Long-term Effects of Snake Envenoming



{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Long-term Sequalae of Local Effects
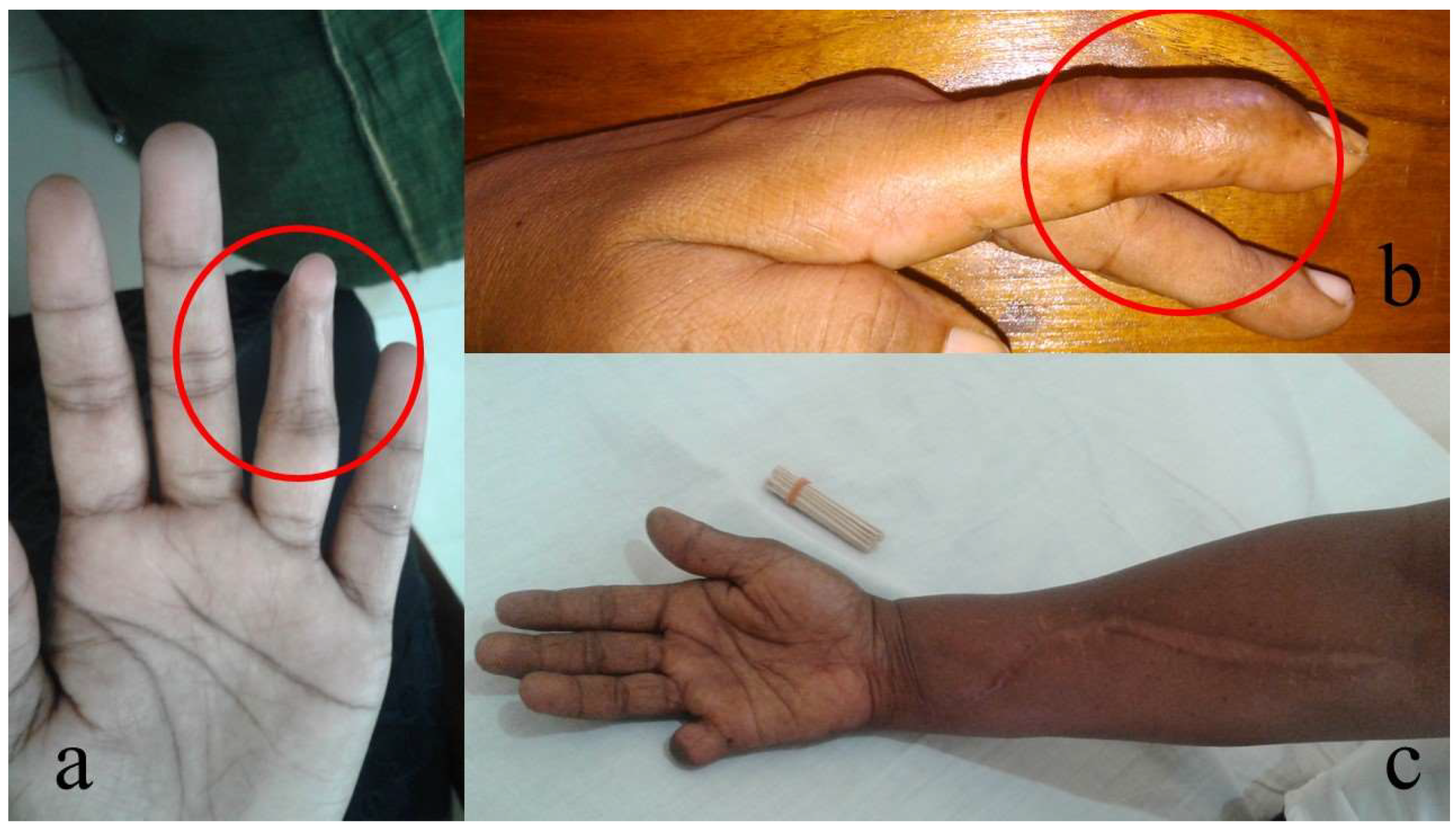
2.1. Local Necrosis Resulting in Amputation
2.2. Chronic Ulcers
2.3. Chronic Local Pain and Swelling
2.4. Blindness due to Primary Venom Effects
3. Chronic Kidney Disease
4. Neurological Effects
4.1. Neuromuscular Paralysis
4.2. Neurological Effects Secondary to Hypoxic or Ischemic Events
4.3. Blindness
4.4. Neurological Effects following Intracranial Haemorrhage
4.5. Reduced Parasympathetic Activity
4.6. Anosmia and Changes in Taste Sensation
5. Endocrine Effects—Hypopituitarism
6. Psychological Effects
7. Knowledge Gaps
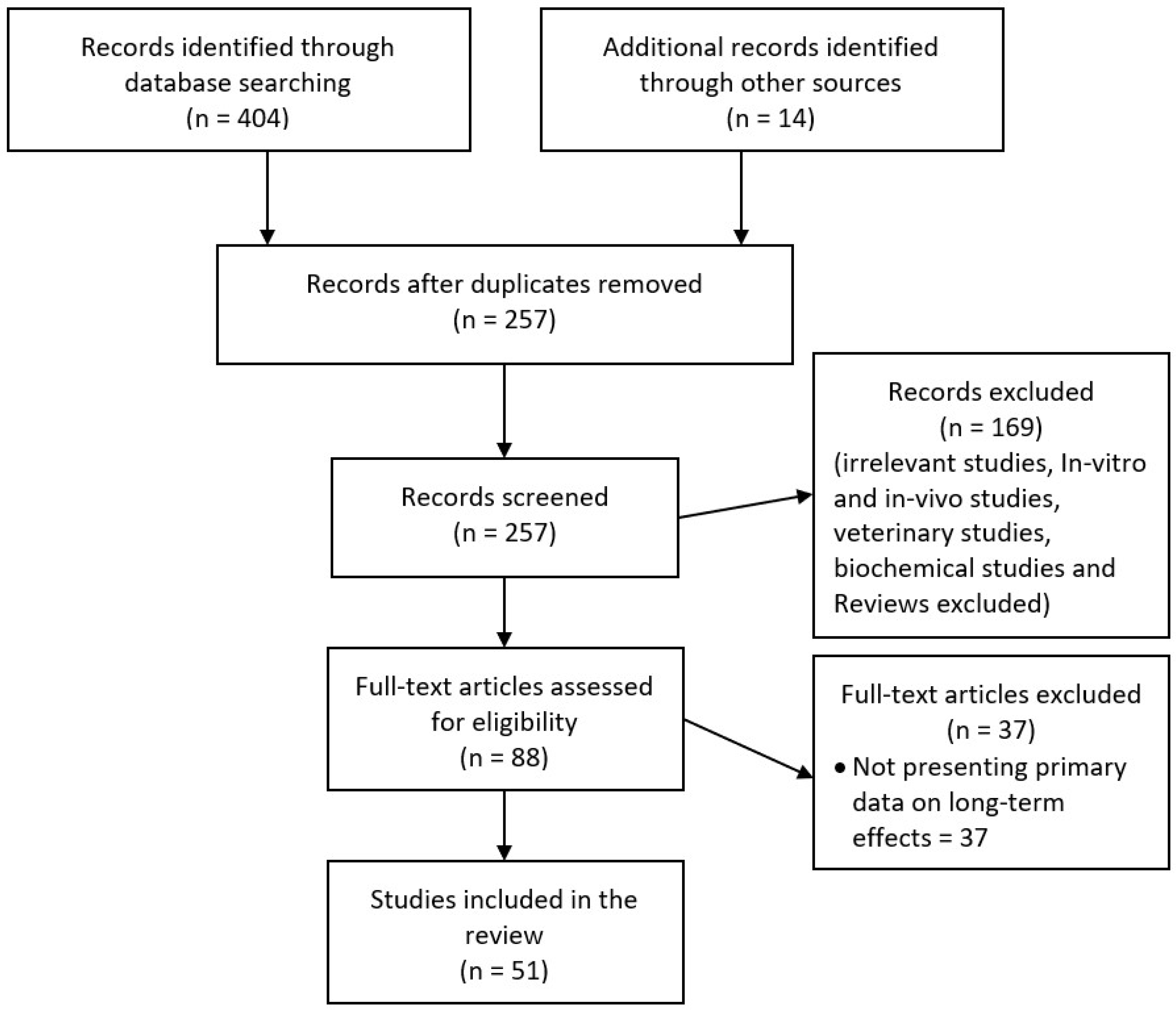
8. Methods
Author Contributions
Funding
Conflicts of Interest
References
- Harrison, R.A.; Hargreaves, A.; Wagstaff, S.C.; Faragher, B.; Lalloo, D.G. Snake envenoming: a disease of poverty. PLoS Negl. Trop. Dis. 2009, 3, e569. [Google Scholar] [CrossRef]
- Kasturiratne, A.; Wickremasinghe, A.R.; De Silva, N.; Gunawardena, N.K. The Global Burden of Snakebite: A Literature Analysis and Modelling Based on Regional Estimates of Envenoming and Deaths. PLoS Med. 2008, 5, e218. [Google Scholar] [CrossRef]
- Isbister, G.K. Snakebite doesn’t cause disseminated intravascular coagulation: coagulopathy and thrombotic microangiopathy in snake envenoming. Semin. Thromb. Hemost. 2010, 36, 444–451. [Google Scholar] [CrossRef]
- Gutiérrez, J.M.; Ponce-Soto, L.A.; Marangoni, S.; Lomonte, B.; Alberto Ponce-Soto, L.; Marangoni, S.; Lomonte, B. Systemic and local myotoxicity induced by snake venom group II phospholipases A2: comparison between crotoxin, crotoxin B and a Lys49 PLA2 homologue. Toxicon 2008, 51, 80–92. [Google Scholar] [CrossRef]
- Ranawaka, U.K.; Lalloo, D.G.; Silva, H.J. De Neurotoxicity in Snakebite—The Limits of Our Knowledge. PLoS Negl. Trop. Dis. 2013, 7, e2302. [Google Scholar] [CrossRef]
- Sitprija, V. Snakebite nephropathy. Nephrology 2006, 11, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Herath, H.M.N.J.; Wazil, A.W.M.; Abeysekara, D.T.D.J.; Jeewani, N.D.C.; Weerakoon, K.G.A.D.; Ratnatunga, N.V.I.; Bandara, E.H.C.K.; Kularatne, S.A.M. Chronic kidney disease in snake envenomed patients with acute kidney injury in Sri Lanka: A descriptive study. Postgrad. Med. J. 2012, 88, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Antonypillai, C.N.; Wass, J.A.H.; Warrell, D.A.; Rajaratnam, H.N. Hypopituitarism following envenoming by Russell’s Vipers (Daboia siamensis and D. russelii) resembling Sheehan’s syndrome: First case report from Sri Lanka, a review of the literature and recommendations for endocrine management. QJM Int. J. Med. 2011, 104, 97–108. [Google Scholar] [CrossRef]
- Jayawardana, S.; Gnanathasan, A.; Arambepola, C.; Chang, T. Chronic Musculoskeletal Disabilities following Snake Envenoming in Sri Lanka: A Population-Based Study. PLoS Negl. Trop. Dis. 2016, 10, e0005103. [Google Scholar] [CrossRef]
- Jayawardana, S.; Arambepola, C.; Chang, T.; Gnanathasan, A. Long-term health complications following snake envenoming. J. Multidiscip. Healthc. 2018, 11, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.S.; Wijesinghe, C.A.; Jayamanne, S.F.; Buckley, N.A.; Dawson, A.H.; Lalloo, D.G.; de Silva, H.J. Delayed psychological morbidity associated with snakebite envenoming. PLoS Neglected Trop. Dis. 2011, 5, e1255. [Google Scholar] [CrossRef] [PubMed]
- Anz, A.W.; Schweppe, M.; Halvorson, J.; Bushnell, B.; Sternberg, M.; Koman, L.A. Management of Venomous Snakebite Injury to the Extremities. J. Am. Acad. Orthop. Surg. 2010, 18, 749–759. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.C.; Liu, P.Y.; Chiang, L.C.; Lai, C.S.; Lai, K.L.; Ho, C.H.; Wang, T.H.; Yang, C.C. Naja atra snakebite in Taiwan. Clin. Toxicol. 2018, 56, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.P.; Chuang, J.F.; Hsu, Y.P.; Wang, S.Y.; Fu, C.Y.; Yuan, K.C.; Chen, C.H.; Kang, S.C.; Liao, C.H. Predictors of the development of post-snakebite compartment syndrome. Scand. J. Trauma. Resusc. Emerg. Med. 2015, 23, 97. [Google Scholar] [CrossRef] [PubMed]
- Wagener, M.; Naidoo, M.; Aldous, C. Wound infection secondary to snakebite. South African Med. J. 2017, 107, 315. [Google Scholar] [CrossRef]
- Abubakar, S.B.; Habib, A.G.; Mathew, J. Amputation and disability following snakebite in Nigeria. Trop. Doct. 2010, 40, 114–116. [Google Scholar] [CrossRef]
- Wong, O.F.; Lam, T.S.K.; Fung, H.T.; Choy, C.H. Five-year experience with Chinese cobra (Naja atra)-related injuries in two acute hospitals in Hong Kong. Hong Kong Med. J. 2010, 16, 36–43. [Google Scholar] [PubMed]
- Wang, W.; Chen, Q.F.; Yin, R.X.; Zhu, J.J.; Li, Q.B.; Chang, H.H.; Wu, Y.B.; Michelson, E. Clinical features and treatment experience: A review of 292 Chinese cobra snakebites. Environ. Toxicol. Pharmacol. 2014, 37, 648–655. [Google Scholar] [CrossRef]
- Kularatne, S.A.M.; Budagoda, B.D.S.S.; Gawarammana, I.B.; Kularatne, W.K.S. Epidemiology, clinical profile and management issues of cobra (Naja naja) bites in Sri Lanka: first authenticated case series. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 924–930. [Google Scholar] [CrossRef]
- Milani Júnior, R.; Jorge, M.T.; de Campos, F.P.; Martins, F.P.; Bousso, A.; Cardoso, J.L.; Ribeiro, L.A.; Fan, H.W.; França, F.O.; Sano-Martins, I.S.; et al. Snake bites by the Jararacuçu (Bothrops jararacussu): clinicopathological studies of 29 proven cases in São Paulo State, Brazil. QJM Mon. J. Assoc. Physicians 1997, 90, 323–334. [Google Scholar] [CrossRef]
- Kallel, H.; Mayence, C.; Houcke, S.; Mathien, C.; Mehdaoui, H.; Gutiérrez, J.M.; Megarbane, B.; Hommel, D.; Resiere, D. Severe snakebite envenomation in French Guiana: When antivenom is not available. Toxicon 2018, 146, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Roriz, K.R.P.S.; Zaqueo, K.D.; Setubal, S.S.; Katsuragawa, T.H.; da Silva, R.R.; Fernandes, C.F.C.; Cardoso, L.A.P.; Rodrigues, M.M.D.S.; Soares, A.M.; Stábeli, R.G.; et al. Epidemiological study of snakebite cases in Brazilian western Amazonia. Rev. Soc. Bras. Med. Trop. 2018, 51, 338–346. [Google Scholar] [CrossRef]
- Ribeiro, L.A.; Jorge, M.T.; Lebrão, M.L. Prognostic factors for local necrosis in Bothrops jararaca (Brazilian pit viper) bites. Trans. R. Soc. Trop. Med. Hyg. 2001, 95, 630–634. [Google Scholar] [CrossRef]
- Maduwage, K.; Isbister, G.K.; Silva, A.; Bowatta, S.; Mendis, S.; Gawarammana, I. Epidemiology and clinical effects of hump-nosed pit viper (Genus: Hypnale) envenoming in Sri Lanka. Toxicon 2013, 61, 11–15. [Google Scholar] [CrossRef]
- Ariaratnam, C.A.; Thuraisingam, V.; Kularatne, S.A.M.; Sheriff, M.H.R.; Theakston, R.D.G.; de Silva, A.; Warrell, D.A. Frequent and potentially fatal envenoming by hump-nosed pit vipers (Hypnale hypnale and H. nepa) in Sri Lanka: lack of effective antivenom. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 1120–1126. [Google Scholar] [CrossRef]
- Mello, L.F.B.; Barcelos, M.G.; Meohas, W.; Pinto, L.W.; Melo, P.A.; Nogueira Neto, N.C.; Smith, J. Chronic ulceration of the leg following extensive scarring due to a snake bite complicated by squamous cell carcinoma. Skeletal Radiol. 2000, 29, 298–301. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Guidelines for the Prevention and Clinical Management of Snakebite in Africa; World Health Organisation: Brazzaville, Congo, 2010. [Google Scholar]
- Spano, S.J.; Vohra, R.; Macias, F. Long-term complications of rattlesnake bites: A telephone survey from central California. Wilderness Environ. Med. 2014, 25, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Kleggetveit, I.P.; Skulberg, P.K.; E, J. Complex regional pain syndrome following viper bite. Scand. J. Pain 2016, 10, 15–18. [Google Scholar] [CrossRef]
- Seo, Y.H.; Park, M.R.; Yoo, S.H. Development of complex regional pain syndrome after a snake bite: A case report. Korean J. Pain 2014, 27, 68–71. [Google Scholar] [CrossRef] [PubMed]
- Aktug Ergan, S.; Yoleri, O.; Yavasi, S.; Olmez, N.; Memis, A. Complex Regional Pain Syndrome Caused By Snake Bite: A Case Report. Türkiye Fiziksel Tip ve Rehabilitasyon Dergisi 2012, 58, 72–74. [Google Scholar]
- Wongtongkam, N.; Wilde, H.; Sitthi-Amorn, C.; Ratanabanangkoon, K. A study of 225 Malayan pit viper bites in Thailand. Mil. Med. 2005, 170, 342–348. [Google Scholar] [CrossRef]
- Chu, E.R.; Weinstein, S.A.; White, J.; Warrell, D.A. Venom ophthalmia caused by venoms of spitting elapid and other snakes: Report of ten cases with review of epidemiology, clinical features, pathophysiology and management. Toxicon 2010, 56, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Warrell, D.A.; Ormerod, L. Snake Venom Ophthalmia and Blindness Caused by the Spitting Cobra (Naja Nigricollis) in Nigeria. Am. J. Trop. Med. Hyg. 1976, 25, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Kularatne, S.A.M. Epidemiology and clinical picture of the Russell’s viper (Daboia russelli russelli) bite in Anuradhapura, Sri Lanka: A prospective study of 336 patients. Southeast Asian J. Trop. Med. Public Health 2000, 34, 855–862. [Google Scholar]
- Warrell, D.A.; Phillips, R.E. Bites by Russell’s viper (Vipera russelli siamensis) in Burma: haemostatic, vascular, and renal disturbances and response to treatment. Lancet 1985, 2, 427–433. [Google Scholar]
- Phillips, R.E.; Theakston, R.D.G.; Warrell, D.A.; Galigedara, Y.; Aloysius, D.J. Paralysis, Rhabdomyolysis and Haemolysis Caused by Bites of Russell’s Viper (Vipera russelli pulchella) in Sri Lanka: Failure of Indian (Haffkine) Antivenom. Q. J. Med. 1988, 68, 691–716. [Google Scholar]
- Hung, D.-Z.; Wu, M.-L.; Deng, J.-F.; Lin-Shiau, S.-Y. Russell’s viper snakebite in Taiwan: differences from other Asian countries. Toxicon 2002, 40, 1291–1298. [Google Scholar] [CrossRef]
- Al-homrany, M. Acute Renal Failure Following Snake Bite: Case Report and Review. Saudi J. Kidney Dis. Transpl. 1996, 7, 309–312. [Google Scholar]
- Alves, E.C.; Gonc, J.D.A.; Sousa, D.D.B.; De Oliveira, S.; Nascimento, F.; Santos, S.; Moura, M.; Wen, F.H.; Monteiro, W.M.; Carlos, L.; et al. Predicting acute renal failure in Bothrops snakebite patients in a tertiary reference center, Western Brazilian Amazon. PLoS ONE 2018, 13, 1–16. [Google Scholar] [CrossRef]
- Albuquerque, P.L.M.M.; Silva Junior, G.B.; Jacinto, C.N.; Lima, J.B.; Lima, C.B.; Amaral, Y.S.; Veras, M.D.S.B.; Mota, R.M.S.; Daher, E.F. Acute kidney injury after snakebite accident treated in a Brazilian tertiary care centre. Nephrology 2014, 19, 764–770. [Google Scholar] [CrossRef]
- Pinho, F.M.O.; Zanetta, M.T.D.; Brdmann, E.A. Acute renal failure after Crotalus durissus snakebite: A prospective survey on 100 patients. Kidney Int. 2005, 67, 659–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, G.E.; Brown, S.G.A.; Buckley, N.A.; O’Leary, M.A.; Page, C.B.; Currie, B.J.; White, J.; Isbister, G.K. Clinical effects and antivenom dosing in brown snake (Pseudonaja spp.) envenoming--Australian snakebite project (ASP-14). PLoS ONE 2012, 7, e53188. [Google Scholar] [CrossRef] [PubMed]
- Johnston, C.I.; Ryan, N.M.; O’Leary, M.A.; Brown, S.G.A.; Isbister, G.K. Australian taipan (Oxyuranus spp.) envenoming: clinical effects and potential benefits of early antivenom therapy—Australian Snakebite Project (ASP-25). Clin. Toxicol. 2017, 55, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Isbister, G.K.; O’Leary, M.A.; Elliott, M.; Brown, S.G.A. Tiger snake (Notechis spp) envenoming: Australian Snakebite Project (ASP-13). Med. J. Aust. 2012, 197, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Waikhom, R.; Sircar, D.; Patil, K.; Bennikal, M.; Gupta, S.D.; Pandey, R. Long-term renal outcome of snake bite and acute kidney injury: A single-center experience. Ren. Fail. 2012, 34, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Pulimaddi, R.; Parveda, A.R.; Brahmanpally, B.; Kalakanda, P.M.; Ramakrishna, K.; Chinnapaka, V.R.D. Incidence & prognosis of acute kidney injury in individuals of snakebite in a tertiary care hospital in India. Indian J. Med. Res. 2017, 145, 163–174. [Google Scholar]
- Golay, V.; Roychowdhary, A.; Pandey, R.; Singh, A.; Pasari, A.; Abraham, A. Single Center Experience of a Rare Presentation. Saudi J. Kidney Dis. Transplant. 2012, 23, 1262–1267. [Google Scholar]
- Sinha, R.; Nandi, M.; Tullus, K.; Marks, S.D.; Taraphder, A. Ten-year follow-up of children after acute renal failure from a developing country. Nephrol. Dial. Transplant. 2009, 24, 829–833. [Google Scholar] [CrossRef] [PubMed]
- Prasarnpun, S.; Walsh, J.; Awad, S.S.; Harris, J.B. Envenoming bites by kraits: the biological basis of treatment-resistant neuromuscular paralysis. Brain 2005, 128, 2987–2996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, J.B.; Scott-Davey, T. Secreted phospholipases A2 of snake venoms: effects on the peripheral neuromuscular system with comments on the role of phospholipases A2 in disorders of the CNS and their uses in industry. Toxins (Basel) 2013, 1, 2533–2571. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.; Cristofori-Armstrong, B.; Rash, L.D.; Hodgson, W.C.; Isbister, G.K. Defining the role of post-synaptic α-neurotoxins in paralysis due to snake envenoming in humans. Cell. Mol. Life Sci. 2018, 75, 4465–4478. [Google Scholar] [CrossRef]
- Tasoulis, T.; Isbister, G. A Review and Database of Snake Venom Proteomes. Toxins (Basel) 2017, 9, 290. [Google Scholar] [CrossRef]
- Kularatne, S.A.M. Common krait (Bungarus caeruleus) bite in Anuradhapura, Sri Lanka: a prospective clinical study, 1996–98. Postgrad. Med. J. 2002, 78, 276–280. [Google Scholar] [CrossRef]
- Connolly, S.; Trevett, A.J.; Nwokolo, N.C.; Lalloo, D.G.; Naraqi, S.; Mantle, D.; Schofield, I.S.; Fawcett, P.R.W.; Harris, J.B.; Warrell, D.A. Neuromuscular effects of Papuan Taipan snake venom. Ann. Neurol. 1995, 38, 916–920. [Google Scholar] [CrossRef]
- Silva, A.; Maduwage, K.; Sedgwick, M.; Pilapitiya, S.; Weerawansa, P.; Dahanayaka, N.J.; Buckley, N.A.; Johnston, C.; Siribaddana, S.; Isbister, G.K. Neuromuscular Effects of Common Krait (Bungarus caeruleus) Envenoming in Sri Lanka. PLoS Negl. Trop. Dis. 2016, 10, e0004368. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.J.; Wijegunasinghe, D.; Samarakoon, S.; Palipana, H.; Gunasekera, S.; de Silva, H.A.; Lalloo, D.G.; Ranawaka, U.K.; de Silva, H.J. Neurophysiological findings in patients 1 year after snake bite induced neurotoxicity in Sri Lanka. Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Weinelt, W.; Sattler, R.W.; Mebs, D. Persistent paresis of the facialis muscle after European adder (Vipera berus) bite on the forehead. Toxicon 2002, 40, 1627–1629. [Google Scholar] [CrossRef]
- Awasthi, R.; Narang, S.; Chowdhury, P.P. Cerebellar ataxia following snake bite. J. Assoc. Physicians India 2010, 58, 391–393. [Google Scholar]
- Chaudhary, S.C.; Sawlani, K.K.; Malhotra, H.S.; Singh, J. Snake bite-induced leucoencephalopathy. BMJ Case Rep. 2013, 2012–2014. [Google Scholar] [CrossRef]
- Samanta, S.K.; Mahapatra, N.C.; Fariduddin, K.; Mazumdar, D.B.; Mandal, K. Cortical blindness and paraplegia following hypoxic ischemic encephalopathy as a complication of common krait bite. Nepal J. Ophthalmol. 2011, 3, 206–209. [Google Scholar] [CrossRef]
- De Silva, U.; Sarathchandra, C.; Senanayake, H.; Pilapitiya, S.; Siribaddana, S.; Silva, A. Hyponatraemia and seizures in Merrem’s hump-nosed pit viper (Hypnale hypnale) envenoming: a case report. J. Med. Case Rep. 2018, 2–4. [Google Scholar]
- Dhaliwal, U. Cortical blindness: an unusual sequela of snake bite. Indian J. Ophthalmol. 1999, 47, 191–192. [Google Scholar] [PubMed]
- Jalali, S.; Padhi, T.R.; Bansal, R.; Sahoo, K.; Basu, S.; Mathai, A. Visual loss with inner retinal dysfunction, after snake bite: Two case reports. Doc. Ophthalmol. 2013, 127, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Guttmann-Friedmann, A. Blindness After Snake-Bite. Br. J. Ophthalmol. 1956, 40, 57–59. [Google Scholar] [CrossRef] [PubMed]
- Mosquera, A.; Idrovo, L.; Tafur, A.; Del Brutto, H. Stroke following Bothrops spp. snakebite. Neurology 2003, 60, 1577–1580. [Google Scholar] [CrossRef]
- Berling, I.; Brown, S.G.A.; Miteff, F.; Levi, C.; Isbister, G.K. Intracranial haemorrhages associated with venom induced consumption coagulopathy in Australian snakebites (ASP-21). Toxicon 2015, 102, 8–13. [Google Scholar] [CrossRef]
- Bartholdi, D.; Selic, C.; Meier, J.; Jung, H. Viper snakebite causing symptomatic intracerebral haemorrhage. J. Neurol. 2004, 251, 889–891. [Google Scholar] [CrossRef]
- Adepoju, F.; Katibi, O.; Ernest, S.; Monsudi, K.; Olorunsola, B. Blindness and scalp haematoma in a child following a snakebite. Afr. Health Sci. 2015, 15, 1041. [Google Scholar]
- Mustapha, S.K.; Mubi, B.M.; Askira, B.H. Bilateral blindness following snakebite. Trop. Doct. 2010, 40, 117–118. [Google Scholar] [CrossRef] [PubMed]
- Laothong, C.; Sitprija, V. Decreased parasympathetic activities in Malayan krait (Bungarus candidus) envenoming. Toxicon 2001, 39, 1353–1357. [Google Scholar] [CrossRef]
- Isbister, G.K.; Hooper, M.R.; Dowsett, R.; Maw, G.; Murray, L.; White, J. Collett’s snake (Pseudechis colletti) envenoming in snake handlers. QJM 2006, 99, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Pearn, J.; McGuire, B.; McGuire, L.; Richardson, P. The envenomation syndrome caused by the Australian Red-bellied Black Snake Pseudechis porphyriacus. Toxicon 2000, 38, 1715–1729. [Google Scholar] [CrossRef]
- Sethi, M.; Cook, M.; Winkel, K.D. Persistent anosmia and olfactory bulb atrophy after mulga (Pseudechis australis) snakebite. J. Clin. Neurosci. 2016, 29, 199–201. [Google Scholar] [CrossRef]
- Warrell, D.A.; Phillips, R.E.; Moore, R.A.; Burke, C.W. Acute and chronic pitutary failure resembling Sheehan’s syndrome following bites by Russell’s viper in Burma. Lancet 1987, 330, 763–767. [Google Scholar]
- Jeevagan, V.; Katulanda, P.; Gnanathasan, C.A.; Warrell, D. A Acute pituitary insufficiency and hypokalaemia following envenoming by Russell’s viper (Daboia russelii) in Sri Lanka: Exploring the pathophysiological mechanisms. Toxicon 2013, 63, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Senthilkumaran, S.; Menezes, R.G.; Hussain, S.A.; Luis, S.A.; Thirumalaikolundusubramanian, P. Russell’s Viper Envenomation-Associated Addisonian Crisis. Wilderness Environ. Med. 2018, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Proby, C.; Tha, A.; Thet, W.; Hla, M.; Burrin, J.M.; Joplin, G.F. Immediate and long-term effects on hormone levels following bites by the Burmese Russell’s viper. Q. J. Med. 1990, 75, 399–411. [Google Scholar] [PubMed]
- Srinivasan, K.G.; Srividya, S.; Usha Nandhini, K.P.; Ramprabananth, S. Chronic pituitary failure resembling Sheehan’s syndrome following a bite of Russell’s viper: A case report. Neuroradiol. J. 2010, 23, 38–41. [Google Scholar] [CrossRef]
- Shivaprasad, C.; Aiswarya, Y.; Sridevi, A.; Anupam, B.; Amit, G.; Rakesh, B.; Annie, P.A.; Anish, K. Delayed hypopituitarism following Russell’s viper envenomation: a case series and literature review. Pituitary 2019, 22, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Prabhakar, A.; Gupta, V.; Bhansali, A.; Vyas, S.; Khandelwal, N. Hypopitutarism secondary to snake envenomation. Neurol. India 2013, 61, 310–311. [Google Scholar]
- Nagaraju, N.B.; Bhalla, A.; Sharma, N.; Mokta, J.; Singh, S.; Gupta, P.; Rai, A.; Subbiah, S.; Bhansali, A.; Dutta, P. Pituitary dysfunction in survivors of Russell’s viper snake bite envenomation: A prospective study. Neurol. India 2018, 66, 1351–1358. [Google Scholar]
- Ratnakaran, B.; Punnoose, V.; Das, S.; Kartha, A. Psychosis in secondary empty sella syndrome following a Russell’s viper bite. Indian J. Psychol. Med. 2016, 38, 254–256. [Google Scholar] [CrossRef] [PubMed]
- Golay, V.; Roychowdhary, A.; Dasgupta, S.; Pandey, R. Hypopituitarism in patients with vasculotoxic snake bite envenomation related acute kidney injury: A prospective study on the prevalence and outcomes of this complication. Pituitary 2014, 17, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, S.K.; Bandyopadhyay, R.; Cutts, A.; Pal, S.K. Hypopituitarism following poisonous viperbite. J. Indian Med. Assoc. 2013, 110, 120–122. [Google Scholar]
- Muhammed, A.; Dalhat, M.M.; Joseph, B.O.; Ahmed, A.; Nguku, P.; Poggensee, G.; Adeiza, M.; Yahya, G.I.; Hamza, M.; Habib, Z.G.; et al. Predictors of depression among patients receiving treatment for snakebite in General Hospital, Kaltungo, Gombe State, Nigeria: August 2015. Int. J. Ment. Health Syst. 2017, 11, 1–7. [Google Scholar] [CrossRef]
- Wijesinghe, C.; Williams, S.; Kasturiratne, A.; Dolawaththa, N.; Wimalaratne, P.; Wijewickrema, B.; Jayamanne, S.; Isbister, G.; Dawson, A.; Lalloo, D.; et al. A Randomized Controlled Trial of a Brief Intervention for Delayed Psychological Effects in Snakebite Victims. PLoS Negl. Trop. Dis. 2015, 9, e0003989. [Google Scholar] [CrossRef]
- Williams, D.; Gutiérrez, J.M.; Harrison, R.; Warrell, D.A.; White, J.; Winkel, K.D.; Gopalakrishnakone, P. The Global Snake Bite Initiative: An antidote for snake bite. Lancet 2010, 375, 89–91. [Google Scholar] [CrossRef]
- Isbister, G.K.; Silva, A. Addressing the global challenge of snake envenoming. Lancet 2018, 6736, 1–2. [Google Scholar] [CrossRef]
- Silva, A.; Marikar, F.; Murugananthan, A.; Agampodi, S. Awareness and perceptions on prevention, first aid and treatment of snakebites among Sri Lankan farmers: A knowledge practice mismatch? J. Occup. Med. Toxicol. 2014, 9, 20. [Google Scholar] [CrossRef]
- Isbister, G.K. Snake antivenom research: the importance of case definition. Emerg. Med. J. 2005, 22, 399–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waiddyanatha, S.; Silva, A.; Siribaddana, S.; Isbister, G.K. Long-term Effects of Snake Envenoming. Toxins 2019, 11, 193. https://doi.org/10.3390/toxins11040193
Waiddyanatha S, Silva A, Siribaddana S, Isbister GK. Long-term Effects of Snake Envenoming. Toxins. 2019; 11(4):193. https://doi.org/10.3390/toxins11040193
Chicago/Turabian StyleWaiddyanatha, Subodha, Anjana Silva, Sisira Siribaddana, and Geoffrey K. Isbister. 2019. "Long-term Effects of Snake Envenoming" Toxins 11, no. 4: 193. https://doi.org/10.3390/toxins11040193
APA StyleWaiddyanatha, S., Silva, A., Siribaddana, S., & Isbister, G. K. (2019). Long-term Effects of Snake Envenoming. Toxins, 11(4), 193. https://doi.org/10.3390/toxins11040193