Disability, Physical Inactivity, and Impaired Health-Related Quality of Life Are Not Different in Metabolically Healthy vs. Unhealthy Obese Subjects




Abstract
:1. Introduction
2. Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Popkin, B.M. Does global obesity represent a global public health challenge? Am. J. Clin. Nutr. 2011, 93, 232–233. [Google Scholar] [CrossRef] [PubMed]
- Wildman, R.P.; Muntner, P.; Reynolds, K.; McGinn, A.P.; Rajpathak, S.; Wylie-Rosett, J.; Sowers, M.R. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: Prevalence and correlates of 2 phenotypes among the US population (NHANES 1999–2004). Arch. Intern. Med. 2008, 168, 1617–1624. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Lee, D.C.; Katzmarzyk, P.T.; Ruiz, J.R.; Sui, X.; Church, T.S.; Blair, S.N. The intriguing metabolically healthy but obese phenotype: Cardiovascular prognosis and role of fitness. Eur. Heart J. 2013, 34, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Karelis, A.D. Metabolically healthy but obese individuals. Lancet 2008, 372, 1281–1283. [Google Scholar] [CrossRef]
- Karelis, A.D.; St-Pierre, D.H.; Conus, F.; Rabasa-Lhoret, R.; Poehlman, E.T. Metabolic and body composition factors in subgroups of obesity: What do we know? J. Clin. Endocrinol. Metab. 2004, 89, 2569–2575. [Google Scholar] [CrossRef] [PubMed]
- Dalleck, L.C.; Van Guilder, G.P.; Richardson, T.B.; Bredle, D.L.; Janot, J.M. A community-based exercise intervention transitions metabolically abnormal obese adults to a metabolically healthy obese phenotype. Diabetes Metab. Syndr. Obes. 2014, 7, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Hinnohuo, G.M.; Czernichow, S.; Dugravot, A.; Batty, G.D.; Kivimaki, M.; Singh-Manoux, M. Metabolically healthy obesity and risk of mortality. Diabetes Care 2013, 36, 2294–2300. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Definition of Health. Available online: http://www.who.int/about/definition/en/print.html (accessed on 2 August 2010).
- Lohman, T.J.; Roache, A.F.; Martorell, R. Antropometric standardization reference manual. Med. Sci. Sports Exerc. 2002, 24, 952. [Google Scholar] [CrossRef]
- Ridker, P.M.; Libby, P.; Buring, J.E. Risk Markers and the Primary Prevention of Cardiovascular Disease. In Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine, 10th ed.; Mann, D.L., Zipes, D.P., Libby, P., Bonow, R.O., Braunwald, E., Eds.; Elsevier Saunders: Philadelphia, PA, USA, 2015; Chapter 39. [Google Scholar]
- Matsuda, M.; DeFronzo, R. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Kuk, J.L.; Ardern, C.I. Are metabolically normal but obese individuals at lower risk for all-cause mortality? Diabetes Care 2009, 32, 2297–2299. [Google Scholar] [CrossRef] [PubMed]
- Calori, G.; Lattuada, G.; Piemonti, L.; Garancini, M.P.; Ragogna, F.; Villa, M. Prevalence, metabolic features, and prognosis of metabolically healthy obese Italian individuals: The Cremona Study. Diabetes Care 2011, 34, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Stern, S.E.; Williams, K.; Ferrannini, E.; DeFronzo, R.A.; Bogardus, C.; Stern, M.P. Identification of individuals with insulin resistance using routine clinical measurements. Diabetes 2005, 54, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for Processing and Analysis of the International Physical Activity Questionnaire. Available online: http://www.ipaq.ki.se (accessed on 14 September 2014).
- Donini, L.M.; Brunani, A.; Sirtori, A.; Savina, C.; Tempera, S.; Cuzzolaro, M.; Spera, G.; Cimolin, V.; Precilios, H.; Raggi, A.; et al. Assessing disability in morbidly obese individuals: The Italian Society of Obesity Test for Obesity-Related Disabilities. Disabil. Rehabil. 2011, 33, 2509–2518. [Google Scholar] [CrossRef] [PubMed]
- McHorney, C.A.; Ware, J.E., Jr.; Raczek, A.E. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Cadenas-Sánchez, C.; Sui, X.; Blair, S.N.; Lavie, C.J. Role of fitness in the metabolically healthy but obese phenotype: A Review and Update. Prog. Cardiovasc. Dis. 2015, 58, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Kantartzis, K.; Machann, J.; Schick, F.; Thamer, C.; Rittig, K.; Balletshofer, B.; Machicao, F.; Fritsche, A.; Häring, H.U. Identification and characterization of metabolically benign obesity in humans. Arch. Intern. Med. 2008, 168, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Brochu, M.; Tchernof, A.; Dionne, I.J.; Sites, C.K.; Eltabbakh, G.H.; Sims, E.A.; Poehlman, E.T. What are the physical characteristics associated with a normal metabolic profile despite a high level of obesity in postmenopausal women? J. Clin. Endocrinol. Metab. 2001, 86, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Rey-Lopez, J.P.; de Rezende, L.F.; Pastor-Valero, M.; Tess, B.H. The prevalence of metabolically healthy obesity: A systematic review and critical evaluation of the definitions used. Obes. Rev. 2014, 15, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Philips, C.M.; Perry, I.J. Does inflammation determine metabolic health status in obese and nonobese adults? J. Clin. Endocrinol. Metab. 2013, 98, E1610–E1619. [Google Scholar] [CrossRef] [PubMed]
- Pataky, Z.; Bobbioni-Harsch, E.; Golay, A. Open questions about metabolically normal obesity. Int. J. Obes. 2010, 34, S18–S23. [Google Scholar] [CrossRef] [PubMed]
- Velho, S.; Paccaud, F.; Waeber, G.; Vollenweider, P.; Marques-Vidal, P. Metabolically healthy obesity: Different prevalences using different criteria. Eur. J. Clin. Nutr. 2010, 64, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Miranda, J.; Perez-Martinez, P. It is time to define metabolically obese but normal-weight (MONW) individuals. Clin. Endocrinol. 2013, 79, 314–315. [Google Scholar] [CrossRef] [PubMed]
- Meigs, J.B.; Wilson, P.W.; Fox, C.S.; Vasan, R.S.; Nathan, D.M.; Sullivan, L.M.; D’Agostino, R.B. Body mass index, metabolic syndrome, and risk of type 2 diabetes or cardiovascular disease. J. Clin. Endocrinol. Metab. 2006, 91, 2906–2912. [Google Scholar] [CrossRef] [PubMed]
- Arnlov, J.; Sundstrom, J.; Ingelsson, E.; Lind, L. Impact of BMI and the metabolic syndrome on the risk of diabetes in middle-aged men. Diabetes Care 2011, 34, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Bobbioni-Harsch, E.; Pataky, Z.; Makoundou, V.; Laville, M.; Disse, E.; Anderwald, C.; Konrad, T.; Golay, A. From metabolic normality to cardiometabolic risk factors in subjects with obesity. Obesity 2012, 20, 2063–2069. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.K.; Zinman, B.; Retnakaran, R. Are metabolically healthy overweight and obesity benign conditions? Ann. Intern. Med. 2013, 159, 758–769. [Google Scholar] [CrossRef] [PubMed]
- Snih, S.A.; Ottenbacher, K.J.; Markides, K.S.; Kuo, Y.F.; Eschbach, K.; Goodwin, J.S. The effect of obesity on disability vs. mortality in older Americans. Arch. Intern. Med. 2007, 167, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Diehr, P.; Bild, D.E.; Harris, T.B.; Duxbury, A.; Siscovick, D.; Rossi, M. Body mass index and mortality in nonsmoking older adults: The Cardiovascular Health Study. Am. J. Public Health 1998, 88, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Rissanen, A.; Heliovaara, M.; Knekt, P.; Reunanen, A.; Aromaa, A.; Maatela, J. Risk of disability and mortality due to overweight in a Finnish population. BMJ 1990, 301, 835–837. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, S.L.; Saito, Y.; Crimmins, E.M. The impact of obesity on active life expectancy in older American men and women. Gerontologist 2005, 45, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Ostir, G.V.; Markides, K.S.; Freeman, D.H.; Goodwin, J.S. Obesity and health conditions in elderly Mexican Americans: The Hispanic EPESE. Ethn. Dis. 2000, 10, 31–38. [Google Scholar] [PubMed]
- Armour, B.S.; Courtney-Long, E.; Campbell, V.A.; Wethington, H.R. Estimating disability prevalence among adults by body mass index: 2003–2009 National Health Interview Survey. Prev. Chronic Dis. 2012, 9, E178. [Google Scholar] [CrossRef] [PubMed]
- Walter, S.; Kunst, A.; Mackenbach, J.; Hofman, A.; Tiemeier, H. Mortality and disability: The effect of overweight and obesity. Int. J. Obes. 2009, 33, 1410–1418. [Google Scholar] [CrossRef] [PubMed]
- Majer, I.M.; Nusselder, W.J.; Mackenbach, J.P.; Klijs, B.; van Baal, P.H.M. Mortality risk associated with disability: A Population-Based Record Linkage Study. Am. J. Public Health. 2011, 101, e9–e15. [Google Scholar] [CrossRef] [PubMed]
- Nusselder, W.J.; Looman, C.W.; Mackenbach, J.P. Nondisease factors affected trajectories of disability in a prospective study. J. Clin. Epidemiol. 2005, 58, 484–494. [Google Scholar] [CrossRef] [PubMed]
- Middelbeck, L.; Breda, J. Obesity and Sedentariness: Reviewing the Current Situation within the WHO European Region. Curr. Obes. Rep. 2013, 2, 42–49. [Google Scholar] [CrossRef]
- Kim, Y.; Wilkens, L.R.; Park, S.Y.; Goodman, M.T.; Monroe, K.R.; Kolonel, L.N. Association between various sedentary behaviours and all-cause, cardiovascular disease and cancer mortality: The Multiethnic Cohort Study. Int. J. Epidemiol. 2013, 42, 1040–1056. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.V.; Walsh, M.K.; Pratt, J.A.; Toosizadeh, N.; Najafi, B.; Travison, T.G. Changes in spatiotemporal gait patterns during flat ground walking and obstacle crossing 1 year after bariatric surgery. Surg. Obes. Relat. Dis. 2016, 12, 1080–1085. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.V. The impact of weight classification on safety: Timing steps to adapt to external constraints. J. Musculoskelet. Neuronal Interact. 2015, 15, 103–108. [Google Scholar] [PubMed]
- Ranavolo, A.; Donini, L.M.; Mari, S.; Serrao, M.; Silvetti, A.; Iavicoli, S.; Cava, E.; Asprino, R.; Pinto, A.; Draicchio, F. Lower-limb joint coordination pattern in obese subjects. BioMed. Res. Int. 2013, 2013, 142323. [Google Scholar] [CrossRef] [PubMed]
- The WHOQOL Group. The World Health Organization quality of life assessment (WHOQOL). Development and psychometric properties. Soc. Sci. Med. 1998, 46, 1569–1585. [Google Scholar]
- Kolotkin, R.L.; Meter, K.; Williams, G.R. Quality of life and obesity. Obes. Rev. 2001, 2, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Cui, W.; Zack, M.M.; Wethington, H. Health-related quality of life and body mass index among US adolescents. Qual. Life Res. 2014, 23, 2139–2150. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Cuzzolaro, M.; Spera, G.; Badiali, M.; Basso, N.; Bollea, M.R.; Bosello, O.; Brunani, A.; Busetto, L.; Cairella, G.; et al. Obesity and Eating Disorders. Indications for the different levels of care. An Italian Expert Consensus Document. Eat. Weight Disord. 2010, 15, 1–31. [Google Scholar] [PubMed]
- Sharma, A.M.; Kushner, R.F. A proposed clinical staging system for obesity. Int. J. Obes. 2009, 33, 289–295. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| MHO (n = 102) | MUO (n = 151) | p | ||||
|---|---|---|---|---|---|---|
| Age (years) | 47.9 ± 11.9 | 52.5 ± 11.7 | 0.001 | |||
| Anthropometry and body composition | BMI | Males | kg/m2 | 34.5 ± 4.4 | 39 ± 5.7 | 0.02 |
| Females | kg/m2 | 37.7 ± 6.2 | 39.8 ± 7 | 0.03 | ||
| BMI 30–34.9 kg/m2 (%) | 46.1 | 23.2 | <0.001 | |||
| BMI 35–39.9 kg/m2 (%) | 53.9 | 76.8 | ||||
| Waist circumference | Males | cm | 114.2 ± 10.9 | 124.5 ± 10.8 | 0.14 ** | |
| Females | cm | 113.5 ± 19.1 | 118.1 ± 15.1 | 0.69 ** | ||
| WC >102 cm in Males or >88 cm in Females (%) | 97 | 99.3 | 0.14 | |||
| Body fat | Males | % | 27.1 ± 5.1 | 30.4 ± 4.1 | 0.56 ** | |
| Females | % | 39.9 ± 3.8 | 39 ± 4.1 | 0.02 ** | ||
| Fat mass | Males | kg | 27.6 ± 8.2 | 34 ± 7 | 0.4 ** | |
| Females | kg | 38.8 ± 9 | 38.3 ± 10 | 0.007 ** | ||
| Lean body mass | Males | kg | 70.4 ± 6.3 | 71.1 ± 14.7 | 0.76 ** | |
| Females | kg | 55.3 ± 9 | 54.7 ± 10.6 | 0.12 ** | ||
| Clinical status | Blood pressure | SBP (mmHg) | 124.3 ± 12.4 | 132.7 ± 12.8 | 0.001 * | |
| DBP (mmHg) | 78.9 ± 9.8 | 83.3 ± 10 | 0.02 * | |||
| Hypertension (≥130/85 mmHg) § (%) | 38.6 | 88 | <0.001 | |||
| Glycaemia | mg/dL | 91.2 ± 15.4 | 105.6 ± 25.2 | <0.001 * | ||
| Glycaemia ≥ 100 mg/dL §§ (%) | 7.9 | 72.5 | <0.001 | |||
| HOMA-IR | Score | 2.5 ± 2.1 | 5.8 ± 9.2 | <0.001 * | ||
| HOMA-IR > 2.5 (%) | 38.8 | 67 | <0.001 | |||
| Matsuda ISI | Index | 7.3 ± 5 | 5.4 ± 3.4 | 0.08 * | ||
| Matsuda index < 3 (%) | 7.5 | 21.2 | 0.046 | |||
| Triglycerides | mg/dL | 99.1 ± 13.5 | 161.8 ± 93.5 | <0.001 * | ||
| Triglycerides 1 ≥ 50 mg/dL §§§ (%) | 3 | 44.9 | <0.001 | |||
| HDL | mg/dL | 55.6 ± 11.8 | 46.6 ± 11.3 | <0.001 * | ||
| HDL < 40 mg/dL (M) or <50 mg/dL (F) §§§ (%) | 16.7 | 61.5 | <0.001 | |||
| hs-CRP | μg/L | 6517.1 ± 11,409.9 | 5294.1 ± 5612.2 | 0.37 * | ||
| hs-CRP > 3000 μg/L | 55.7 | 54 | 0.83 | |||
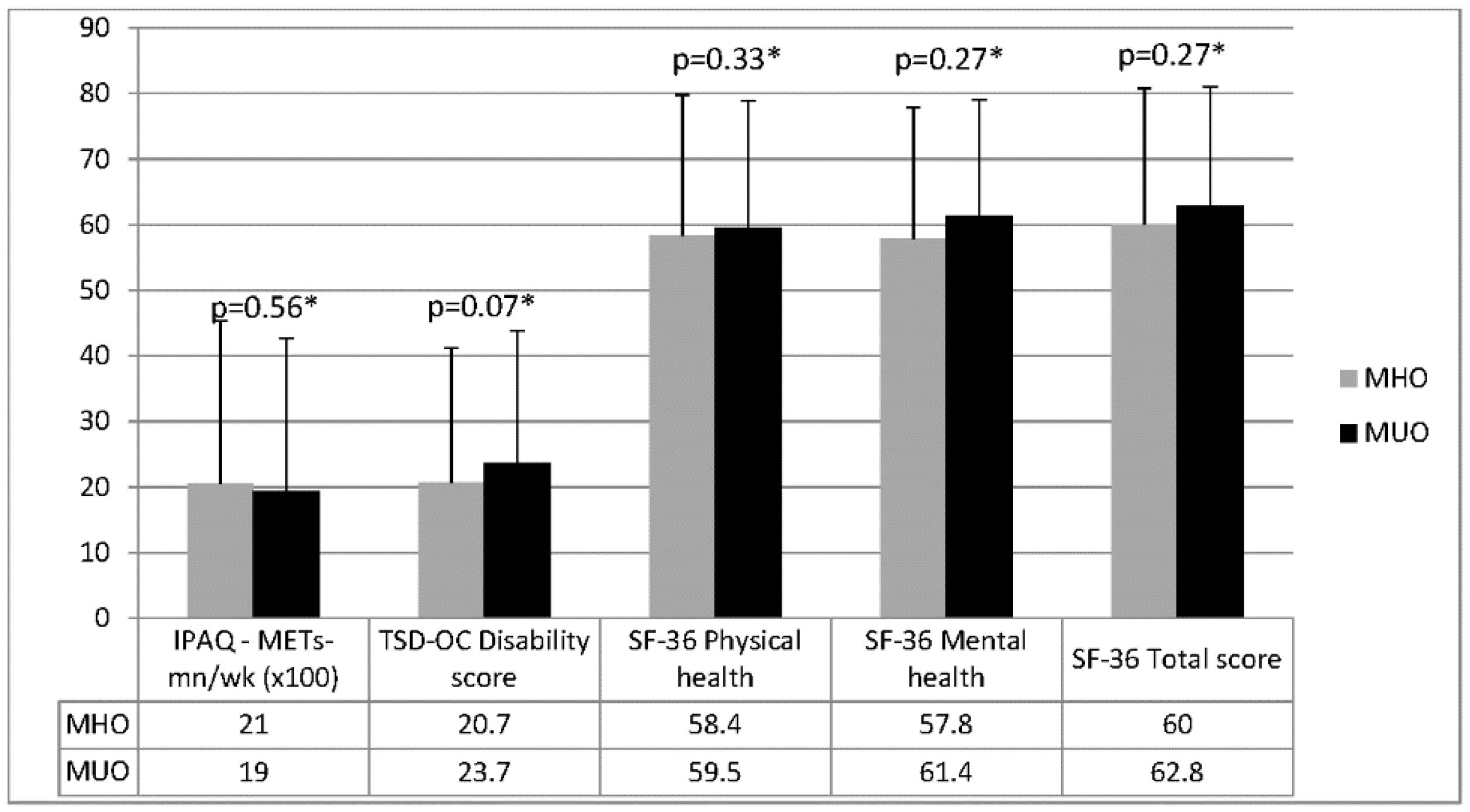
| Physical functioning and quality of life | IPAQ | METs-mn/week | 2055.3 ± 2474.7 | 1932.8 ± 2334.4 | 0.56 * | |
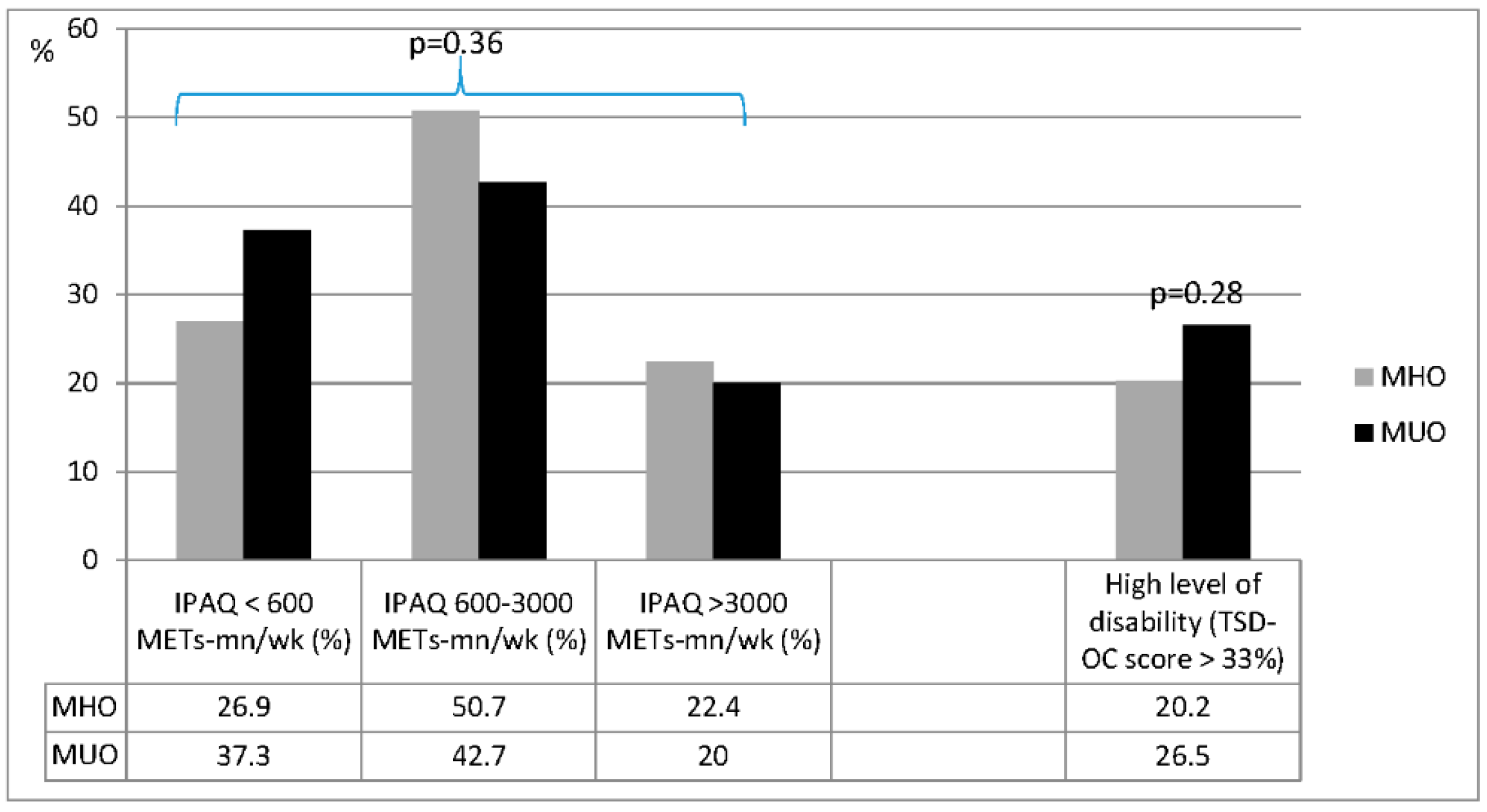
| IPAQ < 600 METs-mn/week (%) | 26.9 | 37.3 | 0.36 | |||
| IPAQ 600–3000 METs-mn/week (%) | 50.7 | 42.7 | ||||
| IPAQ > 3000 METs-mn/week (%) | 22,4 | 20 | ||||
| TSD-OC | Disability score | 20.7 ± 20.5 | 23.7 ± 20.1 | 0.07 * | ||
| >33% (%) | 20.2 | 26.5 | 0.28 | |||
| SF-36 | Physical health | 58.4 ± 21.4 | 59.5 ± 19.4 | 0.33 * | ||
| Mental health | 57.8 ± 20.1 | 61.4 ± 17.7 | 0.27 * | |||
| Total score | 60 ± 20.8 | 62.8 ± 18.2 | 0.27 * | |||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donini, L.M.; Merola, G.; Poggiogalle, E.; Lubrano, C.; Gnessi, L.; Mariani, S.; Migliaccio, S.; Lenzi, A. Disability, Physical Inactivity, and Impaired Health-Related Quality of Life Are Not Different in Metabolically Healthy vs. Unhealthy Obese Subjects. Nutrients 2016, 8, 759. https://doi.org/10.3390/nu8120759
Donini LM, Merola G, Poggiogalle E, Lubrano C, Gnessi L, Mariani S, Migliaccio S, Lenzi A. Disability, Physical Inactivity, and Impaired Health-Related Quality of Life Are Not Different in Metabolically Healthy vs. Unhealthy Obese Subjects. Nutrients. 2016; 8(12):759. https://doi.org/10.3390/nu8120759
Chicago/Turabian StyleDonini, Lorenzo M., Gianluca Merola, Eleonora Poggiogalle, Carla Lubrano, Lucio Gnessi, Stefania Mariani, Silvia Migliaccio, and Andrea Lenzi. 2016. "Disability, Physical Inactivity, and Impaired Health-Related Quality of Life Are Not Different in Metabolically Healthy vs. Unhealthy Obese Subjects" Nutrients 8, no. 12: 759. https://doi.org/10.3390/nu8120759
APA StyleDonini, L. M., Merola, G., Poggiogalle, E., Lubrano, C., Gnessi, L., Mariani, S., Migliaccio, S., & Lenzi, A. (2016). Disability, Physical Inactivity, and Impaired Health-Related Quality of Life Are Not Different in Metabolically Healthy vs. Unhealthy Obese Subjects. Nutrients, 8(12), 759. https://doi.org/10.3390/nu8120759