Shifting the Immune-Suppressive to Predominant Immune-Stimulatory Radiation Effects by SBRT-PArtial Tumor Irradiation Targeting HYpoxic Segment (SBRT-PATHY)

 , ,
, ,  ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Translational Oncology Research
2.1. Partial Tumor Irradiation
2.2. Preclinical Findings
2.3. Translation of the Preclinical Findings to the Clinic
3. Clinical Outcomes
4. Immunohistochemistry and Gene-Expression Findings Following SBRT-PATHY
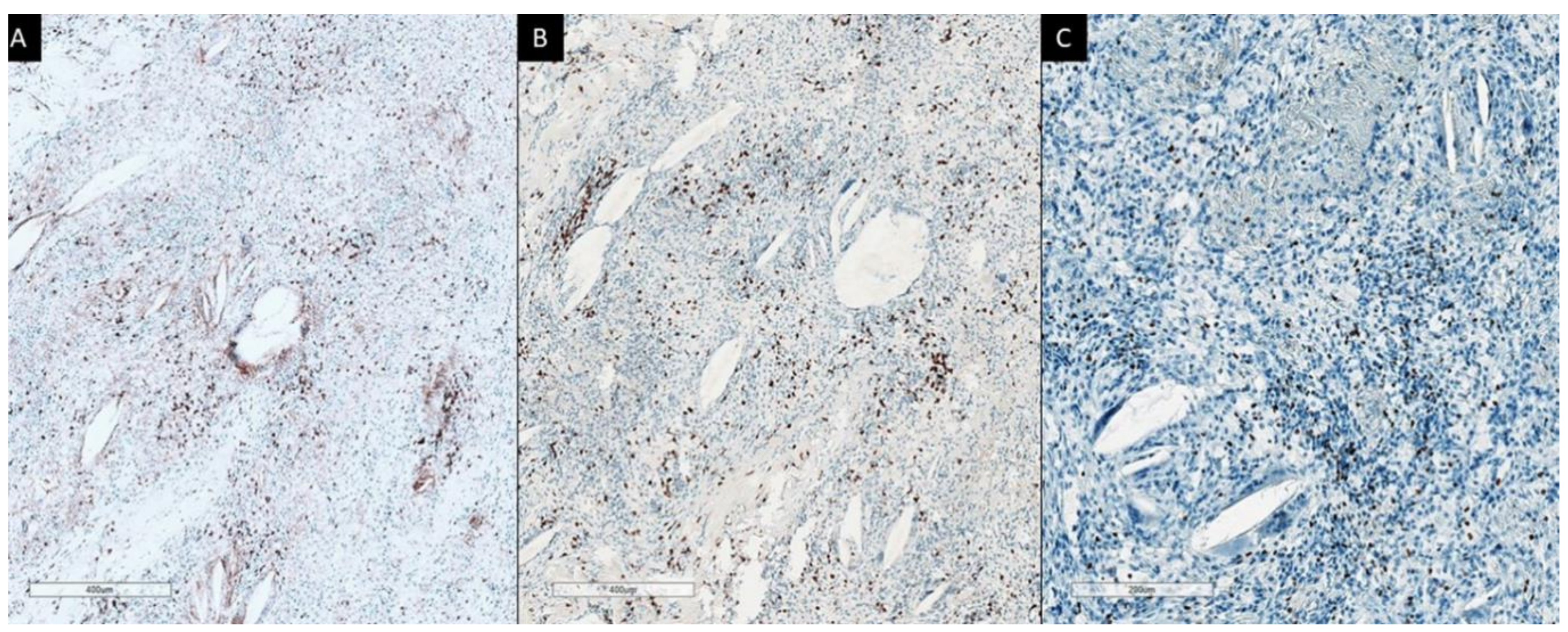
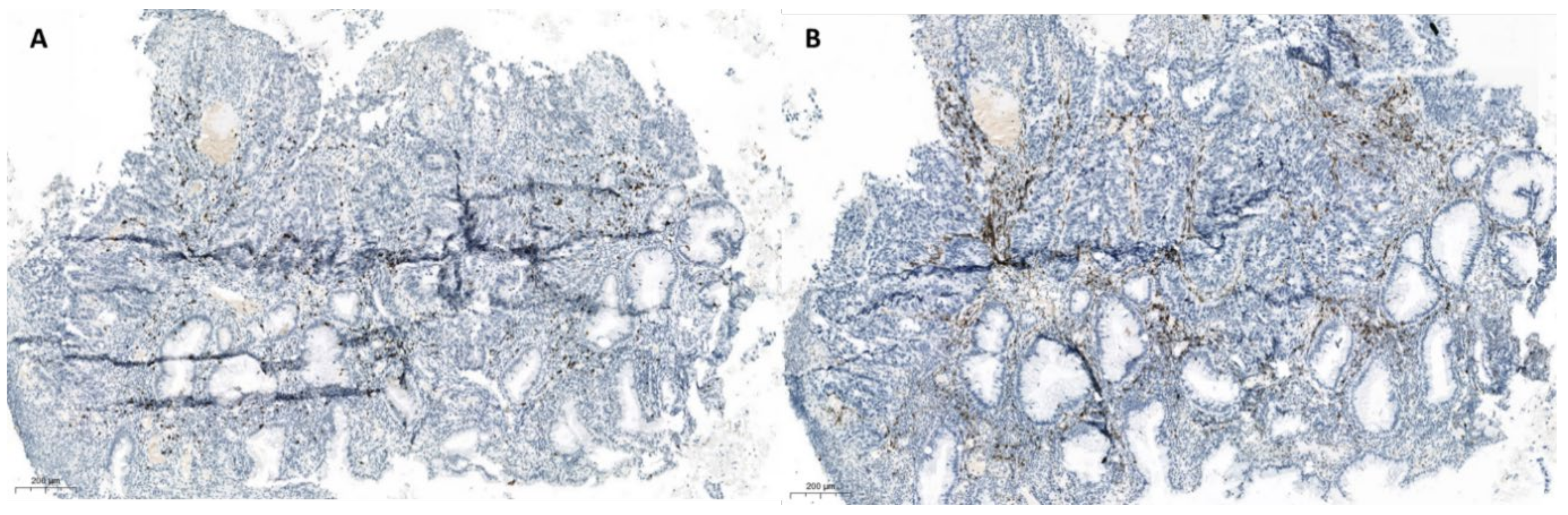
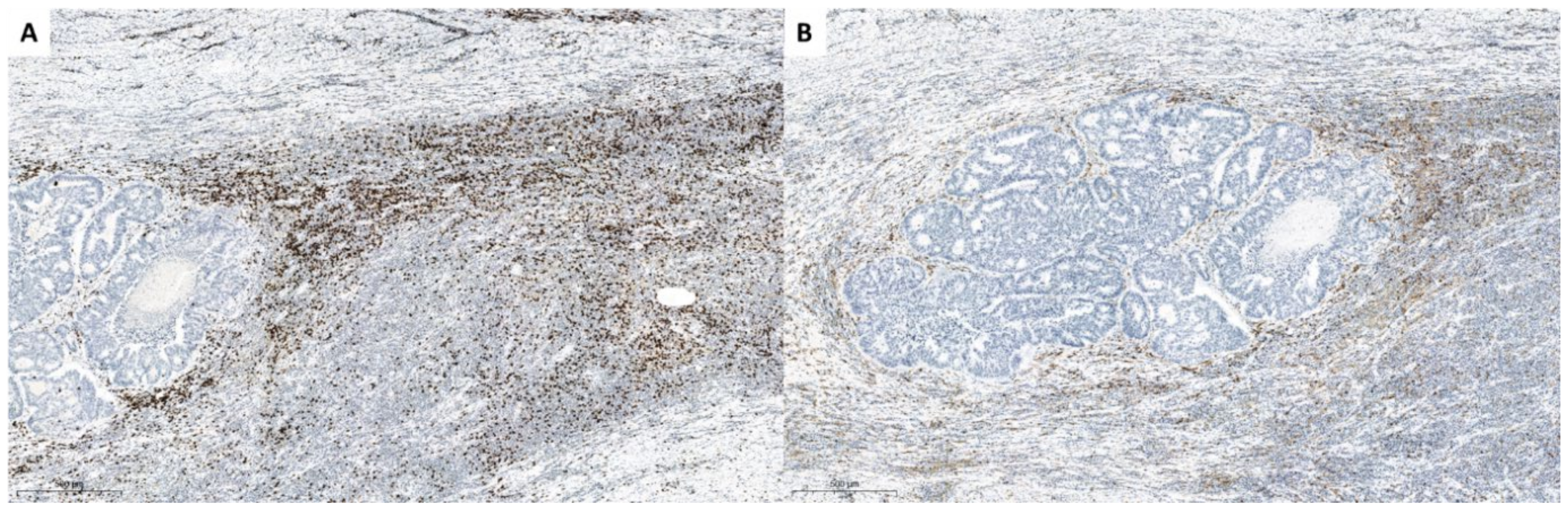
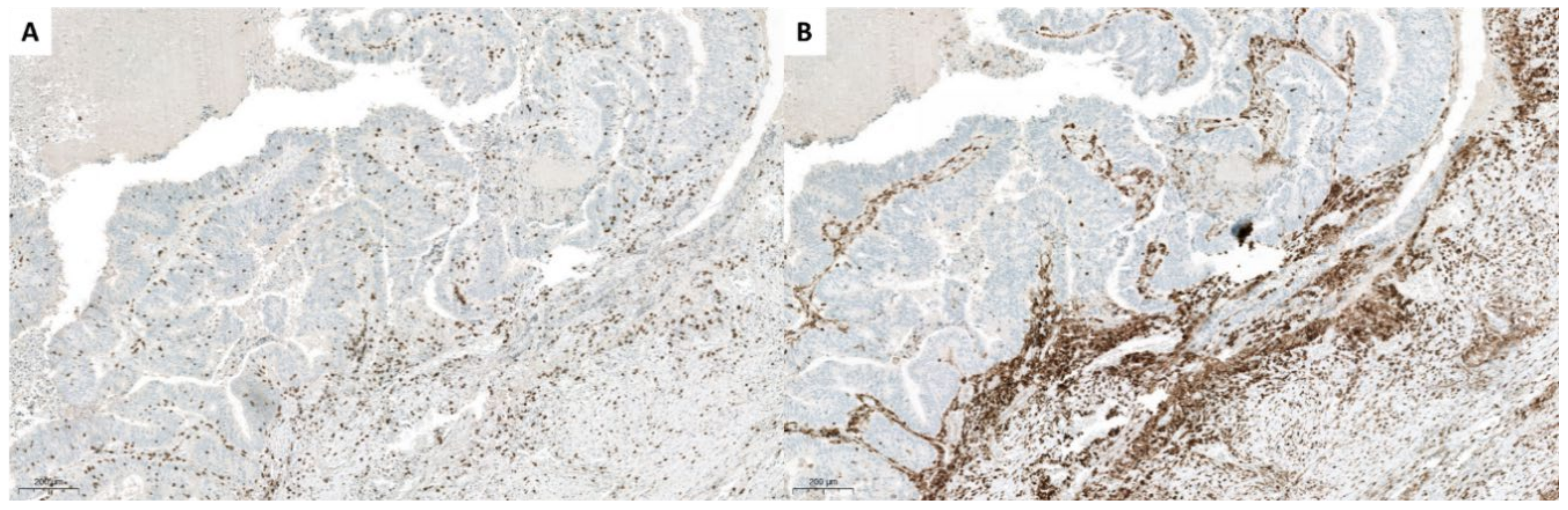
4.1. Immunohistochemistry
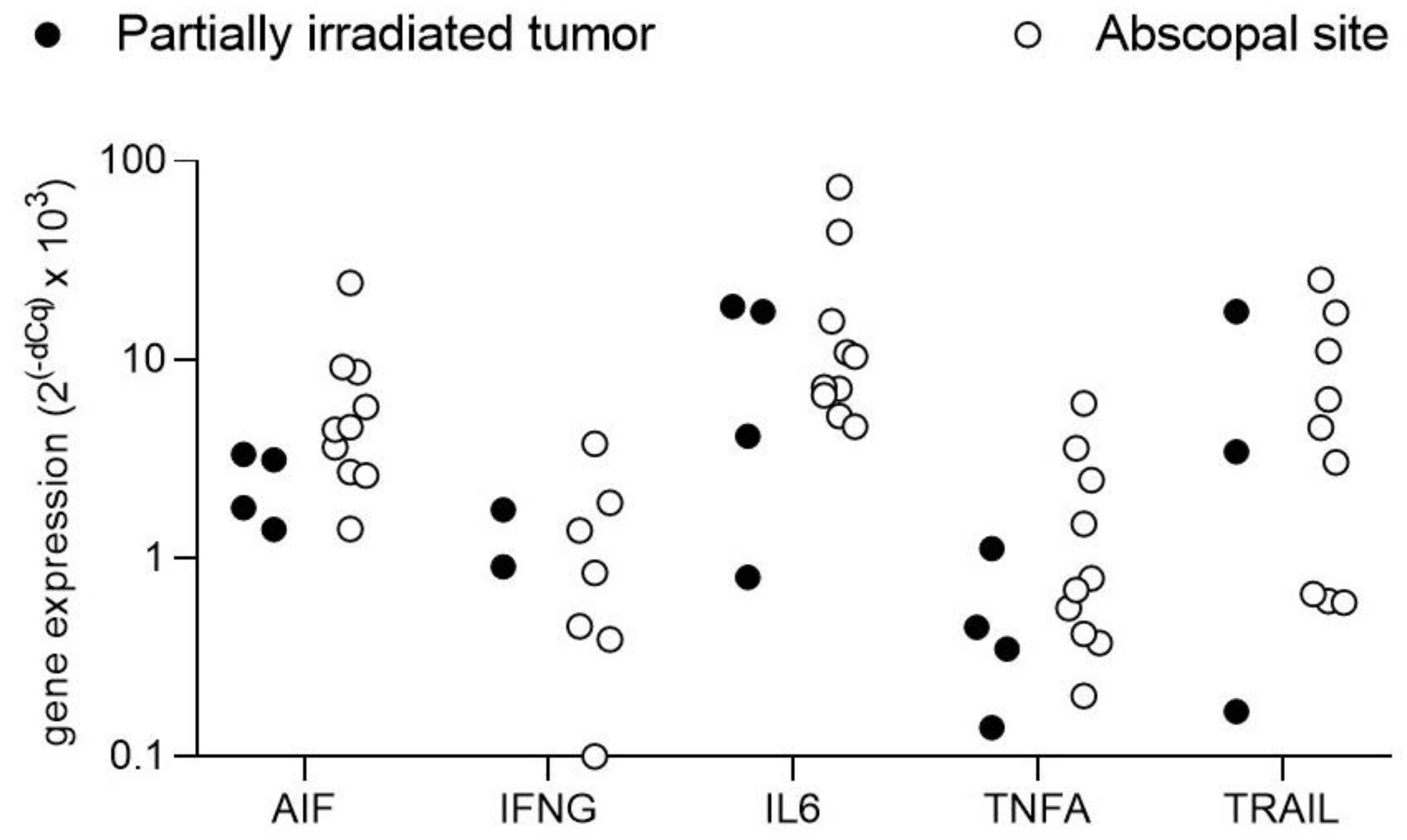
4.2. Transcript Expression of Cell Death Related Signaling Molecules
5. Why Timing of SBRT-PATHY May Be Important to Break Tumor Tolerance
6. Discussion
7. Conclusions
8. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Milano, M.T.; Katz, A.W.; Zhang, H.; Okunieff, P. Oligometastases Treated With Stereotactic Body Radiotherapy: Long-Term Follow-Up of Prospective Study. Int. J. Radiat. Oncol. 2012, 83, 878–886. [Google Scholar] [CrossRef] [PubMed]
- Palma, A.D.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in pa-tients with oligometastatic cancers (SABR-COMET): A randomised, phase 2, open-label trial. Lancet 2019, 18, 2051–2058. [Google Scholar] [CrossRef]
- Fyles, A.W.; Milosevic, M.; Wong, R.; Kavanagh, M.-C.; Pintilie, M.; Sun, A.; Chapman, W.; Levin, W.; Manchul, L.; Keane, T.J.; et al. Oxygenation predicts radiation response and survival in patients with cervix cancer. Radiother. Oncol. 1998, 48, 149–156. [Google Scholar] [CrossRef]
- Tubin, S.; Yan, W.; Mourad, W.F.; Fossati, P.; Khan, M.K. The future of radiation-induced abscopal response: Beyond conventional radiotherapy approaches. Futur. Oncol. 2020, 16, 1137–1151. [Google Scholar] [CrossRef] [PubMed]
- Ludgate, C.M. Optimizing Cancer Treatments to Induce an Acute Immune Response: Radiation Abscopal Effects, PAMPs, and DAMPs. Clin. Cancer Res. 2012, 18, 4522–4525. [Google Scholar] [CrossRef] [Green Version]
- Reits, E.A.; Hodge, J.W.; Herberts, C.A.; Groothuis, T.A.; Chakraborty, M.; Wansley, E.K.; Camphausen, K.; Luiten, R.M.; De Ru, A.H.; Neijssen, J.; et al. Radiation modulates the peptide repertoire, enhances MHC class I expression, and induces successful antitumor immunotherapy. J. Exp. Med. 2006, 203, 1259–1271. [Google Scholar] [CrossRef]
- Merrick, A.; Errington, F.; Milward, K.; O’Donnell, D.; Harrington, K.; Bateman, A.; Pandha, H.; Vile, R.; Morrison, E.; Selby, P.; et al. Immunosuppressive effects of radiation on human dendritic cells: Reduced IL-12 production on activation and impairment of naïve T-cell priming. Br. J. Cancer 2005, 92, 1450–1458. [Google Scholar] [CrossRef]
- MacLennan, I.C.; Kay, H.E. Analysis of treatment in childhood leukemia. IV. The critical association between dose fractionation and immunosuppression induced by cranial irradiation. Cancer 1978, 41, 108–111. [Google Scholar]
- Ladbury, C.J.; Rusthoven, C.G.; Camidge, D.R.; Kavanagh, B.D.; Nath, S.K. Impact of Radiation Dose to the Host Immune System on Tumor Control and Survival for Stage III Non-Small Cell Lung Cancer Treated with Definitive Radiation Therapy. Int. J. Radiat. Oncol. 2019, 105, 346–355. [Google Scholar] [CrossRef]
- Wirsdörfer, F.; Jendrossek, V. The Role of Lymphocytes in Radiotherapy-Induced Adverse Late Effects in the Lung. Front. Immunol. 2016, 7. [Google Scholar] [CrossRef] [Green Version]
- Routman, D.M.; Garant, A.; Lester, S.C.; Day, C.N.; Harmsen, W.S.; Sanheuza, C.T.; Yoon, H.H.; Neben-Wittich, M.A.; Martenson, J.A.; Haddock, M.G.; et al. A comparison of grade 4 Lymphopenia with proton versus photon radiation ther-apy for esophageal Cancer. Adv. Radiat. Oncol. 2019, 4, 63–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, B.I.; Metes, D.M. Peripheral blood lymphocyte depletion after hepatic arterial 90Yttrium microsphere therapy for hepato-cellular carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1179–1184. [Google Scholar] [CrossRef] [PubMed]
- Grossman, S.A.; Ellsworth, S.; Campian, J.; Wild, A.T.; Herman, J.M.; Laheru, D.; Brock, M.; Balmanoukian, A.; Ye, X. Survival in patients with severe Lymphopenia following treatment with radia-tion and chemotherapy for newly diagnosed solid tumors. J. Natl. Compr. Canc. Netw. 2015, 13, 1225–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afghahi, A.; Mathur, M.; Seto, T.; Desai, M.; Kenkare, P.; Das, K.C.H.K.; Thompson, C.A.; Luft, H.S.; Yu, P.P.; Gomez, S.L.; et al. Lymphopenia after adjuvant radiotherapy (RT) to predict poor survival in tri-ple-negative breast cancer (TNBC). J. Clin. Oncol. 2015, 33 (Suppl. S15), 1069. [Google Scholar] [CrossRef]
- Wild, A.T.; Ye, X.; Ellsworth, S.G.; Smith, J.A.; Narang, A.K.; Garg, T.; Campian, J.; Laheru, D.A.; Zheng, L.; Wolfgang, C.L.; et al. The Association Between Chemoradiation-related Lymphopenia and Clinical Outcomes in Patients with Locally Advanced Pancreatic Adenocarcinoma. Am. J. Clin. Oncol. 2015, 38, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mole, R.J. Whole body irradiation—Radiology or medicine? Br. J. Radiol. 1953, 26, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Desouky, O.; Ding, N.; Zhou, G. Targeted and non-targeted effects of ionizing radiation. J. Radiat. Res. Appl. Sci. 2015, 8, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Dagoglu, N.; Karaman, S.; Caglar, H.B.; Oral, E.N. Abscopal Effect of Radiotherapy in the Immunotherapy Era: Systematic Review of Reported Cases. Cureus 2019, 11, 4103. [Google Scholar] [CrossRef] [Green Version]
- Kaminski, J.M.; Shinohara, E.; Summers, J.B.; Niermann, K.J.; Morimoto, A.; Brousal, J. The controversial abscopal effect. Cancer Treat. Rev. 2005, 31, 159–172. [Google Scholar] [CrossRef]
- Nagasawa, H.; Little, J.B. Induction of sister chromatid exchanges by extremely low doses of alpha-particles. Cancer Res. 1992, 52, 6394–6396. [Google Scholar]
- Tubin, S.; Raunik, W. Hunting for abscopal and bystander effects: Clinical exploitation of non-targeted effects induced by partial high-single-dose irradiation of the hypoxic tumour segment in oligometastatic patients. Acta Oncol. 2017, 56, 1333–1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billena, C.; Khan, A.J. A Current Review of Spatial Fractionation: Back to the Future? Int. J. Radiat. Oncol. 2019, 104, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Yan, W.; Khan, M.K.; Wu, X.; Simone, C.B.; Fan, J.; Gressen, E.; Zhang, X.; Limoli, C.L.; Bahig, H.; Tubin, S.; et al. Spatially fractionated radiation therapy: History, present and the future. Clin. Transl. Radiat. Oncol. 2020, 20, 30–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Ahmed, M.M.; Wright, J.; Gupta, S.; Pollack, A. On Modern Technical Approaches of Three-Dimensional High-Dose Lattice Radiotherapy (Lrt). Cureus 2010, 2, 9. [Google Scholar] [CrossRef] [Green Version]
- Asur, R.; Butterworth, K.T.; Penagaricano, J.A.; Prise, K.M.; Griffin, R.J. High dose bystander effects in spatially fractionated radiation therapy. Cancer Lett. 2015, 356, 52–57. [Google Scholar] [CrossRef] [Green Version]
- Kohler, H. Zur roentiefentherapie mit massendosen MMW. Fortschr. Med. 1909, 56, 2314–2316. [Google Scholar]
- Sharif, S.F.; Hariri, R.J.; Chang, V.A.; Barie, P.S.; Wang, R.S.; Ghajar, J.B. Human astrocyte production of tumor necrosis factor-alpha, interleukin-1 beta and interleukin-6 following exposure to lipopolysaccharide endotoxin. Neurol. Res. 1993, 15, 109–116. [Google Scholar] [CrossRef]
- Ivanov, V.N.; Hei, T.K. A role for TRAIL/TRAIL-R2 in radiation-induced apoptosis and radiation-induced bystander response of human neural stem cells. Apoptosis 2014, 19, 399–413. [Google Scholar] [CrossRef] [Green Version]
- Sathishkumar, S.; Dey, S.; Meigooni, A.S.; Regine, W.F.; Kudrimoti, M.S.; Ahmed, M.M.; Mohiuddin, M. The impact of TNF-alpha induction on therapeutic efficacy following high dose spatially fractionated (GRID) radiation. Technol. Cancer Res. Treat. 2002, 1, 141–147. [Google Scholar] [CrossRef] [Green Version]
- Shareef, M.M.; Cui, N.; Burikhanov, R.; Gupta, S.; Satishkumar, S.; Shajahan, S.; Mohiuddin, M.; Rangnekar, V.M.; Ahmed, M.M. Role of tumor necrosis factor-alpha and TRAIL in high-dose radiation-induced by-stander signaling in lung adenocarcinoma. Cancer Res. 2007, 67, 11811–11820. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.; Shareef, M.; Gupta, S.; Zagurovskaya-Sultanov, M.; Kadhim, M.; Mohiuddin, M.; Ahmed, M. Potential Utilization of Bystander/Abscopal-Mediated Signal Transduction Events in the Treatment of Solid Tumors. Curr. Signal. Transduct. Ther. 2007, 2, 129–143. [Google Scholar] [CrossRef]
- Kanagavelu, S.; Gupta, S.; Wu, X.; Philip, S.; Wattenberg, M.M.; Hodge, J.W.; Couto, M.D.; Chung, K.D.; Ahmed, M.M. In Vivo Effects of Lattice Radiation Therapy on Local and Distant Lung Cancer: Potential Role of Immunomodulation. Radiat. Res. 2014, 182, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Markovsky, E.; Budhu, S.; Samstein, R.M.; Li, H.; Russell, J.; Zhang, Z.; Drill, E.; Bodden, C.; Chen, Q.; Powell, S.N.; et al. An Antitumor Immune Response Is Evoked by Partial-Volume Single-Dose Radiation in 2 Murine Models. Int. J. Radiat. Oncol. 2019, 103, 697–708. [Google Scholar] [CrossRef]
- Brizel, D.M.; Sibley, G.S.; Prosnitz, L.R.; Scher, R.L.; Dewhirst, M.W. Tumor hypoxia adversely affects the prognosis of carcinoma of the head and neck. Int. J. Radiat. Oncol. 1997, 38, 285–289. [Google Scholar] [CrossRef]
- Mohiuddin, M.; Fujita, M.; Regine, W.F.; Megooni, A.S.; Ibbott, G.S.; Ahmed, M.M. High-dose spatially-fractionated radiation (GRID): A new paradigm in the man-agement of advanced cancers. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 721–727. [Google Scholar] [CrossRef]
- Tubin, S.; Ahmed, M.M.; Gupta, S. Radiation and hypoxia-induced non-targeted effects in normoxic and hypoxic conditions in human lung cancer cells. Int. J. Radiat. Biol. 2018, 94, 199–211. [Google Scholar] [CrossRef]
- Schaue, D.; Ratikan, J.A.; Iwamoto, K.S.; McBride, W.H. Maximizing Tumor Immunity with Fractionated Radiation. Int. J. Radiat. Oncol. 2012, 83, 1306–1310. [Google Scholar] [CrossRef] [Green Version]
- Vanpouille-Box, C.; Formenti, S.C.; DeMaria, S. TREX1 dictates the immune fate of irradiated cancer cells. OncoImmunology 2017, 6, e1339857. [Google Scholar] [CrossRef] [Green Version]
- Tubin, S.; Khan, K.M.; Salerno, G.; Mourad, W.F.; Yan, W.; Jeremic, B. Mono-institutional Phase II study of innovative stereotactic body radiotherapy targeting partial tumor hypoxic (SBRT-PATHY) clonogenic cells in unresectable bulky non-small cell lung cancer: Profound non tar-geted effects by sparing peri-tumoral immune microenvironment. Radiat. Oncol. 2019, 14, 212. [Google Scholar]
- Massaccesi, M.; DiNapoli, N.; Boldrini, L.; Cervone, L.; Placidi, L.; Stimato, G.; Azario, L.; Frascino, V.; Manfrida, S.; Mattiucci, G.; et al. Re-Treatment of Recurrent Bulky Lesions with High Single Dose Partial Irradiation Targeting the Hypoxic Tumor Segment (PITH): A Case Series. Int. J. Radiat. Oncol. 2019, 105, E578. [Google Scholar] [CrossRef]
- Tubin, S.; Popper, H.; Brcic, L. Novel stereotactic body radiation therapy (SBRT)-based partial tumor irradiation targeting hypoxic segment of bulky tumors (SBRT-PATHY): Improvement of the radiotherapy outcome by exploiting the bystander and abscopal effects. Radiat. Oncol. 2019, 14, 21. [Google Scholar] [CrossRef] [PubMed]
- Tubin, S.; Fossati, P.; Georg, P.; Stock, M.; Ashdown, M.; Mirzaei, S.; Andrzejewski, P.; Galalae, R.M.; Lütgendorf-Caucig, C.; Hug, E.; et al. Particle-based partial tumor irradiation targeting hypoxic segment and sparing the peritu-moral immune microenvironment for unresectable bulky tumors. Unpublished work. 2003. [Google Scholar]
- Tubin, S.; Ashdown, M.L.; Jeremic, B. Time-synchronized immune-guided SBRT partial bulky tumor irradiation targeting hypoxic segment while sparing the peritumoral immune microenvironment. Radiat. Oncol. 2019, 14, 1–7. [Google Scholar] [CrossRef]
- Tubin, S.; Ashdown, M.; Raunik, W. Clinical Exploration of the Non-Targeted Effects of SBRT in Oligometastatic Patients with Bulky Tumors Treated by Partial High-Dose Irradiation of Hypoxic Tumor Segment: Phase I Proof of Principle Trial. Available online: https://clinicaltrials.gov/ct2/results?cond=&term=Tubin&cntry=AT&state=&city=&dist= (accessed on 19 November 2019).
- Shohan, J. Some Theoretical Considerations on the Present Status of Roentgen Therapy. N. Engl. J. Med. 1916, 175, 321–327. [Google Scholar] [CrossRef]
- Hellström, K.E.; Hellström, I. Evidence that tumor antigens enhance tumor growth in vivo by interacting with a radiosensitive (suppressor?) cell population. Proc. Natl. Acad. Sci. USA 1978, 75, 436–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellström, K.E.; Hellström, I.; Kant, J.A.; Tamerius, J.D. Regression and inhibition of sarcoma growth by interference with a radio-sensitive T-cell population. J. Exp. Med. 1978, 148, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Slone, H.B.; Peters, L.J.; Milas, L. Effect of Host Immune Capability on Radiocurability and Subsequent Transplantability of a Murine Fibrosarcoma2. J. Natl. Cancer Inst. 1979, 63, 1229–1235. [Google Scholar] [CrossRef]
- Awwad, M.; North, R.J. Sublethal, whole-body ionizing irradiation can be tumor promotive or tumor destructive depending on the stage of development of underlying antitumor immunity. Cancer Immunol. Immunother. 1988, 26, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Gajewski, T.F.; Meng, Y.; Blank, C.; Brown, I.; Kacha, A.; Kline, J.; Harlin, H. Immune resistance orchestrated by the tumor microenvironment. Immunol. Rev. 2006, 213, 131–145. [Google Scholar] [CrossRef]
- Fujimura, T.; Kambayashi, Y.; Aiba, S. Crosstalk between regulatory T cells (Tregs) and myeloid derived suppressor cells (MDSCs) during melanoma growth. OncoImmunology 2012, 1, 1433–1434. [Google Scholar] [CrossRef] [Green Version]
- Arenas-Ramirez, N.; Woytschak, J.; Boyman, O. Interleukin-2: Biology, Design and Application. Trends Immunol. 2015, 36, 763–777. [Google Scholar] [CrossRef] [Green Version]
- Jiang, T.; Zhou, C.; Ren, S. Role of IL-2 in cancer immunotherapy. OncoImmunology 2016, 5, e1163462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.J.; Ashkar, A.A. The Dual Nature of Type I and Type II Interferons. Front. Immunol. 2018, 9, 2061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bocci, V. Interleukins. Clin. Pharm. 1991, 21, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Busse, D.; De La Rosa, M.; Hobiger, K.; Thurley, K.; Flossdorf, M.; Scheffold, A.; Höfer, T. Competing feedback loops shape IL-2 signaling between helper and regulatory T lymphocytes in cellular microenvironments. Proc. Natl. Acad. Sci. USA 2010, 107, 3058–3063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coventry, B.J.; Ashdown, M.L.; Quinn, M.A.; Markovic, S.N.; Yatomi-Clarke, S.L.; Robinson, A.P. CRP identifies homeostatic immune oscillations in cancer patients: A potential treatment targeting tool? J. Transl. Med. 2009, 7, 102–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leontovich, A.A.; Alexey, A.L. Fluctuation of systemic immunity in melanoma and implications for timing of therapy. Front. Biosci. 2012, 958–975. [Google Scholar] [CrossRef] [Green Version]
- Leontovich, A.A.; Dronca, R.S.; Nevala, W.K.; Thompson, M.A.; Kottschade, L.A.; Ivanov, L.V.; Markovic, S.N. Effect of the lymphocyte-to-monocyte ratio on the clinical outcome of chemotherapy administration in advanced melanoma patients. Melanoma Res. 2017, 27, 32–42. [Google Scholar] [CrossRef]
- Idzko, M.; Ferrari, D.; Eltzschig, H.K. Nucleotide signalling during inflammation. Nat. Cell Biol. 2014, 509, 310–317. [Google Scholar] [CrossRef] [Green Version]
- Galluzzi, L.; Vitale, I.; Warren, S.; Adjemian, S.; Agostinis, P.; Martinez, A.B.; Chan, T.A.; Coukos, G.; DeMaria, S.; Deutsch, E.; et al. Consensus guidelines for the definition, detection and interpretation of immunogenic cell death. J. Immunother. Cancer 2020, 8, e000337. [Google Scholar] [CrossRef] [Green Version]
- Ashrafizadeh, M.; Farhood, B.; Musa, A.E.; Taeb, S.; Najafi, M. Damage-associated molecular patterns in tumor radiotherapy. Int. Immunopharmacol. 2020, 86, 106761. [Google Scholar] [CrossRef]
- Park, B.; Yee, C.; Lee, K.-M. The Effect of Radiation on the Immune Response to Cancers. Int. J. Mol. Sci. 2014, 15, 927–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalbasi, A.; June, C.H.; Haas, N.; Vapiwala, N. Radiation and immunotherapy: A synergistic combination. J. Clin. Investig. 2013, 123, 2756–2763. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Ruiz, M.E.; Vanpouille-Box, C.; Melero, I.; Formenti, S.C.; DeMaria, S. Immunological Mechanisms Responsible for Radiation-Induced Abscopal Effect. Trends Immunol. 2018, 39, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Wennerberg, E.; Lhuillier, C.; Vanpouille-Box, C.; Pilones, K.A.; García-Martínez, E.; Rudqvist, N.-P.; Formenti, S.C.; DeMaria, S. Barriers to Radiation-Induced In Situ Tumor Vaccination. Front. Immunol. 2017, 8, 229. [Google Scholar] [CrossRef]
- Gooden, M.J.; de Bock, G.H.; Leffers, N.; Daemen, T.; Nijman, H.W. The prognostic influence of tumour-infiltrating lymphocytes in cancer: A systemat-ic review with metaanalysis. Br. J. Cancer 2011, 105, 93–103. [Google Scholar] [CrossRef] [Green Version]
- Fridman, W.H.; Galon, J.; Pagès, F.; Tartour, E.; Sautès-Fridman, C.; Kroemer, G. Prognostic and Predictive Impact of Intra- and Peritumoral Immune Infiltrates. Cancer Res. 2011, 71, 5601–5605. [Google Scholar] [CrossRef] [Green Version]
- Laghi, L.; Bianchi, P.; Miranda, E.; Balladore, E.; Pacetti, V.; Grizzi, F.; Allavena, P.; Torri, V.; Repici, A.; Santoro, A.; et al. CD3+ cells at the invasive margin of deeply invading (pT3–T4) colorectal cancer and risk of post-surgical metastasis: A longitudinal study. Lancet Oncol. 2009, 10, 877–884. [Google Scholar] [CrossRef]
- Dieci, M.V.; Criscitiello, C.; Goubar, A.; Viale, G.; Conte, P.; Guarneri, V.; Ficarra, G.; Mathieu, M.C.; Delaloge, S.; Curigliano, G.; et al. Prognostic value of tumor-infiltrating lymphocytes on residual disease after pri-mary chemotherapy for triple-negative breast cancer: A retrospective multicenter study. Ann. Oncol. 2014, 25, 611–618. [Google Scholar] [CrossRef]
- Horne, Z.D.; Jack, R.; Gray, Z.T.; Siegfried, J.M.; Wilson, D.O.; Yousem, S.A.; Nason, K.S.; Landreneau, R.J.; Luketich, J.D.; Schuchert, M.J. Increased levels of tumor-infiltrating lymphocytes are associated with improved recur-rence-free survival in stage 1A non-small-cell lung cancer. J. Surg. Res. 2011, 171, 1–5. [Google Scholar] [CrossRef]
- Schumacher, K.; Haensch, W.; Roefzaad, C.; Schlag, P.M. Prognostic significance of activated CD8 (+) T cell infiltrations within esoph-ageal carcinomas. Cancer Res. 2001, 61, 3932–3936. [Google Scholar]
- Wahlin, B.E.; Sander, B.; Christensson, B.; Kimby, E.; Weitzel, J.N.; Buys, S.S.; Sherman, W.H.; Daniels, A.M.; Ursin, G.; Daniels, J.R.; et al. CD8+ T-Cell Content in Diagnostic Lymph Nodes Measured by Flow Cytometry Is a Predictor of Survival in Follicular Lymphoma. Clin. Cancer Res. 2007, 13, 388–397. [Google Scholar] [CrossRef] [Green Version]
- Delavallée, L.; Cabon, L.; Galán-Malo, P.; Lorenzo, H.K.; Susin, S.A. AIF-mediated caspase-independent necroptosis: A new chance for targeted therapeutics. IUBMB Life 2011, 63, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Kotredes, K.P.; Gamero, A.M. Interferons as Inducers of Apoptosis in Malignant Cells. J. Interf. Cytokine Res. 2013, 33, 162–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Du, F.; Wang, X. TNF-α Induces Two Distinct Caspase-8 Activation Pathways. Cell 2008, 133, 693–703. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; El-Deiry, W.S. TRAIL and apoptosis induction by TNF-family death receptors. Oncogene 2003, 22, 8628–8633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regis, G.; Icardi, L.; Conti, L.; Chiarle, R.; Piva, R.; Giovarelli, M.; Poli, V.; Novelli, F. IL-6, but not IFN-γ, triggers apoptosis and inhibits in vivo growth of human malignant T cells on STAT3 silencing. Leuk. 2009, 23, 2102–2108. [Google Scholar] [CrossRef] [PubMed]
- Pucci, S.; Mazzarelli, P.; Paola, M.; Sesti, F.; Fabiola, S.; Boothman, D.A.; David, B.A.; Spagnoli, L.G.; Luigi, S.G. Interleukin-6 affects cell death escaping mechanisms acting on Bax-Ku70-Clusterin interactions in human colon cancer progression. Cell Cycle 2009, 8, 473–481. [Google Scholar] [CrossRef] [Green Version]
- Brix, N.; Tiefenthaller, A.; Anders, H.; Belka, C.; Lauber, K. Abscopal, immunological effects of radiotherapy: Narrowing the gap between clinical and preclinical experiences. Immunol. Rev. 2017, 280, 249–279. [Google Scholar] [CrossRef]
- Wang, R.; Zhou, T.; Liu, W.; Zuo, L. Molecular mechanism of bystander effects and related abscopal/cohort effects in cancer therapy. Oncotarget 2018, 9, 18637–18647. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year of Publication) [Ref.] | Tubin et al. (2017) [21] | Tubin et al. (2019) [37] | Massaccesi * et al. (2019) [38] | Tubin et al. (2019) [39] | Tubin ** et al. (2020) [40] | Tubin et al. (2019) [41] | Tubin *** et al. (2020) [42] |
|---|---|---|---|---|---|---|---|
| Type of study | Retrospective | Retrospective phase II | Retrospective case series (re-irradiation) | Retrospective | Retrospective | Prospective | Prospective phase I |
| Number of patient sunderwent SBRT-PATHY | 7 | 20 | 8 | 23 | 3 | 8 | 20 |
| Median follow up (months) | 6 (2–9) | 13 (4–27) | 7 (1–15) | 9.4 (4–20) | 5.3 (3–7) | 11.8 (4–22) | 9 (4–12) |
| Local control (bystander effect) | 100% | 95% | 83% | 96% | 67% | 75% | 73% |
| Abscopal response | 28.6% | 45% | Not evaluable | 52% | Not evaluable | 50% | 47% |
| Symptom relief | 100% | 80% | 100% | 96% | 67% | 88% | 82% |
| Treated symptoms | Dyspnea, pain. | Dyspnea, pain, cough, hemoptysis. | Pain, bleeding | Dyspnea, pain, cough. | Pain, Dysphagia. | Dyspnea, pain, cough. | Dyspnea, pain, cough, haemoptysis, edema-extremities, dysphonia. |
| Toxicity | none | Fatigue G1 (15%) | none | none | none | none | Fatigue G1 (20%) |
| Hematological toxicity/leucopenia | none | none | none | none | none | none | none |
| Median total dose/dose-fraction (Gy) | 10/10 | 10–30/10 | 10/10 | 10–30/10 | 36/12 | 30/10 | 30/10 |
| Gene-Expression Findings | |||||
|---|---|---|---|---|---|
| Tumor Site | Immunohistochemistry Findings | TNF | IL6 | TRAIL | IFNG |
| Patient 1. SCC lung (partially irradiated, bystander site) | 80% necrosis, 20% viable tumor cells, dense aggregation of lymphocytes in PIM, focal accumulation of CD20+ B-lymphocytes, dense infiltration of CD3+ T-lymphocytes (CD8+), high number of CD14+ myeloid-derived suppressor cells, small number of CD15+ myeloid-derived suppressor cells, CD56+NK cells were not detectable; AIF was highly expressed. | + | + | + | + |
| AC lung (unirradiated, abscopal site) | 80% necrosis, 20% viable tumor cells, no aggregation of lymphocytes, CD20+ B-lymphocytes absent, CD3+ T-lymphocytes present (predominantly CD4+), low number of CD14+ myeloid-derived suppressor cells, small number of CD15+ myeloid-derived suppressor cells, CD56+NK cells were not detectable; AIF was highly expressed. | + | + | + | − |
| Metastatic lymph nodes hilus/mediastinum (unirradiated, abscopal site) | 100% necrosis, no viable tumor cells, present some CD20+ B-lymphocytes, prevalent infiltration of CD3+ T-lymphocytes (CD8+), high number of CD14+ myeloid-derived suppressor cells, small number of CD15+ myeloid-derived suppressor cells, CD56+NK cells were not detectable; AIF was highly expressed. | + | + | + | + |
| Patient 2. AC lung (partially irradiated, bystander site) | 100% necrosis, no viable tumor cells, dense lymphocytic infiltrates in PIM-region, foamy macrophages and multinucleated giant cells, all lymphocytes were CD3+ (CD8+ T-lymphocytes), CD4:CD8 ratio 1:2, higher number of FoxP3 positive cells, CD20+ and PD-L1 were negative; AIF was highly expressed. | + | + | + | − |
| AC lung (prior SBRT-PATHY) | Majority of lymphocytes were CD3+ with equal distribution of CD4+ and CD8+ cells, FoxP3 also stained isolated cells, CD20+ and PD-L1 negative. | NA | |||
| Metastatic lymph nodes hilus/mediastinum (unirradiated, abscopal site) | 100% necrosis, no viable tumor cells; AIF was highly expressed. | + | + | + | − |
| Patient 3. AC rectum (partially irradiated, bystander site) | 75% necrosis, 25% viable tumor cells, lymphocytic reaction with focal fibrosis, CD3+ T lymphocytes formed the majority of cells, predominance of CD8+ (CD4:CD8 ratio 1:2), CD20+ cells within vital tumor tissue, FoxP3 was negative, PD-L1 negative, very strong cytoplasmatic expression of CD14+ in PIM-region; AIF was highly expressed. | + | + | + | + |
| AC rectum (prior SBRT-PATHY) | More CD4+ T-lymphocytes than CD8+ T-lymphocytes, and few cells were also CD20+ and FoxP3+. PD-L1 negative. | NA | |||
| Metastatic lymph nodes pelvis/mesorectum (unirradiated, abscopal site) | 100% necrosis, no viable tumor cells. AIF was highly expressed. | + | + | + | + |
| AC caecum (unirradiated, abscopal site) | AIF was highly expressed. | + | + | + | + |
| Patient 4. AC rectum (partially irradiated, bystander site) | 75% necrosis, 25% viable tumor cells, lymphocytic reaction with focal fibrosis, CD3+ T lymphocytes formed the majority of cells, more or less the same number of CD4+ and CD8+ T-lymphocytes (CD4:CD8 ratio 1:1), FoxP3 was negative, PD-L1 negative. Very strong cytoplasmatic expression of CD14+ in PIM-region; AIF was highly expressed. | + | + | − | − |
| AC rectum (prior SBRT-PATHY) | Similar number of CD4+ and CD8+ cells and few cells were also CD20+ and FoxP3+. PD-L1 negative. Very strong cytoplasmatic expression of CD14. | NA | |||
| Metastatic lymph nodes pelvis/mesorectum (unirradiated, abscopal site) | 100% necrosis, no viable tumor cells. AIF was highly expressed. | + | + | + | + |
| Immunostimulatory Effects | |
|---|---|
| Calreticulin translocation to the surface of tumor cells (“eat me” signal) * | Increased tumor cells phagocytosis Promotes pro-inflammatory cytokines release from APCs |
| Release of HMGB1 protein (“danger signal”) * | DC migration and maturation (increase in efficiency of antigen processing and presentation) Release of pro-inflammatory cytokines and chemokines from APCs |
| Release of ATP * | Release of pro-inflammatory cytokines from APCs (priming of IFN-γ-producing cytotoxic CD8+ T cells) |
| HSP increase (membrane-bound expression and extracellular release) * | Stimulate innate and adaptive immune responses |
| Decrease of CD47 surface expression (“do not-eat-me” signal) | Increase tumor cells phagocytosis |
| Accumulation of cytosolic DNA in irradiated tumor cells * | Activation of the cGAS/STING pathway and production of type I IFNs and other pro-inflammatory cytokines (APCs maturation, cross-presentation and T cell recruitment) |
| Smac release from mitochondria | Increase tumor cells sensitivity to granzyme-induced apoptosis |
| Generation of novel peptides and increase of the pool of intracellular peptides presented | Increase the anti-tumor immune response |
| Increased MHC-I expression (critical for antigen recognition by CD8+ TCRs) | Enhance recognition and killing of cancer cells by cytotoxic T cells |
| Increase of NKG2D ligands, co-stimulatory molecules (e.g., CD80) and adhesion molecules (e.g., ICAM-1, E-selectin) on tumor cells | Enhance recognition and killing of cancer cells by cytotoxic lymphocytes |
| Upregulation of “death receptors” (e.g., FAS/CD95) | Enhance recognition and killing of cancer cells by cytotoxic lymphocytes |
| Release of chemokines (e.g., CXCL9, CXCL10, CXCL16,), increase of adhesion molecules on the vascular endothelium (e.g., VCAM-1), normalization of the tumor vasculature | Facilitate the recruitment of effector T-cells to the tumor site |
| Immunosuppressive Effects | |
| Upregulation of PDL-1 on cancer cells | Inhibit CTL-mediated tumor killing |
| Accumulation of regulatory T cells (related to intrinsic higher radio-resistance and increase of immunosuppressive mediators and cytokines induced by radiation) | Immunosuppression |
| Accumulation of immunosuppressive myeloid cells (N2 neutrophils, M2 macrophages, MDSCs) secondary to the increase of CSF-1, SDF-1, CCL2 induced by radiation | Immunosuppression |
| Induction of TGF-beta secretion | Multiple immunosuppressive effects |
| Upregulation of the transcription of HIF-1α | Multiple immunosuppressive effects |
| Upregulation of adenosine | Multiple immunosuppressive effects |
| Killing of tumor-infiltrating immune cells (e.g., lymphocytes, APCs) | Immunosuppression |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tubin, S.; Gupta, S.; Grusch, M.; Popper, H.H.; Brcic, L.; Ashdown, M.L.; Khleif, S.N.; Peter-Vörösmarty, B.; Hyden, M.; Negrini, S.; et al. Shifting the Immune-Suppressive to Predominant Immune-Stimulatory Radiation Effects by SBRT-PArtial Tumor Irradiation Targeting HYpoxic Segment (SBRT-PATHY). Cancers 2021, 13, 50. https://doi.org/10.3390/cancers13010050
Tubin S, Gupta S, Grusch M, Popper HH, Brcic L, Ashdown ML, Khleif SN, Peter-Vörösmarty B, Hyden M, Negrini S, et al. Shifting the Immune-Suppressive to Predominant Immune-Stimulatory Radiation Effects by SBRT-PArtial Tumor Irradiation Targeting HYpoxic Segment (SBRT-PATHY). Cancers. 2021; 13(1):50. https://doi.org/10.3390/cancers13010050
Chicago/Turabian StyleTubin, Slavisa, Seema Gupta, Michael Grusch, Helmuth H. Popper, Luka Brcic, Martin L. Ashdown, Samir N. Khleif, Barbara Peter-Vörösmarty, Martin Hyden, Simone Negrini, and et al. 2021. "Shifting the Immune-Suppressive to Predominant Immune-Stimulatory Radiation Effects by SBRT-PArtial Tumor Irradiation Targeting HYpoxic Segment (SBRT-PATHY)" Cancers 13, no. 1: 50. https://doi.org/10.3390/cancers13010050
APA StyleTubin, S., Gupta, S., Grusch, M., Popper, H. H., Brcic, L., Ashdown, M. L., Khleif, S. N., Peter-Vörösmarty, B., Hyden, M., Negrini, S., Fossati, P., & Hug, E. (2021). Shifting the Immune-Suppressive to Predominant Immune-Stimulatory Radiation Effects by SBRT-PArtial Tumor Irradiation Targeting HYpoxic Segment (SBRT-PATHY). Cancers, 13(1), 50. https://doi.org/10.3390/cancers13010050