Dietary Impact of Adding Potassium Chloride to Foods as a Sodium Reduction Technique

Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Dietary Data
2.2. Food Product Group Classification
2.3. Reformulation Scenarios
2.4. Data Analyses
3. Results
3.1. Reformulation Scenarios
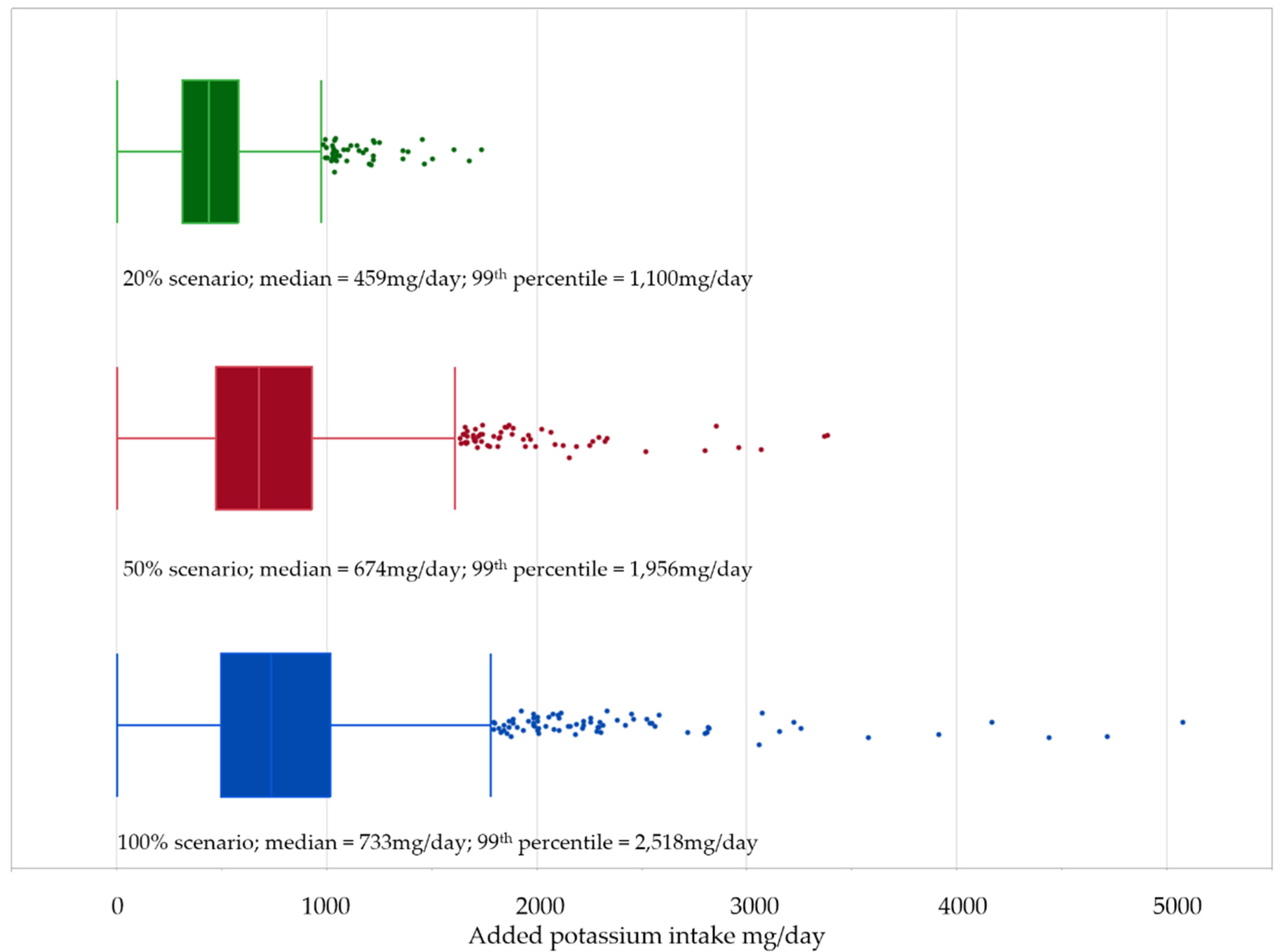
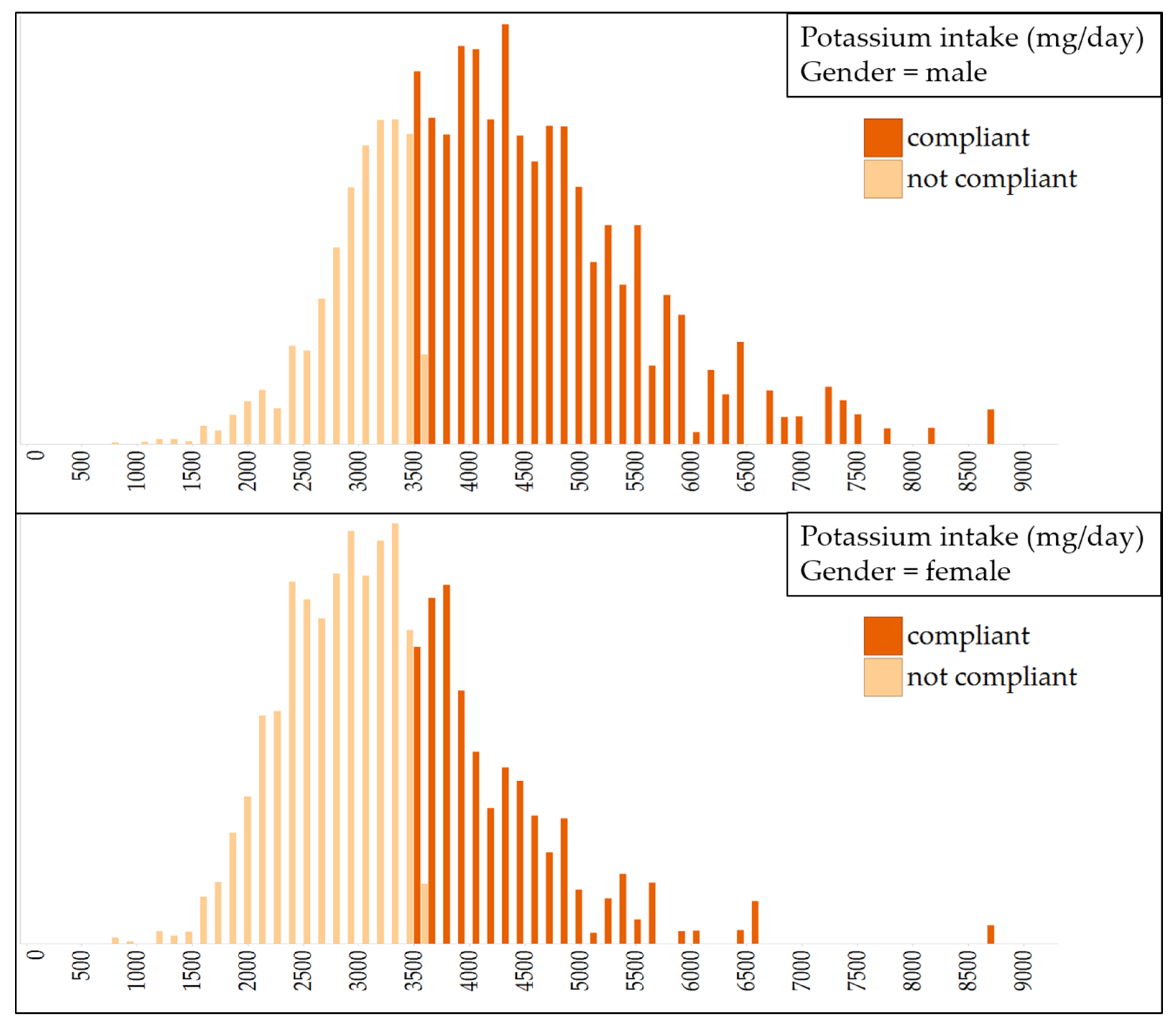
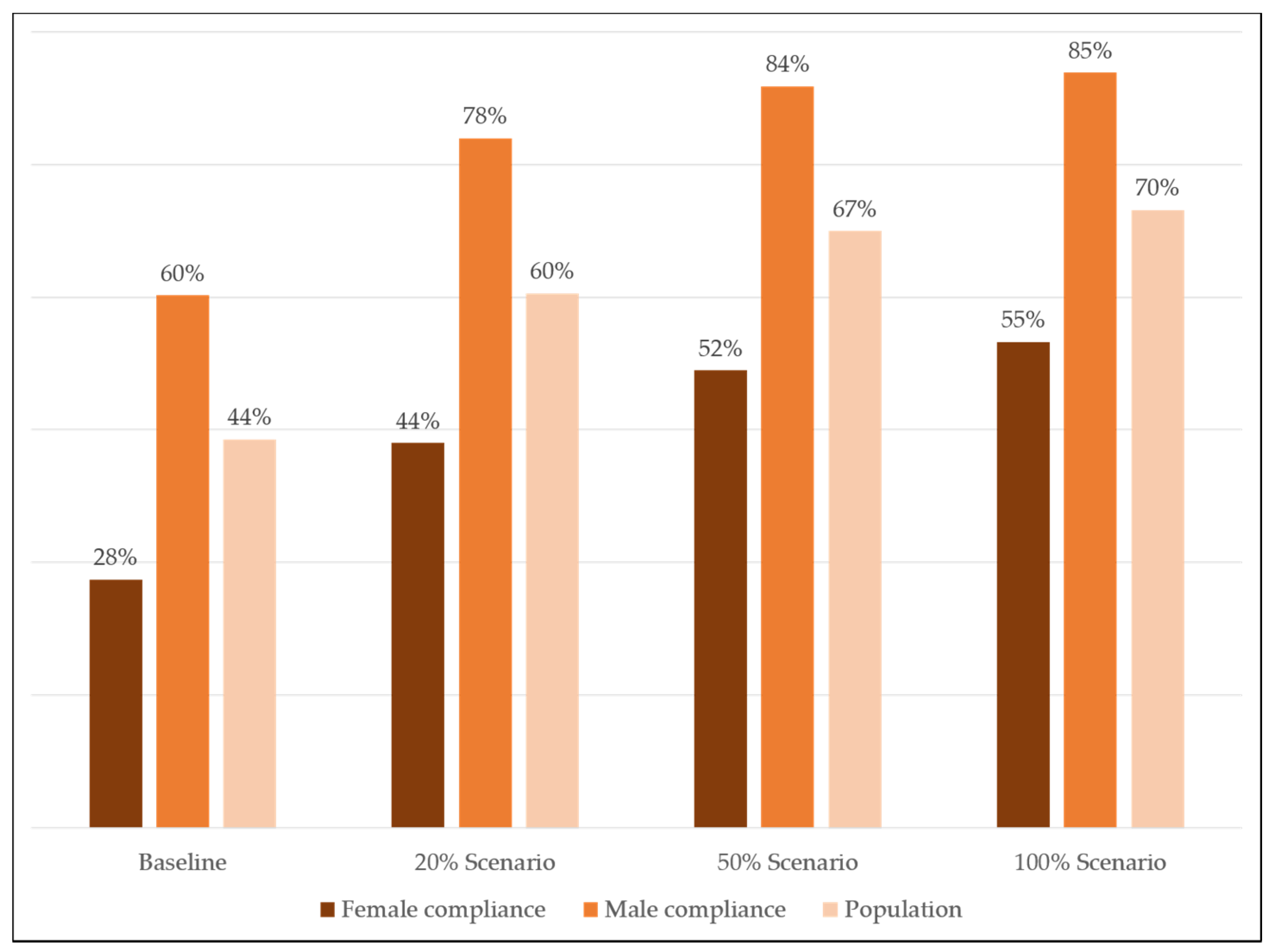
3.2. Impact of Reformulation on Intake
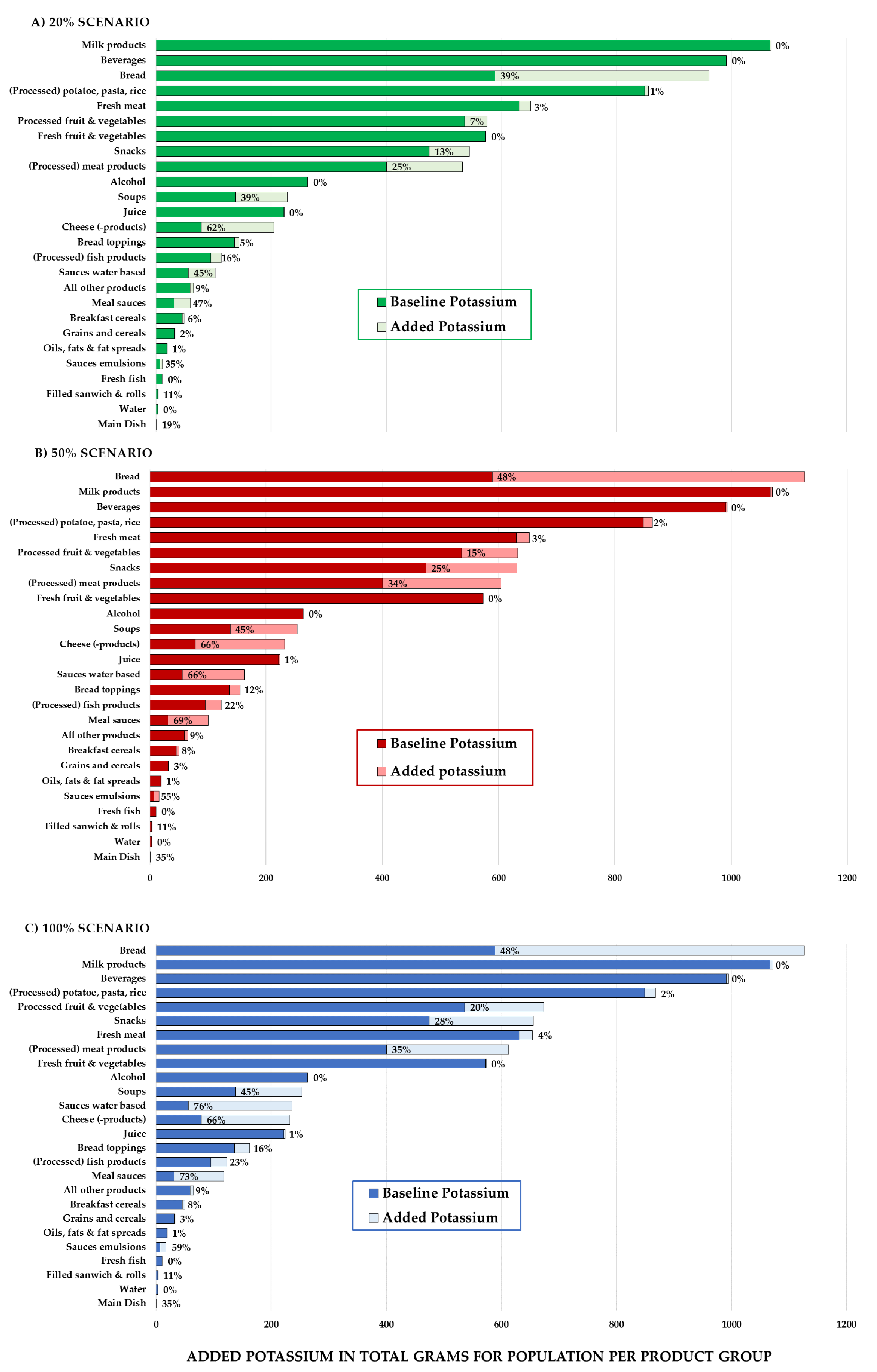
3.3. Impact of Reformulation per Food Group
4. Discussion
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| DNFCS | Dutch National Food Consumption Survey |
| EFSA | European Food Safety Authority |
| IQR | Interquartile range |
| NEVO | Nederlands Voedingsstoffenbestand (Dutch Food Composition Database) |
| RIVM | Rijksinstituut Voor Volksgezondheid en Milieu (Dutch National Institute for Public Health and the Environment) |
| WHO | World Health Organization |
References
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analyses. BMJ 2013, 346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, F.J.; Li, J.; MacGregor, G.A. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ 2013, 346. [Google Scholar] [CrossRef] [PubMed]
- Powles, J.; Fahimi, S.; Micha, R.; Khatibzadeh, S.; Shi, P.; Ezzati, M.; Engell, R.; Lim, S.; Danaei, G.; Mozaffarian, D. Global, regional and national sodium intakes in 1990 and 2010: A systematic analysis of 24 h urinary sodium excretion and dietary surveys worldwide. BMJ Open 2013, 3. [Google Scholar] [CrossRef] [PubMed]
- Dötsch-Klerk, M.; PMM Goossens, W.; Meijer, G.W.; van het Hof, K.H. Reducing salt in food; setting product-specific criteria aiming at a salt intake of 5 g per day. Eur. J. Clin. Nutr. 2015, 69, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Hendriksen, M.A.H.; Verkaik-Kloosterman, J.; Noort, M.W.; van Raaij, J.M.A. Nutritional impact of sodium reduction strategies on sodium intake from processed foods. Eur. J. Clin. Nutr. 2015, 69, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Bruins, M.J.; Dotsch-Klerk, M.; Matthee, J.; Kearney, M.; van Elk, K.; Weber, P.; Eggersdorfer, M. A Modelling Approach to Estimate the Impact of Sodium Reduction in Soups on Cardiovascular Health in the Netherlands. Nutrients 2015, 7, 8010–8019. [Google Scholar] [CrossRef] [PubMed]
- Hendriksen, M.A.H.; van Raaij, J.M.A.; Geleijnse, J.M.; Breda, J.; Boshuizen, H.C. Health Gain by Salt Reduction in Europe: A Modelling Study. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Nghiem, N.; Blakely, T.; Cobiac, L.J.; Pearson, A.L.; Wilson, N. Health and Economic Impacts of Eight Different Dietary Salt Reduction Interventions. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.E.; Brandeau, M.L.; Basu, S. Expansion of the National Salt Reduction Initiative: A Mathematical Model of Benefits and Risks of Population-Level Sodium Reduction. Med. Decis. Mak. 2016, 36, 72–85. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.; Kabir, Z.; Bennett, K.; Hotchkiss, J.W.; Kee, F.; Leyland, A.H.; Davies, C.; Bandosz, P.; Guzman-Castillo, M.; O’Flaherty, M.; et al. Modelling Future Coronary Heart Disease Mortality to 2030 in the British Isles. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Reducing Salt Intake in Populations. In Proceedings of the WHO Forum and Technical Meeting, Paris, France, 5–7 October 2006; WHO Document Production Services: Geneva, Switzerland, 2007. [Google Scholar]
- Zandstra, E.H.; Lion, R.; Newson, R.S. Salt reduction: Moving from consumer awareness to action. Food Qual. Preference 2016, 48, 376–381. [Google Scholar] [CrossRef]
- Liem, D.G.; Miremadi, F.; Keast, R.S.J. Reducing Sodium in Foods: The Effect on Flavor. Nutrients 2011, 3, 694–711. [Google Scholar] [CrossRef] [PubMed]
- Kloss, L.; Meyer, J.D.; Graeve, L.; Vetter, W. Sodium intake and its reduction by food reformulation in the European Union—A review. NFS J. 2015, 1, 9–19. [Google Scholar] [CrossRef]
- Murphy, C.; Cardello, A.V.; Brand, J.G. Tastes of fifteen halide salts following water and NaCl: Anion and cation effects. Physiol. Behav. 1981, 26, 1083–1095. [Google Scholar] [CrossRef]
- Van Der Klaauw, N.J.; Smith, D.V. Taste quality profiles for fifteen organic and inorganic salts. Physiol. Behav. 1995, 58, 295–306. [Google Scholar] [CrossRef]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses. BMJ 2013, 346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binia, A.; Jaeger, J.; Hu, Y.; Singh, A.; Zimmermann, D. Daily potassium intake and sodium-to-potassium ratio in the reduction of blood pressure: A meta-analysis of randomized controlled trials. J. Hypertens. 2015, 33, 1509–1520. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Guideline: Potassium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Morris, C.; Labarre, C.; Koliandris, A.L.; Hewson, L.; Wolf, B.; Taylor, A.J.; Hort, J. Effect of pulsed delivery and bouillon base on saltiness and bitterness perceptions of salt delivery profiles partially substituted with KCl. Food Qual. Preference 2010, 21, 489–494. [Google Scholar] [CrossRef]
- Mueller, E.; Koehler, P.; Scherf, K.A. Applicability of salt reduction strategies in pizza crust. Food Chem. 2016, 192, 1116–1123. [Google Scholar] [CrossRef] [PubMed]
- Charlton, K.E.; MacGregor, E.; Vorster, N.H.; Levitt, N.S.; Steyn, K. Partial replacement of NaCl can be achieved with potassium, magnesium and calcium salts in brown bread. Int. J. Food Sci. Nutr. 2007, 58, 508–521. [Google Scholar] [CrossRef] [PubMed]
- Braschi, A.; Gill, L.; Naismith, D.J. Partial substitution of sodium with potassium in white bread: Feasibility and bioavailability. Int. J. Food. Sci. Nutr. 2009, 60, 507–521. [Google Scholar] [CrossRef] [PubMed]
- Grummer, J.; Karalus, M.; Zhang, K.; Vickers, Z.; Schoenfuss, T.C. Manufacture of reduced-sodium Cheddar-style cheese with mineral salt replacers. J. Dairy Sci. 2012, 95, 2830–2839. [Google Scholar] [CrossRef] [PubMed]
- Katsiari, M.C.; Voutsinas, L.P.; Alichanidis, E.; Roussis, I.G. Reduction of sodium content in Feta cheese by partial substitution of NaCl by KCl. Int. Dairy J. 1997, 7, 465–472. [Google Scholar] [CrossRef]
- US Department of Agriculture and US Department of Health and Human Services. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans; US Department of Agriculture and US Department of Health and Human Services: Washington, DC, USA, 2010. [Google Scholar]
- Safe Upper Levels for Vitamins and Minerals. Expert Group on Vitamins and Minerals, FSA, 2013. Available online: https://cot.food.gov.uk/sites/default/files/vitmin2003.pdf (accessed on 25 February 2016).
- U.S. Food and Drug Administration (FDA). CFR-Code of Federal Regulations Title 21. Part 184—Direct Food Substances Affirmed as Generally Recognized as Safe, Subpart B—Listing of Specific Substances Affirmed as GRAS, Section 184.1622 Potassium Chloride. Available online: http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=184.1622 (accessed on 25 February 2016).
- JECFA. Evaluation of Certain Food Additives—Chloride: Ammonium, Magnesium, Potassium; Twenty-third Report of the Joint FAO/WHO Expert Committee on Food Additives (JECFA); WHO Technical Report Series: Geneva, Switzerland, 1980. [Google Scholar]
- EFSA Panel on Dietetic Products NaAN. Scientific Opinion on the substantiation of health claims related to potassium and maintenance of normal muscular and neurological function (ID 320, 386) and maintenance of normal blood pressure (ID 321) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J. 2010, 8, 1469. [Google Scholar]
- European Food Safety Authority. Opinion of the Scientific Panel on Dietetic Products, Nutrition and Allergies on a request from the Commission related to the Tolerable Upper Intake Level of Potassium. EFSA J. 2005, 193, 1–19. [Google Scholar]
- Drewnowski, A.; Rehm, C.D.; Maillot, M.; Mendoza, A.; Monsivais, P. The feasibility of meeting the WHO guidelines for sodium and potassium: A cross-national comparison study. BMJ Open 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- DNFCS-Core Survey (2007–2010). Part of the Dutch National Food Consumption Survey; National Institute for Public Health and the Environment: Bilthoven, The Netherlands, 2010. [Google Scholar]
- NEVO-table (Dutch Food Composition Database NEVO): Nederlands Voedingsstoffenbestand 2011. Available online: http://www.rivm.nl/nevo_en/nevo/ (accessed on 25 February 2016).
- Dazult Software. Available online: www.dazult.com (accessed on 25 February 2016).
- Statistical Software Package JMP. Available online: www.jmp.com (accessed on 25 February 2016).
- Whelton, P.K. Sodium, Potassium, Blood Pressure, and Cardiovascular Disease. Humans. Curr. Hypertens. Rep. 2014, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Perez, V.; Chang, E.T. Sodium-to-Potassium Ratio and Blood Pressure, Hypertension, and Related Factors, 2014, American Society for Nutrition. Adv. Nutr. 2014, 5, 712–741. [Google Scholar] [CrossRef] [PubMed]
- Newson, R.S.; Elmadfa, I.; Biro, G.; Cheng, Y.; Prakash, V.; Rust, P.; Barna, M.; Lion, R.; Meijer, G.W.; Neufingerl, N.; et al. Barriers for progress in salt reduction in the general population. Int. Study Appet. 2013, 71, 22–31. [Google Scholar]
- Kieneker, L.M.; Gansevoort, R.T.; de Boer, R.A.; Brouwers, F.P.; Feskens, E.J.M.; Geleijnse, J.M.; Navis, G.; Bakker, S.J.L.; Joosten, M.M. Urinary potassium excretion and risk of cardiovascular events. Am J. Clin. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Men (N = 1048) | Women (N = 1058) | Total (N = 2106) |
|---|---|---|---|
| Age (years) | |||
| Mean | 39 | 39 | 39 |
| Standard deviation | 15 | 15 | 15 |
| Minimum | 18 | 18 | 18 |
| Maximum | 65 | 65 | 65 |
| BMI (kg/m2) | |||
| Mean | 26 | 25 | 25 |
| Standard deviation | 4 | 6 | 5 |
| Minimum | 16 | 14 | 14 |
| Maximum | 49 | 57 | 57 |
| Energy intake at baseline (kcal/day) | |||
| Median | 2619 | 1911 | 2230 |
| IQR | 964 | 712 | 990 |
| Minimum | 418 | 279 | 279 |
| Maximum | 8139 | 4658 | 8139 |
| Sodium intake at baseline (mg/day) * | |||
| Median | 3101 | 2302 | 2649 |
| IQR | 1304 | 1060 | 1310 |
| Minimum | 400 | 331 | 331 |
| Maximum | 8726 | 6068 | 8726 |
| Potassium intake at baseline (mg/day) | |||
| Median | 3789 | 2946 | 3334 |
| IQR | 1485 | 1204 | 1434 |
| Minimum | 804 | 704 | 704 |
| Maximum | 8798 | 8723 | 8798 |
| Food Group Men | Women | All | |
|---|---|---|---|
| Milk products | 14.5% | 14.7% | 14.6% |
| Beverages | 13.4% | 13.7% | 13.6% |
| (Processed) potato, pasta, rice | 12.6% | 10.4% | 11.6% |
| Fresh meat | 8.9% | 8.3% | 8.6% |
| Bread | 8.2% | 7.9% | 8.1% |
| Fresh fruit and vegetables | 6.2% | 9.9% | 7.8% |
| Processed fruit & vegetables | 6.8% | 8.0% | 7.3% |
| Snacks | 6.2% | 6.9% | 6.5% |
| (Processed) meat products | 6.1% | 4.7% | 5.5% |
| Alcohol | 4.8% | 2.1% | 3.6% |
| Juice | 2.7% | 3.5% | 3.0% |
| Soups | 1.9% | 1.9% | 1.9% |
| Bread toppings | 1.9% | 1.8% | 1.9% |
| (Processed) fish products | 1.2% | 1.4% | 1.3% |
| 12 remaining food groups | 4.6% | 4.9% | 4.7% |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Buren, L.; Dötsch-Klerk, M.; Seewi, G.; Newson, R.S. Dietary Impact of Adding Potassium Chloride to Foods as a Sodium Reduction Technique. Nutrients 2016, 8, 235. https://doi.org/10.3390/nu8040235
Van Buren L, Dötsch-Klerk M, Seewi G, Newson RS. Dietary Impact of Adding Potassium Chloride to Foods as a Sodium Reduction Technique. Nutrients. 2016; 8(4):235. https://doi.org/10.3390/nu8040235
Chicago/Turabian StyleVan Buren, Leo, Mariska Dötsch-Klerk, Gila Seewi, and Rachel S. Newson. 2016. "Dietary Impact of Adding Potassium Chloride to Foods as a Sodium Reduction Technique" Nutrients 8, no. 4: 235. https://doi.org/10.3390/nu8040235
APA StyleVan Buren, L., Dötsch-Klerk, M., Seewi, G., & Newson, R. S. (2016). Dietary Impact of Adding Potassium Chloride to Foods as a Sodium Reduction Technique. Nutrients, 8(4), 235. https://doi.org/10.3390/nu8040235