The Effect of Salt Intake and Potassium Supplementation on Serum Gastrin Levels in Chinese Adults: A Randomized Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Dietary Intervention
2.3. BP Measurement
2.4. Biochemical Analyses
2.5. 24 h Urinary Sodium, Potassium and Creatinine Determination
2.6. Statistical Analyses
3. Results
3.1. Profiles of Studied Subjects
3.2. Effects of Salt Intake and Potassium Supplementation on BP and 24 h Urinary Sodium and Potassium Excretion
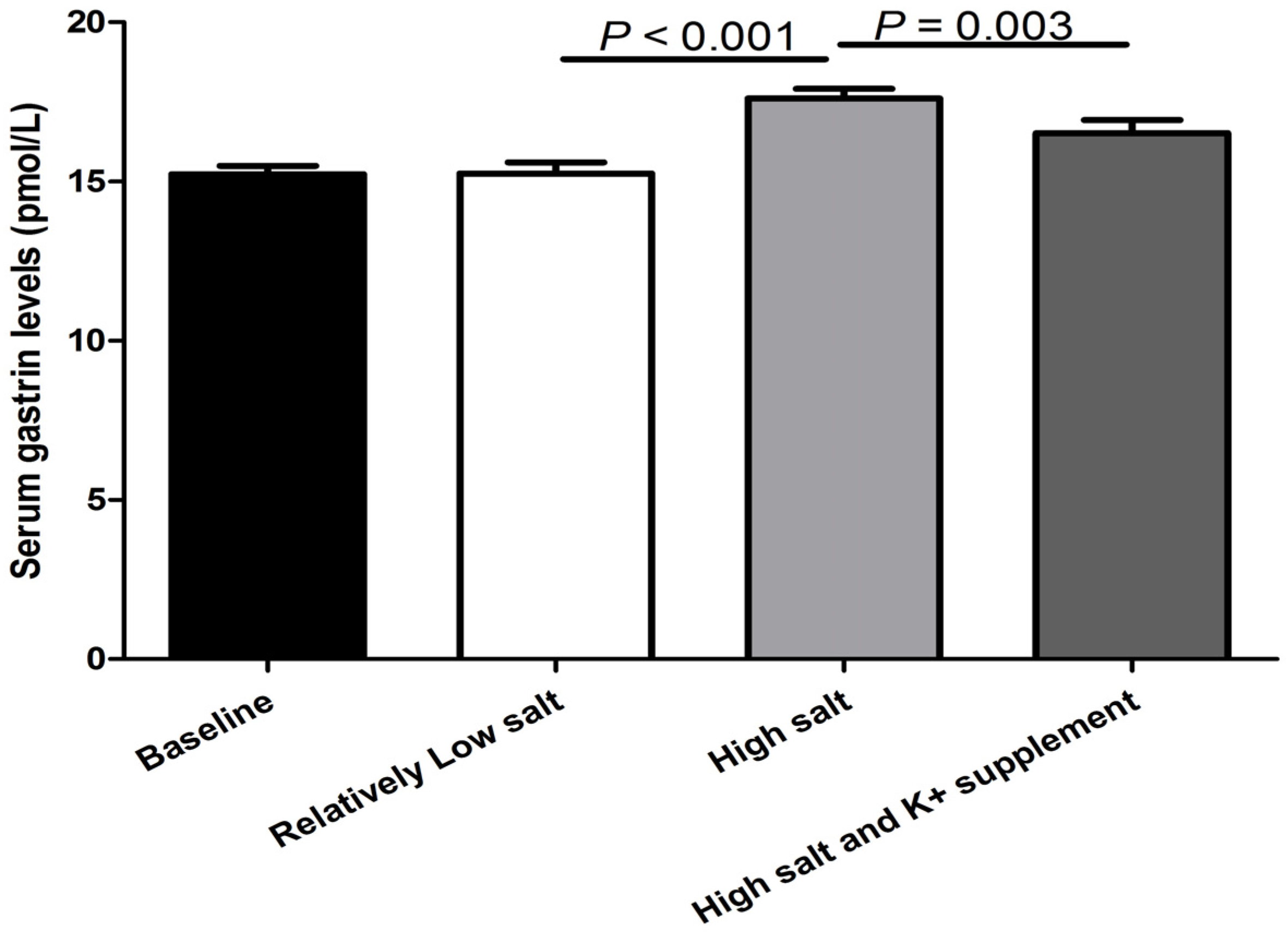
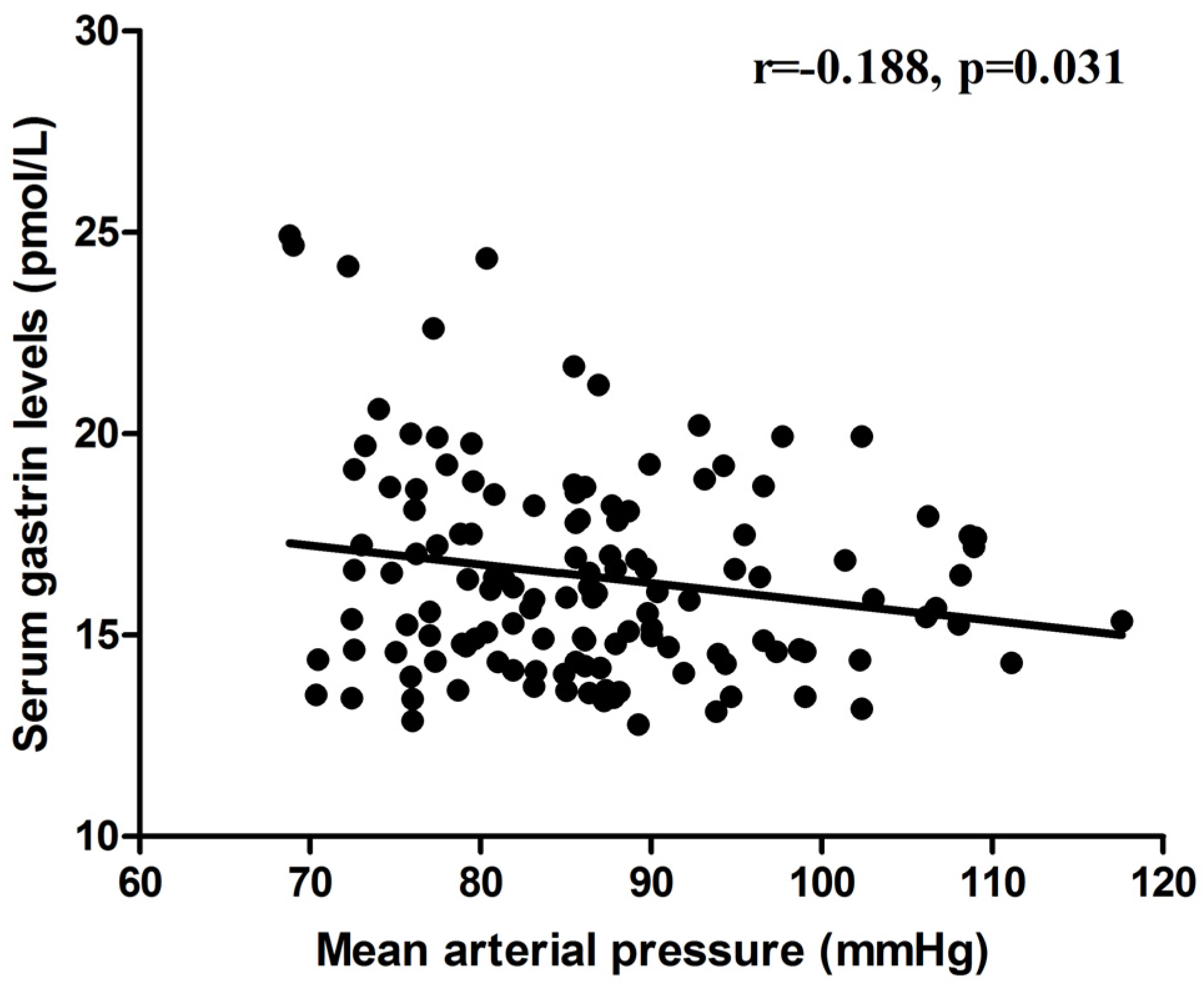
3.3. Effects of Salt Intake and Potassium Supplementation on Fasting Gastrin Levels
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- O’Donnell, M.; Mente, A.; Yusuf, S. Evidence relating sodium intake to blood pressure and CVD. Curr. Cardiol. Rep. 2014, 16, 529. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; MacGregor, G.A. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J. Hum. Hypertens. 2009, 23, 363–384. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.; Mente, A.; Yusuf, S. Sodium intake and cardiovascular health. Circ. Res. 2015, 116, 1046–1057. [Google Scholar] [CrossRef] [PubMed]
- Appel, L.J.; Frohlich, E.D.; Hall, J.E.; Pearson, T.A.; Sacco, R.L.; Seals, D.R.; Sacks, F.M.; Smith, S.C., Jr.; Vafiadis, D.K.; van Horn, L.V. The importance of population-wide sodium reduction as a means to prevent cardiovascular disease and stroke: A call to action from the American Heart Association. Circulation 2011, 123, 1138–1143. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Mori, T.; Huang, T.; Lombard, J.H. Effect of high-salt diet on NO release and superoxide production in rat aorta. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, H575–H583. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; White, J.; Guo, L.; Zhao, X.; Wang, J.; Smart, E.J.; Li, X.A. Salt inactivates endothelial nitric oxide synthase in endothelial cells. J. Nutr. 2009, 139, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Oberleithner, H.; Riethmuller, C.; Schillers, H.; MacGregor, G.A.; de Wardener, H.E.; Hausberg, M. Plasma sodium stiffens vascular endothelium and reduces nitric oxide release. Proc. Natl. Acad. Sci. USA 2007, 104, 16281–16286. [Google Scholar] [CrossRef] [PubMed]
- Lastra, G.; Dhuper, S.; Johnson, M.S.; Sowers, J.R. Salt, aldosterone, and insulin resistance: Impact on the cardiovascular system. Nat. Rev. Cardiol. 2010, 7, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Michell, A.R.; Debnam, E.S.; Unwin, R.J. Regulation of renal function by the gastrointestinal tract: Potential role of gut-derived peptides and hormones. Annu. Rev. Physiol. 2008, 70, 379–403. [Google Scholar] [CrossRef] [PubMed]
- Wank, S.A. G protein-coupled receptors in gastrointestinal physiology. I.CCK receptors: An exemplary family. Am. J. Physiol. 1998, 274, G607–G613. [Google Scholar] [PubMed]
- Pisegna, J.R.; Tarasova, N.I.; Kopp, J.A.; Jose, P.; Farnsworth, D.W.; Michejda, C.J.; Wank, S.A. Postprandial changes in renal function are mediated by elevated serum gastrin acting at cholecystokinin type B receptors (CCKBR) in the kidney. Regul. Pept. 1996, 64, 151. [Google Scholar]
- Koh, T.J. Extragastric effects of gastrin gene knock-out mice. Pharmacol. Toxicol. 2002, 91, 368–374. [Google Scholar] [CrossRef] [PubMed]
- De Weerth, A.; Jonas, L.; Schade, R.; Schoneberg, T.; Wolf, G.; Pace, A.; Kirchhoff, F.; Schulz, M.; Heinig, T.; Greten, H.; et al. Gastrin/cholecystokinin type B receptors in the kidney: Molecular, pharmacological, functional characterization, and localization. Eur. J. Clin. Investig. 1998, 28, 592–601. [Google Scholar] [CrossRef]
- Dufresne, M.; Seva, C.; Fourmy, D. Cholecystokinin and gastrin receptors. Physiol. Rev. 2006, 86, 805–847. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Asico, L.D.; Zheng, S.; Villar, V.A.; He, D.; Zhou, L.; Zeng, C.; Jose, P.A. Gastrin and D1 dopamine receptor interact to induce natriuresis and diuresis. Hypertension 2013, 62, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Melis, M.; Krenning, E.P.; Bernard, B.F.; de Visser, M.; Rolleman, E.; de Jong, M. Renal uptake and retention of radiolabeled somatostatin, bombesin, neurotensin, minigastrin and CCK analogues: Species and gender differences. Nucl. Med. Biol. 2007, 34, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Adrogue, H.J.; Madias, N.E. Sodium and potassium in the pathogenesis of hypertension. N. Engl. J. Med. 2007, 356, 1966–1978. [Google Scholar] [CrossRef] [PubMed]
- Brunner, H.R.; Baer, L.; Sealey, J.E.; Ledingham, J.G.; Laragh, J.H. The influence of potassium administration and of potassium deprivation on plasma renin in normal and hypertensive subjects. J. Clin. Investig. 1970, 49, 2128–2138. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R.; Obarzanek, E.; Cutler, J.A.; Buring, J.E.; Rexrode, K.M.; Kumanyika, S.K.; Appel, L.J.; Whelton, P.K. Joint effects of sodium and potassium intake on subsequent cardiovascular disease: The Trials of Hypertension Prevention follow-up study. Arch. Intern. Med. 2009, 169, 32–40. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Marciniak, M.; Carney, C.; Markandu, N.D.; Anand, V.; Fraser, W.D.; Dalton, R.N.; Kaski, J.C.; MacGregor, G.A. Effects of potassium chloride and potassium bicarbonate on endothelial function, cardiovascular risk factors, and bone turnover in mild hypertensives. Hypertension 2010, 55, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Waitzberg, D.L.; Logullo, L.C.; Bittencourt, A.F.; Torrinhas, R.S.; Shiroma, G.M.; Paulino, N.P.; Teixeira-da-Silva, M.L. Effect of synbiotic in constipated adult women—A randomized, double-blind, placebo-controlled study of clinical response. Clin. Nutr. 2013, 32, 27–33. [Google Scholar] [CrossRef] [PubMed]
- GenSalt Collaborative Research Group. GenSalt: Rationale, design, methods and baseline characteristics of study participants. J. Hum. Hypertens. 2007, 21, 639–646. [Google Scholar]
- Gu, D.; Zhao, Q.; Chen, J.; Chen, J.C.; Huang, J.; Bazzano, L.A.; Lu, F.; Mu, J.; Li, J.; Cao, J.; et al. Reproducibility of blood pressure responses to dietary sodium and potassium interventions: The GenSalt study. Hypertension 2013, 62, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; Ji, C.; Donfrancesco, C.; Palmieri, L.; Ippolito, R.; Vanuzzo, D.; Giampaoli, S.; Strazzullo, P. Geographic and socioeconomic variation of sodium and potassium intake in Italy: Results from the MINISAL-GIRCSI programme. BMJ Open 2015, 5, e007467. [Google Scholar] [CrossRef] [PubMed]
- Fukae, H.; Kinoshita, H.; Fujimoto, S.; Kita, T.; Nakazato, M.; Eto, T. Changes in urinary levels and renal expression of uroguanylin on low or high salt diets in rats. Nephron 2002, 92, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, J.N.; Nieman, M.; Sabo, J.; Sanford, L.P.; Hawkins, J.A.; Elitsur, N.; Gawenis, L.R.; Clarke, L.L.; Cohen, M.B. Uroguanylin knockout mice have increased blood pressure and impaired natriuretic response to enteral NaCl load. J. Clin. Investig. 2003, 112, 1244–1254. [Google Scholar] [CrossRef] [PubMed]
- Rehfeld, J.F.; Friis-Hansen, L.; Goetze, J.P.; Hansen, T.V. The biology of cholecystokinin and gastrin peptides. Curr. Top. Med. Chem. 2007, 7, 1154–1165. [Google Scholar] [CrossRef] [PubMed]
- Von, S.T.; Ahrens, M.; de Weerth, A.; Bobrowski, C.; Wolf, G.; Jonas, L.; Jocks, T.; Schulz, M.; Blaker, M.; Neumaier, M.; et al. CCKB/gastrin receptors mediate changes in sodium and potassium absorption in the isolated perfused rat kidney. Kidney Int. 2000, 58, 995–1003. [Google Scholar]
- Liu, T.; Jose, P.A. Gastrin induces sodium-hydrogen exchanger 3 phosphorylation and mTOR activation via a phosphoinositide 3-kinase-/protein kinase C-dependent but AKT-independent pathway in renal proximal tubule cells derived from a normotensive male human. Endocrinology 2013, 154, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Konkalmatt, P.R.; Yang, Y.; Jose, P.A. Gastrin decreases Na+,K+-ATPase activity via a PI 3-kinase- and PKC-dependent pathway in human renal proximal tubule cells. Am. J. Physiol. Endocrinol. Metab. 2016, 310, E565–E571. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Ehret, G.B.; Rice, K.; Verwoert, G.C.; Launer, L.J.; Dehghan, A.; Glazer, N.L.; Morrison, A.C.; Johnson, A.D.; Aspelund, T.; et al. Genome-wide association study of blood pressure and hypertension. Nat. Genet. 2009, 41, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.S.; Go, M.J.; Kim, Y.J.; Heo, J.Y.; Oh, J.H.; Ban, H.J.; Yoon, D.; Lee, M.H.; Kim, D.J.; Park, M.; et al. A large-scale genome-wide association study of Asian populations uncovers genetic factors influencing eight quantitative traits. Nat. Genet. 2009, 41, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Wang, W.; Ning, B.; Liu, X.; Gong, J.; Gan, F.; Gao, X.; Zhang, L.; Jose, P.A.; Qin, C.; et al. Basal and postprandial serum levels of gastrin in normotensive and hypertensive adults. Clin. Exp. Hypertens. 2013, 35, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Banday, A.A.; Lokhandwala, M.F. Novel gastro-renal axis and sodium regulation during hypertension. Hypertension 2013, 62, 834–835. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Values |
|---|---|
| Age, year | 51.8 ± 1.1 |
| Sex (M/F) | 21/23 |
| Body mass index, kg/m2 | 23.5 ± 0.4 |
| Alcohol (n, %) | 4 (9.1) |
| Smoking (n, %) | 19 (43.2) |
| Hypertension (n, %) | 5 (11.4) |
| Systolic blood pressure, mmHg | 110.4 ± 2.2 |
| Diastolic blood pressure, mmHg | 72.5 ± 1.3 |
| Mean arterial pressure, mmHg | 85.1 ± 1.5 |
| Glucose, mmol/L | 3.91 ± 0.10 |
| Total cholesterol, mmol/L | 4.11 ± 0.13 |
| Triglycerides, mmol/L | 1.24 ± 0.08 |
| LDL-cholesterol, mmol/L | 2.30 ± 0.11 |
| HDL-cholesterol, mmol/L | 1.20 ± 0.04 |
| Serum creatinine, umol/L | 56.6 ± 1.3 |
| Periods | SBP | DBP | 24-h Urinary Na+ | 24-h Urinary K+ | 24-h Urinary Creatinine |
|---|---|---|---|---|---|
| Baseline | 110.4 ± 2.2 | 72.5 ± 1.3 | 173.7 ± 10.5 | 47.0 ± 3.0 | 9002.7 ± 519.0 |
| Relatively low salt | 108.8 ± 1.9 | 73.8 ± 1.1 | 101.2 ± 5.8 § | 37.9 ± 2.9 § | 8248.2 ± 350.2 |
| High salt | 116.2 ± 2.7 * | 76.9 ± 1.3 * | 251.7 ± 9.3 * | 42.3 ± 4.1 | 8462.1 ± 574.3 |
| High salt and K+ supplement | 107.3 ± 2.0 † | 71.9 ± 1.3 † | 266.0 ± 13.5 | 73.0 ± 4.0 † | 8839.8 ± 668.9 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-Y.; He, W.-W.; Liu, Y.-C.; Lin, Y.-F.; Hong, L.-F. The Effect of Salt Intake and Potassium Supplementation on Serum Gastrin Levels in Chinese Adults: A Randomized Trial. Nutrients 2017, 9, 389. https://doi.org/10.3390/nu9040389
Wang Y-Y, He W-W, Liu Y-C, Lin Y-F, Hong L-F. The Effect of Salt Intake and Potassium Supplementation on Serum Gastrin Levels in Chinese Adults: A Randomized Trial. Nutrients. 2017; 9(4):389. https://doi.org/10.3390/nu9040389
Chicago/Turabian StyleWang, Yuan-Yuan, Wen-Wen He, Yan-Chun Liu, Yi-Feng Lin, and Lu-Fei Hong. 2017. "The Effect of Salt Intake and Potassium Supplementation on Serum Gastrin Levels in Chinese Adults: A Randomized Trial" Nutrients 9, no. 4: 389. https://doi.org/10.3390/nu9040389
APA StyleWang, Y. -Y., He, W. -W., Liu, Y. -C., Lin, Y. -F., & Hong, L. -F. (2017). The Effect of Salt Intake and Potassium Supplementation on Serum Gastrin Levels in Chinese Adults: A Randomized Trial. Nutrients, 9(4), 389. https://doi.org/10.3390/nu9040389