Epidemiology and Clinical Features of Ciguatera Fish Poisoning in Hong Kong

Abstract
:1. Introduction
2. Published Reports and Statistics on Ciguatera
3. First Reports of Ciguatera in Hong Kong
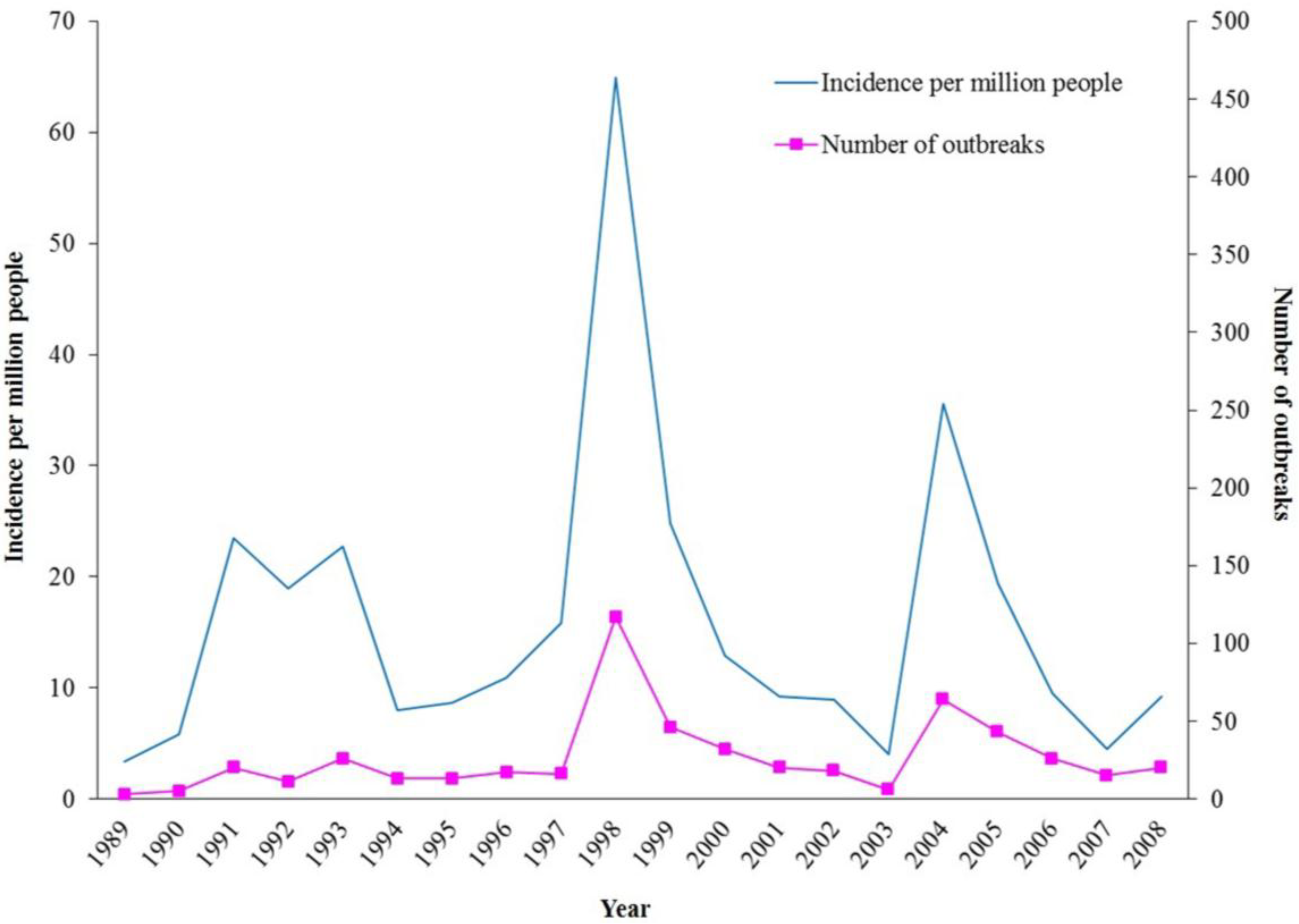
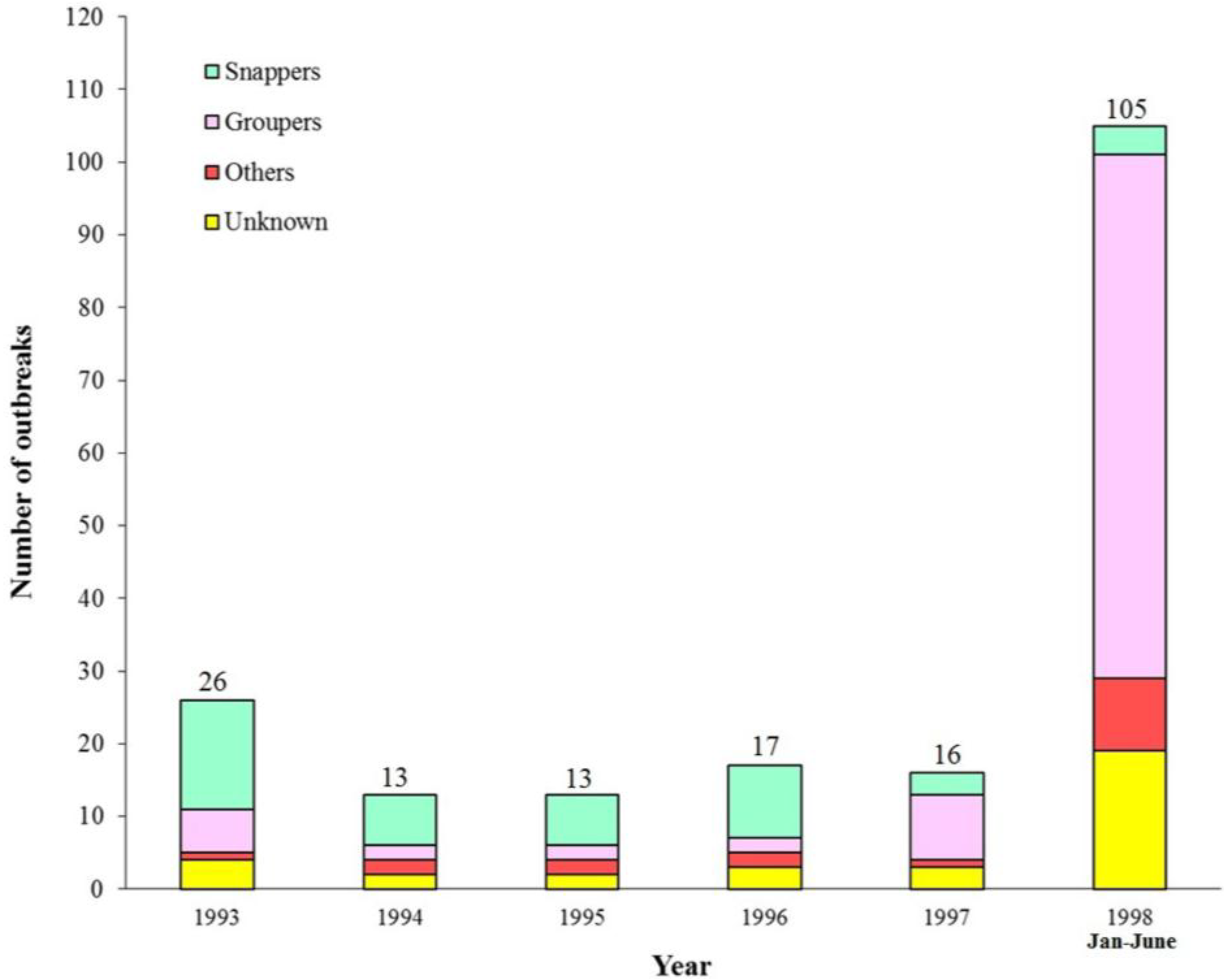
4. Incidence of Ciguatera and the Fish Species Responsible


5. Ciguatoxins Responsible
6. Clinical Manifestations and Notable Cases

{kind=link}
{kind=link}
| Choi et al. [11] a | Au [16] a | Chan et al. [21] b | |
|---|---|---|---|
| 1988–1992 (n = 397) | 1993–2005 (n = 300) | 2003–2006 (n = 18) c | |
| Incubation period (range, median) | 1–30 h (7.5 h) | 0.25–43 h (5.5 h) | 1–7 h |
| Gastrointestinal | |||
| Nausea | 29 | 40 | 61 |
| Vomiting | 22 | 31 | 78 |
| Abdominal pain | 47 | 59 | 56 |
| Diarrhea | 58 | 74 | 94 |
| Neurological | |||
| Paresthesia/numbness (4 limbs) | 78 | 79 | 67 |
| Paresthesia/numbness (perioral/tongue/face) | 30 | 54 | 50 |
| Muscle weakness | 44 | 54 | 50 |
| Myalgia | 24 | - e | 22 |
| Headache | 19 | 19 | 0 |
| Hot/cold reversal | 16 | 19 | 6 |
| Dizziness d | - e | 37 | 61 |
| Cardiovascular | |||
| Bradycardia | 0.3 | - e | 94 |
| Hypotension | 0.3 | - e | 94 |
| General | |||
| Fatigue | 59 | - e | 6 |
| Pruritus | 11 | - e | 6 |
| Skin rash | 2 | - e | 0 |
7. Diagnosis and Treatment
8. Prevention
9. Conclusions
Acknowledgments
Conflicts of Interest
References
- FAO. Ciguatera fish poisoning. In Marine Biotoxins. FAO Food and Nutrition Paper 80; Food and Agriculture Organization of the United Nations: Rome, Italy, 2004; pp. 185–218. [Google Scholar]
- Litaker, R.W.; Vandersea, M.W.; Faust, M.A.; Kibler, S.R.; Nau, A.W.; Holland, W.C.; Chinain, M.; Holmes, M.J.; Tester, P.A. Global distribution of ciguatera causing dinoflagellates in the genus Gambierdiscus. Toxicon 2010, 56, 711–730. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.J. Ciguatera: Australian perspectives on a global problem. Toxicon 2006, 48, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Vetter, I.; Zimmermann, K.; Lewis, R.J. Ciguatera toxins: Pharmacology, toxicology, and detection. In Seafood and Freshwater Toxins: Pharmacology, Toxicology, and Detection, 3rd ed.; Botana, L.M., Ed.; CRC Press: Boca Raton, FL, USA, 2014; pp. 925–950. [Google Scholar]
- Geller, R.J.; Benowitz, N.L. Orthostatic hypotension in ciguatera fish poisoning. Arch. Intern. Med. 1992, 152, 2131–2133. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.Y.K. Ciguatera caused by consumption of humphead wrasse. Toxicon 2013, 76, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.Y.K. Large outbreaks of ciguatera after consumption of brown marbled grouper. Toxins 2014, 6, 2041–2049. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.Y.K.; Wang, A.Y.M. Life-threatening bradycardia and hypotension in a patient with ciguatera fish poisoning. Trans. R. Soc. Trop. Med. Hyg. 1993, 87, 71. [Google Scholar] [CrossRef] [PubMed]
- Dickey, R.W.; Plakas, S.M. Ciguatera: A public health perspective. Toxicon 2010, 56, 123–136. [Google Scholar] [CrossRef] [PubMed]
- Glaziou, P.; Legrand, A.M. The epidemiology of ciguatera fish poisoning. Toxicon 1994, 32, 863–873. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.M.Y.; Wong, M.M.H. Epidemiology of ciguatera poisoning in Hong Kong. Public Health Epidemiol. Report 1994, 3, 12–14. [Google Scholar]
- Chan, T.Y.K.; Critchley, J.A.J.H.; Chan, J.C.N.; Tomlinson, B.; Lai, V.S.M.; Anderson, P.J.; Lau, G.S.N. The drug and poisons information bureau at the Chinese university of Hong Kong. J. Hong Kong Med. Assoc. 1993, 45, 202–205. [Google Scholar]
- Leung, K.P.; Chan, T.Y.K.; Sze, F.K.H. Ciguatera poisoning in Hong Kong: A report of two cases. Southeast Asian J. Trop. Med. Public Health 1992, 22, 543–544. [Google Scholar]
- Kwan, L.C.; Cheung, D.K.; Kam, K.M. Peak occurrences of ciguatera fish poisoning precede cholera outbreaks in Hong Kong. Epidemiol. Infect. 2003, 131, 621–626. [Google Scholar] [CrossRef]
- Wong, C.K.; Hung, P.; Lee, K.L.H.; Kam, K.M. Study of an outbreak of ciguatera fish poisoning in Hong Kong. Toxicon 2005, 46, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Au, A. Ciguatera fish poisoning on the rise—A review of cases (January 2004–May 2005). Communicable Diseases Watch 2005, 13, 49–50. [Google Scholar]
- Chan, T.Y.K. Ciguatera poisoning in Hong Kong. H.K. Epidemiol. Assoc. Newsl. 1999, 3, 3. [Google Scholar]
- Wong, C.K.; Hung, P.; Lee, K.L.H.; Mok, T.; Chung, T.; Kam, K.M. Features of ciguatera fish poisoning cases in Hong Kong 2004–2007. Biomed. Environ. Sci. 2008, 21, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.; Hung, P.; Lee, K.L.H.; Kam, K.M. Solid-phase extraction clean-up of ciguatoxin-contaminated coral fish extracts for use in the mouse bioassay. Food Addit. Contam. 2009, 26, 236–247. [Google Scholar] [CrossRef]
- Wong, C.K.; Hung, P.; Lo, J.Y. Ciguatera fish poisoning in Hong Kong—A 10-year perspective on the class of ciguatoxins. Toxicon 2014, 86, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.Y.K.; Chan, J.C.M.; Wong, R.S.M. Incidence and severity of hypotension and bradycardia in ciguatera (abstract). Clin. Toxicol. 2014, 52, 353. [Google Scholar] [CrossRef]
- Cheng, C.C.; Chung, C.H. Ciguatera fish poisoning: A challenge to emergency physicians. Hong Kong J. Emerg. Med. 2004, 11, 173–177. [Google Scholar]
- Sia, J.Y.S.; Kan, P.G. Ciguatera fish poisoning: A challenge to emergency physicians (letter). Hong Kong J. Emerg. Med. 2004, 11, 251–252. [Google Scholar]
- Chan, T.Y.K. Severe bradycardia and prolonged hypotension in ciguatera. Singapore Med. J. 2013, 54, e120–e122. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.Y.K. Lengthy persistence of ciguatoxin in the body. Trans. R. Soc. Trop. Med. Hyg. 1998, 92, 662. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.Y.K.; Kwok, T.C.Y. Chronicity of neurological features in ciguatera fish poisoning. Hum. Exp. Toxicol. 2001, 20, 426–428. [Google Scholar] [CrossRef] [PubMed]
- Pearn, J.H.; Lewis, R.J.; Ruff, T.; Tait, M.; Quinn, J.; Murtha, W.; King, G.; Mallett, A.; Gillespie, N.C. Ciguatera and mannitol: Experience with a new treatment regimen. Med. J. Aust. 1989, 151, 77–80. [Google Scholar] [PubMed]
- Schnorf, H.; Taurarii, M.; Cundy, T. Ciguatera fish poisoning: A double-blind randomized trial of mannitol therapy. Neurology 2002, 58, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Centre for Food Safety. Food Safety Focus (Hong Kong), 51st issue. Ciguatera fish poisoning. Available online: http://www.cfs.gov.hk/english/multimedia/multimedia_pub/files/FSF51_2010-10-20.pdf (accessed on 22 August 2014).
- Food and Environmental Hygiene Department. Code of Practice on the Import and Sale of Live Marine Fish for Human Consumption for Prevention and Control of Ciguatera Fish Poisoning. Available online: http://www.cfs.gov.hk/english/whatsnew/whatsnew_fsf/files/fish_cop_e.pdf (accessed on 22 August 2014).
- Centre for Food Safety. Food Safety Ordinance (Chapter 612). Available online: http://www.cfs.gov.hk/english/whatsnew/whatsnew_fstr/whatsnew_fstr_Food_Safety_Bill.html (accessed on 22 August 2014).
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, T.Y.K. Epidemiology and Clinical Features of Ciguatera Fish Poisoning in Hong Kong. Toxins 2014, 6, 2989-2997. https://doi.org/10.3390/toxins6102989
Chan TYK. Epidemiology and Clinical Features of Ciguatera Fish Poisoning in Hong Kong. Toxins. 2014; 6(10):2989-2997. https://doi.org/10.3390/toxins6102989
Chicago/Turabian StyleChan, Thomas Y. K. 2014. "Epidemiology and Clinical Features of Ciguatera Fish Poisoning in Hong Kong" Toxins 6, no. 10: 2989-2997. https://doi.org/10.3390/toxins6102989
APA StyleChan, T. Y. K. (2014). Epidemiology and Clinical Features of Ciguatera Fish Poisoning in Hong Kong. Toxins, 6(10), 2989-2997. https://doi.org/10.3390/toxins6102989