Impact of Maternal Selenium Status on Infant Outcome during the First 6 Months of Life

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Clinical Data
2.3. Selenium Analysis of Blood and Breastmilk
2.4. Statistical Analysis
3. Results
3.1. Demographics and Nutrition
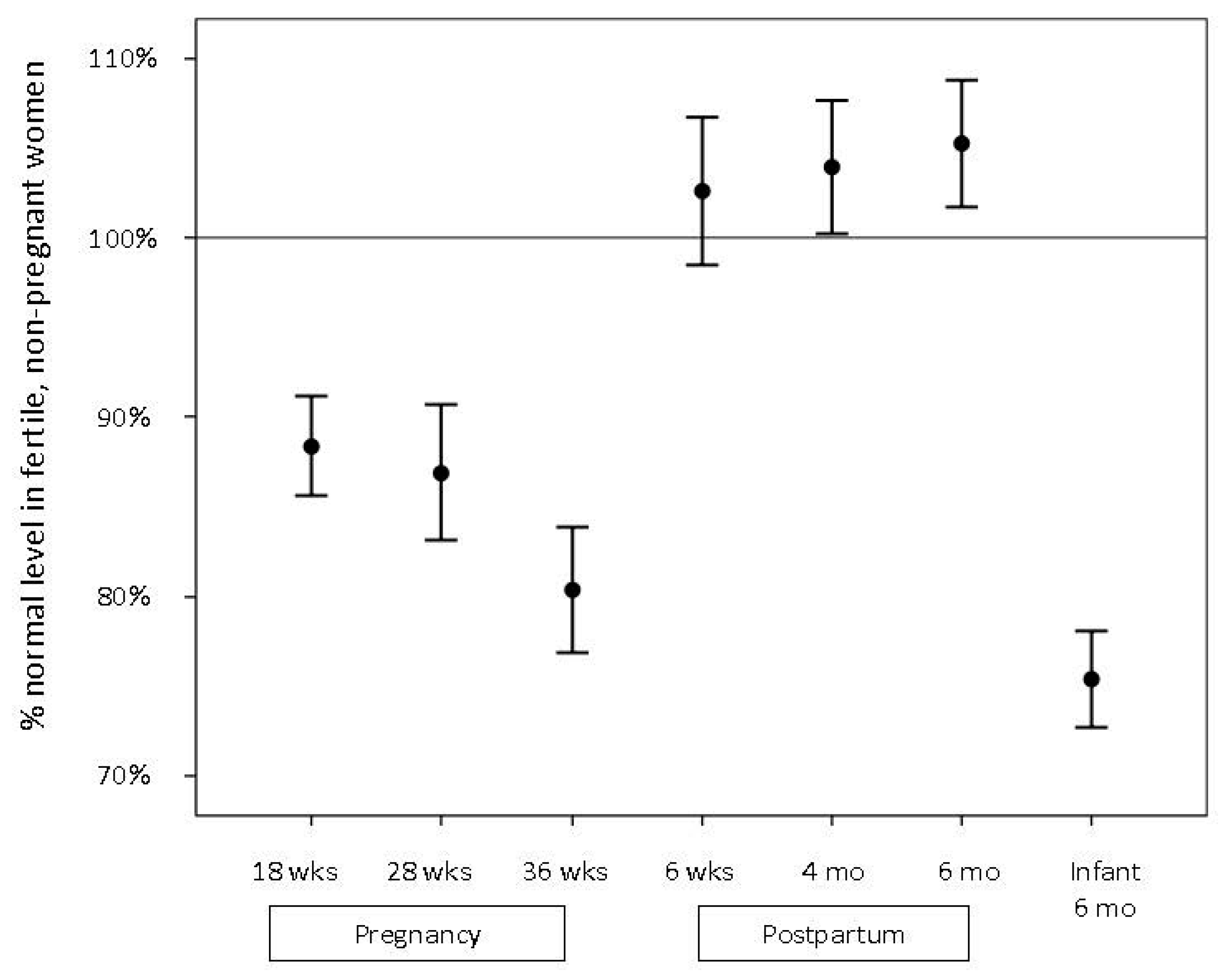
3.2. Selenium Levels in Pregnant, Lactating, and Never-Pregnant Women
3.3. Selenium Levels in Breastmilk
3.4. Selenium Levels in Infants at 6 Months
3.5. Selenium Levels and Infant Neurodevelopment
3.6. Selenium Levels and Infant Infections
4. Discussion
4.1. Serum Selenium Levels in Never-Pregnant, Pregnant, and Lactating Women
4.2. Selenium Levels in Breastmilk
4.3. Selenium Intake and Serum Levels in Infants
4.4. Selenium Levels and Infant Clinical Status
4.5. Strength and Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflict of Interest
References
- Rayman, M.P. The importance of selenium to human health. Lancet 2000, 356, 233–241. [Google Scholar] [CrossRef]
- Spallholz, J.E.; Boylan, L.M.; Larsen, H.S. Advances in understanding selenium’s role in the immune system. Ann. N. Y. Acad. Sci. 1990, 587, 123–139. [Google Scholar] [CrossRef] [PubMed]
- Kiremidjian-Schumacher, L.; Roy, M.; Wishe, H.I.; Cohen, M.W.; Stotzky, G. Supplementation with selenium and human immune cell functions. II. Effect on cytotoxic lymphocytes and natural killer cells. Biol. Trace Elem. Res. 1994, 41, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Guvenc, H.; Karatas, F.; Guvenc, M.; Kunc, S.; Aygun, A.D.; Bektas, S. Low levels of selenium in mothers and their newborns in pregnancies with a neural tube defect. Pediatrics 1995, 95, 879–882. [Google Scholar] [PubMed]
- Skroder, H.M.; Hamadani, J.D.; Tofail, F.; Persson, L.A.; Vahter, M.E.; Kippler, M.J. Selenium status in pregnancy influences children’s cognitive function at 1.5 years of age. Clin. Nutr. 2015, 34, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Polanska, K.; Krol, A.; Sobala, W.; Gromadzinska, J.; Brodzka, R.; Calamandrei, G.; Chiarotti, F.; Wasowicz, W.; Hanke, W. Selenium status during pregnancy and child psychomotor development-Polish Mother and Child Cohort study. Pediatr. Res. 2016, 79, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Costantine, M.M. Physiologic and pharmacokinetic changes in pregnancy. Front. Pharmacol. 2014, 5, 65. [Google Scholar] [CrossRef] [PubMed]
- Hansen, S.; Nieboer, E.; Sandanger, T.M.; Wilsgaard, T.; Thomassen, Y.; Veyhe, A.S.; Odland, J.Ø. Changes in maternal blood concentrations of selected essential and toxic elements during and after pregnancy. J. Environ. Monit. 2011, 13, 2143–2152. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo Alvarez, S.; Castanon, S.G.; Ruata, M.L.; Aragues, E.F.; Terraz, P.B.; Irazabal, Y.G.; González, E.G.; Rodríquez, B.G. Updating of normal levels of copper, zinc and selenium in serum of pregnant women. J. Trace Elem. Med. Biol. 2007, 21, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Dorea, J.G. Selenium and breast-feeding. Br. J. Nutr. 2002, 88, 443–461. [Google Scholar] [CrossRef] [PubMed]
- Muntau, A.C.; Streiter, M.; Kappler, M.; Roschinger, W.; Schmid, I.; Rehnert, A.; Schramel, P.; Roscher, A.A. Age-related reference values for serum selenium concentrations in infants and children. Clin. Chem. 2002, 48, 555–560. [Google Scholar] [PubMed]
- Jacobson, B.E.; Lockitch, G. Direct determination of selenium in serum by graphite-furnace atomic absorption spectrometry with deuterium background correction and a reduced palladium modifier: age-specific reference ranges. Clin. Chem. 1988, 34, 709–714. [Google Scholar] [PubMed]
- Rossipal, E.; Tiran, B. Selenium and glutathione peroxidase levels in healthy infants and children in Austria and the influence of nutrition regimens on these levels. Nutrition 1995, 11, 573–575. [Google Scholar] [PubMed]
- Birgisdottir, B.E.; Knutsen, H.K.; Haugen, M.; Gjelstad, I.M.; Jenssen, M.T.; Ellingsen, D.G.; Thomassen, Y.; Alexander, J.; Meltzer, H.M.; Brantsaeter, A.L. Essential and toxic element concentrations in blood and urine and their associations with diet: results from a Norwegian population study including high-consumers of seafood and game. Sci. Total Environ. 2013, 463–464, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Gao, D.; He, Z.; Wu, J.; Ma, Q.; Song, H.; Mei, L.; Wu, Y. Long-term results of combined splenorenal shunt and porta-azygos devascularization in patients with portal hypertension. Zhonghua Wai Ke Za Zhi 1998, 36, 327–329. (In Chinese) [Google Scholar] [PubMed]
- Schonhaut, L.; Armijo, I.; Schonstedt, M.; Alvarez, J.; Cordero, M. Validity of the ages and stages questionnaires in term and preterm infants. Pediatrics 2013, 131, 1468–1474. [Google Scholar] [CrossRef] [PubMed]
- Bolann, B.J.; Distante, S.; Morkrid, L.; Ulvik, R.J. Bloodletting therapy in hemochromatosis: Does it affect trace element homeostasis? J. Trace Elem. Med. Biol. 2015, 31, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Matos, C.; Moutinho, C.; Almeida, C.; Guerra, A.; Balcao, V. Trace element compositional changes in human milk during the first four months of lactation. Int. J. Food Sci. Nutr. 2014, 65, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Lung, F.W.; Shu, B.C.; Chiang, T.L.; Lin, S.J. Twin-singleton influence on infant development: A national birth cohort study. Child Care Health Dev. 2009, 35, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Hurst, R.; Armah, C.N.; Dainty, J.R.; Hart, D.J.; Teucher, B.; Goldson, A.J.; Broadlev, M.R.; Motley, A.K.; Fairweather-Tait, S.J. Establishing optimal selenium status: results of a randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2010, 91, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Niskar, A.S.; Paschal, D.C.; Kieszak, S.M.; Flegal, K.M.; Bowman, B.; Gunter, E.W.; Pirkle, J.L.; Rubin, C.; Sampson, E.J.; McGeehin, M. Serum selenium levels in the US population: Third National Health and Nutrition Examination Survey, 1988–1994. Biol. Trace Elem. Res. 2003, 91, 1–10. [Google Scholar] [CrossRef]
- Kipp, A.P.; Strohm, D.; Brigelius-Flohe, R.; Schomburg, L.; Bechthold, A.; Leschik-Bonnet, E.; Heseker, H. Revised reference values for selenium intake. J. Trace Elem. Med. Biol. 2015, 32, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Trafikowska, U.; Zachara, B.A.; Wiacek, M.; Sobkowiak, E.; Czerwionka-Szaflarska, M. Selenium supply and glutathione peroxidase activity in breastfed Polish infants. Acta Paediatr. 1996, 85, 1143–1145. [Google Scholar] [CrossRef] [PubMed]
- Monsen, A.L.; Refsum, H.; Markestad, T.; Ueland, P.M. Cobalamin status and its biochemical markers methylmalonic acid and homocysteine in different age groups from 4 days to 19 years. Clin Chem. 2003, 49, 2067–2075. [Google Scholar] [CrossRef] [PubMed]
- Greibe, E.; Lildballe, D.L.; Streym, S.; Vestergaard, P.; Rejnmark, L.; Mosekilde, L.; Nexo, E. Cobalamin and haptocorrin in human milk and cobalamin-related variables in mother and child: a 9-mo longitudinal study. Am. J. Clin Nutr. 2013, 98, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Lozoff, B.; Beard, J.; Connor, J.; Barbara, F.; Georgieff, M.; Schallert, T. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutr. Rev. 2006, 64, S34–S43. [Google Scholar] [CrossRef] [PubMed]
- Alvik, A.; Groholt, B. Examination of the cut-off scores determined by the Ages and Stages Questionnaire in a population-based sample of 6 month-old Norwegian infants. BMC Pediatr. 2011, 11, 117. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, C.; Satoh, H. Brain selenium status and behavioral development in selenium-deficient preweanling mice. Physiol. Behav. 1994, 56, 927–932. [Google Scholar] [CrossRef]
- Kupka, R.; Mugusi, F.; Aboud, S.; Msamanga, G.I.; Finkelstein, J.L.; Spiegelman, D.; Fawzi, W.W. Randomized, double-blind, placebo-controlled trial of selenium supplements among HIV-infected pregnant women in Tanzania: effects on maternal and child outcomes. Am. J. Clin Nutr. 2008, 87, 1802–1808. [Google Scholar] [PubMed]
- Stiles, J.; Jernigan, T.L. The basics of brain development. Neuropsychol. Rev. 2010, 20, 327–348. [Google Scholar] [CrossRef] [PubMed]
- MRC Vitamin Study Research Group. Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet 1991, 338, 131–137. [Google Scholar]
- Kiremidjian-Schumacher, L.; Roy, M.; Wishe, H.I.; Cohen, M.W.; Stotzky, G. Regulation of cellular immune responses by selenium. Biol. Trace Elem. Res. 1992, 33, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Heineman, K.R.; Hadders-Algra, M. Evaluation of neuromotor function in infancy—A systematic review of available methods. J. Dev. Behav. Pediatr. 2008, 29, 315–323. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Never-Pregnant Women | Pregnant Women | p Value | |
|---|---|---|---|
| n = 158 | n = 114 | ||
| Age, year, mean + SD | 25.3 + 4.8 | 31.5 + 4.3 | <0.001 * |
| Prepregnancy BMI, kg/m2, mean + SD | 22.5 + 3.0 | 22.8 + 3.1 | 0.38 * |
| Higher education, n (%) ** | 93 (60) | 67 (59) | 0.96 *** |
| Para 0, n (%) | 158 (100) | 63 (55) | <0.001 *** |
| Smoking, n (%) | 4 (3) | 2 (2) | 0.65 *** |
| Regular use of micronutrient supplements (≥3 days/week), n (%) | 35 (22) | 47 (41) | 0.001 *** |
| Serum Selenium, µmol/L | Never-Pregnant Women n = 158 | Pregnant Women | Postpartum Women | Infants 6 Months n = 91 | ||||
|---|---|---|---|---|---|---|---|---|
| Week 18 n = 108 | Week 28 n = 114 | Week 36 n = 114 | 6 Weeks n = 113 | 4 Months n = 113 | 6 Months n = 114 | |||
| Median | 1.07 | 0.96 | 0.92 | 0.85 | 1.07 | 1.08 | 1.11 | 0.81 |
| (25, 75) * | (0.98, 1.16) | (0.86, 1.04) | (0.81, 1.03) | (0.75, 0.96) | (0.96, 1.20) | (0.98, 1.24) | (1.00, 1.25) | (0.74, 0.89) |
| (2.5, 97.5) * | (0.81, 1.59) | (0.71, 1.35) | (0.67, 1.37) | (0.63, 1.33) | (0.74, 1.58) | (0.86, 1.59) | (0.88, 1.51) | (0.56, 1.16) |
| Use of Micronutrient Supplements during Pregnancy | Maternal Serum Selenium, µmol/L, Median (25, 75) * (n = 114) | Infant Serum Selenium, µmol/L, At Age 6 Months, Median (25, 75) * (n = 91) | |||
|---|---|---|---|---|---|
| Pregnancy 18 Weeks | Pregnancy Week 28 | Pregnancy Week 36 | |||
| Non-user, n = 28 | 0.92 (0.83, 1.00) | 0.83 (0.77, 0.98) | 0.77 (0.73, 0.86) | n = 25 | 0.76 (0.71, 0.87) |
| Regular user, n = 86 | 0.98 (0.89, 1.05) | 0.98 (0.89, 1.04) | 0.87 (0.77, 0.98) | n = 66 | 0.83 (0.76, 0.90) |
| p value ** | 0.06 | 0.02 | 0.008 | 0.05 | |
| Use of Micronutrient Supplements Postpartum | 6 Weeks Postpartum | 4 Months Postpartum | 6 Months Postpartum | Infants 6 Months (n = 91) | |
| Non-user, n = 32 | 1.01 (0.95, 1.14) | 1.04 (0.93, 1.14) | 1.08 (0.92, 1.15) | n = 27 | 0.76 (0.69, 0.84) |
| Regular user, n = 82 | 1.10 (0.97, 1.27) | 1.12 (0.99, 1.28) | 1.12 (1.02, 1.29) | n = 64 | 0.83 (0.75, 0.90) |
| p value ** | 0.06 | 0.04 | 0.01 | 0.03 | |
| Parameters | 6 Weeks n = 59 | 4 Months n = 60 | 6 Months n = 61 | p Value * |
|---|---|---|---|---|
| Breastmilk selenium, µmol/L | ||||
| Median | 0.13 | 0.10 | 0.09 | <0.001 |
| (25, 75) ** | (0.11–0.17) | (0.08–0.13) | (0.08–0.13) | |
| (2.5, 97.5) ** | (0.06–0.27) | (0.04–0.36) | (0.03–0.29) | |
| Daily selenium intake, µmol *** | 0.02 | |||
| Median | 0.10 | 0.08 | 0.09 | |
| (25, 75) ** | (0.08, 0.12) | (0.06, 0.10) | (0.07, 0.12) | |
| (2.5, 97.5) ** | (0.05, 0.20) | (0.03, 0.32) | (0.03, 0.29) |
| Maternal Serum Selenium in Week 18 | ASQ Scores | |||||
|---|---|---|---|---|---|---|
| Total | Communication | Problem Solving | Personal-Social Functioning | Gross Motor Function | Fine Motor Function | |
| <0.90 µmol/L (Tertile 1) n = 35 | 213 (189, 236) | 45 (40, 50) | 50 (36, 59) | 45 (30, 50) | 35 (30, 40) | 40 (35, 50) |
| >0.90 µmol/L (Tertile 2–3) n = 70 | 235 (215, 258) | 50 (45, 55) | 55 (50, 60) | 50 (40, 55) | 35 (30, 45) | 50 (40, 55) |
| p value * | 0.002 | 0.12 | 0.005 | 0.02 | 0.57 | 0.02 |
| Infant Infection from Birth to Age 6 Weeks | Maternal Serum Selenium, µmol/L, Median (25, 75) *, n = 107 | Infant Serum Selenium at 6 Months, µmol/L, Median (25, 75) * n = 91 | |||
|---|---|---|---|---|---|
| Pregnancy Week 18 | Pregnancy Week 28 | Pregnancy Week 36 | 6 Weeks Postpartum | ||
| Yes, n = 19 | 0.99 (0.86, 1.04) | 0.87 (0.80, 0.96) | 0.77 (0.71, 0.86) | 0.98 (0.92, 1.10) | 0.77 (0.74, 0.81) |
| No, n = 88 | 0.96 (0.87, 1.04) | 0.93 (0.81, 1.02) | 0.86 (0.77, 0.96) | 1.09 (0.98, 1.26) | 0.83 (0.74, 0.90) |
| p value ** | 0.94 | 0.52 | 0.03 | 0.03 | 0.10 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varsi, K.; Bolann, B.; Torsvik, I.; Rosvold Eik, T.C.; Høl, P.J.; Bjørke-Monsen, A.-L. Impact of Maternal Selenium Status on Infant Outcome during the First 6 Months of Life. Nutrients 2017, 9, 486. https://doi.org/10.3390/nu9050486
Varsi K, Bolann B, Torsvik I, Rosvold Eik TC, Høl PJ, Bjørke-Monsen A-L. Impact of Maternal Selenium Status on Infant Outcome during the First 6 Months of Life. Nutrients. 2017; 9(5):486. https://doi.org/10.3390/nu9050486
Chicago/Turabian StyleVarsi, Kristin, Bjørn Bolann, Ingrid Torsvik, Tina Constanse Rosvold Eik, Paul Johan Høl, and Anne-Lise Bjørke-Monsen. 2017. "Impact of Maternal Selenium Status on Infant Outcome during the First 6 Months of Life" Nutrients 9, no. 5: 486. https://doi.org/10.3390/nu9050486
APA StyleVarsi, K., Bolann, B., Torsvik, I., Rosvold Eik, T. C., Høl, P. J., & Bjørke-Monsen, A. -L. (2017). Impact of Maternal Selenium Status on Infant Outcome during the First 6 Months of Life. Nutrients, 9(5), 486. https://doi.org/10.3390/nu9050486