
Monocarboxylate Transporters 1 and 4 and MTCO1 in Gastric Cancer


Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Data Collection
2.3. Tissue Microarray
2.4. Immunohistochemistry
2.5. Assessment of Immunostaining
2.6. Statistical Analysis
3. Results
3.1. Patients
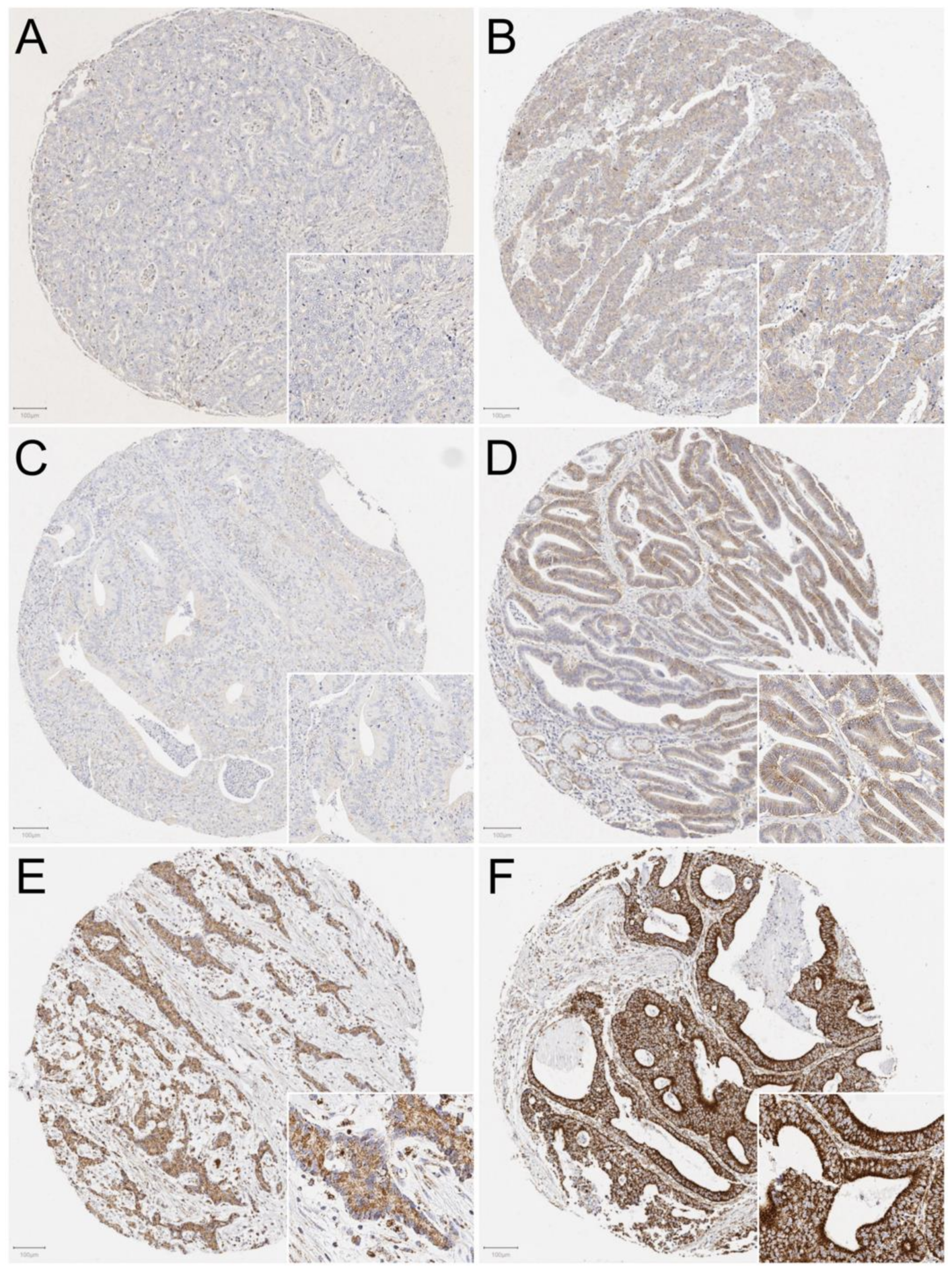
3.2. Assessment of MCT1, MCT4, and MTC01 Staining
3.3. MCT1, MCT4, and MTCO1 Expression Associations with Clinicopathological Variables and Cancer Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 68, 394–424. [Google Scholar] [CrossRef]
- Fitzmaurice, C.; Abate, D.; Abd-Allah, F.; Abdulle, A.; Iseh, K.R.; Islami, F.; Javanbakht, M.; Jayaraman, S.; Al-Aly, Z.; Brewer, J.D.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.; Han, F.; He, Y.; Yang, S.; Hua, L.; Wu, J.; Zhan, W. Stromal-epithelial metabolic coupling in gastric cancer: Stromal MCT4 and mitochondrial TOMM20 as poor prognostic factors. Eur. J. Surg. Oncol. 2014, 40, 1361–1368. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Lee, I.; Chang, W.J.; Ahn, S.M.; Lim, S.H.; Kim, H.S.; Yoo, K.H.; Jung, K.S.; Song, H.; Cho, J.H.; et al. MCT4 as a potential therapeutic target for metastatic gastric cancer with peritoneal carcinomatosis. Oncotarget 2016, 7, 43492–43503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huhta, H.; Helminen, O.; Palomäki, S.; Kauppila, J.H.; Saarnio, J.; Lehenkari, P.P.; Karttunen, T.J. Intratumoral lactate metabolism in Barrett’s esophagus and adenocarcinoma. Oncotarget 2017, 8, 22894–22902. [Google Scholar] [CrossRef] [Green Version]
- Puri, S.; Juvale, K. Monocarboxylate transporter 1 and 4 inhibitors as potential therapeutics for treating solid tumours: A review with structure-activity relationship insights. Eur. J. Med. Chem. 2020, 199, 112393. [Google Scholar] [CrossRef]
- Wang, C.; Wen, Z.; Xie, J.; Zhao, Y.; Zhao, L.; Zhang, S.; Liu, Y.; Xue, Y.; Shi, M. MACC1 mediates chemotherapy sensitivity of 5-FU and cisplatin via regulating MCT1 expression in gastric cancer. Biochem. Biophys. Res. Commun. 2017, 485, 665–671. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, J. Targeting uptake transporters for cancer imaging and treatment. Acta Pharm. Sin. B 2020, 10, 79–90. [Google Scholar] [CrossRef]
- ClinicalTrias.gov. Available online: https://www.clinicaltrials.gov/ct2/show/NCT01791595 (accessed on 15 April 2021).
- Yan, P.; Li, Y.; Tang, Z.; Shu, X.; Liu, X. High monocarboxylate transporter 4 protein expression in stromal cells predicts adverse survival in gastric cancer. Asian Pac. J. Cancer Prev. 2014, 15, 8923–8929. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, C.; Longatto-Filho, A.; Simões, K.; Jacob, C.E.; Bresciani, C.J.C.; Zilberstein, B.; Cecconello, I.; Alves, V.A.F.; Schmitt, F.; Baltazar, F. The prognostic value of CD147/EMMPRIN is associated with monocarboxylate transporter 1 co-expression in gastric cancer. Eur. J. Cancer 2009, 45, 2418–2424. [Google Scholar] [CrossRef]
- Izumi, H.; Takahashi, M.; Uramoto, H.; Nakayama, Y.; Oyama, T.; Wang, K.; Sasaguri, Y.; Nishizawa, S.; Kohno, K. Monocarboxylate transporters 1 and 4 are involved in the invasion activity of human lung cancer cells. Cancer Sci. 2011, 102, 1007–1013. [Google Scholar] [CrossRef]
- Ruan, Y.; Zeng, F.; Cheng, Z.; Zhao, X.; Fu, P.; Chen, H. High expression of monocarboxylate transporter 4 predicts poor prognosis in patients with lung adenocarcinoma. Oncol. Lett. 2017, 14, 5727–5734. [Google Scholar] [CrossRef]
- Abe, Y.; Nakayama, Y.; Katsuki, T.; Inoue, Y.; Minagawa, N.; Torigoe, T.; Higure, A.; Sako, T.; Nagata, N.; Hirata, K. The prognostic significance of the expression of monocarboxylate transporter 4 in patients with right- or left-sided colorectal cancer. Asia Pac. J. Clin. Oncol. 2019, 15, e49–e55. [Google Scholar] [CrossRef]
- Liu, Y.; Sun, X.; Huo, C.; Sun, C.; Zhu, J. Monocarboxylate Transporter 4 (MCT4) Overexpression Is Correlated with Poor Prognosis of Osteosarcoma. Med. Sci. Monit. 2019, 25, 4278–4284. [Google Scholar] [CrossRef]
- Cheng, B.; Chen, X.; Li, Y.; Huang, X.; Yu, J. Prognostic value of monocarboxylate transporter 4 in patients with esophageal squamous cell carcinoma. Oncol. Rep. 2018, 40, 2906–2915. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Han, C.; Zhou, Y.; Zhao, J.; Jing, W.; Zou, H. Altered expression of mitochondrial cytochrome c oxidase I and NADH dehydrogenase 4 transcripts associated with gastric tumorigenesis and tumor dedifferentiation. Mol. Med. Rep. 2012, 5, 1526–1530. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.; Lee, H.; Lee, M.; Pan, S.; Ke, C.; Chiu, A.W.; Wei, Y. Role of Mitochondrial DNA Copy Number Alteration in Human Renal Cell Carcinoma. Int. J. Mol. Sci. 2016, 17, 814. [Google Scholar] [CrossRef]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [Green Version]
- Ruzzo, A.; Graziano, F.; Bagaloni, I.; Di Bartolomeo, M.; Prisciandaro, M.; Aprile, G.; Ongaro, E.; Vincenzi, B.; Perrone, G.; Santini, D.; et al. Glycolytic competence in gastric adenocarcinomas negatively impacts survival outcomes of patients treated with salvage paclitaxel-ramucirumab. Gastric Cancer 2020, 23, 1064–1074. [Google Scholar] [CrossRef]
- Liberti, M.V.; Locasale, J.W. The Warburg Effect: How Does it Benefit Cancer Cells? Trends Biochem. Sci. 2016, 41, 211–218. [Google Scholar] [CrossRef] [Green Version]
- Ramos, H.; Calheiros, J.; Almeida, J.; Barcherini, V.; Santos, S.; Carvalho, A.T.P.; Santos, M.M.M.; Saraiva, L. SLMP53-1 Inhibits Tumor Cell Growth through Regulation of Glucose Metabolism and Angiogenesis in a P53-Dependent Manner. Int. J. Mol. Sci. 2020, 21, 596. [Google Scholar] [CrossRef] [Green Version]
- Halestrap, A.P. The monocarboxylate transporter family—Structure and functional characterization. IUBMB Life 2012, 64, 1–9. [Google Scholar] [CrossRef]
- Granja, S.; Tavares-Valente, D.; Queirós, O.; Baltazar, F. Value of pH regulators in the diagnosis, prognosis and treatment of cancer. Semin. Cancer Biol. 2017, 43, 17–34. [Google Scholar] [CrossRef] [Green Version]
- Takesue, T.; Kawakubo, H.; Hayashida, T.; Tsutsui, M.; Miyao, K.; Fukuda, K.; Nakamura, R.; Takahashi, T.; Wada, N.; Takeuchi, H.; et al. Downregulation of cytochrome c oxidase 1 induced radioresistance in esophageal squamous cell carcinoma. Oncol. Lett. 2017, 14, 4220–4224. [Google Scholar] [CrossRef]
- Ruckenstuhl, C.; Büttner, S.; Carmona-Gutierrez, D.; Eisenberg, T.; Kroemer, G.; Sigrist, S.J.; Fröhlich, K.; Madeo, F. The Warburg Effect Suppresses Oxidative Stress Induced Apoptosis in a Yeast Model for Cancer. PLoS ONE 2009, 4, e4592. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | MCT1 | Total | p-Value | ||
|---|---|---|---|---|---|
| Low | High | ||||
| Year of surgery | |||||
| ≥2000 | 136 (44.6%) | 111 (43.5%) | 247/560 | 0.864 | |
| <2000 | 169 (55.4%) | 144 (56.5%) | 313/560 | ||
| Age | |||||
| <69 | 163 (53.4%) | 120 (47.1%) | 283/560 | 0.149 | |
| ≥69 | 142 (46.6%) | 135 (52.1%) | 277/560 | ||
| Sex | |||||
| Male | 191 (62.6%) | 150 (58.8%) | 341/560 | 0.385 | |
| Female | 114 (37.4%) | 105 (41.2%) | 219/560 | ||
| T | |||||
| T1 + 2 | 103 (33.8%) | 63 (24.7%) | 166/560 | 0.020 | |
| T3 + 4 | 202 (66.2%) | 192 (75.3%) | 394/560 | ||
| Lymph nodes | |||||
| negative | 163 (53.4%) | 132 (51.8%) | 295/560 | 0.734 | |
| positive | 142 (46.6%) | 123 (48.2%) | 265/560 | ||
| Organ metastases | |||||
| negative | 292 (95.7%) | 235 (92.2%) | 527/560 | 0.104 | |
| positive | 13 (4.3%) | 20 (7.8%) | 33/560 | ||
| Stage | |||||
| I + II | 186 (61.0%) | 155 (60.8%) | 341/560 | 0.515 | |
| III + IV | 119 (39.0%) | 100 (39.2%) | 219/560 | ||
| Histological grade in intestinal type | |||||
| I | 99 (62.3%) | 79 (62.7%) | 178/285 | 1.000 | |
| II + III | 60 (37.7%) | 47 (37.3%) | 107/285 | ||
| Lauren | |||||
| Intestinal | 159 (52.1%) | 126 (49.4%) | 285/560 | 0.790 | |
| Diffuse | 137 (44.9%) | 120 (47.1%) | 257/560 | ||
| Other * | 9 (3.0%) | 9 (3.5%) | 18/560 | ||
| Perioperative chemotherapy | |||||
| Yes | 10 (3.3%) | 12 (4.7%) | 538/560 | 0.513 | |
| No | 295 (96.7%) | 243 (94.3%) | 22/560 | ||
| Radicality of resection | |||||
| R0 | 234 (76.7%) | 183 (71.8%) | 417/560 | 0.206 | |
| R1 or R2 | 71 (23.3%) | 72 (28.2%) | 143/560 | ||
| Variable | MCT4 | Total | p-Value | ||
|---|---|---|---|---|---|
| Low | High | ||||
| Year of surgery | |||||
| ≥2000 | 100 (34.5%) | 148 (55.2%) | 248/558 | 0.000 | |
| <2000 | 190 (65.5%) | 120 (44.8%) | 310/558 | ||
| Age | |||||
| <69 | 152 (52.4%) | 129 (48.1%) | 281/558 | 0.351 | |
| ≥69 | 138 (47.6%) | 139 (51.9%) | 277/558 | ||
| Sex | |||||
| Male | 173 (59.7%) | 168 (62.7%) | 341/558 | 0.487 | |
| Female | 117 (40.3%) | 100 (37.3%) | 217/558 | ||
| T | |||||
| T1 + 2 | 96 (33.1%) | 68 (25.4%) | 164/558 | 0.051 | |
| T3 + 4 | 194 (66.9%) | 200 (74.6%) | 394/558 | ||
| Lymph nodes | |||||
| negative | 169 (58.3%) | 124 (46.3%) | 293/558 | 0.005 | |
| positive | 121 (41.7%) | 144 (53.7%) | 265/558 | ||
| Organ metastases | |||||
| negative | 273 (94.1%) | 252 (94.0%) | 525/558 | 1.000 | |
| positive | 17 (5.9%) | 16 (6.0%) | 33/558 | ||
| Stage | |||||
| I + II | 180 (62.1%) | 159 (59.3%) | 339/558 | 0.282 | |
| III + IV | 110 (37.9%) | 109 (40.7%) | 219/558 | ||
| Histological grade in intestinal type | |||||
| I | 80 (66.7%) | 96 (58.9%) | 176/283 | 0.215 | |
| II + III | 40 (33.3%) | 67 (41.1%) | 107/283 | ||
| Lauren | |||||
| Intestinal | 120 (41.4%) | 163 (60.8%) | 283/558 | 0.000 | |
| Diffuse | 159 (54.8%) | 97 (36.2%) | 256/558 | ||
| Other * | 11 (3.8%) | 8 (3.0%) | 19/558 | ||
| Perioperative chemotherapy | |||||
| Yes | 5 (1.7%) | 17 (6.3%) | 22/558 | 0.008 | |
| No | 285 (98.3%) | 251 (93.7%) | 536/558 | ||
| Radicality of resection | |||||
| R0 | 212 (73.1%) | 202 (75.4%) | 0.562 | ||
| R1 or R2 | 78 (26.9%) | 66 (24.6%) | |||
| Variable | MTCO1 | Total | p-Value | ||
|---|---|---|---|---|---|
| Low | High | ||||
| Year of surgery | |||||
| ≥2000 | 149 (49.8%) | 99 (37.6%) | 248/562 | 0.004 | |
| <2000 | 150 (50.2%) | 164 (62.4%) | 314/562 | ||
| Age | |||||
| <69 | 153 (51.2%) | 131 (49.8%) | 284/562 | 0.800 | |
| ≥69 | 146 (48.8%) | 132 (50.2%) | 278/562 | ||
| Sex | |||||
| Male | 173 (57.9%) | 169 (64.3%) | 342/562 | 0.141 | |
| Female | 126 (42.1%) | 94 (35.7%) | 220/562 | ||
| T | |||||
| T1 + 2 | 94 (31.4%) | 74 (28.1%) | 168/562 | 0.407 | |
| T3 + 4 | 205 (68.6%) | 189 (71.9%) | 394/562 | ||
| Lymph nodes | |||||
| negative | 160 (53.5%) | 136 (51.7%) | 296/562 | 0.673 | |
| positive | 139 (46.5%) | 127 (48.3%) | 266/562 | ||
| Organ metastases | |||||
| negative | 275 (92.0%) | 254 (96.6%) | 529/562 | 0.030 | |
| positive | 24 (8.0%) | 9 (3.4%) | 33/562 | ||
| Stage | |||||
| I + II | 179 (59.9%) | 164 (62.4%) | 343/562 | 0.603 | |
| III + IV | 120 (40.1%) | 99 (37.6%) | 219/562 | ||
| Histological grade in intestinal type | |||||
| I | 83 (60.1%) | 95 (64.6%) | 178/285 | 0.464 | |
| II + III | 55 (39.9%) | 52 (35.4%) | 107/285 | ||
| Lauren | |||||
| Intestinal | 138 (46.2%) | 147 (55.9%) | 285/562 | 0.044 | |
| Diffuse | 148 (49.5%) | 110 (41.8%) | 258/562 | ||
| Other * | 13 (4.3%) | 6 (2.3%) | 19/562 | ||
| Perioperative chemotherapy | |||||
| Yes | 15 (5.0%) | 6 (2.3%) | 541/562 | 0.118 | |
| No | 284 (95.0%) | 257 (97.7%) | 21/562 | ||
| Radicality of resection | |||||
| R0 | 219 (73.2%) | 199 (75.7%) | 418/562 | 0.288 | |
| R1 or R2 | 80 (26.8%) | 64 (24.3%) | 144/562 | ||
| MCT1 | MCT4 | MTCO1 | ||||
|---|---|---|---|---|---|---|
| Number of Patients | High MCT1 HR (95% CI) | Number of Patients | High MCT4 HR (95% CI) | Number of Patients | High MTCO1 HR (95% CI) | |
| 5-year survival | ||||||
| All patients (Crude) | 560 | 1.06 (0.86–1.30) | 558 | 1.03 (0.84–1.26) | 562 | 1.08 (0.88–1.32) |
| All patients (Adjusted) a | 560 | 1.03 (0.84–1.26) | 558 | 1.07 (0.86–1.33) | 562 | 1.10 (0.90–1.35) |
| Subgroup analysis | ||||||
| Intestinal type (Crude) | 285 | 1.13 (0.85–1.50) | 283 | 1.14 (0.86–1.52) | 285 | 0.91 (0.69–1.21) |
| Intestinal type (Adjusted) b | 285 | 0.97 (0.72–1.30) | 283 | 1.17 (0.87–1.58) | 285 | 0.94 (0.71–1.25) |
| Diffuse type (Crude) | 257 | 1.04 (0.77–1.41) | 256 | 0.92 (0.67–1.26) | 258 | 1.28 (0.95–1.74) |
| Diffuse type (Adjusted) c | 257 | 1.09 (0.80–1.47) | 256 | 0.93 (0.67–1.30) | 258 | 1.30 (0.96–1.76) |
| Overall survival | ||||||
| All patients (Crude) | 560 | 1.11 (0.92–1.33) | 558 | 1.09 (0.91–1.31) | 562 | 1.08 (0.90–1.29) |
| All patients (Adjusted) a | 560 | 1.07 (0.89–1.28) | 558 | 1.08 (0.89–1.31) | 562 | 1.12 (0.93–1.35) |
| Subgroup analysis | ||||||
| Intestinal type (Crude) | 285 | 1.24 (0.96–1.59) | 283 | 1.12 (0.87–1.44) | 285 | 0.89 (0.69–1.15) |
| Intestinal type (Adjusted) b | 285 | 1.07 (0.82–1.39) | 283 | 1.14 (0.87–1.48) | 285 | 0.96 (0.75–1.24) |
| Diffuse type (Crude) | 257 | 1.04 (0.79–1.36) | 256 | 1.00 (0.75–1.34) | 258 | 1.26 (0.96–1.66) |
| Diffuse type (Adjusted) c | 257 | 1.10 (0.83–1.46) | 256 | 0.97 (0.72–1.31) | 258 | 1.27 (0.96–1.67) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eskuri, M.; Kemi, N.; Kauppila, J.H. Monocarboxylate Transporters 1 and 4 and MTCO1 in Gastric Cancer. Cancers 2021, 13, 2142. https://doi.org/10.3390/cancers13092142
Eskuri M, Kemi N, Kauppila JH. Monocarboxylate Transporters 1 and 4 and MTCO1 in Gastric Cancer. Cancers. 2021; 13(9):2142. https://doi.org/10.3390/cancers13092142
Chicago/Turabian StyleEskuri, Maarit, Niko Kemi, and Joonas H. Kauppila. 2021. "Monocarboxylate Transporters 1 and 4 and MTCO1 in Gastric Cancer" Cancers 13, no. 9: 2142. https://doi.org/10.3390/cancers13092142
APA StyleEskuri, M., Kemi, N., & Kauppila, J. H. (2021). Monocarboxylate Transporters 1 and 4 and MTCO1 in Gastric Cancer. Cancers, 13(9), 2142. https://doi.org/10.3390/cancers13092142