
The 4P: Preventing Preneoplasia through Patients Partnership

Abstract
:Simple Summary
Abstract
1. Introduction
2. Three Prevention Degrees
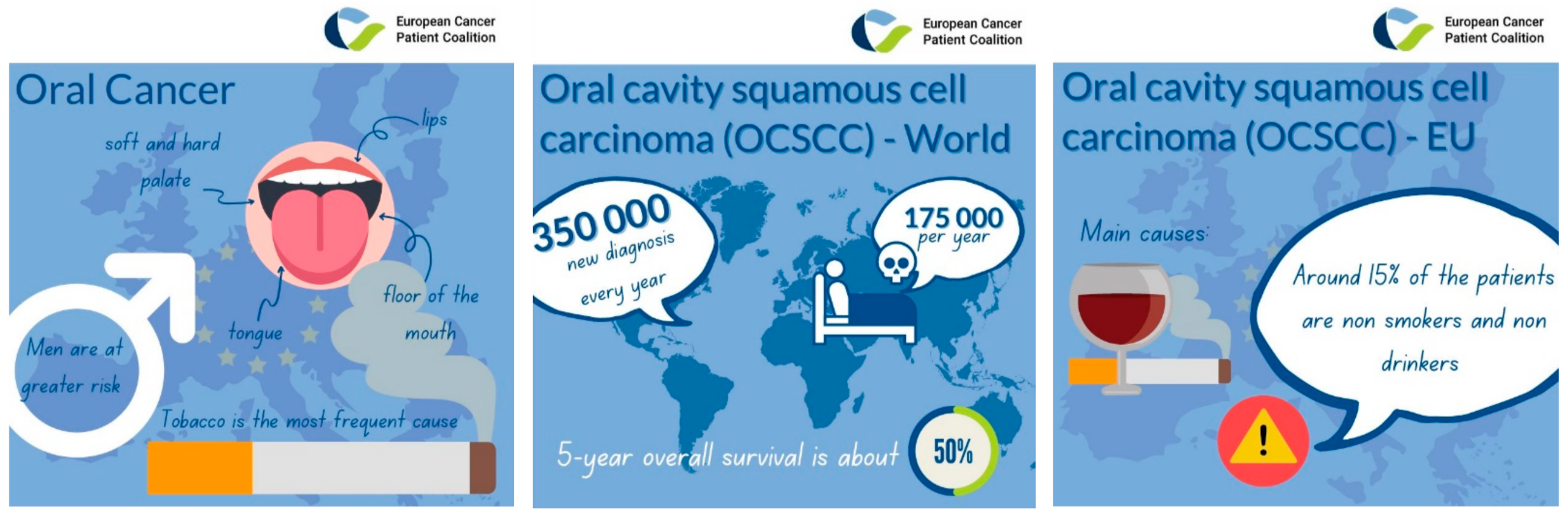
2.1. Primary Prevention: No Smoking/No Drinking Campaigns
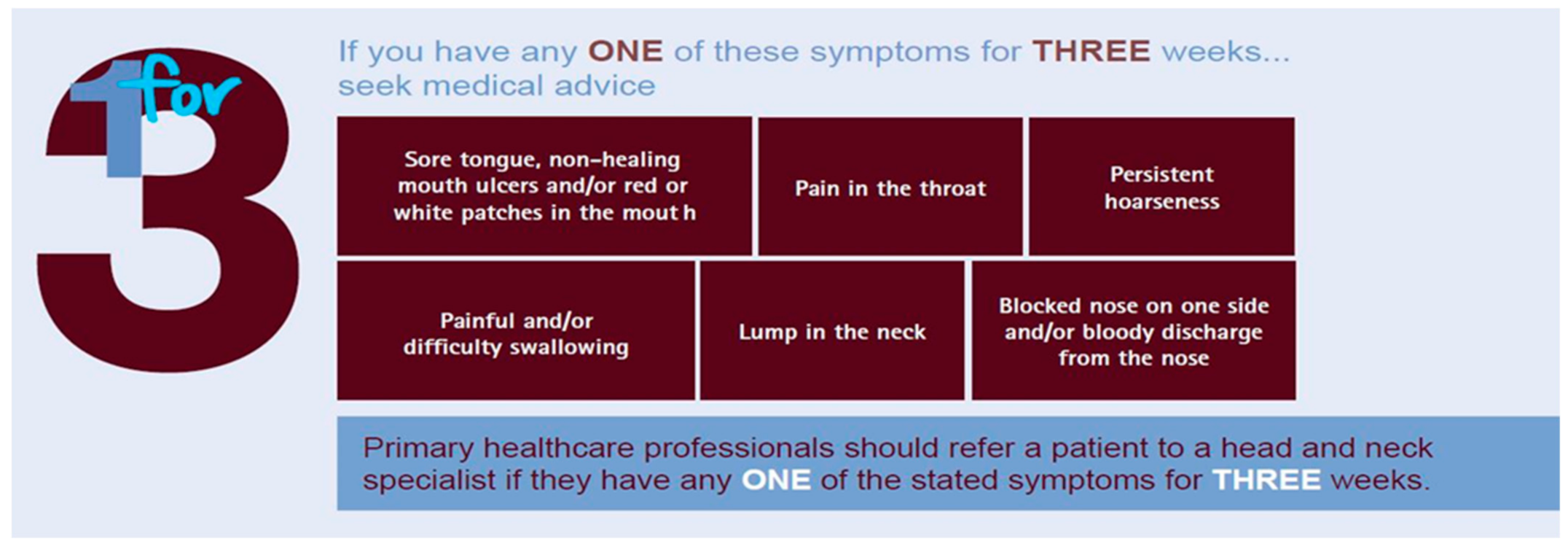
2.2. Secondary Prevention: Catching Cancers Early
2.2.1. Visual Oral Cancer Screening
2.2.2. Self-Examination and Other Screening Methods
2.3. Tertiary Prevention: No Tumoral Relapse
3. Future Needs
3.1. The Help of «First Line» Practitioners: Dentists/Dental Hygienists and Pharmacists
- ✓
- Perform an annual check-up of the oral cavity of patients
- ✓
- Address/refer or biopsy the detected mucosal lesions
- ✓
- Ensure increased follow-up of drinker/smoker patients
- ✓
- Ensure increased follow-up of patients who have already presented one or more cancers of the oral cavity
- Increase the detection rate of these lesions by the development of these clinical new standardized procedures. Oral cancers outcomes will be reduced only if the disease is recognized earlier.
- Change behaviors and lifestyle of the general population by encouraging people to go for a dental consultation. To contribute to health promotion, awareness campaigns, systematic reminders, promoting a free screening consultation for smokers/drinkers would be ways of approaching the public. A first option would be to improve the advice thus as not to scare patients, then to redirect them to a maxillofacial surgeon or an ENT surgeon if needed. Dentists must, therefore, be trained to initiate discussions (help smokers to give up their smoking habits and have good nutrition [9] and then in severe cases to announce bad news and address). A solution could be to set up key health messages as a “to-do dentist list” for oral cancer prevention. In the same line, dentists should pay particular attention to ethnic differences and lower socio-economically patients in the management of their patients, as they have a higher risk of developing OCSSC.
- Communicate: communication between the dentist and the patient provides information about him and the natural history of the lesion or call sign. Dentists might ask patients about the exams that they physically endure, making sure that the medical terminology often used is explained in layman language, talk about the future implications of patients as potential inclusion in clinical trials (understanding of notice formations, benefits/risks) [23].
3.2. The Patient’s Journey
3.3. The Help from Patient Advocacy Groups (PAGs) for a Patient-Centered Prevention
- ✓
- Raise creating screening campaigns
- ✓
- Promote awareness of patient’s families and caregivers
- ✓
- Develop surveys to map existing knowledge
- ✓
- Raise awareness to use medical tools/devices for self-examination, for example, mirrors
- ✓
- Create a national screening day
- ✓
- Send routine dental checkups invitations (annual examination) with or without routine biopsy invitations, especially for drinkers/smokers
- ✓
- Ask patients about the exams that they physically endure
- ✓
- Encourage policies that eradicate exposure to risk factors
4. A Fruitful Partnership
4.1. Involvement in Research
4.2. Advocacy
4.3. Extended Networks
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO); International Agency for Research on Cancer (IARC). A Digital Manual for the Early Diagnosis of Oral Neoplasia [Internet]. France: IARC [Cited 21 November 2013]. Available online: http://screening.iarc.fr/atlasoral.php?lang=1 (accessed on 21 September 2020).
- Lambert, R.; Sauvaget, C.; De Camargo, C.M.; Sankaranarayanan, R. Epidemiology of Cancer from the Oral Cavity and Oropharynx. Eur. J. Gastroenterol. Hepatol. 2011, 23, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, C. Les lésions précancéreuses de la Muqueuse Buccale. Rôle de L’odontologiste: Dépistage et Prise en Charge. Sciences du Vivant. HAL Id: Hal-01739190. Available online: https://hal.univ-lorraine.fr/hal-01739190 (accessed on 20 March 2018).
- Sankaranarayanan, R.; Ramadas, K.; Amarasinghe, H.; Subramanian, S.; Johnson, N. Chapter 5: Oral Cancer: Prevention, Early Detection, and Treatment. In Cancer: Disease Control Priorities, 3rd ed.; Gelband, H., Jha, P., Sankaranarayanan, R., Horton, S., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2015; Volume 3. [Google Scholar]
- Foy, J.P.; Bertolus, C.; Saintigny, P. Oral cancer prevention worldwide: Challenges and perspectives. Oral Oncol. 2019, 88, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Gileva, O.; Libik, T.; Daurova, F.; Mudrova, O.; Redinova, T.; Kovtun, O.; Bazarnyi, V. Oral cancer awareness among aged patients with chronic oral mucosal diseases in Russian Federation. BIO Web Conf. 2020, 22, 01027. [Google Scholar] [CrossRef]
- Wissinger, E.; Griebsch, I.; Lungershausen, J.; Foster, T.; Pashos, C.L. The economic burden of head and neck cancer: A systematic literature review. Pharmacoeconomics 2014, 32, 865–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galleri, A.-C. Cancer de la cavité orale: Mise en Place d’une Campagne de prévention et D’éducation à L’auto-Examen. Chirurgie. HAL Id: Dumas-01989553. Available online: https://dumas.ccsd.cnrs.fr/dumas-01989553 (accessed on 22 January 2019).
- Reichart, P.A. Identification of risk groups for oral precancer and cancer and preventive measures. Clin. Oral Investig. 2001, 5, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Speight, P.M.; Khurram, S.A.; Kujan, O. Oral potentially malignant disorders: Risk of progression to malignancy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 612–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashim, D.; Genden, E.; Posner, M.; Hashibe, M.; Boffetta, P. Head and neck cancer prevention: From primary prevention to impact of clinicians on reducing burden. Ann. Oncol. 2019, 30, 744–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speight, P.M.; Palmer, S.; Moles, D.R.; Downer, M.C.; Smith, D.H.; Henriksson, M.; Augustovski, F. The cost-effectiveness of screening for oral cancer in primary care. Health Technol. Assess. 2006, 10, 1–144, iii–iv. [Google Scholar] [CrossRef] [PubMed]
- Speight, P.; Warnakulasuriya, S.; Ogden, G. Early Detection and Prevention of Oral Cancer: A Management Strategy for Dental Practice; British Dental Association: London, UK, 2010; pp. 1–37. [Google Scholar]
- Nagao, T.; Warnakulasuriya, S. Annual screening for oral cancer detection. Cancer Detect. Prev. 2003, 27, 333–337. [Google Scholar] [CrossRef]
- Epstein, J.B. Screening for oral potentially malignant epithelial lesions and squamous cell carcinoma: A discussion of benefit and risk. J. Can. Dent. Assoc. 2014, 80, e47. [Google Scholar] [CrossRef] [Green Version]
- Sankaranarayanan, R.; Ramadas, K.; Thara, S.; Muwonge, R.; Thomas, G.; Anju, G.; Mathew, B. Long term effect of visual screening on oral cancer incidence and mortality in a randomized trial in Kerala, India. Oral Oncol. 2013, 49, 314–321. [Google Scholar] [CrossRef]
- Warnakulasuriya, K.A.; Ekanayake, A.N.; Sivayoham, S.; Stjernswärd, J.; Pindborg, J.J.; Sobin, L.H.; Perera, K.S. Utilization of primary health care workers for early detection of oral cancer and precancer cases in Sri Lanka. Bull. World Health Organ. 1984, 62, 243–250. [Google Scholar] [PubMed]
- Rethman, M.P.; Carpenter, W.; Cohen, E.E.; Epstein, J.; Evans, C.A.; Flaitz, C.M.; Graham, F.J.; Hujoel, P.P.; Kalmar, J.R.; Koch, W.M.; et al. Evidence-based clinical recommendations regarding screening for oral squamous cell carcinomas. J. Am. Dent. Assoc. 2010, 141, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.; Liu, J.L.; Brocklehurst, P.; Glenny, A.M.; Lingen, M.; Kerr, A.R.; Ogden, G.; Warnakulasuriya, S.; Scully, C. Clinical Assessment to Screen for Oral Cavity Cancer and Potentially Malignant Disorders in Apparently Healthy Adults. Cochrane Database Syst. Rev. 2013, 11, CD010173. [Google Scholar] [CrossRef] [Green Version]
- Brocklehurst, P.; Kujan, O.; O’Malley, L.A.; Ogden, G.; Shepherd, S.; Glenny, A.M. Screening Programmes for the Early Detection and Prevention of Oral Cancer. Cochrane Database Syst. Rev. 2013, 11, CD004150. [Google Scholar] [CrossRef] [Green Version]
- Mohan, P.; Richardson, A.; Potter, J.D.; Coope, P.; Paterson, M. Opportunistic Screening of Oral Potentially Malignant Disorders: A Public Health Need for India. JCO Glob. Oncol. 2020, 6, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Family Welfare (India). Operational Framework Management of Common Cancers. Available online: http://cancerindia.org.in/wp-content/uploads/2017/11/Operational_Framework_Management_of_Common_Cancers.pdf (accessed on 1 August 2016).
- Colloque National de Santé Publique, Palais du Luxembourg—Paris. Le Chirurgien-Dentiste: Un Acteur de la Lutte Contre le Cancer; Sous le haut patronage de M. Xavier Bertrand Ministre de la Santé et des Solidarités; Union Française pour la Santé Bucco-Dentaire (UFSBD): Paris, France, 2005. [Google Scholar]
- Elango, K.J.; Anandkrishnan, N.; Suresh, A.; Iyer, S.K.; Ramaiyer, S.K.; Kuriakose, M.A. Mouth self-examination to improve oral cancer awareness and early detection in a high-risk population. Oral Oncol. 2011, 47, 620–624. [Google Scholar] [CrossRef]
- Johnson, N.W.; Warnakulasuriya, S.; Gupta, P.C.; Dimba, E.; Chindia, M.; Otoh, E.C.; Sankaranarayanan, R.; Califano, J.; Kowalski, L. Global Oral Health Inequalities in Incidence and Outcomes for Oral Cancer: Causes and Solutions. Adv. Dent. Res. 2011, 23, 237–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patton, L.L.; Epstein, J.B.; Kerr, A.R. Adjunctive Techniques for Oral Cancer Examination and Lesion Diagnosis: A Systematic Review of the Literature. J. Am. Dent. Assoc. 2008, 139, 896–905. [Google Scholar] [CrossRef] [Green Version]
- Richards, D. Does Toluidine Blue Detect More Oral Cancer? Evid. Based Dent. Pract. 2010, 11, 104–105. [Google Scholar] [CrossRef]
- Su, W.W.; Yen, A.M.; Chiu, S.Y.; Chen, T.H. A Community-Based RCT for Oral Cancer Screening with Toluidine Blue. J. Dent. Res. 2010, 89, 933–937. [Google Scholar] [CrossRef] [PubMed]
- Recommendations for Oral Lichen. GEMUB (Groupe d’Etude de la MUqueuse Buccale, Study Group of Oral Mucosa from Hôpital Trousseau, Chambray-lès-Tours, France). Available online: https://www.gemub.org/recommandations (accessed on 21 September 2020).
- The EJP RD Short Guide on Patient Partnerships in Rare Diseases Research Projects. Working Group PENREP “Patient ENgagement in Biomedical REsearch Projects”. Available online: https://www.ejprarediseases.org/ (accessed on 1 July 2020).




{kind=link}
{kind=link}
{kind=link}
| Current Cancer PAGs Actions | Potential PAGs Preneoplasia Actions |
|---|---|
| Rising Awareness in H&N Cancers “Make Sense Campaign” | Rising Awareness in preneoplasia “Precancer Campaign” |
| Education on disease prevention | Screening campaigns with routine biopsies |
| Disease Understanding | Clinical Trials understanding to be sensitized |
| Signs and symptoms Understanding | Signs and symptoms education (tools/devices) |
| Encourage Early diagnosis | Encourage early diagnosis |
| Encourage formation to learn best practices | Importance of regular screening |
| Building partnerships with governmental bodies and organizations | Building partnerships with governmental bodies and organizations |
| Europe Standardizing Care | Europe Standardizing Care |
| Bring awareness to the importance of optimal facilities and expertise throughout the entire patient journey | Bring awareness to the importance of optimal, facilities and expertise throughout the entire patient journey |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Virgone, A.; Badreh, S. The 4P: Preventing Preneoplasia through Patients Partnership. Cancers 2021, 13, 4408. https://doi.org/10.3390/cancers13174408
Virgone A, Badreh S. The 4P: Preventing Preneoplasia through Patients Partnership. Cancers. 2021; 13(17):4408. https://doi.org/10.3390/cancers13174408
Chicago/Turabian StyleVirgone, Angélique, and Sara Badreh. 2021. "The 4P: Preventing Preneoplasia through Patients Partnership" Cancers 13, no. 17: 4408. https://doi.org/10.3390/cancers13174408
APA StyleVirgone, A., & Badreh, S. (2021). The 4P: Preventing Preneoplasia through Patients Partnership. Cancers, 13(17), 4408. https://doi.org/10.3390/cancers13174408