
Association of a Combined Cancer Exhaustion Score with Circulating Tumor Cells and Outcome in Ovarian Cancer—A Study of the OVCAD Consortium

 ,
, 

Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Combined Cancer Exhaustion Score (CCES)
2.3. Association of CTC-Related Markers with Biochemical Parameters
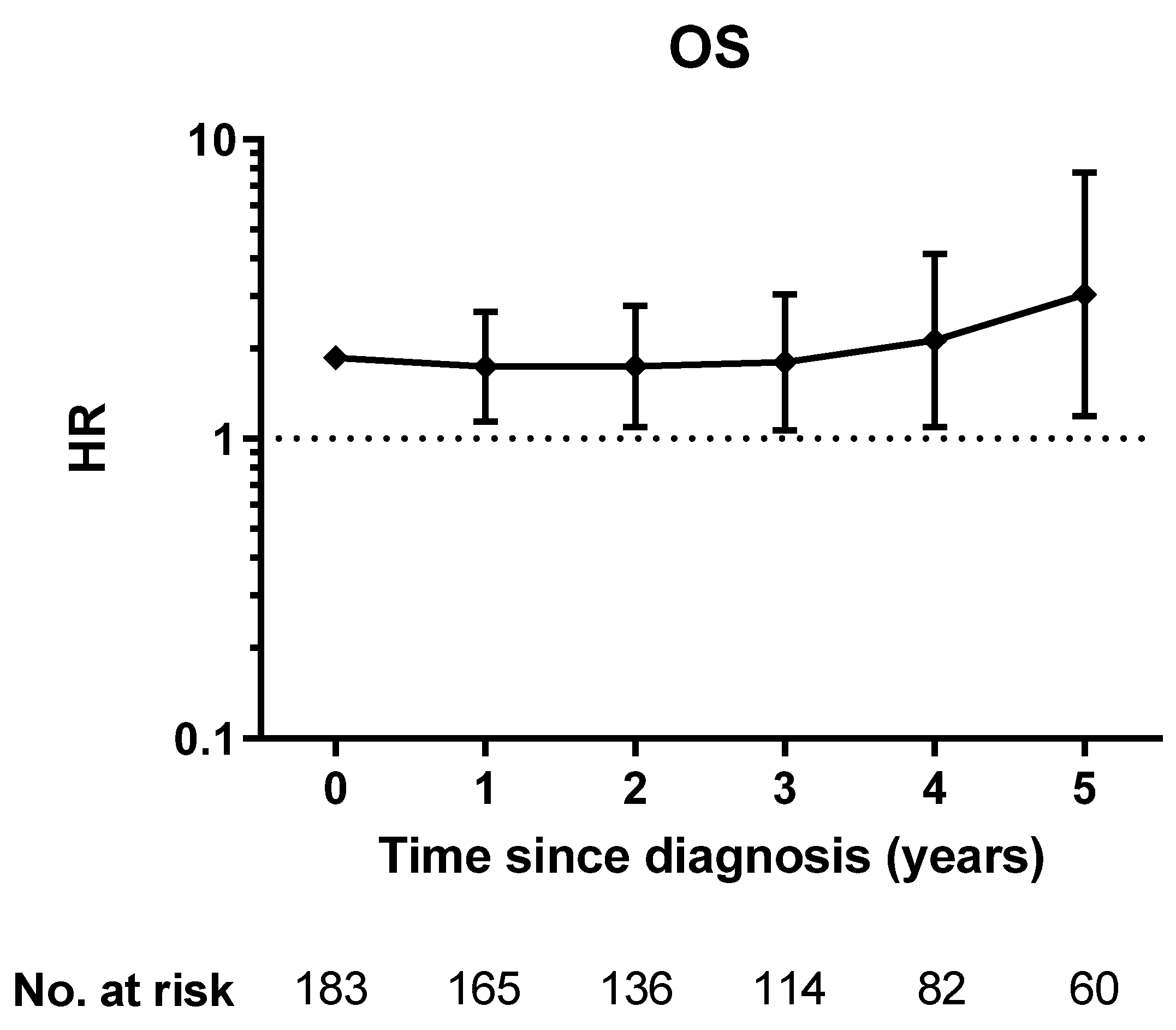
2.4. Association with Outcome
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Blood Samples and CTC Analyses
4.3. Biochemical Analyses
4.4. Combined Cancer Exhaustion Score (CCES)
4.5. Statistics
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alix-Panabieres, C.; Pantel, K. Liquid Biopsy: From Discovery to Clinical Application. Cancer Discov. 2021, 11, 858–873. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Kim, E.J.; Cho, Y.; Kim, S.; Chung, H.H.; Park, N.H.; Song, Y.S. Predictive value of circulating tumor cells (CTCs) captured by microfluidic device in patients with epithelial ovarian cancer. Gynecol. Oncol. 2017, 145, 361–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poveda, A.; Kaye, S.B.; McCormack, R.; Wang, S.; Parekh, T.; Ricci, D.; Lebedinsky, C.A.; Tercero, J.C.; Zintl, P.; Monk, B.J. Circulating tumor cells predict progression free survival and overall survival in patients with relapsed/recurrent advanced ovarian cancer. Gynecol. Oncol. 2011, 122, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Kuhlmann, J.D.; Wimberger, P.; Bankfalvi, A.; Keller, T.; Scholer, S.; Aktas, B.; Buderath, P.; Hauch, S.; Otterbach, F.; Kimmig, R.; et al. ERCC1-positive circulating tumor cells in the blood of ovarian cancer patients as a predictive biomarker for platinum resistance. Clin. Chem. 2014, 60, 1282–1289. [Google Scholar] [CrossRef] [Green Version]
- Aktas, B.; Kasimir-Bauer, S.; Heubner, M.; Kimmig, R.; Wimberger, P. Molecular profiling and prognostic relevance of circulating tumor cells in the blood of ovarian cancer patients at primary diagnosis and after platinum-based chemotherapy. Int. J. Gynecol. Cancer 2011, 21, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Obermayr, E.; Castillo-Tong, D.C.; Pils, D.; Speiser, P.; Braicu, I.; Van Gorp, T.; Mahner, S.; Sehouli, J.; Vergote, I.; Zeillinger, R. Molecular characterization of circulating tumor cells in patients with ovarian cancer improves their prognostic significance—A study of the OVCAD consortium. Gynecol. Oncol. 2013, 128, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Navas, C.; de Miguel-Perez, D.; Exposito-Hernandez, J.; Bayarri, C.; Amezcua, V.; Ortigosa, A.; Valdivia, J.; Guerrero, R.; Garcia Puche, J.L.; Lorente, J.A.; et al. Cooperative and Escaping Mechanisms between Circulating Tumor Cells and Blood Constituents. Cells 2019, 8, 1382. [Google Scholar] [CrossRef] [Green Version]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–503. [Google Scholar] [CrossRef]
- Guthrie, G.J.; Roxburgh, C.S.; Horgan, P.G.; McMillan, D.C. Does interleukin-6 link explain the link between tumour necrosis, local and systemic inflammatory responses and outcome in patients with colorectal cancer? Cancer Treat Rev. 2013, 39, 89–96. [Google Scholar] [CrossRef]
- Mantzorou, M.; Koutelidakis, A.; Theocharis, S.; Giaginis, C. Clinical Value of Nutritional Status in Cancer: What is its Impact and how it Affects Disease Progression and Prognosis? Nutr. Cancer 2017, 69, 1151–1176. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Lis, C.G. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr. J. 2010, 9, 69. [Google Scholar] [CrossRef] [Green Version]
- Mahmoud, F.A.; Rivera, N.I. The role of C-reactive protein as a prognostic indicator in advanced cancer. Curr. Oncol. Rep. 2002, 4, 250–255. [Google Scholar] [CrossRef]
- Roxburgh, C.S.; McMillan, D.C. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010, 6, 149–163. [Google Scholar] [CrossRef] [PubMed]
- Chekerov, R.; Braicu, I.; Castillo-Tong, D.C.; Richter, R.; Cadron, I.; Mahner, S.; Woelber, L.; Marth, C.; Van Gorp, T.; Speiser, P.; et al. Outcome and Clinical Management of 275 Patients With Advanced Ovarian Cancer International Federation of Obstetrics and Gynecology II to IV Inside the European Ovarian Cancer Translational Research Consortium-OVCAD. Int. J. Gynecol. Cancer 2013, 23, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Hefler, L.A.; Concin, N.; Hofstetter, G.; Marth, C.; Mustea, A.; Sehouli, J.; Zeillinger, R.; Leipold, H.; Lass, H.; Grimm, C.; et al. Serum C-reactive protein as independent prognostic variable in patients with ovarian cancer. Clin Cancer Res 2008, 14, 710–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gostner, J.M.; Obermayr, E.; Braicu, I.E.; Concin, N.; Mahner, S.; Vanderstichele, A.; Sehouli, J.; Vergote, I.; Fuchs, D.; Zeillinger, R. Immunobiochemical pathways of neopterin formation and tryptophan breakdown via indoleamine 2,3-dioxygenase correlate with circulating tumor cells in ovarian cancer patients- A study of the OVCAD consortium. Gynecol. Oncol. 2018, 149, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Fleck, A.; Raines, G.; Hawker, F.; Trotter, J.; Wallace, P.I.; Ledingham, I.M.; Calman, K.C. Increased vascular permeability: A major cause of hypoalbuminaemia in disease and injury. Lancet 1985, 1, 781–784. [Google Scholar] [CrossRef]
- Seve, P.; Ray-Coquard, I.; Trillet-Lenoir, V.; Sawyer, M.; Hanson, J.; Broussolle, C.; Negrier, S.; Dumontet, C.; Mackey, J.R. Low serum albumin levels and liver metastasis are powerful prognostic markers for survival in patients with carcinomas of unknown primary site. Cancer 2006, 107, 2698–2705. [Google Scholar] [CrossRef]
- Tuomisto, A.E.; Makinen, M.J.; Vayrynen, J.P. Systemic inflammation in colorectal cancer: Underlying factors, effects, and prognostic significance. World J. Gastroenterol. 2019, 25, 4383–4404. [Google Scholar] [CrossRef]
- Platten, M.; Nollen, E.A.A.; Rohrig, U.F.; Fallarino, F.; Opitz, C.A. Tryptophan metabolism as a common therapeutic target in cancer, neurodegeneration and beyond. Nat. Rev. Drug Discov. 2019, 18, 379–401. [Google Scholar] [CrossRef] [PubMed]
- Lanser, L.; Kink, P.; Egger, E.M.; Willenbacher, W.; Fuchs, D.; Weiss, G.; Kurz, K. Inflammation-Induced Tryptophan Breakdown is Related With Anemia, Fatigue, and Depression in Cancer. Front. Immunol. 2020, 11, 249. [Google Scholar] [CrossRef] [Green Version]
- Badawy, A.A.; Guillemin, G. The Plasma [Kynurenine]/[Tryptophan] Ratio and Indoleamine 2,3-Dioxygenase: Time for Appraisal. Int. J. Tryptophan Res. 2019, 12, 1178646919868978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inaba, T.; Ino, K.; Kajiyama, H.; Yamamoto, E.; Shibata, K.; Nawa, A.; Nagasaka, T.; Akimoto, H.; Takikawa, O.; Kikkawa, F. Role of the immunosuppressive enzyme indoleamine 2,3-dioxygenase in the progression of ovarian carcinoma. Gynecol. Oncol. 2009, 115, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, R.; Kumar, D.; Burns, E.J.; Nadeau, M.; Dake, B.; Laroni, A.; Kozoriz, D.; Weiner, H.L.; Quintana, F.J. Activation of the aryl hydrocarbon receptor induces human type 1 regulatory T cell-like and Foxp3(+) regulatory T cells. Nat. Immunol. 2010, 11, 846–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mezrich, J.D.; Fechner, J.H.; Zhang, X.; Johnson, B.P.; Burlingham, W.J.; Bradfield, C.A. An interaction between kynurenine and the aryl hydrocarbon receptor can generate regulatory T cells. J. Immunol. 2010, 185, 3190–3198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beer, T.M.; Lalani, A.S.; Lee, S.; Mori, M.; Eilers, K.M.; Curd, J.G.; Henner, W.D.; Ryan, C.W.; Venner, P.; Ruether, J.D.; et al. C-reactive protein as a prognostic marker for men with androgen-independent prostate cancer: Results from the ASCENT trial. Cancer 2008, 112, 2377–2383. [Google Scholar] [CrossRef]
- Wen, L.; Guo, L.; Zhang, W.; Li, Y.; Jiang, W.; Di, X.; Ma, J.; Feng, L.; Zhang, K.; Shou, J. Cooperation Between the Inflammation and Coagulation Systems Promotes the Survival of Circulating Tumor Cells in Renal Cell Carcinoma Patients. Front. Oncol. 2019, 9, 504. [Google Scholar] [CrossRef] [PubMed]
- Rustin, G.J.; Vergote, I.; Eisenhauer, E.; Pujade-Lauraine, E.; Quinn, M.; Thigpen, T.; du Bois, A.; Kristensen, G.; Jakobsen, A.; Sagae, S.; et al. Definitions for response and progression in ovarian cancer clinical trials incorporating RECIST 1.1 and CA 125 agreed by the Gynecological Cancer Intergroup (GCIG). Int. J. Gynecol. Cancer 2011, 21, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Aletti, G.D.; Santillan, A.; Eisenhauer, E.L.; Hu, J.; Aletti, G.; Podratz, K.C.; Bristow, R.E.; Chi, D.S.; Cliby, W.A. A new frontier for quality of care in gynecologic oncology surgery: Multi-institutional assessment of short-term outcomes for ovarian cancer using a risk-adjusted model. Gynecol Oncol 2007, 107, 99–106. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n (%) | |
|---|---|
| All | 185 |
| Age | |
| Median, range (years) | 59 (18–83) |
| <55 years | 71 (38.4%) |
| ≥55 years | 114 (61.6%) |
| FIGO stage | |
| IIA-IIIB | 18 (9.7%) |
| IIIC | 135 (73.0%) |
| IV | 32 (17.3%) |
| ECOG performance status | |
| 0 | 96 (51.9%) |
| 1 | 70 (37.8%) |
| 2 | 10 (5.4%) |
| NA | 9 (4.9%) |
| Histotype | |
| LGSOC | 16 |
| HGSOC | 145 |
| other a | 24 |
| Primary treatment | |
| Neoadjuvant chemotherapy | 34 (18.4%) |
| Primary debulking surgery | 151 (81.6%) |
| Residual tumor after surgery | |
| 0 cm | 123 (66.4%) |
| >0 cm | 61 (33.0%) |
| NA | 1 (0.1%) |
| Ascites | |
| <500 mL | 50 (27.0%) |
| ≥500 mL | 100 (54.1%) |
| NA | 35 (18.9%) |
| Albumin | |
| Median, range (g/L) | 40.3 (15.2–80.0) |
| hypoalbuminemia b | 30 (16.2%) |
| normal levels | 113 (61.1%) |
| NA | 72 (38.9%) |
| Kyn/Trp | |
| Median, range | 57.3 (20.7–348.6) |
| <52.5 | 69 (37.3%) |
| ≥52.5 | 108 (58.4%) |
| NA | 8 (4.3%) |
| CRP | |
| Median, range (mg/dL) | 1.99 (0.09–40.06) |
| <1 mg/dL | 34 (18.4%) |
| ≥1 mg/dL | 139 (75.1%) |
| NA | 12 (6.5%) |
| CTCs | |
| PPIC-positive | 34 (18.4%) |
| PPIC-negative | 139 (75.1%) |
| NA | 12 (6.5%) |
| Total | CCES 1 n (%) | CCES 0 n (%) | p | p * | |
|---|---|---|---|---|---|
| 185 | 121 (65.4) | 64 (34.6) | |||
| FIGO stage | 0.039 | n.s. | |||
| IIA-IIIB | 18 | 10 (8.3) | 8 (12.5) | ||
| IIIC | 135 | 84 (69.4) | 51 (79.7) | ||
| IV | 32 | 27 (22.3) | 5 (7.8) | ||
| ECOG performance status | 0.010 | 0.041 | |||
| 0 | 96 | 55 (45.5) | 41 (64.1) | ||
| 1–2 | 80 | 61 (50.4) | 19 (29.7) | ||
| NA | 9 | 5 (4.1) | 4 (6.3) | ||
| Histotype | 0.265 | n.s. | |||
| LGSOC | 16 | 8 | 8 | ||
| HGSOC | 145 | 95 | 50 | ||
| other a | 24 | 18 | 6 | ||
| Ascites | 0.001 | 0.004 | |||
| <500 mL | 42 | 18 (14.9) | 24 (37.5) | ||
| ≥500 mL | 136 | 97 (80.2) | 39 (60.9) | ||
| NA | 7 | 6 (5.0) | 1 (1.6) | ||
| CRP | <0.001 | <0.001 | |||
| <1 mg/dL | 50 | 18 (14.9) | 32 (50.0) | ||
| ≥1 mg/dL | 100 | 82 (67.8) | 18 (28.0) | ||
| NA | 35 | 21 (17.4) | 14 (21.9) |
| CTC-Positive n = 34 | CTC-Negative n = 139 | p | |
|---|---|---|---|
| Albumin (g/L) | 0.149 * | ||
| median | 37.0 | 41.9 | |
| IQR | 33.0–40.7 | 38.0–45.6 | |
| Kyn/Trp | <0.001 | ||
| median | 76.6 | 54.7 | |
| IQR | 60.7–94.5 | 40.4–73.4 | |
| CRP (mg/dL) | 0.001 | ||
| median | 4.33 | 1.52 | |
| IQR | 1.46–7.51 | 0.50–4.50 | |
| CA-125 (U/mL) | 0.054 | ||
| Median | 705.9 | 426.2 | |
| IQR | 293.8–1411.6 | 105.7–1103.4 |
| Univariate | Multiple | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Overall survival | ||||||
| Age | ||||||
| <55 years | 1 | 1 | ||||
| ≥55 years | 1.921 | 1.317–2.801 | 0.001 | 1.669 | 1.139–2.445 | 0.009 |
| FIGO stage | ||||||
| IIA-IIIB | 1 | 1 | ||||
| IIIC | 2.468 | 1.132–5.382 | 0.023 | 2.231 | 1.015–4.906 | 0.046 |
| IV | 5.089 | 2.165–11.962 | <0.001 | 3.544 | 1.489–8.437 | 0.004 |
| ECOG performance status | * | |||||
| 0 | 1 | |||||
| 1 | 1.199 | 0.840–1.712 | 0.317 | |||
| Residual tumor load | ||||||
| no | 1 | 1 | ||||
| yes | 2.165 | 1.508–3.107 | <0.001 | 1.721 | 1.193–2.482 | 0.004 |
| CCES | ||||||
| 0 | 1 | 1 | ||||
| 1 | 2.234 | 1.503–3.320 | <0.001 | 1.867 | 1.247–2.796 | 0.002 |
| CTCs | * | |||||
| PPIC-negative | 1 | 1 | ||||
| PPIC-positive | 1.220 | 0.786–1.896 | 0.376 | |||
| CRP | * | |||||
| <1 mg/dL | 1 | |||||
| >1 mg/dL | 1.137 | 0.754–1.716 | 0.540 | |||
| Albumin | * | |||||
| >35 g/L | 1 | |||||
| ≤35 g/L | 1.830 | 1.143–2.930 | 0.012 | |||
| Kyn/Trp | * | |||||
| <median | 1 | |||||
| ≥median | 2.133 | 1.449–3.140 | <0.001 | |||
| Progression-free survival | ||||||
| Age | ||||||
| <55 years | 1 | 1 | ||||
| ≥55 years | 1.648 | 1.154–2.353 | 0.006 | 1.431 | 0.995–2.059 | 0.053 |
| FIGO stage | ||||||
| IIA-IIIB | 1 | 1 | 1 | |||
| IIIC | 1.803 | 0.956–3.400 | 0.069 | 1.614 | 0.845–3.081 | 0.147 |
| IV | 3.319 | 1.604–6.869 | 0.001 | 2.098 | 0.985–4.468 | 0.055 |
| ECOG performance status | * | |||||
| 0 | 1 | |||||
| 1 | 1.177 | 0.833–1.663 | 0.355 | |||
| Residual tumor load | ||||||
| no | 1 | 1 | ||||
| yes | 2.598 | 1.811–3.727 | <0.001 | 2.228 | 1.531–3.241 | <0.001 |
| CCES | ||||||
| 0 | 1 | 1 | ||||
| 1 | 1.747 | 1.222–2.496 | 0.002 | 1.571 | 1.080–2.286 | 0.018 |
| CTCs | * | |||||
| PPIC-negative | 1 | |||||
| PPIC-positive | 1.191 | 0.780–1.818 | 0.419 | |||
| CRP | * | |||||
| <1 mg/dL | 1 | |||||
| >1 mg/dL | 1.369 | 0.921–2.034 | 0.120 | |||
| Albumin | * | |||||
| >35 g/L | 1 | |||||
| ≤35 g/L | 1.253 | 0.785–2.002 | 0.344 | |||
| Kyn/Trp | * | |||||
| <median | 1 | |||||
| ≥median | 1.752 | 1.231–2.494 | 0.002 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obermayr, E.; Braicu, E.I.; Polterauer, S.; Loverix, L.; Concin, N.; Woelber, L.; Mahner, S.; Sehouli, J.; Van Gorp, T.; Vergote, I.; et al. Association of a Combined Cancer Exhaustion Score with Circulating Tumor Cells and Outcome in Ovarian Cancer—A Study of the OVCAD Consortium. Cancers 2021, 13, 5865. https://doi.org/10.3390/cancers13235865
Obermayr E, Braicu EI, Polterauer S, Loverix L, Concin N, Woelber L, Mahner S, Sehouli J, Van Gorp T, Vergote I, et al. Association of a Combined Cancer Exhaustion Score with Circulating Tumor Cells and Outcome in Ovarian Cancer—A Study of the OVCAD Consortium. Cancers. 2021; 13(23):5865. https://doi.org/10.3390/cancers13235865
Chicago/Turabian StyleObermayr, Eva, Elena Ioana Braicu, Stephan Polterauer, Liselore Loverix, Nicole Concin, Linn Woelber, Sven Mahner, Jalid Sehouli, Toon Van Gorp, Ignace Vergote, and et al. 2021. "Association of a Combined Cancer Exhaustion Score with Circulating Tumor Cells and Outcome in Ovarian Cancer—A Study of the OVCAD Consortium" Cancers 13, no. 23: 5865. https://doi.org/10.3390/cancers13235865
APA StyleObermayr, E., Braicu, E. I., Polterauer, S., Loverix, L., Concin, N., Woelber, L., Mahner, S., Sehouli, J., Van Gorp, T., Vergote, I., Zeillinger, R., & Aust, S. (2021). Association of a Combined Cancer Exhaustion Score with Circulating Tumor Cells and Outcome in Ovarian Cancer—A Study of the OVCAD Consortium. Cancers, 13(23), 5865. https://doi.org/10.3390/cancers13235865