Oxidative Damage and Inflammation in Obese Diabetic Emirati Subjects


Abstract
:1. Introduction
2. Experimental Design
2.1. Methods
2.2. Statistical Analyses
3. Results

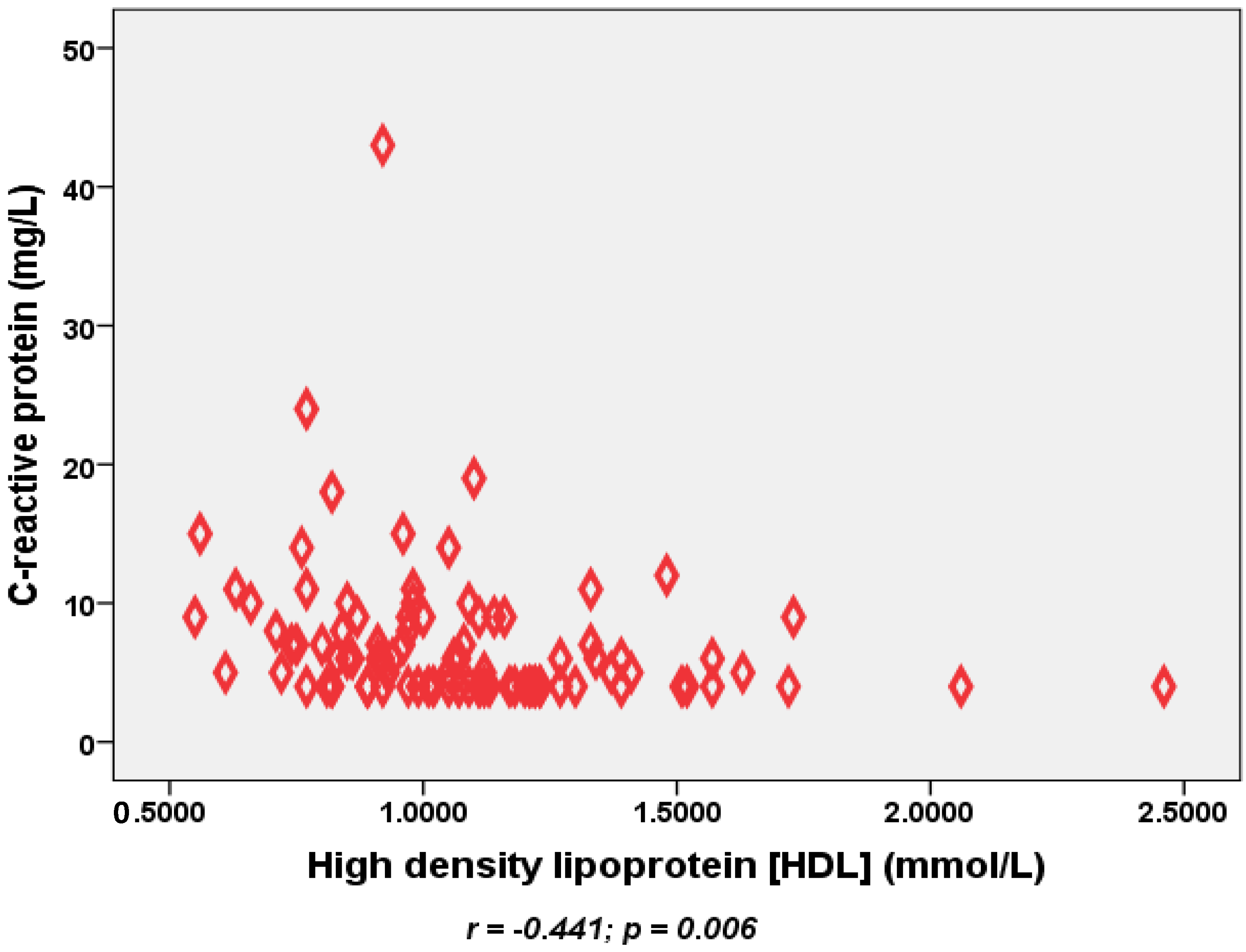{kind=link}
| Variable | Body Mass Index (BMI) † | ||
|---|---|---|---|
| Satisfactory (n = 10) | Increased Risk (n = 30) | High Risk (n = 60) | |
| Age (year) | 56 (4) | 54 (2) | 49 (1) |
| Male:female (n) | 7:3 | 15:15 | 19:41 |
| Smoking (n) | 2 | 1 | 5 |
| Duration of diabetes (year) | 1.9 (0.4) | 2.3 (0.2) | 2 (0.1) |
| Previous ischemic heart disease (n) | 0 | 5 | 9 |
| Previous cerebrovascular disease (n) | 0 | 1 | 0 |
| Previous hypertension (n) | 6 | 18 | 38 |
| Total number of drugs/patient | 2.2 | 2.1 | 2.0 |
| Number of patients taking statins | 9 | 22 | 43 |
| Systolic BP (mmHg) | 142 (6) | 138 (4) | 133 (2) |
| Diastolic BP (mmHg) | 79 (5) | 78 (2) | 80 (1) |
| High cholesterol | 7 | 25 | 42 |
| Waist circumference * (cm) | 91 (3.5) | 95 (1.4) | 110 (1.5) |
| Hip circumference * (cm) | 95 (3.1) | 101 (1.2) | 118 (1.3) |
| HbA1c (%) | 7.97 (0.8) | 7.95 (0.5) | 8.1 (0.2) |
| Total cholesterol (mmol/L) | 4.55 (0.3) | 4.46 (0.2) | 4.55 (0.1) |
| LDL (mmol/L) | 2.8 (0.29) | 2.8 (0.19) | 2.9 (0.12) |
| HDL * (mmol/L) | 1.24 (0.1) | 1.04 (0.1) | 1.07 (0.04) |
| Triglycerides (mmol/L) | 1.0 (0.14) | 1.39 (0.16) | 1.46 (0.15) |
| Variable | BMI | |||
|---|---|---|---|---|
| Satisfactory (n = 7) | Increased Risk (n = 15) | High Risk (n = 19) | p-Value | |
| CRP (mg/L) † | 4.6 (0.4) | 5.8 (0.6) | 6.5 (0.7) | 0.250 |
| IL6 (pg/mL) | 3.03 (0.42) | 3.87 (0.42) | 3.33 (0.37) | 0.476 |
| TNFα (pg/mL) | 1.13 (0.25) | 1.63 (0.40) | 3.45 (1.14) | 0.667 |
| Vitamin C (mg/L) | 23.3 (12) | 27.3 (5) | 20.6 (3) | 0.382 |
| Vitamin E (mg/L) | 9.5 (2.2) | 10.4 (1.0) | 8.1 (1.2) | 0.233 |
| Vitamin A (mg/L) | 0.98 (0.28) | 0.88 (0.1) | 0.75 (0.1) | 0.577 |
| Protein carbonyl (nmol/mg) | 0.47 (0.18) | 0.71 (0.1) | 0.48 (0.1) | 0.192 |
| MDA (nM/mL) † | 11.8 (8.1) | 11.6 (2.8) | 5.45 (1.2) | 0.474 |
| Variable | BMI | |||
|---|---|---|---|---|
| Satisfactory (n = 3) | Increased Risk (n = 15) | High Risk (n = 41) | p-Value | |
| CRP † | 4.3 (0.3) | 5.9 (0.9) | 10.0 (1.3) | 0.020 * |
| IL6 | 3.15 (0.52) | 3.11 (0.46) | 2.93 (0.51) | 0.773 |
| TNFα | 1.19 (0.9) | 1.32 (1.8) | 2.04 (3.3) | 0.767 |
| Vitamin C | 55.8 (3.6) | 30.7 (4.7) | 29.6 (2.8) | 0.080 |
| Vitamin E | 9.4 (3.8) | 5.7 (0.8) | 8.5 (0.6) | 0.031 * |
| Vitamin A | 0.73 (0.25) | 0.46 (0.09) | 0.61 (0.05) | 0.082 |
| Protein carbonyl | 0.94 (0.06) | 0.76 (0.07) | 0.65 (0.07) | 0.334 |
| MDA † | 8.9 (1.8) | 17.3 (4.5) | 11.8 (1.9) | 0.270 |
| Male | Waist Circumference | |||
|---|---|---|---|---|
| Satisfactory (n = 5) | Increased Risk (n = 15) | High Risk (n = 21) | p-Value | |
| CRP | 4.8 (0.6) | 4.8 (0.3) | 7.0 (0.7) | 0.065 |
| IL6 | 3.39 (0.5) | 3.36 (0.4) | 3.58 (0.4) | 0.874 |
| TNFα | 0.87 (0.3) | 3.39 (1.4) | 2.04 (0.5) | 0.338 |
| Vitamin C | 33.8 (14) | 23 (0.5) | 21 (4) | 0.781 |
| Vitamin E | 8.7 (2) | 10.5 (1) | 8.3 (1) | 0.225 |
| Vitamin A | 1.1 (0.4) | 0.93 (0.07) | 0.70 (0.1) | 0.157 |
| Protein carbonyl | 0.598 (0.16) | 0.527 (0.12) | 0.582 (0.09) | 0.967 |
| MDA | 17.2 (11) | 7.7 (2.7) | 7.6 (1.6) | 0.787 |
| Female | Waist Circumference | ||||||
|---|---|---|---|---|---|---|---|
| Satisfactory (n = 3) | Increased Risk (n = 5) | High Risk (n = 51) | p-Value | ||||
| CRP | 4 (0.0) | 4.6 (0.4) | 9.4 (1) | 0.021 * | |||
| IL6 | 2.85 (0.4) | 4.55 (1.0) | 2.84 (0.3) | 0.131 | |||
| TNFα | 0.76 (0.4) | 1.52 (0.5) | 1.90 (0.4) | 0.714 | |||
| Vitamin C | 54.7 (5) | 45.6 (9) | 28.4 (3) | 0.016 * | |||
| Vitamin E | 6.2 (3) | 9.3 (2) | 7.8 (0.5) | 0.563 | |||
| Vitamin A | 0.4 (0.1) | 0.57 (0.2) | 0.59 (0.1) | 0.734 | |||
| Protein carbonyl | 0.870 (0.13) | 0.890 (0.1) | 0.664 (0.06) | 0.247 | |||
| MDA | 7.56 (0.9) | 12.2 (2.6) | 13.03 (2) | 0.719 | |||

4. Discussion
5. Conclusions
Acknowledgment
Author Contributions
Conflicts of Interest
References
- World Health Orgnization. Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. World Health Org. Tech. Rep. Ser. 2000, 894, 1–253. [Google Scholar]
- McLellan, F. Obesity rising to alarming levels around the world. Lancet 2002, 359, 1412. [Google Scholar] [CrossRef]
- British Nutrition Foundation. The report of a British nutrition foundation task force. In Cardiovascular Disease, Diet, Nutrition and Emerging Risk Factors; Balckwell Publishing Ltd.: Oxford, UK, 2005. [Google Scholar]
- Malik, A.; Babir, A.; Abi Saab, B.; Roglic, G.; King, H. Glucose intolerance and associated factors in the UAE. Diabetes Res. Clin. Pract. 2005, 69, 188–195. [Google Scholar] [CrossRef]
- Baik, I.; Ascherio, A.; Rimm, E.B.; Giovannucci, E.; Spiegelman, D.; Stampfer, M.J.; Willett, W.C. Adiposity and mortality in men. Am. J. Epidemiol. 2000, 152, 264–271. [Google Scholar] [CrossRef]
- Rexode, K.M.; Carey, V.J.; Hennekens, C.H.; Walters, E.E.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C.; Manson, J.E. Abdominal adiposity and coronary heart disease in women. JAMA 1998, 280, 1843–1848. [Google Scholar] [CrossRef]
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Baustista, L.; Franzosi, M.G.; Commerford, P.; Lang, C.C.; Rumboldt, Z.; Onen, C.L.; Lisheng, L.; et al. Obesity and risk of myocardial infarction in 27,000 participants from 52 countrries: A case-control study. Lancet 2006, 366, 1640–1649. [Google Scholar] [CrossRef]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Trayhurn, P. The bology of obesity. Proc. Nutr. Soc. 2005, 64, 31–38. [Google Scholar] [CrossRef]
- Pouliot, M.C.; Despres, J.P.; Lemieux, S.; Moorjani, S.; Bouchard, C.; Tremblay, A.; Nadeau, A.; Lupien, P.J. Waist circumference and abdominal sagittal diameter: Best simple anthropometric indexes of abdominal visceral adipose tissue accumulation and related cardiovascular risk in men and women. Am. J. Cardiol. 1994, 73, 460–468. [Google Scholar] [CrossRef]
- Gariballa, S.; Afandi, B.; Abuhaltem, M.; Yassin, J.; Habib, H.; Ibrahim, W. Oxidative damage and inflammation in obese diabetic Emirati subjects supplemented with antioxidants and B-vitamins. Nutr. Metab. (Lond.) 2013, 10, 21. [Google Scholar] [CrossRef]
- Li, X.Y.; Chow, C.K. An improved method for the measurement of malondialdehyde in biological samples. Lipids 2004, 29, 73–75. [Google Scholar] [CrossRef]
- Levine, R.L.; Garland, D.; Oliver, C.N.; Amici, A.; Climent, I.; Lenz, A.; Ahn, B.; Shaltiel, S.; Stadtman, E. Determination of carbonyl content in oxidatively modified proteins. Methods Enzymol. 1990, 186, 464–478. [Google Scholar]
- Esteghamati, A.; Ashraf, H.; Rashidi, A.; Meysamie, A. Waist circumference cut-off points for the diagnosis of metabolic syndrome in Iranian adults. Diabetes Res. Clin. Pract. 2008, 82, 104–107. [Google Scholar] [CrossRef]
- Hill, M.F. Emerging role for antioxidant therapy in protection against diabetic cardiac complications: Experimental and clinical evidence for utilization of classic and new antioxidants. Curr. Cardiol. Rev. 2008, 4, 259–268. [Google Scholar] [CrossRef]
- Evans, J.L. Antoxidants: Do they have a role in the treatment of insulin resistance? Indian J. Med. Res. 2007, 125, 355–372. [Google Scholar]
- Evans, J.; Goldfine, I.D.; Maddux, B.A.; Grodsky, G.M. Oxidative stress and stress activated signalling pathways: A unifying hypothesis of type 2 diabetes. Endocr. Rev. 2002, 23, 599–622. [Google Scholar] [CrossRef]
- Carter, P.; Gray, L.J.; Troughton, J.; Khunti, K.; Davies, M.J. Fruit and vegetable intake and incidence of type 2 diabetes mellitus: Systematic review and meta-analysis. BMJ 2010, 341, c4229. [Google Scholar] [CrossRef]
- Puchau, B.; Zulet, A.; Gonzalez, A.; Hermsdorff, H.; Martinez, J. Dietary total antioxidant capacity is negatively associated with some metabolic syndrome features in healthy young men. Nutrition 2010, 26, 534–541. [Google Scholar] [CrossRef]
- Barter, P. High density lipoprotein: A therapeutic target in type 2 diabetes. Endocrinol. Metab. 2013, 28, 169–177. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gariballa, S.; Kosanovic, M.; Yasin, J.; Essa, A.E. Oxidative Damage and Inflammation in Obese Diabetic Emirati Subjects. Nutrients 2014, 6, 4872-4880. https://doi.org/10.3390/nu6114872
Gariballa S, Kosanovic M, Yasin J, Essa AE. Oxidative Damage and Inflammation in Obese Diabetic Emirati Subjects. Nutrients. 2014; 6(11):4872-4880. https://doi.org/10.3390/nu6114872
Chicago/Turabian StyleGariballa, Salah, Melita Kosanovic, Javed Yasin, and Awad El Essa. 2014. "Oxidative Damage and Inflammation in Obese Diabetic Emirati Subjects" Nutrients 6, no. 11: 4872-4880. https://doi.org/10.3390/nu6114872
APA StyleGariballa, S., Kosanovic, M., Yasin, J., & Essa, A. E. (2014). Oxidative Damage and Inflammation in Obese Diabetic Emirati Subjects. Nutrients, 6(11), 4872-4880. https://doi.org/10.3390/nu6114872