, M.; Martinez-Gonzalez, M. Adherence to the Mediterranean Diet Is Inversely Associated with Metabolic Syndrome Occurrence: A Meta-Analysis of Observational Studies. Int. J. Food Sci. Nutr. 2017, 68, 138–148. [Google Scholar] [CrossRef]
- World Health Organization. WHO European Regional Obesity Report 2022. Available online: https://www.who.int/europe/publications/i/item/9789289057738 (accessed on 27 January 2024).
- Dai, H.; Alsalhe, T.A.; Chalghaf, N.; Riccò, M.; Bragazzi, N.L.; Wu, J. The Global Burden of Disease Attributable to High Body Mass Index in 195 Countries and Territories, 1990-2017: An Analysis of the Global Burden of Disease Study. PLoS Med. 2020, 17, e1003198. [Google Scholar] [CrossRef]
- World Obesity Day Atlases|Obesity Atlas 2024. Available online: https://data.worldobesity.org/publications/?cat=22 (accessed on 14 March 2024).
- Tsai, A.G.; Williamson, D.F.; Glick, H.A. Direct Medical Cost of Overweight and Obesity in the USA: A Quantitative Systematic Review. Obes. Rev. 2011, 12, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.O.; Wyatt, H.R.; Peters, J.C. Energy Balance and Obesity. Circulation 2012, 126, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D. Perspective: Obesity-an Unexplained Epidemic. Am. J. Clin. Nutr. 2022, 115, 1445–1450. [Google Scholar] [CrossRef] [PubMed]
- Poulimeneas, D.; Anastasiou, C.A.; Santos, I.; Hill, J.O.; Panagiotakos, D.B.; Yannakoulia, M. Exploring the Relationship between the Mediterranean Diet and Weight Loss Maintenance: The MedWeight Study. Br. J. Nutr. 2020, 124, 874–880. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E. The Role of the Mediterranean Diet on Weight Loss and Obesity-Related Diseases. Rev. Endocr. Metab. Disord. 2020, 21, 315–327. [Google Scholar] [CrossRef]
- Thom, G.; Lean, M. Is There an Optimal Diet for Weight Management and Metabolic Health? Gastroenterology 2017, 152, 1739–1751. [Google Scholar] [CrossRef]
- Fung, T.T.; Pan, A.; Hou, T.; Chiuve, S.E.; Tobias, D.K.; Mozaffarian, D.; Willett, W.C.; Hu, F.B. Long-Term Change in Diet Quality Is Associated with Body Weight Change in Men and Women123. J. Nutr. 2015, 145, 1850–1856. [Google Scholar] [CrossRef]
- Pavlidou, E.; Papadopoulou, S.K.; Fasoulas, A.; Papaliagkas, V.; Alexatou, O.; Chatzidimitriou, M.; Mentzelou, M.; Giaginis, C. Diabesity and Dietary Interventions: Evaluating the Impact of Mediterranean Diet and Other Types of Diets on Obesity and Type 2 Diabetes Management. Nutrients 2024, 16, 34. [Google Scholar] [CrossRef] [PubMed]
- Damigou, E.; Faka, A.; Kouvari, M.; Anastasiou, C.; Kosti, R.I.; Chalkias, C.; Panagiotakos, D. Adherence to a Mediterranean Type of Diet in the World: A Geographical Analysis Based on a Systematic Review of 57 Studies with 1,125,560 Participants. Int. J. Food Sci. Nutr. 2023, 74, 799–813. [Google Scholar] [CrossRef]
- Vilarnau, C.; Stracker, D.M.; Funtikov, A.; da Silva, R.; Estruch, R.; Bach-Faig, A. Worldwide Adherence to Mediterranean Diet between 1960 and 2011. Eur. J. Clin. Nutr. 2019, 72, 83–91. [Google Scholar] [CrossRef]
- da Silva, R.; Bach-Faig, A.; Raidó Quintana, B.; Buckland, G.; Vaz de Almeida, M.D.; Serra-Majem, L. Worldwide Variation of Adherence to the Mediterranean Diet, in 1961–1965 and 2000–2003. Public Health Nutr. 2009, 12, 1676–1684. [Google Scholar] [CrossRef]
- Pitsavos, C.; Panagiotakos, D.B.; Chrysohoou, C.; Stefanadis, C. Epidemiology of Cardiovascular Risk Factors in Greece: Aims, Design and Baseline Characteristics of the ATTICA Study. BMC Public Health 2003, 3, 32. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Georgousopoulou, E.N.; Pitsavos, C.; Chrysohoou, C.; Metaxa, V.; Georgiopoulos, G.A.; Kalogeropoulou, K.; Tousoulis, D.; Stefanadis, C.; ATTICA Study group. Ten-Year (2002–2012) Cardiovascular Disease Incidence and All-Cause Mortality, in Urban Greek Population: The ATTICA Study. Int. J. Cardiol. 2015, 180, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Damigou, E.; Kouvari, M.; Chrysohoou, C.; Barkas, F.; Kravvariti, E.; Pitsavos, C.; Skoumas, J.; Michelis, E.; Liberopoulos, E.; Tsioufis, C.; et al. Lifestyle Trajectories Are Associated with Incidence of Cardiovascular Disease: Highlights from the ATTICA Epidemiological Cohort Study (2002–2022). Life 2023, 13, 1142. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S17–S38. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou, G.; Georgoudis, G.; Papandreou, M.; Spyropoulos, P.; Georgakopoulos, D.; Kalfakakou, V.; Evangelou, A. Reliability Measures of the Short International Physical Activity Questionnaire (IPAQ) in Greek Young Adults. Hell. J. Cardiol. 2009, 50, 283–294. [Google Scholar]
- Sember, V.; Meh, K.; Sorić, M.; Starc, G.; Rocha, P.; Jurak, G. Validity and Reliability of International Physical Activity Questionnaires for Adults across EU Countries: Systematic Review and Meta Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7161. [Google Scholar] [CrossRef]
- Katsouyanni, K.; Rimm, E.B.; Gnardellis, C.; Trichopoulos, D.; Polychronopoulos, E.; Trichopoulou, A. Reproducibility and Relative Validity of an Extensive Semi-Quantitative Food Frequency Questionnaire Using Dietary Records and Biochemical Markers among Greek Schoolteachers. Int. J. Epidemiol. 1997, 26, S118. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary Patterns: A Mediterranean Diet Score and Its Relation to Clinical and Biological Markers of Cardiovascular Disease Risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef]
- Zaragoza-Martí, A.; Cabañero-Martínez, M.J.; Hurtado-Sánchez, J.A.; Laguna-Pérez, A.; Ferrer-Cascales, R. Evaluation of Mediterranean Diet Adherence Scores: A Systematic Review. BMJ Open 2018, 8, e019033. [Google Scholar] [CrossRef] [PubMed]
- Anastasiou, C.A.; Karfopoulou, E.; Yannakoulia, M. Weight Regaining: From Statistics and Behaviors to Physiology and Metabolism. Metabolism 2015, 64, 1395–1407. [Google Scholar] [CrossRef] [PubMed]
- Paixão, C.; Dias, C.M.; Jorge, R.; Carraça, E.V.; Yannakoulia, M.; de Zwaan, M.; Soini, S.; Hill, J.O.; Teixeira, P.J.; Santos, I. Successful Weight Loss Maintenance: A Systematic Review of Weight Control Registries. Obes. Rev. 2020, 21, e13003. [Google Scholar] [CrossRef] [PubMed]
- Yannakoulia, M.; Poulimeneas, D.; Mamalaki, E.; Anastasiou, C.A. Dietary Modifications for Weight Loss and Weight Loss Maintenance. Metabolism 2019, 92, 153–162. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, H.; Wang, Z.; Huang, F.; Zhang, X.; Du, W.; Su, C.; Ouyang, Y.; Li, L.; Bai, J.; et al. Trajectories of Dietary Patterns and Their Associations with Overweight/Obesity among Chinese Adults: China Health and Nutrition Survey 1991–2018. Nutrients 2021, 13, 2835. [Google Scholar] [CrossRef]
- Kang, M.; Boushey, C.J.; Shvetsov, Y.B.; Setiawan, V.W.; Paik, H.-Y.; Wilkens, L.R.; Le Marchand, L.; Park, S.-Y. Changes in Diet Quality and Body Weight over 10 Years: The Multiethnic Cohort Study. Br. J. Nutr. 2021, 126, 1389–1397. [Google Scholar] [CrossRef]
- Angulo, E.; Stern, D.; Castellanos-Gutiérrez, A.; Monge, A.; Lajous, M.; Bromage, S.; Fung, T.T.; Li, Y.; Bhupathiraju, S.N.; Deitchler, M.; et al. Changes in the Global Diet Quality Score, Weight, and Waist Circumference in Mexican Women. J. Nutr. 2021, 151, 152S–161S. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Chrysohoou, C.; Pitsavos, C.; Stefanadis, C. Association between the Prevalence of Obesity and Adherence to the Mediterranean Diet: The ATTICA Study. Nutrition 2006, 22, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Georgoulis, M.; Damigou, E.; Chrysohoou, C.; Barkas, F.; Anastasiou, G.; Kravvariti, E.; Tsioufis, C.; Liberopoulos, E.; Sfikakis, P.P.; Pitsavos, C.; et al. Mediterranean Diet Trajectories and 20-Year Incidence of Cardiovascular Disease: The ATTICA Cohort Study (2002–2022). Nutr. Metab. Cardiovasc. Dis. 2023, 34, 153–166. [Google Scholar] [CrossRef]
- Lichtenstein, A.H.; Appel, L.J.; Vadiveloo, M.; Hu, F.B.; Kris-Etherton, P.M.; Rebholz, C.M.; Sacks, F.M.; Thorndike, A.N.; Van Horn, L.; Wylie-Rosett, J.; et al. 2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e472–e487. [Google Scholar] [CrossRef]
- Lotfi, K.; Saneei, P.; Hajhashemy, Z.; Esmaillzadeh, A. Adherence to the Mediterranean Diet, Five-Year Weight Change, and Risk of Overweight and Obesity: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Adv. Nutr. 2022, 13, 152–166. [Google Scholar] [CrossRef]
- Twells, L.K.; Janssen, I.; Kuk, J.L. Canadian Adult Obesity Clinical Practice Guidelines: Epidemiology of Adult Obesity. Available online: https://obesitycanada.ca/guidelines/epidemiology (accessed on 20 March 2024).
- Mancini, J.G.; Filion, K.B.; Atallah, R.; Eisenberg, M.J. Systematic Review of the Mediterranean Diet for Long-Term Weight Loss. Am. J. Med. 2016, 129, 407–415.e4. [Google Scholar] [CrossRef] [PubMed]
- Bendall, C.L.; Mayr, H.L.; Opie, R.S.; Bes-Rastrollo, M.; Itsiopoulos, C.; Thomas, C.J. Central Obesity and the Mediterranean Diet: A Systematic Review of Intervention Trials. Crit. Rev. Food Sci. Nutr. 2018, 58, 3070–3084. [Google Scholar] [CrossRef] [PubMed]
- Barnard, N.D.; Alwarith, J.; Rembert, E.; Brandon, L.; Nguyen, M.; Goergen, A.; Horne, T.; do Nascimento, G.F.; Lakkadi, K.; Tura, A.; et al. A Mediterranean Diet and Low-Fat Vegan Diet to Improve Body Weight and Cardiometabolic Risk Factors: A Randomized, Cross-over Trial. J. Am. Nutr. Assoc. 2022, 41, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Konieczna, J.; Ruiz-Canela, M.; Galmes-Panades, A.M.; Abete, I.; Babio, N.; Fiol, M.; Martín-Sánchez, V.; Estruch, R.; Vidal, J.; Buil-Cosiales, P.; et al. An Energy-Reduced Mediterranean Diet, Physical Activity, and Body Composition: An Interim Subgroup Analysis of the PREDIMED-Plus Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e2337994. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Buil-Cosiales, P.; Corella, D.; Bulló, M.; Fitó, M.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Wärnberg, J.; López-Miranda, J.; et al. Cohort Profile: Design and Methods of the PREDIMED-Plus Randomized Trial. Int. J. Epidemiol. 2019, 48, 387–388o. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Tomaino, L.; Dernini, S.; Berry, E.M.; Lairon, D.; Ngo de la Cruz, J.; Bach-Faig, A.; Donini, L.M.; Medina, F.-X.; Belahsen, R.; et al. Updating the Mediterranean Diet Pyramid towards Sustainability: Focus on Environmental Concerns. Int. J. Environ. Res. Public Health 2020, 17, 8758. [Google Scholar] [CrossRef] [PubMed]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean Diet Pyramid Today. Science and Cultural Updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef]
- Moussavi, N.; Gavino, V.; Receveur, O. Could the Quality of Dietary Fat, and Not Just Its Quantity, Be Related to Risk of Obesity? Obesity 2008, 16, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Salleh, S.N.; Fairus, A.A.H.; Zahary, M.N.; Bhaskar Raj, N.; Mhd Jalil, A.M. Unravelling the Effects of Soluble Dietary Fibre Supplementation on Energy Intake and Perceived Satiety in Healthy Adults: Evidence from Systematic Review and Meta-Analysis of Randomised-Controlled Trials. Foods 2019, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Merra, G.; Noce, A.; Marrone, G.; Cintoni, M.; Tarsitano, M.G.; Capacci, A.; De Lorenzo, A. Influence of Mediterranean Diet on Human Gut Microbiota. Nutrients 2020, 13, 7. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Cantone, E.; Cassarano, S.; Tuccinardi, D.; Barrea, L.; Savastano, S.; Colao, A. Gut Microbiota: A New Path to Treat Obesity. Int. J. Obes. Suppl. 2019, 9, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Townsend, J.R.; Kirby, T.O.; Sapp, P.A.; Gonzalez, A.M.; Marshall, T.M.; Esposito, R. Nutrient Synergy: Definition, Evidence, and Future Directions. Front. Nutr. 2023, 10, 1279925. [Google Scholar] [CrossRef]
- Bes-Rastrollo, M.; Sánchez-Villegas, A.; de la Fuente, C.; de Irala, J.; Martinez, J.A.; Martínez-González, M.A. Olive Oil Consumption and Weight Change: The SUN Prospective Cohort Study. Lipids 2006, 41, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Zamora Zamora, F.; Martínez Galiano, J.M.; Gaforio Martínez, J.J.; Delgado Rodríguez, M. [Olive Oil and Body Weight. Systematic Review and Meta-Analysis of Randomized Controlled Trials]. Rev. Esp. Salud Publica 2018, 92, e201811083. [Google Scholar]
- Hill, J.O. Understanding and Addressing the Epidemic of Obesity: An Energy Balance Perspective. Endocr. Rev. 2006, 27, 750–761. [Google Scholar] [CrossRef]
- Mozaffarian, D. Foods, Obesity, and Diabetes-Are All Calories Created Equal? Nutr. Rev. 2017, 75, 19–31. [Google Scholar] [CrossRef]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef]
- Koutras, Y.; Chrysostomou, S.; Poulimeneas, D.; Yannakoulia, M. Examining the Associations between a Posteriori Dietary Patterns and Obesity Indexes: Systematic Review of Observational Studies. Nutr. Health 2022, 28, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Blundell, J.E.; Dulloo, A.G.; Salvador, J.; Frühbeck, G.; on behalf of the EASO SAB Working Group on BMI. Beyond BMI—Phenotyping the Obesities. Obes. Facts 2014, 7, 322–328. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Trajectories of Body Weight, 2002–2022 | p-Value * | ||||
|---|---|---|---|---|---|
| Socio-Demographic Characteristics | Always Had a Normal Weight | Acquired Overweight/Obesity | Acquired a Normal Weight | Always Had Overweight/Obesity | |
| N | 719 | 57 | 25 | 781 | - |
| Age, mean (SD) | 36 (10) | 38 (10) | 49 (10) a,b | 40 (9) a | <0.001 |
| Sex, %men | 31 | 30 | 76 a,b | 65 a,b | <0.001 |
| High socio-economic status, % | 39 | 32 | 41 | 38 | 0.784 |
| Clinical characteristics | |||||
| Diabetes mellitus, % | 1.3 | 3.7 | 0 | 5 a | <0.001 |
| Hypercholesterolemia, % | 24 | 30 | 56 a | 40 a | <0.001 |
| Hypertension, % | 11 | 20 | 43 a | 32 a | <0.001 |
| Cardiometabolic parameters | |||||
| Total cholesterol, mg/dL, mean (SD) | 178 (37) | 182 (43) | 214 (43) a,b | 193 (40) a | <0.001 |
| LDL, mg/dL, mean (SD) | 109 (34) | 117 (40) | 137 (42) a | 123 (37) a | <0.001 |
| HDL, mg/dL, mean (SD) | 53 (14) | 49 (12) | 47 (16) | 45 (13) a | <0.001 |
| Triglycerides, mg/dL, median (IQR) | 70 (46) | 79 (73) | 105 (65) a | 107 (82) a,b | <0.001 |
| SBP, mmHg, mean (SD) | 112 (15) | 119 (17) a | 129 (20) a | 123 (16) a | <0.001 |
| DBP, mmHg, mean (SD) | 73 (10) | 77 (11) | 85 (12) a,b | 81 (11) a,b | <0.001 |
| HOMA-IR, median (IQR) | 2.6 (0.9) | 2.6 (0.8) | 2.8 (1.0) | 2.9 (1.1) a | <0.001 |
| hsCRP, mg/L, median (IQR) | 0.60 (1.3) | 0.62 (1.1) | 1.5 (2.0) | 1.4 (2.1) a,b | <0.001 |
| eGFR, mL/min/1.73 m2, median (IQR) | 142 (112) | 146 (113) | 129 (120) | 126 (113) a | 0.021 |
| Lifestyle characteristics | |||||
| Ever smokers, % | 54 | 59 | 52 | 60 | 0.072 |
| Pack-years of cigarette smoking, median (IQR) | 280 (420) | 260 (440) | 433 (590) a,b | 420 (600) a | <0.001 |
| Physically active, % | 40 | 33 | 36 | 31 a | 0.009 |
| Trajectories of Body Weight, 2002–2022 | p-Value * | ||||
|---|---|---|---|---|---|
| Dietary Habits | Always Had a Normal Weight | Acquired Overweight/Obesity | Acquired a Normal Weight | Always Had Overweight/Obesity | |
| N | 719 | 57 | 25 | 781 | - |
| Baseline MedDietScore (2002), median (IQR) | 28 (2.3) | 28 (2.1) | 26 (2.3) a,b | 25 (2.7) a,b | <0.001 |
| MedDietScore (2012), median (IQR) | 27 (2.4) | 27 (2.2) | 25 (2.6) a | 25 (2.8) a,b | <0.001 |
| MedDietScore (2022), median (IQR) | 22 (4.0) | 22 (6.0) | 20 (4) a | 19 (3.0) a | <0.001 |
| Mediterranean-type diet trajectories 2002–2012, % | a,b | a,b | <0.001 | ||
| Always low | 8 | 2 | 72 | 56 | |
| Low to high | 1 | 2 | 12 | 6 | |
| High to low | 2 | 8 | 0 | 2 | |
| Always high | 89 | 88 | 16 | 36 | |
| Mediterranean-type diet trajectories 2002–2022, % | a,b | a,b | <0.001 | ||
| Always low | 7 | 4 | 64 | 54 | |
| Low to high | 2 | 0 | 20 | 8 | |
| High to low | 45 | 55 | 12 | 31 | |
| Always high | 46 | 41 | 4 | 7 | |
| Dietary Habits (Independent Variables) | Models * | |||
|---|---|---|---|---|
| Model 1: BMI in 2022 (kg/m2), b (SE) | p-Value | Model 2: Mean BMI during 2002–2022 (kg/m2), b (SE) | p-Value | |
| Baseline MedDietScore (2002), per 1/55 | −0.13 (0.02) | <0.001 | −0.08 (0.02) | <0.001 |
| MedDietScore (2012), per 1/55 | −0.11 (0.02) | <0.001 | −0.08 (0.02) | <0.001 |
| MedDietScore (2022), per 1/55 | −0.05 (0.02) | 0.019 | −0.09 (0.02) | <0.001 |
| Mediterranean-type diet trajectories 2002–2012 vs always low | ||||
| Low to high | 0.30 (0.73) | 0.683 | −0.26 (0.55) | 0.639 |
| High to low | −4.09 (0.77) | <0.001 | −3.08 (0.60) | <0.001 |
| Always high | −4.37 (0.48) | <0.001 | −3.37 (0.38) | <0.001 |
| Mediterranean-type diet trajectories 2002–2022 vs always low | ||||
| Low to high | −0.47 (0.64) | 0.459 | −0.81 (0.57) | 0.159 |
| High to low | −3.88 (0.43) | <0.001 | −3.16 (0.35) | <0.001 |
| Always high | −6.54 (0.54) | <0.001 | −5.28 (0.49) | <0.001 |
| Dietary Habits (Independent Variables) | Models | ||
|---|---|---|---|
| Model 1: Crude | Model 2: Age- and Sex-Adjusted | Model 3: Adjusted for Age, Sex, SES, Energy Intake, Smoking, Physical Activity, Hypertension, Hypercholesterolemia and Diabetes Mellitus | |
| OR (95%CI) * | OR (95%CI) * | OR (95%CI) * | |
| Baseline MedDietScore (2002), per 1/55 | 0.81 (0.78, 0.85) | 0.88 (0.86, 0.92) | 0.92 (0.89, 0.95) |
| MedDietScore (2012), per 1/55 | 0.84 (0.81, 0.87) | 0.90 (0.88, 0.93) | 0.93 (0.91, 0.96) |
| MedDietScore (2022), per 1/55 | 0.93 (0.92, 0.95) | 0.96 (0.94, 0.97) | 0.96 (0.94, 0.99) |
| Mediterranean-type diet trajectories 2002–2012 vs always low | |||
| Low to high | 0.84 (0.40, 1.74) | 0.83 (0.40, 1.72) | 1.28 (0.44, 3.65) |
| High to low | 0.11 (0.05, 0.24) | 0.13 (0.06, 0.28) | 0.17 (0.07, 0.42) |
| Always high | 0.07 (0.05, 0.09) | 0.08 (0.05, 0.11) | 0.03 (0.03, 0.12) |
| Mediterranean-type diet trajectories 2002–2022 vs always low | |||
| Low to high | 0.47 (0.27, 0.84) | 0.57 (0.32, 1.03) | 0.70 (0.29, 1.67) |
| High to low | 0.11 (0.08, 0.15) | 0.08 (0.06, 0.12) | 0.10 (0.05, 0.17) |
| Always high | 0.02 (0.01, 0.03) | 0.01 (0.01, 0.02) | 0.02 (0.01, 0.05) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damigou, E.; Georgoulis, M.; Chrysohoou, C.; Barkas, F.; Vlachopoulou, E.; Adamidis, P.S.; Kravvariti, E.; Tsioufis, C.; Pitsavos, C.; Liberopoulos, E.; et al. Mediterranean-Type Diet Adherence and Body Mass Index through 20 Years of Follow-Up: Results from the ATTICA Cohort Study (2002–2022). Nutrients 2024, 16, 1128. https://doi.org/10.3390/nu16081128
Damigou E, Georgoulis M, Chrysohoou C, Barkas F, Vlachopoulou E, Adamidis PS, Kravvariti E, Tsioufis C, Pitsavos C, Liberopoulos E, et al. Mediterranean-Type Diet Adherence and Body Mass Index through 20 Years of Follow-Up: Results from the ATTICA Cohort Study (2002–2022). Nutrients. 2024; 16(8):1128. https://doi.org/10.3390/nu16081128
Chicago/Turabian StyleDamigou, Evangelia, Michael Georgoulis, Christina Chrysohoou, Fotios Barkas, Elpiniki Vlachopoulou, Petros S. Adamidis, Evrydiki Kravvariti, Costas Tsioufis, Christos Pitsavos, Evangelos Liberopoulos, and et al. 2024. "Mediterranean-Type Diet Adherence and Body Mass Index through 20 Years of Follow-Up: Results from the ATTICA Cohort Study (2002–2022)" Nutrients 16, no. 8: 1128. https://doi.org/10.3390/nu16081128
APA StyleDamigou, E., Georgoulis, M., Chrysohoou, C., Barkas, F., Vlachopoulou, E., Adamidis, P. S., Kravvariti, E., Tsioufis, C., Pitsavos, C., Liberopoulos, E., Sfikakis, P. P., & Panagiotakos, D. (2024). Mediterranean-Type Diet Adherence and Body Mass Index through 20 Years of Follow-Up: Results from the ATTICA Cohort Study (2002–2022). Nutrients, 16(8), 1128. https://doi.org/10.3390/nu16081128