Outcomes According to MSKCC Risk Score with Focus on the Intermediate-Risk Group in Metastatic Renal Cell Carcinoma Patients Treated with First-Line Sunitinib: A Retrospective Analysis of 2390 Patients

 ,
,  ,
,
Abstract
:1. Background
2. Materials and Methods
2.1. Study Design and Treatment
2.2. Data Source
2.3. Outcome Assessment
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
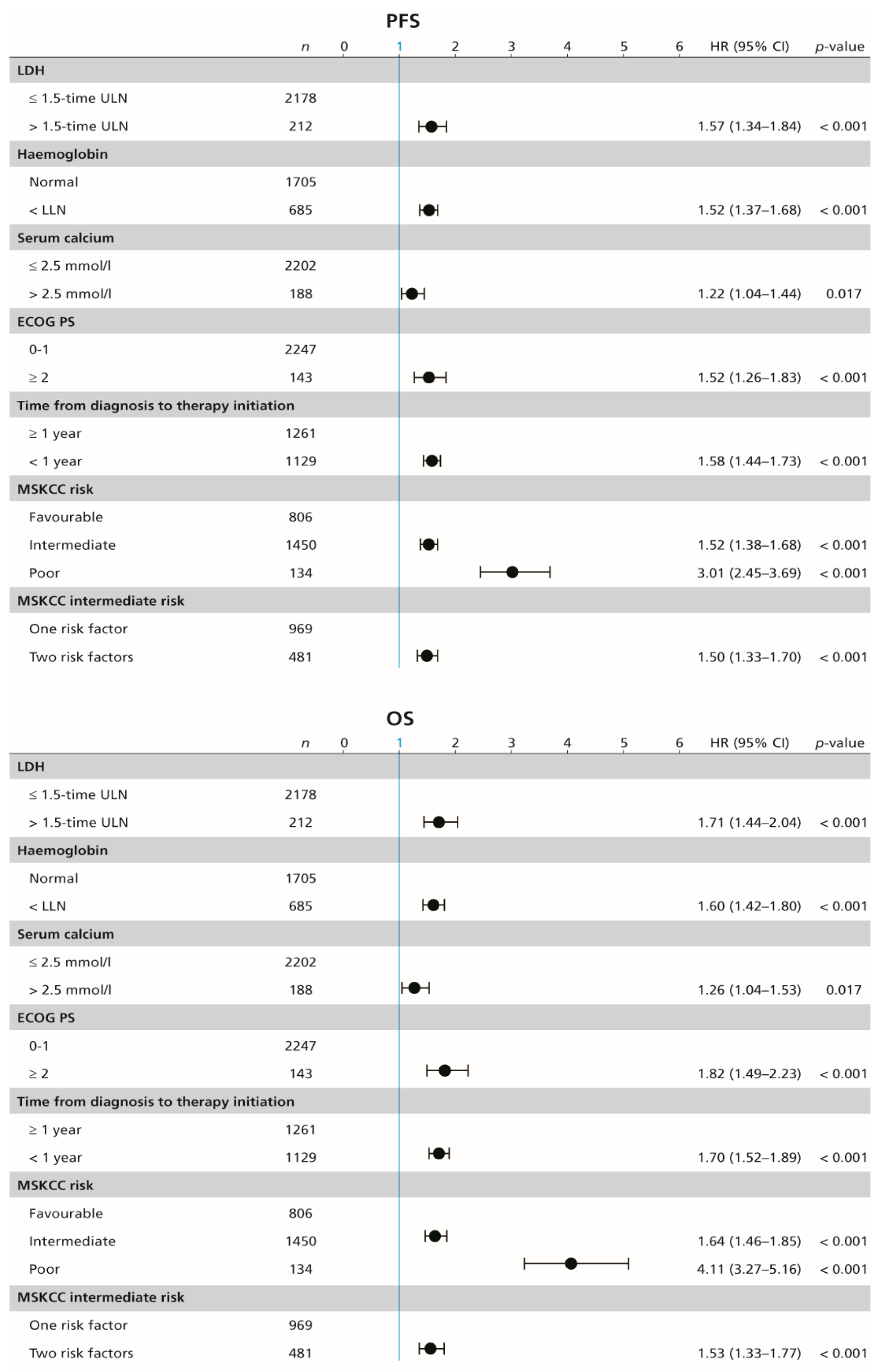
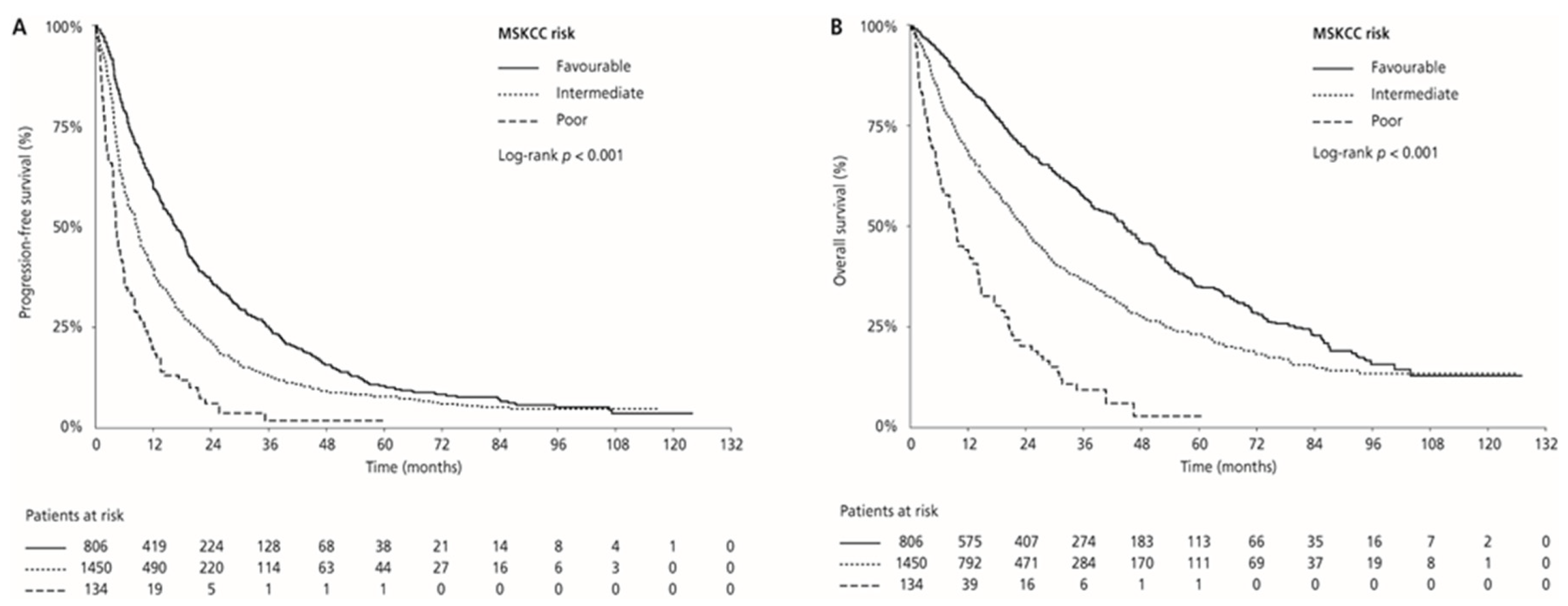
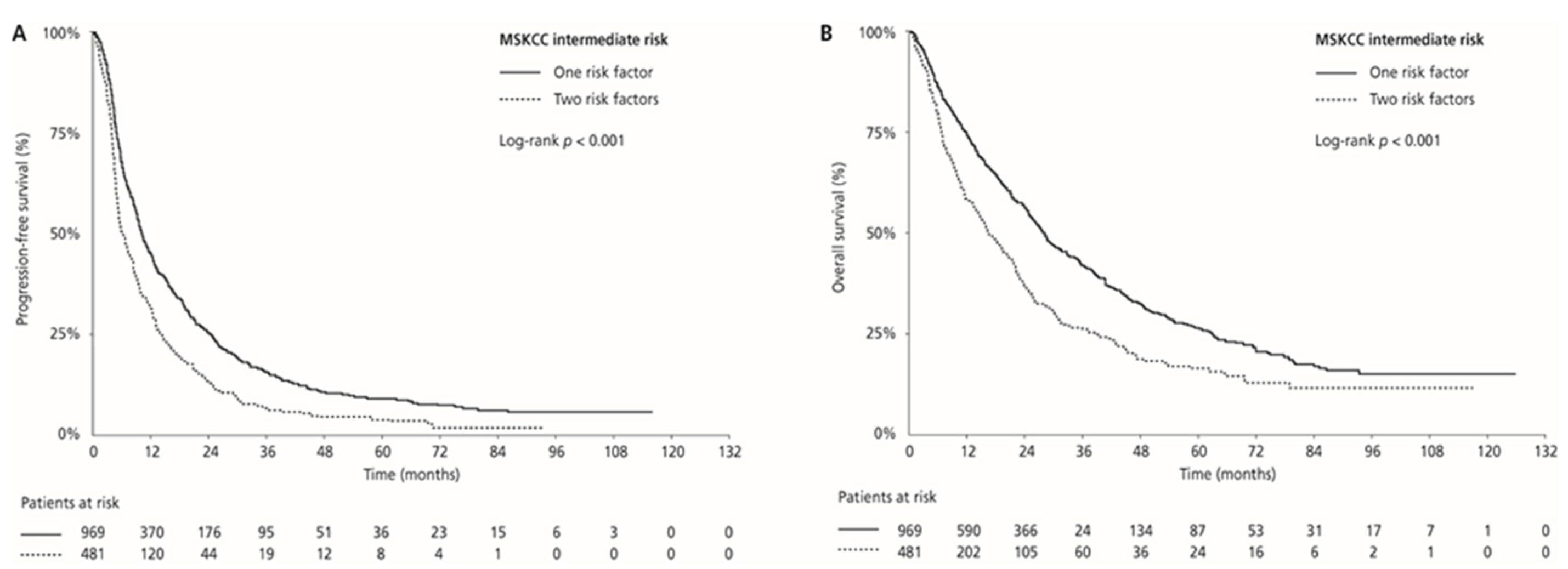
3.2. Treatment Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Znaor, A.; Lortet-Tieulent, J.; Laversanne, M.; Jemal, A.; Bray, F. International variations and trends in renal cell carcinoma incidence and mortality. Eur. Urol. 2015, 67, 519. [Google Scholar] [CrossRef]
- Srigley, J.R.; Delahunt, B.; Eble, J.N.; Egevad, L.; Epstein, J.I.; Grignon, D.; Hes, O.; Moch, H.; Montironi, R.; Tickoo, S.K.; et al. The International Society of Urological Pathology (ISUP) Vancouver classification of renal neoplasia. Am. J. Surg. Pathol. 2013, 37, 1469–1489. [Google Scholar] [CrossRef]
- Motzer, R.J.; Bacik, J.; Murphy, B.A.; Russo, P.; Mazumdar, M. Interferon-alfa as a comparative treatment for clinical trials of new therapies against advanced renal cell carcinoma. J. Clin. Oncol. 2002, 20, 289–296. [Google Scholar] [CrossRef]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Oudard, S.; Negrier, S.; Szczylik, C.; Pili, R.; Bjarnason, G.A.; et al. Overall survival and updated results for sunitinib compared with interferon alfa in patients with metastatic renal cell carcinoma. J. Clin. Oncol. 2009, 27, 3584–3590. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, C.N.; Davis, I.D.; Mardiak, J.; Szczylik, C.; Lee, E.; Wagstaff, J.; Barrios, C.H.; Salman, P.; Gladkov, O.A.; Kavina, A.; et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a randomized phase III trial. J. Clin. Oncol. 2010, 28, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- Buchler, T.; Klapka, R.; Melichar, B.; Brabec, P.; Dusek, L.; Vyzula, R.; Abrahamova, J. Sunitinib followed by sorafenib or vice versa for metastatic renal cell carcinoma – data from the Czech registry. Ann. Oncol. 2012, 23, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumours. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 3, 205–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motzer, R.J.; Mazumdar, M.; Bacik, J.; Berg, W.; Amsterdam, A.; Ferrara, J. Survival and prognostic stratification of 670 patients with advanced renal cell carcinoma. J. Clin. Oncol. 1999, 17, 2530–2540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekhail, T.M.; Abou-Jawde, R.M.; Boumerhi, G.; Malhi, S.; Wood, L.; Elson, P.; Bukowski, R. Validation and extension of the Memorial Sloan-Kettering prognostic factors model for survival in patients with previously untreated metastatic renal cell carcinoma. J. Clin. Oncol. 2005, 23, 832–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heng, D.Y.; Xie, W.; Regan, M.M.; Harshman, L.C.; Bjarnason, G.A.; Vaishampayan, U.N.; Mackenzie, M.; Wood, L.; Donskov, F.; Tan, M.H.; et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol. 2013, 14, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T.; et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Cella, D.; Reeves, J.; Hawkins, R.; Guo, J.; Nathan, P.; Staehler, M.; de Souza, P.; Merchan, J.R.; et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N. Engl. J. Med. 2013, 369, 722–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escudier, B.; Pluzanska, A.; Koralewski, P.; Ravaud, A.; Bracarda, S.; Szczylik, C.; Chevreau, C.; Filipek, M.; Melichar, B.; Bajetta, E.; et al. Bevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: a randomised, double-blind phase III trial. Lancet 2007, 370, 2103–2111. [Google Scholar] [CrossRef]
- Hutson, T.E.; Lesovoy, V.; Al-Shukri, S.; Stus, V.P.; Lipatov, O.N.; Bair, A.H.; Rosbrook, B.; Chen, C.; Kim, S.; Vogelzang, N.J. Axitinib versus sorafenib as first-line therapy in patients with metastatic renal-cell carcinoma: a randomised open-label phase 3 trial. Lancet Oncol. 2013, 14, 1287–1294. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Halabi, S.; Sanford, B.L.; Hahn, O.; Michaelson, M.D.; Walsh, M.K.; Feldman, D.R.; Olencki, T.; Picus, J.; Small, E.J.; et al. Cabozantinib Versus Sunitinib As Initial Targeted Therapy for Patients With Metastatic Renal Cell Carcinoma of Poor or Intermediate Risk: The Alliance A031203 CABOSUN Trial. J. Clin. Oncol. 2017, 35, 591–597. [Google Scholar] [CrossRef]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Arén Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulières, D.; Melichar, B.; et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef]
- Rini, B.I.; Powles, T.; Atkins, M.B.; Escudier, B.; McDermott, D.F.; Suarez, C.; Bracarda, S.; Stadler, W.M.; Donskov, F.; Lee, J.L.; et al. Atezolizumab plus bevacizumab versus sunitinib in patients with previously untreated metastatic renal cell carcinoma (IMmotion151): a multicentre, open-label, phase 3, randomised controlled trial. Lancet. 2019, 393, 2404–2415. [Google Scholar] [CrossRef]
- Motzer, R.J.; Penkov, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Negrier, S.; Uemura, M.; et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef]
- Rini, B.I.; Hutson, T.E.; Figlin, R.A.; Lechuga, M.J.; Valota, O.; Serfass, L.; Rosbrook, B.; Motzer, R.J. Sunitinib in Patients With Metastatic Renal Cell Carcinoma: Clinical Outcome According to International Metastatic Renal Cell Carcinoma Database Consortium Risk Group. Clin. Genitourin Cancer 2018, 16, 298–304. [Google Scholar] [CrossRef]
- Kubackova, K.; Melichar, B.; Bortlicek, Z.; Pavlik, T.; Poprach, A.; Svoboda, M.; Lakomy, R.; Vyzula, R.; Kiss, I.; Dusek, L.; et al. Comparison of Two Prognostic Models in Patients with Metastatic Renal Cancer Treated with Sunitinib: a Retrospective, Registry-Based Study. Target. Oncol. 2015, 10, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Kwon, W.A.; Cho, I.C.; Yu, A.; Nam, B.H.; Joung, J.Y.; Seo, H.K.; Lee, K.H.; Chung, J. Validation of the MSKCC and Heng risk criteria models for predicting survival in patients with metastatic renal cell carcinoma treated with sunitinib. Ann. Surg. Oncol. 2013, 20, 4397–4404. [Google Scholar] [CrossRef] [PubMed]
- Bamias, A.; Karadimou, A.; Lampaki, S.; Lainakis, G.; Malettou, L.; Timotheadou, E.; Papazisis, K.; Andreadis, C.; Kontovinis, L.; Anastasiou, I.; et al. Prognostic stratification of patients with advanced renal cell carcinoma treated with sunitinib: comparison with the Memorial Sloan-Kettering prognostic factors model. BMC Cancer 2010, 10, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gore, M.E.; Szczylik, C.; Porta, C.; Bracarda, S.; Bjarnason, G.A.; Oudard, S.; Lee, S.H.; Haanen, J.; Castellano, D.; Vrdoljak, E.; et al. Final results from the large sunitinib global expanded-access trial in metastatic renal cell carcinoma. Br. J. Cancer 2015, 113, 9–12. [Google Scholar] [CrossRef] [Green Version]
- Motzer, R.J.; Nosov, D.; Eisen, T.; Bondarenko, I.; Lesovoy, V.; Lipatov, O.; Tomczak, P.; Lyulko, O.; Alyasova, A.; Harza, M.; et al. Tivozanib versus sorafenib as initial targeted therapy for patients with metastatic renal cell carcinoma: results from a phase III trial. J. Clin. Oncol. 2013, 31, 3791–3799. [Google Scholar] [CrossRef]
- Eichelberg, C.; Vervenne, W.L.; De Santis, M.; Fischer von Weikersthal, L.; Goebell, P.J.; Lerchenmüller, C.; Zimmermann, U.; Bos, M.M.; Freier, W.; Schirrmacher-Memmel, S.; et al. SWITCH: a randomised, sequential, open-label study to evaluate the efficacy and safety of sorafenibsunitinib versus sunitinib-sorafenib in the treatment of metastatic renal cell cancer. Eur. Urol. 2015, 68, 837–847. [Google Scholar] [CrossRef] [Green Version]
- Sella, A.; Michaelson, M.D.; Matczak, E.; Simantov, R.; Lin, X.; Figlin, R.A. Heterogeneity of Patients With Intermediate-Prognosis Metastatic Renal Cell Carcinoma Treated With Sunitinib. Clin Genitourin Cancer 2017, 15, 291–299. [Google Scholar] [CrossRef]
- Tamada, S.; Iguchi, T.; Yasuda, S.; Kato, M.; Yamasaki, T.; Nakatani, T. The difference in the survival rate of patients with metastatic renal cell carcinoma in the intermediate-risk group of the Memorial Sloan Kettering Cancer Center criteria. Oncotarget. 2018, 9, 27752–27759. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, A.; Miyake, H.; Harada, K.I.; Inoue, T.A.; Fujisawa, M. Prognostic outcome in patients treated with tyrosine kinase inhibitors as first-line molecular-targeted therapy for metastatic renal cell carcinoma: Experience in real-world clinical practice in Japan. Mol. Clin. Oncol. 2015, 3, 601–606. [Google Scholar] [CrossRef]
- Melichar, B. Laboratory medicine and medical oncology: the tale of two Cinderellas. Clin. Chem. Lab. Med. 2013, 51, 99–112. [Google Scholar] [CrossRef]
- Ravaud, A.; Barrios, C.H.; Alekseev, B.; Tay, M.H.; Agarwala, S.S.; Yalcin, S.; Lin, C.C.; Roman, L.; Shkolnik, M.; Anak, O.; et al. RECORD-2: phase II randomized study of everolimus and bevacizumab versus interferon α-2a and bevacizumab as first-line therapy in patients with metastatic renal cell carcinoma. Ann. Oncol. 2015, 26, 1378–1384. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | MSKCC Risk Group | |||||
|---|---|---|---|---|---|---|
| Favourable | Intermediate | Poor | Intermediate | All Patients | ||
| One Risk Factor | Two Risk Factors | |||||
| n (%) | 806 (33.7) | 1450 (60.7) | 134 (5.6) | 969 (40.5) | 481 (20.1) | 2390 (100) |
| Gender, n (%) | ||||||
| Female | 225 (27.9) | 405 (27.9) | 37 (27.6) | 261 (26.9) | 144 (29.9) | 667 (27.9) |
| Male | 581 (72.1) | 1045 (72.1) | 97 (72.4) | 708 (73.1) | 337 (70.1) | 1723 (72.1) |
| Age at diagnosis (yr): median | 57.9 | 61.5 | 62.6 | 60.8 | 62.8 | 60.3 |
| Histology, n (%) | ||||||
| Clear cell carcinoma | 772 (95.8) | 1365 (94.1) | 125 (93.3) | 908 (93.7) | 457 (95.0) | 2262 (94.6) |
| Papillary carcinoma | 30 (3.7) | 72 (5.0) | 7 (5.3) | 53 (5.5) | 19 (4.0) | 109 (4.5) |
| Chromophobe carcinoma | 2 (0.3) | 6 (0.4) | 1 (0.8) | 5 (0.5) | 1 (0.2) | 9 (0.4) |
| Bellini duct carcinoma | 1 (0.1) | 5 (0.3) | 0 (0) | 2 (0.2) | 3 (0.6) | 6 (0.3) |
| Oncocytoma | 1 (0.1) | 1 (0.1) | 0 (0) | 1 (0.1) | 0 (0) | 2 (0.1) |
| Unknown | 0 (0) | 1 (0.1) | 1 (0.7) | 0 (0) | 1 (0.2) | 2 (0.1) |
| Stage at diagnosis, n (%) | ||||||
| I | 209 (25.9) | 139 (9.6) | 1 (0.7) | 117 (12.1) | 22 (4.6) | 349 (14.6) |
| II | 162 (20.1) | 144 (9.9) | 2 (1.5) | 119 (12.3) | 25 (5.2) | 308 (12.9) |
| III | 180 (22.3) | 251 (17.3) | 15 (11.2) | 176 (18.2) | 75 (15.6) | 446 (18.7) |
| IV | 110 (13.6) | 791 (54.6) | 112 (83.6) | 464 (47.9) | 327 (68.0) | 1013 (42.4) |
| Unknown | 145 (18.0) | 125 (8.6) | 4 (3.0) | 93 (9.6) | 32 (6.7) | 274 (11.5) |
| Primary tumour grade, n (%) | ||||||
| G1 | 76 (9.4) | 98 (6.8) | 8 (6.0) | 69 (7.1) | 29 (6.0) | 182 (7.6) |
| G2 | 342 (42.4) | 459 (31.7) | 45 (33.6) | 327 (33.7) | 132 (27.4) | 846 (35.4) |
| G3–4 | 219 (27.2) | 646 (44.6) | 63 (47.0) | 397 (41.0) | 249 (51.8) | 928 (38.8) |
| Unknown | 169 (21.0) | 247 (17.0) | 18 (13.4) | 176 (18.2) | 71 (14.8) | 434 (18.2) |
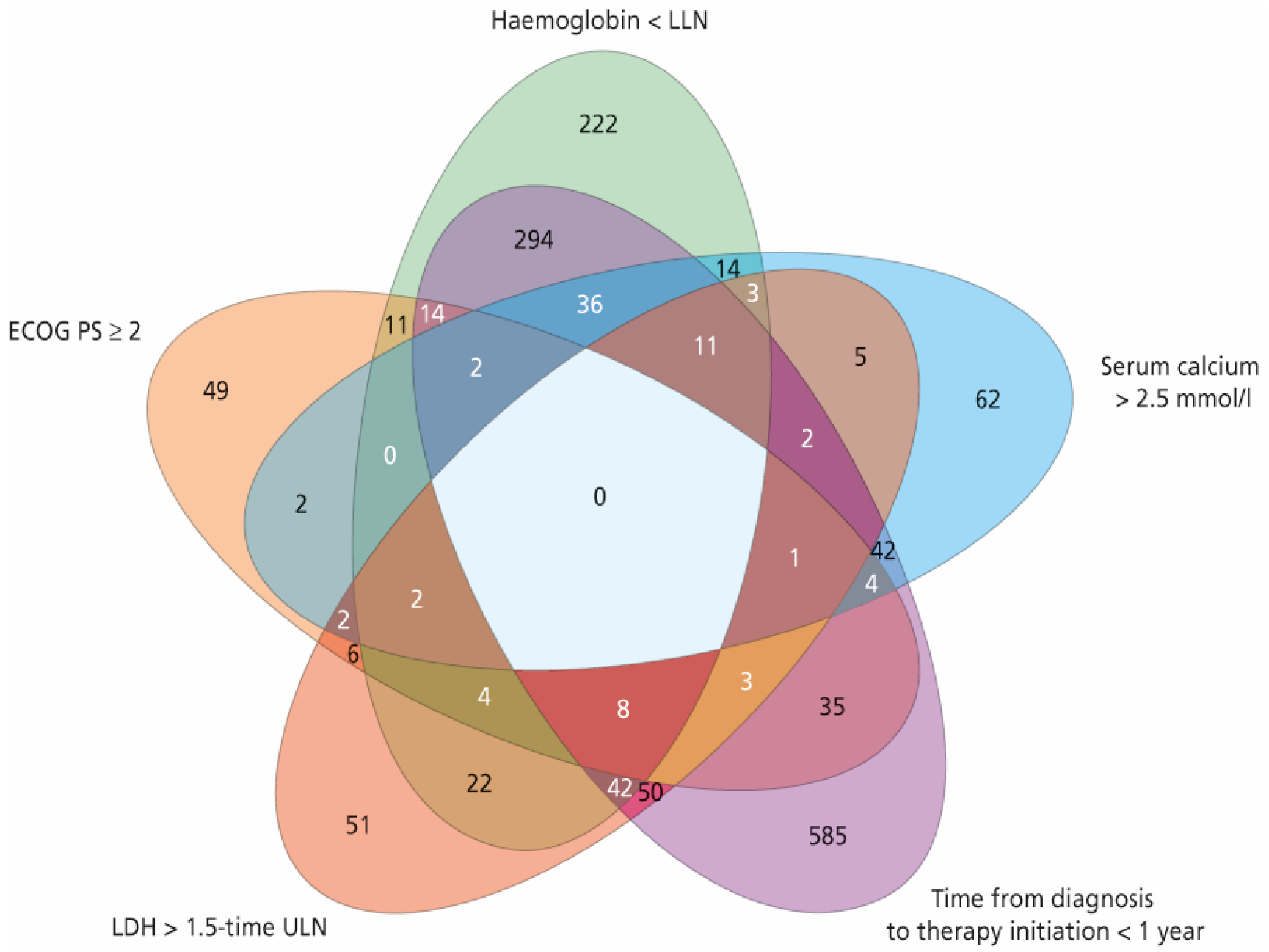
| MSKCC Risk Factors | ||||||
| ECOG PS 0–1, n (%) | 806 (100) | 1347 (92.9) | 94 (70.1) | 920 (94.9) | 427 (88.8) | 2247 (94.0) |
| ECOG PS ≥ 2, n (%) | 0 (0) | 103 (7.1) | 40 (29.9) | 49 (5.1) | 54 (11.2) | 143 (6.0) |
| Serum calcium ≤ 2.5 mmol/l, n (%) | 806 (100) | 1325 (91.4) | 71 (53.0) | 907 (93.6) | 418 (86.9) | 2202 (92.1) |
| Serum calcium > 2.5 mmol/l, n (%) | 0 (0) | 125 (8.6) | 63 (47.0) | 62 (6.4) | 63 (13.1) | 188 (7.9) |
| Haemoglobin normal, n (%) | 806 (100) | 887 (61.2) | 12 (9.0) | 747 (77.1) | 140 (29.1) | 1705 (71.3) |
| Haemoglobin < LLN, n (%) | 0 (0) | 563 (38.8) | 122 (91.0) | 222 (22.9) | 341 (70.9) | 685 (28.7) |
| Time from diagnosis to therapy initiation ≥ 1 year, n (%) | 806 (100) | 444 (30.6) | 11 (8.2) | 384 (39.6) | 60 (12.5) | 1261 (52.8) |
| Time from diagnosis to therapy initiation < 1 year, n (%) | 0 (0) | 1006 (69.4) | 123 (91.8) | 585 (60.4) | 421 (87.5) | 1129 (47.2) |
| LDH ≤ 1.5 time ULN, n (%) | 806 (100) | 1316 (90.8) | 56 (41.8) | 918 (94.7) | 398 (82.7) | 2178 (91.1) |
| LDH > 1.5 time ULN, n (%) | 0 (0) | 134 (9.2) | 78 (58.2) | 51 (5.3) | 83 (17.3) | 212 (8.9) |
| Outcomes | MSKCC Risk Group | |||||
|---|---|---|---|---|---|---|
| Favourable | Intermediate | Poor | Intermediate | All Patients | ||
| One Risk Factor | Two Risk Factors | |||||
| Objective Overall Response | ||||||
| n | 806 | 1450 | 134 | 969 | 481 | 2390 |
| Objective response rate (%) † | 33.0 | 24.1 | 13.4 | 26.7 | 18.7 | 26.5 |
| p-value < 0.001 | p-value = 0.001 | |||||
| Complete response (%) | 7.4 | 4.6 | 0.7 | 5.8 | 2.1 | 5.3 |
| Partial response (%) | 25.6 | 19.5 | 12.7 | 20.9 | 16.6 | 21.2 |
| Stable disease (%) | 35.1 | 32.9 | 18.7 | 33.7 | 31.2 | 32.8 |
| Progressive disease (%) | 15.9 | 24.0 | 39.6 | 22.7 | 26.6 | 22.1 |
| Not evaluable (%) | 16.0 | 19.0 | 28.4 | 16.8 | 23.5 | 18.5 |
| Overall Survival (OS) | ||||||
| n | 806 | 1450 | 134 | 969 | 481 | 2390 |
| Median survival (months; 95% CI) | 44.7 (40.9–50.5) | 24.1 (21.9–26.0) | 9.5 (7.2–14.1) | 28.2 (25.9–30.7) | 16.2 (14.5–20.2) | 28.5 (26.3–30.5) |
| p-value < 0.001 | p-value < 0.001 | - | ||||
| 1-year survival (%; 95% CI) | 85.0 (82.4–87.6) | 69.1 (66.6–71.7) | 44.3 (35.0–53.7) | 74.3 (71.4–77.2) | 58.0 (53.1–62.9) | 73.3 (71.4–75.2) |
| 3-year survival (%; 95 %CI) | 57.3 (53.4–61.3) | 37.1 (34.1–40.1) | 9.6 (3.1–16.2) | 42.0 (38.3–45.7) | 26.3 (21.4–31.2) | 42.9 (40.5–45.2) |
| 5-year survival (%; 95% CI) | 35.6 (31.2–40.1) | 23.4 (20.4–26.4) | 3.2 (0.0–8.8) | 26.5 (22.7–30.3) | 16.5 (11.8–21.2) | 26.8 (24.3–29.2) |
| 10-year survival (%; 95% CI) | 13.5 (8.1–18.9) | 13.8 (10.5–17.0) | 0 (0.0–0.0) | 15.1 (11.0–19.1) | 0 (0.0–0.0) | 12.7 (9.8–15.7) |
| Progression-Free Survival (PFS) | ||||||
| n | 806 | 1450 | 134 | 969 | 481 | 2390 |
| Median survival (months; 95% CI) | 17.0 (15.4–18.8) | 9.0 (8.3–9.5) | 4.5 (3.9–6.1) | 10.1 (9.4–11.4) | 6.2 (5.5–7.5) | 10.6 (9.9–11.5) |
| p-value < 0.001 | p-value < 0.001 | - | ||||
| 1-year survival (%; 95% CI) | 61.8 (58.3–65.3) | 40.7 (38.0–43.4) | 20.8 (13.1–28.5) | 45.1 (41.8–48.4) | 31.6 (27.1–36.1) | 46.9 (44.7–49.0) |
| 3-year survival (%; 95%CI) | 25.1 (21.7–28.5) | 13.0 (11.0–15.1) | 1.8 (0.0–5.1) | 15.9 (13.2–18.6) | 7.0 (4.2–9.7) | 16.6 (14.9–18.4) |
| 5-year survival (%; 95% CI) | 10.4 (7.7–13.2) | 8.0 (6.2–9.8) | 1.8 (0.0–5.1) | 9.7 (7.3–12.0) | 4.5 (2.1–6.9) | 8.4 (7.0–9.9) |
| 10-year survival (%; 95% CI) | 3.7 (1.2–6.2) | 0 (0.0–0.0) | 0 (0.0–0.0) | 0 (0.0–0.0) | 0 (0.0–0.0) | 3.7 (2.1–5.3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiala, O.; Finek, J.; Poprach, A.; Melichar, B.; Kopecký, J.; Zemanova, M.; Kopeckova, K.; Mlcoch, T.; Dolezal, T.; Capkova, L.; et al. Outcomes According to MSKCC Risk Score with Focus on the Intermediate-Risk Group in Metastatic Renal Cell Carcinoma Patients Treated with First-Line Sunitinib: A Retrospective Analysis of 2390 Patients. Cancers 2020, 12, 808. https://doi.org/10.3390/cancers12040808
Fiala O, Finek J, Poprach A, Melichar B, Kopecký J, Zemanova M, Kopeckova K, Mlcoch T, Dolezal T, Capkova L, et al. Outcomes According to MSKCC Risk Score with Focus on the Intermediate-Risk Group in Metastatic Renal Cell Carcinoma Patients Treated with First-Line Sunitinib: A Retrospective Analysis of 2390 Patients. Cancers. 2020; 12(4):808. https://doi.org/10.3390/cancers12040808
Chicago/Turabian StyleFiala, Ondrej, Jindrich Finek, Alexandr Poprach, Bohuslav Melichar, Jindrich Kopecký, Milada Zemanova, Katerina Kopeckova, Tomas Mlcoch, Tomas Dolezal, Lenka Capkova, and et al. 2020. "Outcomes According to MSKCC Risk Score with Focus on the Intermediate-Risk Group in Metastatic Renal Cell Carcinoma Patients Treated with First-Line Sunitinib: A Retrospective Analysis of 2390 Patients" Cancers 12, no. 4: 808. https://doi.org/10.3390/cancers12040808
APA StyleFiala, O., Finek, J., Poprach, A., Melichar, B., Kopecký, J., Zemanova, M., Kopeckova, K., Mlcoch, T., Dolezal, T., Capkova, L., & Buchler, T. (2020). Outcomes According to MSKCC Risk Score with Focus on the Intermediate-Risk Group in Metastatic Renal Cell Carcinoma Patients Treated with First-Line Sunitinib: A Retrospective Analysis of 2390 Patients. Cancers, 12(4), 808. https://doi.org/10.3390/cancers12040808