Emerging Evidence on Neutrophil Motility Supporting Its Usefulness to Define Vitamin C Intake Requirements



Abstract
:1. Introduction
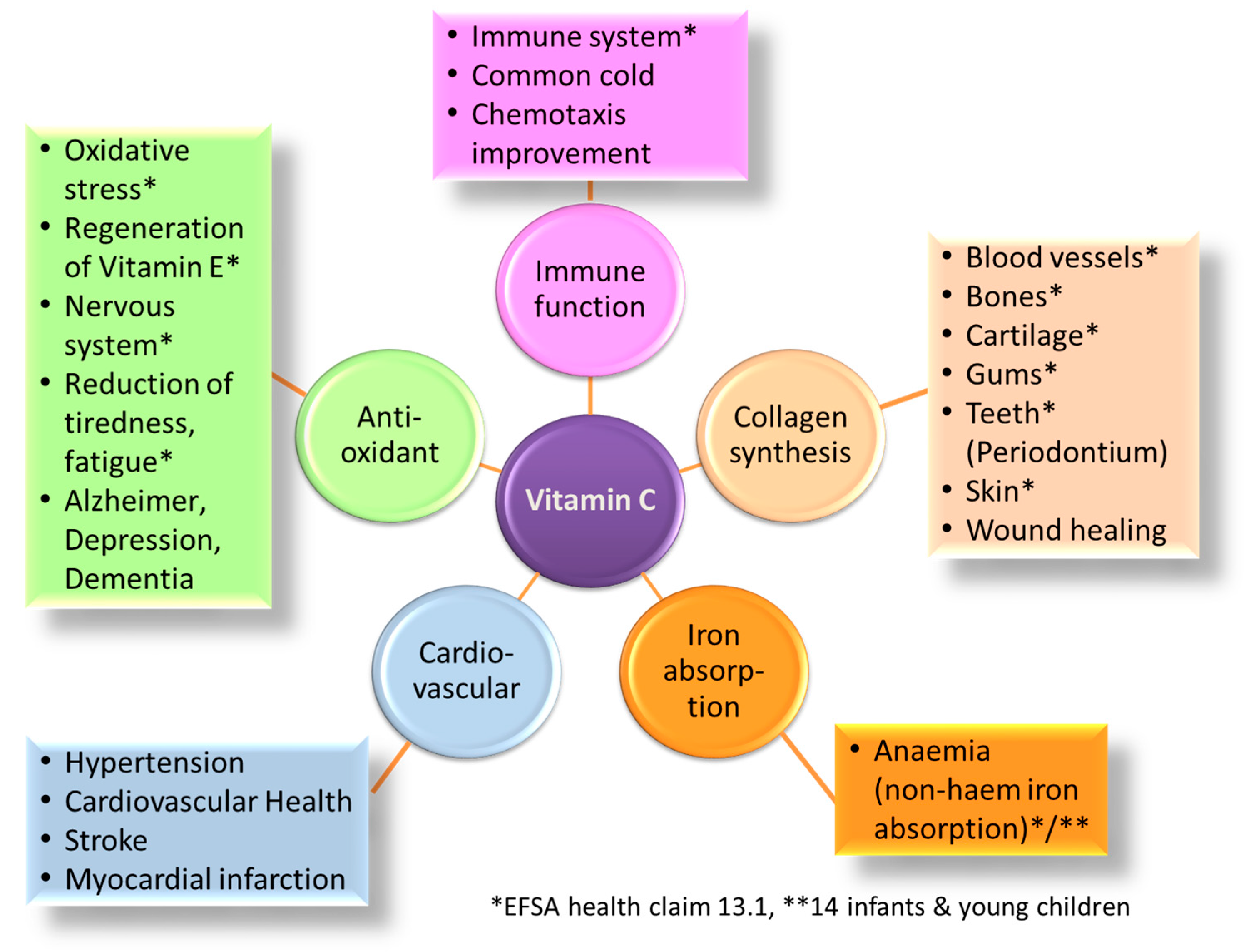
2. Physiologic Functions of Vitamin C in Human Health
3. Approaches Used to Define Vitamin C Requirements
4. New Insights Support Reassessment of Current Vitamin C RDAs
5. The Improvement of Neutrophil Function by Vitamin C in a Broader Human Health Perspective
5.1. Common Cold
5.2. Non-Communicable Diseases
6. Vitamin C Status in the General Population
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Institute of Medicine. Dietary Reference Intakes of Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academic Press: Washington, DC, USA, 2000; ISBN 978-0-309-06935-9. [Google Scholar]
- Schleicher, R.L.; Carroll, M.D.; Ford, E.S.; Lacher, D.A. Serum vitamin C and the prevalence of vitamin C deficiency in the United States: 2003–2004 National health and nutrition examination survey (NHANES). Am. J. Clin. Nutr. 2009, 90, 1252–1263. [Google Scholar] [CrossRef] [PubMed]
- Schwager, J.; Bompard, A.; Weber, P.; Raederstorff, D. Ascorbic acid modulates cell migration in differentiated HL-60 cells and peripheral blood leukocytes. Mol. Nutr. Food Res. 2015, 59, 1513–1523. [Google Scholar] [CrossRef] [PubMed]
- Bozonet, S.M.; Carr, A.C.; Pullar, J.M.; Vissers, M.C. Enhanced human neutrophil vitamin C status, chemotaxis and oxidant generation following dietary supplementation with vitamin C-rich sungold kiwifruit. Nutrients 2015, 7, 2574–2588. [Google Scholar] [CrossRef] [PubMed]
- Padayatty, S.J.; Levine, M. Vitamin c: The known, the unknown, and goldilocks. Oral Dis. 2016, 22, 463–493. [Google Scholar] [CrossRef] [PubMed]
- Linster, C.L.; Van Schaftingen, E. Vitamin c. Biosynthesis, recycling and degradation in mammals. FEBS J. 2007, 274, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Buettner, G.R.; Jurkiewicz, B.A. Catalytic metals, ascorbate and free radicals: Combinations to avoid. Radiat. Res. 1996, 145, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.; Mazur, M.; Telser, J. Free radicals and antioxidants in normal physiological functions and human disease. Int. J. Biochem. Cell Biol. 2007, 39, 44–84. [Google Scholar] [CrossRef] [PubMed]
- Swindells, K.; Rhodes, L.E. Influence of oral antioxidants on ultraviolet radiation-induced skin damage in humans. Photodermatol. Photoimmunol. Photomed. 2004, 20, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Eberlein-Konig, B.; Placzek, M.; Przybilla, B. Protective effect against sunburn of combined systemic ascorbic acid (vitamin C) and d-alpha-tocopherol (vitamin E). J. Am. Acad. Dermatol. 1998, 38, 45–48. [Google Scholar] [CrossRef]
- Buettner, G.R. The pecking order of free radicals and antioxidants: Lipid peroxidation, alpha-tocopherol, and ascorbate. Arch. Biochem. Biophys. 1993, 300, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.K.; Buettner, G.R. Interaction of vitamin C and vitamin E during free radical stress in plasma: An esr study. Free Radic. Biol. Med. 1993, 14, 649–653. [Google Scholar] [CrossRef]
- Benzie, I.; Strain, J.J. Effect of vitamin C supplementation on concentrations of vitamins C and E in fasting plasma. Asia Pac. J. Clin. Nutr. 1999, 8, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Forth, W.; Rummel, W. Iron absorption. Physiol. Rev. 1973, 53, 724–792. [Google Scholar] [PubMed]
- Lynch, S.R.; Cook, J.D. Interaction of vitamin C and iron. Ann. N. Y. Acad. Sci. 1980, 355, 32–44. [Google Scholar] [CrossRef] [PubMed]
- Scheers, N.; Andlid, T.; Alminger, M.; Sandberg, A.S. Determination of Fe2+ and Fe3+ in aqueous solutions containing food chelators by differential pulse anodic stripping voltammetry. Electroanalysis 2010, 22, 1090–1096. [Google Scholar] [CrossRef]
- Fritz, I.B. Carnitine and its role in fatty acid metabolism. Adv. Lipid Res. 1963, 1, 285–334. [Google Scholar] [PubMed]
- Fritz, I.B.; Yue, K.T. Long-chain carnitine acyltransferase and the role of acylcarnitine derivatives in the catalytic increase of fatty acid oxidation induced by carnitine. J. Lipid Res. 1963, 4, 279–288. [Google Scholar] [PubMed]
- Ramsay, R.R.; Gandour, R.D.; van der Leij, F.R. Molecular enzymology of carnitine transfer and transport. Biochim. Biophys. Acta 2001, 1546, 21–43. [Google Scholar] [CrossRef]
- Furusawa, H.; Sato, Y.; Tanaka, Y.; Inai, Y.; Amano, A.; Iwama, M.; Kondo, Y.; Handa, S.; Murata, A.; Nishikimi, M.; et al. Vitamin C is not essential for carnitine biosynthesis in vivo: Verification in vitamin C-depleted senescence marker protein-30/gluconolactonase knockout mice. Biol. Pharm. Bull. 2008, 31, 1673–1679. [Google Scholar] [CrossRef] [PubMed]
- Rush, R.A.; Geffen, L.B. Dopamine beta-hydroxylase in health and disease. Crit. Rev. Clin. Lab. Sci. 1980, 12, 241–277. [Google Scholar] [CrossRef] [PubMed]
- Prigge, S.T.; Kolhekar, A.S.; Eipper, B.A.; Mains, R.E.; Amzel, L.M. Substrate-mediated electron transfer in peptidylglycine alpha-hydroxylating monooxygenase. Nat. Struct. Biol. 1999, 6, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Dengler, V.L.; Galbraith, M.D.; Espinosa, J.M. Transcriptional regulation by hypoxia inducible factors. Crit. Rev. Biochem. Mol. Biol. 2014, 49, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Lindblad, B.; Lindstedt, G.; Lindstedt, S. The mechanism of enzymic formation of homogentisate from p-hydroxyphenylpyruvate. J. Am. Chem. Soc. 1970, 92, 7446–7449. [Google Scholar] [CrossRef] [PubMed]
- Kukkola, L.; Hieta, R.; Kivirikko, K.I.; Myllyharju, J. Identification and characterization of a third human, rat, and mouse collagen prolyl 4-hydroxylase isoenzyme. J. Biol. Chem. 2003, 278, 47685–47693. [Google Scholar] [CrossRef] [PubMed]
- Prockop, D.J.; Kivirikko, K.I. Collagens: Molecular biology, diseases, and potentials for therapy. Annu. Rev. Biochem. 1995, 64, 403–434. [Google Scholar] [CrossRef] [PubMed]
- Aghajanian, P.; Hall, S.; Wongworawat, M.D.; Mohan, S. The roles and mechanisms of actions of vitamin C in bone: New developments. J. Bone Miner. Res. 2015, 30, 1945–1955. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Li, M.; Hara, K.; Sasaki, M.; Tabata, C.; de Freitas, P.H.; Hongo, H.; Suzuki, R.; Kobayashi, M.; Inoue, K.; et al. Morphological assessment of bone mineralization in tibial metaphyses of ascorbic acid-deficient ods rats. Biomed. Res. 2011, 32, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Masse, P.G.; Jougleux, J.L.; Tranchant, C.C.; Dosy, J.; Caissie, M.; Coburn, S.P. Enhancement of calcium/vitamin D supplement efficacy by administering concomitantly three key nutrients essential to bone collagen matrix for the treatment of osteopenia in middle-aged women: A one-year follow-up. J. Clin. Biochem. Nutr. 2010, 46, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Blass, S.C.; Goost, H.; Tolba, R.H.; Stoffel-Wagner, B.; Kabir, K.; Burger, C.; Stehle, P.; Ellinger, S. Time to wound closure in trauma patients with disorders in wound healing is shortened by supplements containing antioxidant micronutrients and glutamine: A prct. Clin. Nutr. 2012, 31, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.; Fuhrman, M.P. Nutrients and wound healing: Still searching for the magic bullet. Nutr. Clin. Pract. 2005, 20, 331–347. [Google Scholar] [CrossRef] [PubMed]
- Stechmiller, J.K. Understanding the role of nutrition and wound healing. Nutr. Clin. Pract. 2010, 25, 61–68. [Google Scholar] [CrossRef] [PubMed]
- McRae, M.P. Vitamin C supplementation lowers serum low-density lipoprotein cholesterol and triglycerides: A meta-analysis of 13 randomized controlled trials. J. Chiropr. Med. 2008, 7, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Hallfrisch, J.; Singh, V.N.; Muller, D.C.; Baldwin, H.; Bannon, M.E.; Andres, R. High plasma vitamin C associated with high plasma HDL- and HDL2 cholesterol. Am. J. Clin. Nutr. 1994, 60, 100–105. [Google Scholar] [PubMed]
- Ashor, A.W.; Siervo, M.; van der Velde, F.; Willis, N.D.; Mathers, J.C. Systematic review and meta-analysis of randomised controlled trials testing the effects of vitamin C supplementation on blood lipids. Clin. Nutr. 2016, 35, 626–637. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.A.; Hudes, E.S.; Browner, W.S. Serum ascorbic acid and cardiovascular disease prevalence in US. Adults. Epidemiology. 1998, 9, 316–321. [Google Scholar] [CrossRef] [PubMed]
- May, J.M.; Harrison, F.E. Role of vitamin C in the function of the vascular endothelium. Antioxid. Redox Signal. 2013, 19, 2068–2083. [Google Scholar] [CrossRef] [PubMed]
- Ashor, A.W.; Lara, J.; Mathers, J.C.; Siervo, M. Effect of vitamin C on endothelial function in health and disease: A systematic review and meta-analysis of randomised controlled trials. Atherosclerosis 2014, 235, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Ashor, A.W.; Siervo, M.; Lara, J.; Oggioni, C.; Afshar, S.; Mathers, J.C. Effect of vitamin C and vitamin E supplementation on endothelial function: A systematic review and meta-analysis of randomised controlled trials. Br. J. Nutr. 2015, 113, 1182–1194. [Google Scholar] [CrossRef] [PubMed]
- Juraschek, S.P.; Guallar, E.; Appel, L.J.; Miller, E.R., 3rd. Effects of vitamin C supplementation on blood pressure: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2012, 95, 1079–1088. [Google Scholar] [CrossRef] [PubMed]
- Wintergerst, E.S.; Maggini, S.; Hornig, D.H. Immune-enhancing role of vitamin C and zinc and effect on clinical conditions. Ann. Nutr. Metab. 2006, 50, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Pike, J.; Chandra, R.K. Effect of vitamin and trace element supplementation on immune indices in healthy elderly. Int. J. Vitam. Nutr. Res. 1995, 65, 117–121. [Google Scholar] [PubMed]
- Manning, J.; Mitchell, B.; Appadurai, D.A.; Shakya, A.; Pierce, L.J.; Wang, H.; Nganga, V.; Swanson, P.C.; May, J.M.; Tantin, D.; et al. Vitamin C promotes maturation of t-cells. Antioxid. Redox Signal. 2013, 19, 2054–2067. [Google Scholar] [CrossRef] [PubMed]
- Washko, P.; Rotrosen, D.; Levine, M. Ascorbic acid transport and accumulation in human neutrophils. J. Biol. Chem. 1989, 264, 18996–19002. [Google Scholar] [PubMed]
- Levine, M.; Conry-Cantilena, C.; Wang, Y.; Welch, R.W.; Washko, P.W.; Dhariwal, K.R.; Park, J.B.; Lazarev, A.; Graumlich, J.F.; King, J.; et al. Vitamin C pharmacokinetics in healthy volunteers: Evidence for a recommended dietary allowance. Proc. Natl. Acad. Sci. USA 1996, 93, 3704–3709. [Google Scholar] [CrossRef] [PubMed]
- Vohra, K.; Khan, A.J.; Telang, V.; Rosenfeld, W.; Evans, H.E. Improvement of neutrophil migration by systemic vitamin c in neonates. J. Perinatol. 1990, 10, 134–136. [Google Scholar] [PubMed]
- Boxer, L.A.; Vanderbilt, B.; Bonsib, S.; Jersild, R.; Yang, H.H.; Baehner, R.L. Enhancement of chemotactic response and microtubule assembly in human leukocytes by ascorbic acid. J. Cell. Physiol. 1979, 100, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Frei, B. Toward a new recommended dietary allowance for vitamin C based on antioxidant and health effects in humans. Am. J. Clin. Nutr. 1999, 69, 1086–1107. [Google Scholar] [PubMed]
- Hume, R.; Weyers, E. Changes in leucocyte ascorbic acid during the common cold. Scott. Med. J. 1973, 18, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Lykkesfeldt, J.; Loft, S.; Nielsen, J.B.; Poulsen, H.E. Ascorbic acid and dehydroascorbic acid as biomarkers of oxidative stress caused by smoking. Am. J. Clin. Nutr. 1997, 65, 959–963. [Google Scholar] [PubMed]
- The Nutrition Information Centre of the University of Stellenbosch. Available online: http://www.sun.ac.za/english/faculty/healthsciences/nicus/Pages/Vitamin-C.aspx (accessed on 5 October 2016).
- Department of Health. Dietary Reference Values for Food, Energy and Nutrients for the United Kingdom in Report on Health and Social Subjects; Department of Health: London, UK, 1991.
- Food and Agriculture Organization; World Health Organization. Human Vitamin and Mineral Requirements; Training Materials for Agricultural Planning; Food and Agriculture Organization: Bangkok, Thailand, 2002. [Google Scholar]
- Australian National Health and Medical Research Council; New Zealand Ministry of Health. Nutrient Reference Values for Australia and New Zealand. Available online: https://www.nrv.gov.au/nutrients/vitamin-c (accessed on 16 November 2016).
- Barba, C.V.; Cabrera, M.I. Recommended energy and nutrient intakes for Filipinos 2002. Asia Pac. J. Clin. Nutr. 2008, 17 (Suppl. 2), 399–404. [Google Scholar] [CrossRef] [PubMed]
- German Nutrition Society. New reference values for vitamin C intake. Ann. Nutr. Metab. 2015, 67, 13–20. [Google Scholar] [CrossRef]
- Health Promotion Board. Recommended Dietary Allowances. Available online: http://www.hpb.gov.sg/HOPPortal/health-article/2652 (accessed on 23 October 2016).
- National Institute of Health and Nutrition. Dietary Reference Intakes for Japanese (2015). Available online: http://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/overview.pdf (accessed on 1 November 2016).
- Deutsche Gesellschaft für Ernährung; Österreichische Gesellschaft für Ernährung; Schweizerische Gesellschaft für Ernährung; Schweizerische Vereinigung für Ernährung. Referenzwerte für die Nährstoffzufuhr; Umschau Verlag: Frankfurt, Germany, 2008. [Google Scholar]
- Levine, M.; Dhariwal, K.R.; Washko, P.W.; Welch, R.W.; Wang, Y. Cellular functions of ascorbic acid: A means to determine vitamin c requirements. Asia Pac. J. Clin. Nutr. 1993, 2 (Suppl. 1), 5–13. [Google Scholar] [PubMed]
- Levine, M.; Dhariwal, K.R.; Welch, R.W.; Wang, Y.; Park, J.B. Determination of optimal vitamin C requirements in humans. Am. J. Clin. Nutr. 1995, 62 (Suppl. 6), 1347S–1356S. [Google Scholar] [PubMed]
- EFSA NDA Panel. Scientific opinion on dietary reference values for Vitamin C. EFSA J. 2013. [Google Scholar] [CrossRef]
- Benzie, I.F. Vitamin C: Prospective functional markers for defining optimal nutritional status. Proc. Nutr. Soc. 1999, 58, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Ginter, E. Ascorbic acid in cholesterol metabolism and in detoxification of xenobiotic substances: Problem of optimum vitamin C intake. Nutrition 1989, 5, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Bates, C.J. Proline and hydroxyproline excretion and vitamin C status in elderly human subjects. Clin. Sci. Mol. Med. 1977, 52, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Hevia, P.; Omaye, S.T.; Jacob, R.A. Urinary hydroxyproline excretion and vitamin C status in healthy young men. Am. J. Clin. Nutr. 1990, 51, 644–648. [Google Scholar] [PubMed]
- Rodrigo, R.; Prat, H.; Passalacqua, W.; Araya, J.; Bachler, J.P. Decrease in oxidative stress through supplementation of vitamins C and E is associated with a reduction in blood pressure in patients with essential hypertension. Clin. Sci. (Lond.) 2008, 114, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Bendich, A.; Langseth, L. The health effects of vitamin c supplementation: A review. J. Am. Coll. Nutr. 1995, 14, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Weber, P.; Bendich, A.; Schalch, W. Vitamin C and human health—A review of recent data relevant to human requirements. Int. J. Vitam. Nutr. Res. 1996, 66, 19–30. [Google Scholar] [PubMed]
- Petrie, R.J.; Doyle, A.D.; Yamada, K.M. Random versus directionally persistent cell migration. Nat. Rev. Mol. Cell Biol. 2009, 10, 538–549. [Google Scholar] [CrossRef] [PubMed]
- Amulic, B.; Cazalet, C.; Hayes, G.L.; Metzler, K.D.; Zychlinsky, A. Neutrophil function: From mechanisms to disease. Annu. Rev. Immunol. 2012, 30, 459–489. [Google Scholar] [CrossRef] [PubMed]
- Foxman, E.F.; Campbell, J.J.; Butcher, E.C. Multistep navigation and the combinatorial control of leukocyte chemotaxis. J. Cell Biol. 1997, 139, 1349–1360. [Google Scholar] [CrossRef] [PubMed]
- Johnston, C.S.; Huang, S. Effect of ascorbic acid nutriture on blood histamine and neutrophil chemotaxis in guinea pigs. J. Nutr. 1991, 121, 126–130. [Google Scholar] [PubMed]
- Lykkesfeldt, J.; Poulsen, H.E. Is vitamin c supplementation beneficial? Lessons learned from randomised controlled trials. Br. J. Nutr. 2010, 103, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Bozonet, S.M.; Pullar, J.M.; Simcock, J.W.; Vissers, M.C. Human skeletal muscle ascorbate is highly responsive to changes in vitamin c intake and plasma concentrations. Am. J. Clin. Nutr. 2013, 97, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Pullar, J.M.; Moran, S.; Vissers, M.C.M. Bioavailability of vitamin C from kiwifruit in non-smoking males: Determination of ‘healthy’ and ‘optimal’ intakes. J. Nutr. Sci. 2012, 1, e14. [Google Scholar] [CrossRef] [PubMed]
- Savini, I.; Rossi, A.; Pierro, C.; Avigliano, L.; Catani, M.V. Svct1 and Svct2: Key proteins for vitamin C uptake. Amino Acid 2008, 34, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Scientific Committee on Food; Scientific Panel on Dietetic Products, Nutrition and Allergies. Tolerable Upper Intake Levels for Vitamins and Minerals; European Food Safety Authority: Parma, Italy, 2006; ISBN 92-9199-014-0. [Google Scholar]
- Levine, M.; Wang, Y.; Padayatty, S.J.; Morrow, J. A new recommended dietary allowance of vitamin C for healthy young women. Proc. Natl. Acad. Sci. USA 2001, 98, 9842–9846. [Google Scholar] [CrossRef] [PubMed]
- Mehmood, Z.-T.-N.H.; Papandreou, D. An updated mini review of vitamin D and obesity: Adipogenesis and inflammation state. Open Access Maced. J. Med. Sci. 2016, 4, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Khatami, M. Inflammation, aging, and cancer: Tumoricidal versus tumorigenesis of immunity. Cell Biochem. Biophys. 2009, 55, 55–79. [Google Scholar] [CrossRef] [PubMed]
- Hemila, H.; Chalker, E. Vitamin C for preventing and treating the common cold. Cochrane Database Syst. Rev. 2013, 1. [Google Scholar] [CrossRef]
- Moser, U. Vitamins—Wrong approaches. Int. J. Vitam. Nutr. Res. 2012, 82, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.; Vodicka, T.A.; Blair, P.S.; Buckley, D.I.; Heneghan, C.; Hay, A.D.; Team, T.P. Duration of symptoms of respiratory tract infections in children: Systematic review. BMJ 2013, 347, f7027. [Google Scholar] [CrossRef] [PubMed]
- Frei, B. Authors perspective—What is the optimum intake of Vitamin C. Crit. Rev. Food. Sci. Nutr. 2012, 52, 815–829. [Google Scholar] [CrossRef] [PubMed]
- Moser, M.A.; Chun, O.K. Vitamin C and heart health: A review based on findings from epidemiologic studies. Int. J. Mol. Sci. 2016, 17. [Google Scholar] [CrossRef] [PubMed]
- Ross, R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Nyyssonen, K.; Parviainen, M.T.; Salonen, R.; Tuomilehto, J.; Salonen, J.T. Vitamin C deficiency and risk of myocardial infarction: Prospective population study of men from eastern Finland. BMJ 1997, 314, 634–638. [Google Scholar] [CrossRef] [PubMed]
- Khaw, K.T.; Bingham, S.; Welch, A.; Luben, R.; Wareham, N.; Oakes, S.; Day, N. Relation between plasma ascorbic acid and mortality in men and women in epic-norfolk prospective study: A prospective population study. European prospective investigation into cancer and nutrition. Lancet 2001, 357, 657–663. [Google Scholar] [CrossRef]
- Singh, R.B.; Ghosh, S.; Niaz, M.A.; Singh, R.; Beegum, R.; Chibo, H.; Shoumin, Z.; Postiglione, A. Dietary intake, plasma levels of antioxidant vitamins, and oxidative stress in relation to coronary artery disease in elderly subjects. Am. J. Cardiol. 1995, 76, 1233–1238. [Google Scholar] [CrossRef]
- Eichholzer, M.; Stahelin, H.B.; Gey, K.F. Inverse correlation between essential antioxidants in plasma and subsequent risk to develop cancer, ischemic heart disease and stroke respectively: 12-Year follow-up of the prospective Basel study. EXS 1992, 62, 398–410. [Google Scholar] [CrossRef] [PubMed]
- Sahyoun, N.R.; Jacques, P.F.; Russell, R.M. Carotenoids, vitamins C and E, and mortality in an elderly population. Am. J. Epidemiol. 1996, 144, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Langlois, M.; Duprez, D.; Delanghe, J.; De Buyzere, M.; Clement, D.L. Serum vitamin C concentration is low in peripheral arterial disease and is associated with inflammation and severity of atherosclerosis. Circulation 2001, 103, 1863–1868. [Google Scholar] [CrossRef] [PubMed]
- Lachance, P.; Langseth, L. The rda concept: Time for a change? Nutr. Rev. 1994, 52, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Harrison, F.E. A critical review of vitamin C for the prevention of age-related cognitive decline and Alzheimer’s disease. J. Alzheimer's Dis. 2012, 29, 711–726. [Google Scholar] [CrossRef]
- De Bruijn, R.F.A.G.; Ikram, M.A. Cardiovascular risk factors and future risk of alzheimer’s disease. BMC Med. 2014, 12, 130. [Google Scholar] [CrossRef] [PubMed]
- Tramutola, A.; Lanzillotta, C.; Perluigi, M.; Butterfield, D.A. Oxidative stress, protein modification and alzheimer disease. Brain Res. Bull. 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases; Report of a Joint WHO/FAO Consultation; World Health Organization: Geneva, Switzerland, 2003; ISBN 92 4 120916 X. [Google Scholar]
- Birlouez-Aragon, I.; Saavedra, G.; Tessier, F.J.; Galinier, A.; Ait-Ameur, L.; Lacoste, F.; Niamba, C.-N.; Alt, N.; Somoza, V.; Lecerf, J.-M. A diet based on high-heat-treated foods promotes risk factors for diabetes mellitus and cardiovascular diseases. Am. J. Clin. Nutr. 2010, 91, 1220–1226. [Google Scholar] [CrossRef]
- Max Rubner-Institut. Nationale Verzehrsstudie II. Ergebnisbericht, Teil 2. Available online: http://www.was-esse-ich.de/uploads/media/NVSII_Abschlussbericht_Teil_2.pdf (accessed on 2 July 2011).
- Manios, Y.; Moschonis, G.; Grammatikaki, E.; Mavrogianni, C.; van den Heuvel, E.G.H.M.; Bos, R.; Singh-Povel, C. Food group and micronutrient intake adequacy among children, adults and elderly women in greece. Nutrients 2015, 7, 1841–1858. [Google Scholar] [CrossRef] [PubMed]
- Schupbach, R.; Wegmuller, R.; Berguerand, C.; Bui, M.; Herter-Aeberli, I. Micronutrient status and intake in omnivores, vegetarians and vegans in Switzerland. Eur. J. Nutr. 2017, 56, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Clarys, P.; Deliens, T.; Huybrechts, I.; Deriemaeker, P.; Vanaelst, B.; De Keyzer, W.; Hebbelinck, M.; Mullie, P. Comparison of nutritional quality of the vegan, vegetarian, semi-vegetarian, pesco-vegetarian and omnivorous diet. Nutrients 2014, 6, 1318–1332. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Guenther, P.M.; Subar, A.F.; Kirkpatrick, S.I.; Dodd, K.W. Americans do not meet federal dietary recommendations. J. Nutr. 2010, 140, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.M.; Barraj, L.M.; Spungen, J.H.; Herman, D.R.; Randolph, R.K. Global assessment of select phytonutrient intakes by level of fruit and vegetable consumption. Br. J. Nutr. 2014, 112, 1004–1018. [Google Scholar] [CrossRef] [PubMed]
- Bundesamt für Lebensmittelsicherheit und Veterinärwesen. Zu viel Gewicht, zu Wenig Früchte und Gemüse. Available online: https://www.blv.admin.ch/blv/de/home/dokumentation/nsb-news-list.msg-id-64373.html (accessed on 11 November 2016).
- Hall, J.N.; Moore, S.; Harper, S.B.; Lynch, J.W. Global variability in fruit and vegetable consumption. Am. J. Prev. Med. 2009, 36, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Dubuisson, C.; Lioret, S.; Touvier, M.; Dufour, A.; Calamassi-Tran, G.; Volatier, J.-L.; Lafay, L. Trends in food and nutritional intakes of french adults from 1999 to 2007: Results from the inca surveys. Br. J. Nutr. 2010, 103, 1035–1048. [Google Scholar] [CrossRef] [PubMed]
- US Department of Agriculture; Agricultural Research Service; Nutrient Data Laboratory. USDA National Nutrient Database for Standard Reference, Release 28; Version Current; September 2015. Available online: http://www.ars.usda.gov/nea/bhnrc/ndl (accessed on 4 April 2016).
- Elmadfa, I.; Meyer, A.; Nowak, V.; Hasenegger, V.; Putz, P.; Verstraeten, R.; Remaut-DeWinter, A.M.; Kolsteren, P.; Dostalova, J.; Dlouhy, P.; et al. European Nutrition and Health Report 2009, 2010/02/06 ed.; Karger: Basel, Switzerland, 2009; Volume 62. [Google Scholar] [CrossRef]
- Deutsche Gesellschaft für Ernährung e. V. 12. Ernährungsbericht 2012; Deutsche Gesellschaft für Ernährung e. V.: Bonn, Germany, 2012. [Google Scholar]
- Deutsche Gesellschaft für Ernährung e. V. Ernährungsbericht 2008; Deutsche Gesellschaft für Ernährung e. V.: Bonn, Germany, 2008. [Google Scholar]
- Roman Vinas, B.; Ribas Barba, L.; Ngo, J.; Gurinovic, M.; Novakovic, R.; Cavelaars, A.; de Groot, L.C.; Van‘t Veer, P.; Matthys, C.; Serra Majem, L. Projected prevalence of inadequate nutrient intakes in Europe. Ann. Nutr. Metab. 2011, 59, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Troesch, B.; Hoeft, B.; McBurney, M.; Eggersdorfer, M.; Weber, P. Dietary surveys indicate vitamin intakes below recommendations are common in representative western countries. Br. J. Nutr. 2012, 108, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Labour and Welfare. The Japan National Health and Nutrition Survey 2008; Ministry of Health Labour and Welfare: Tokyo, Japan, 2008.
- Kim, J.; Choi, Y.-H. Physical activity, dietary vitamin C, and metabolic syndrome in the Korean adults: The Korea national health and nutrition examination survey 2008 to 2012. Public Health 2016, 135, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Fulgoni, V.L.; Keast, D.R.; Dwyer, J.T. Dietary supplement use is associated with higher intakes of minerals from food sources. Am. J. Clin. Nutr. 2011, 94, 1376–1381. [Google Scholar] [CrossRef] [PubMed]
- Fulgoni, V.L.; Keast, D.R.; Bailey, R.L.; Dwyer, J. Foods, fortificants, and supplements: Where do Americans get their nutrients? J. Nutr. 2011, 141, 1847–1854. [Google Scholar] [CrossRef] [PubMed]
- Skeie, G.; Braaten, T.; Hjartåker, A.; Lentjes, M.; Amiano, P.; Jakszyn, P.; Pala, V.; Palanca, A.; Niekerk, E.M.; Verhagen, H.; et al. Use of dietary supplements in the European prospective investigation into cancer and nutrition calibration study. Eur. J. Clin. Nutr. 2009, 63, S226–S238. [Google Scholar] [CrossRef] [PubMed]
- Nagy, S. Vitamin C contents of citrus fruit and their products: A review. J. Agric. Food Chem. 1980, 28, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Vanderslice, J.T.; Higgs, D.J. Vitamin C content of foods: Sample variability. Am. J. Clin. Nutr. 1991, 54, 1323S–1327S. [Google Scholar] [PubMed]
- Marti, N.; Mena, P.; Canovas, J.A.; Micol, V.; Saura, D. Vitamin C and the role of citrus juices as functional food. Nat. Prod. Commun. 2009, 4, 677–700. [Google Scholar] [PubMed]
- Cahill, L.; Corey, P.N.; El-Sohemy, A. Vitamin C deficiency in a population of young Canadian adults. Am. J. Epidemiol. 2009, 170, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Hampl, J.S.; Taylor, C.A.; Johnston, C.S. Vitamin C deficiency and depletion in the United States: The third national health and nutrition examination survey, 1988 to 1994. Am. J. Public Health 2004, 94, 870–875. [Google Scholar] [CrossRef] [PubMed]
- Coleman-Jensen, A.; Nord, M.; Singh, A. Household Food Security in the United States in 2012; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2013.
- World Health Organization. Fact Sheet No. 311: Obesity and Overweight. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 2 May 2014).
- EFSA NDA Panel. Scientific opinion on the substantiation of health claims related to vitamin C and protection of DNA, proteins and lipids from oxidative damage (ID 129, 138, 143, 148), antioxidant function of lutein (ID 146), maintenance of vision (ID 141, 142), collagen formation (ID 130, 131, 136, 137, 149), function of the nervous system (ID 133), function of the immune system (ID 134), function of the immune system during and after extreme physical exercise (ID 144), non-haem iron absorption (ID 132, 147), energy-yielding metabolism (ID 135), and relief in case of irritation in the upper respiratory tract (ID 1714, 1715) pursuant to article 13(1) of regulation (EC) No. 1924/2006. EFSA J. 2009, 7, 1226. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Country | Men (mg) | Women (mg) |
|---|---|---|
| Germany, Austria, and Switzerland [56,59] | 110 | 95 |
| United States [1] | 90 | 75 |
| United Kingdom [52] | 40 | 40 |
| Australia and New Zealand [54] | 45 | 45 |
| Japan [58] | 100 | 100 |
| Philippines [55] | 75 | 70 |
| Singapore [57] | 105 | 85 |
| South Africa [51] | 90 | 90 |
| FAO/WHO [53] | 45 | 45 |
| Food | Content per 100 g (mg) | Unit | Content per Unit (mg) |
|---|---|---|---|
| Vegetables | |||
| Red pepper | 128 | 1 piece (119 g) | 152 |
| Green pepper | 80 | 1 piece (119 g) | 96 |
| Broccoli | 89 | 1 cup 1 (91 g) | 81 |
| Brussels sprouts | 85 | 1 cup 1 (88 g) | 75 |
| Cabbage | 37 | 1 cup 1 (89 g) | 33 |
| Cauliflower | 48 | 1 cup 1 (107 g) | 52 |
| Tomato | 14 | 1 piece (123 g) | 17 |
| Green peas | 40 | 1 cup 1 (145 g) | 58 |
| Fruits | |||
| Orange | 53 | 1 piece (96 g) | 70 |
| Kiwi | 93 | 1 piece (69 g) | 64 |
| Mango | 36 | 1 piece 2 (336 g) | 122 |
| Strawberry | 59 | 1 cup 1 (144 g) | 85 |
| Cantaloupe melon | 37 | 1 wedge (69 g) | 25 |
| Grapefruit | 33 | 1 piece (118 g) | 39 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elste, V.; Troesch, B.; Eggersdorfer, M.; Weber, P. Emerging Evidence on Neutrophil Motility Supporting Its Usefulness to Define Vitamin C Intake Requirements. Nutrients 2017, 9, 503. https://doi.org/10.3390/nu9050503
Elste V, Troesch B, Eggersdorfer M, Weber P. Emerging Evidence on Neutrophil Motility Supporting Its Usefulness to Define Vitamin C Intake Requirements. Nutrients. 2017; 9(5):503. https://doi.org/10.3390/nu9050503
Chicago/Turabian StyleElste, Volker, Barbara Troesch, Manfred Eggersdorfer, and Peter Weber. 2017. "Emerging Evidence on Neutrophil Motility Supporting Its Usefulness to Define Vitamin C Intake Requirements" Nutrients 9, no. 5: 503. https://doi.org/10.3390/nu9050503
APA StyleElste, V., Troesch, B., Eggersdorfer, M., & Weber, P. (2017). Emerging Evidence on Neutrophil Motility Supporting Its Usefulness to Define Vitamin C Intake Requirements. Nutrients, 9(5), 503. https://doi.org/10.3390/nu9050503