
Application of Machine Learning Methods to Improve the Performance of Ultrasound in Head and Neck Oncology: A Literature Review



Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Study Screening and Selection Criteria
2.3. Data Extraction and Reporting
- -
- Publication details: Data of publication and authorship information.
- -
- Proposed clinical application: Diagnostic, prognostic, or toxicity assessment.
- -
- Patient population: Anatomic site and type of head and neck cancer including primary tumor, lymph nodes.
- -
- Study details: Study type (retrospective vs. prospective, single-center vs. multi-center), sample sizes (number of patients, number of datasets, testing/independent validation), treatment information, and outcome measures.
- -
- Methodology: US instrumentation and probe frequency, radiomics platform employed (software and type of algorithm), statistical methodology, and performance metrics reported.
2.4. Radiomics Quality Score (RQS)
3. Results
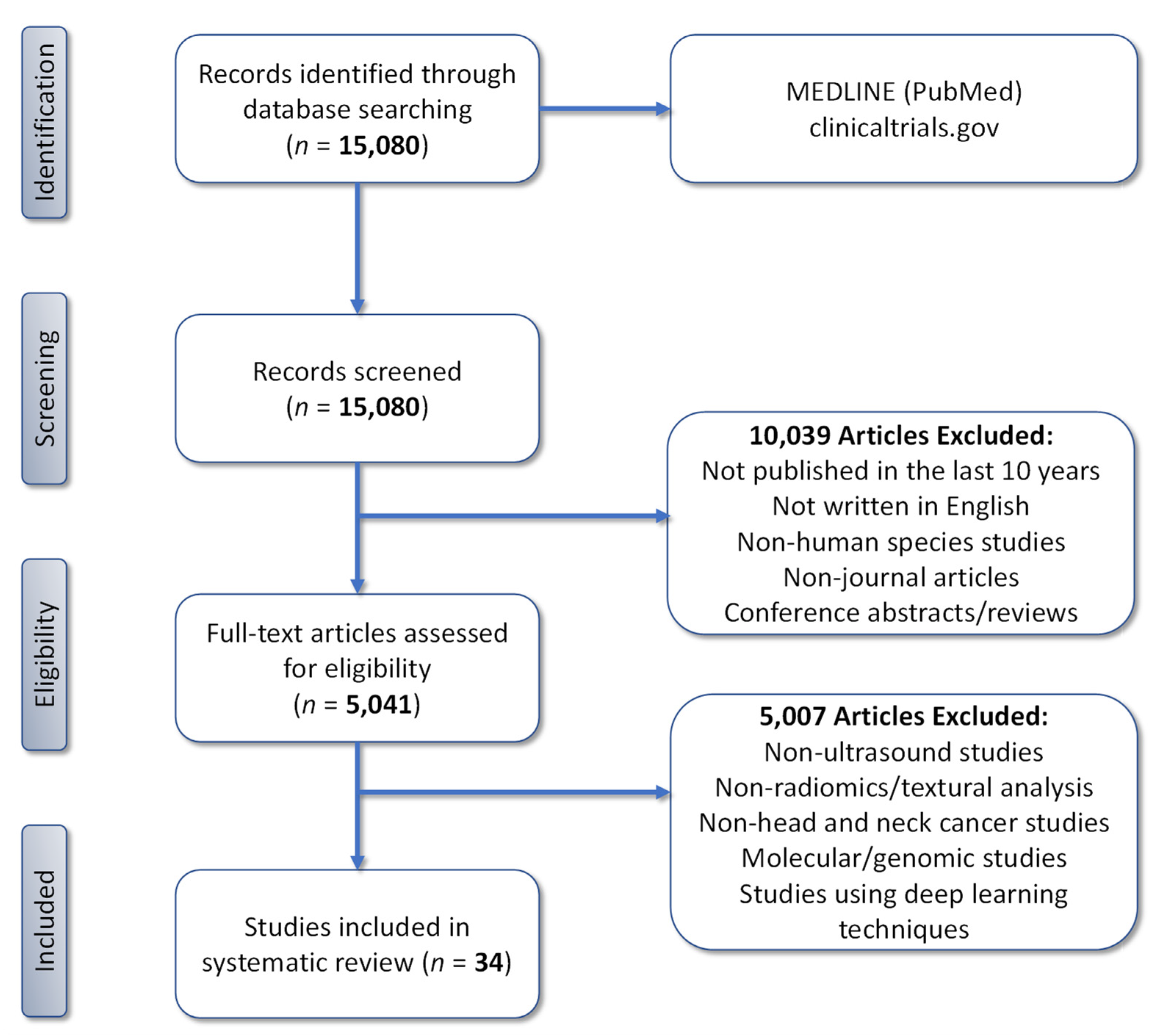
3.1. Search Results
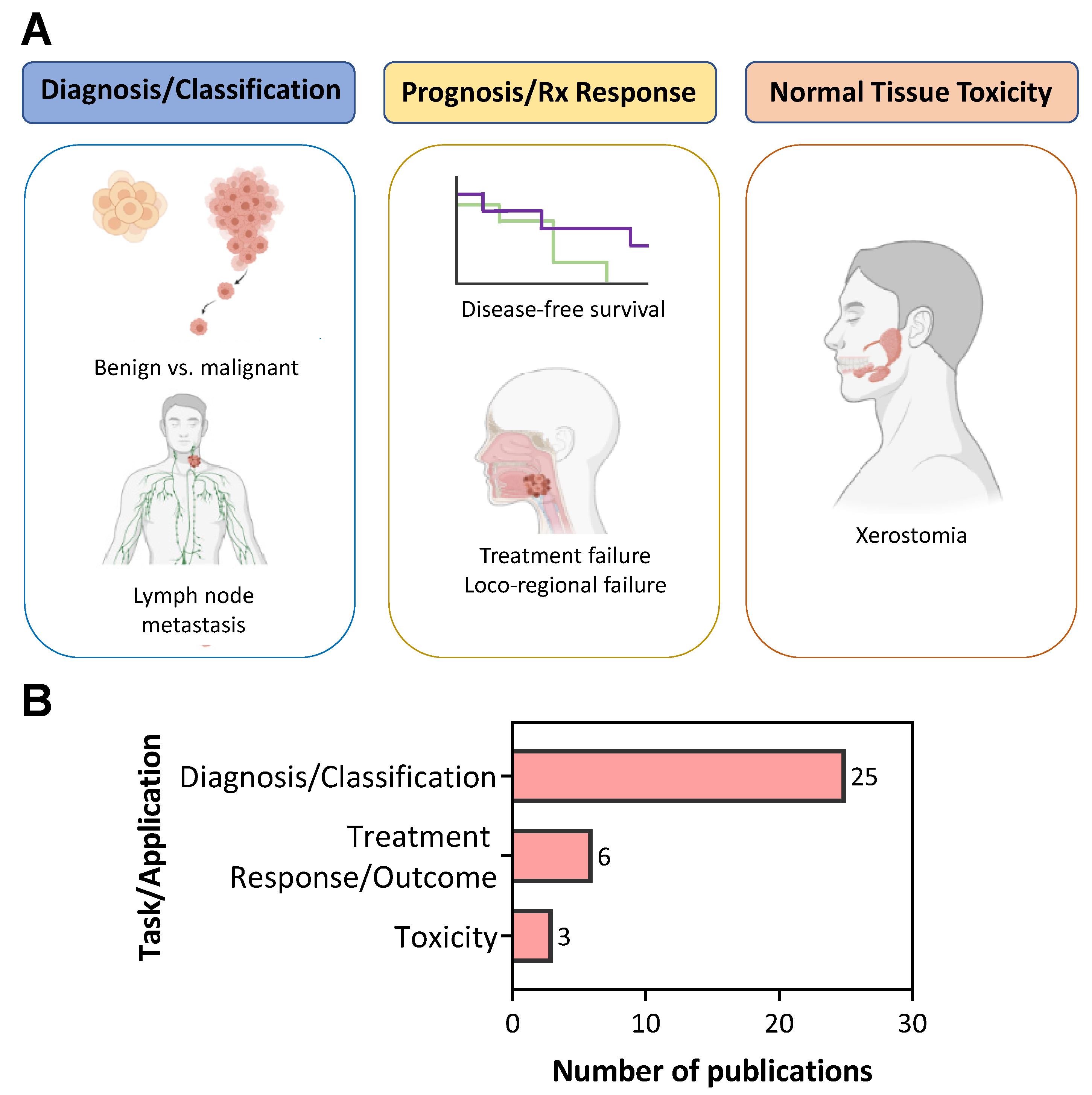
3.2. Clinical Applications of US Radiomics in Head and Neck Oncology
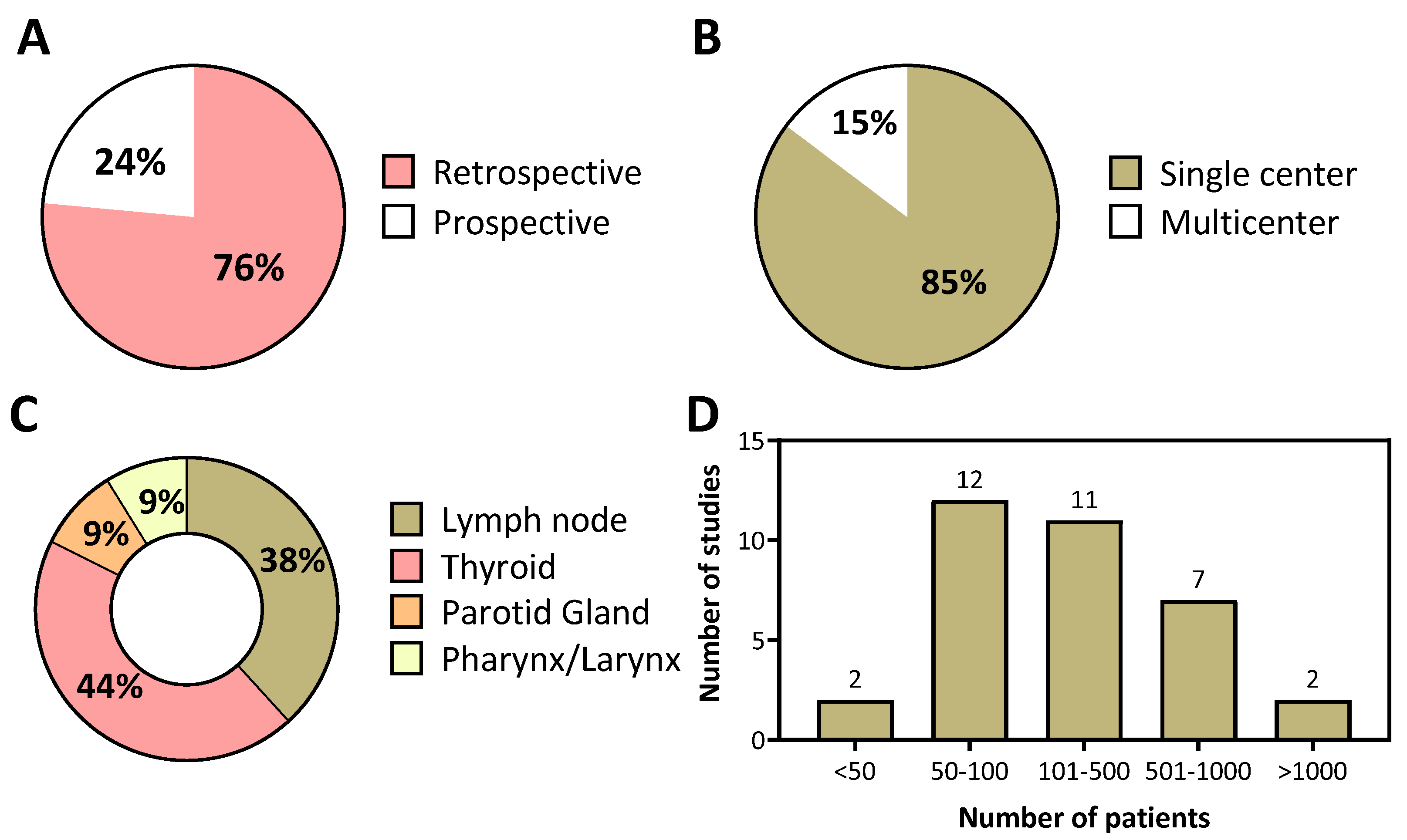
3.3. Characteristics of US Radiomics Studies in Head and Neck Cancer
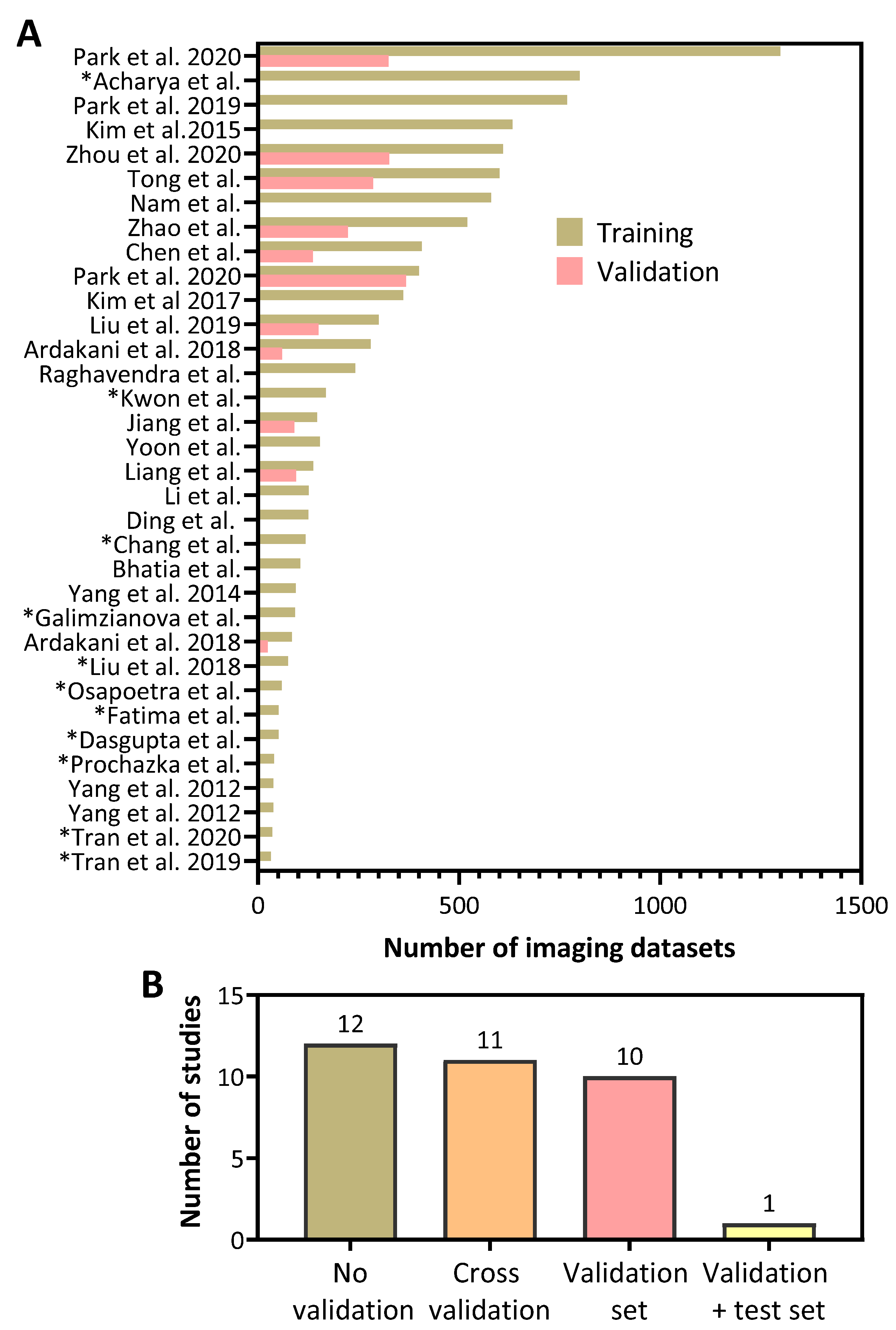
3.4. Imaging Datasets in US Radiomics Studies
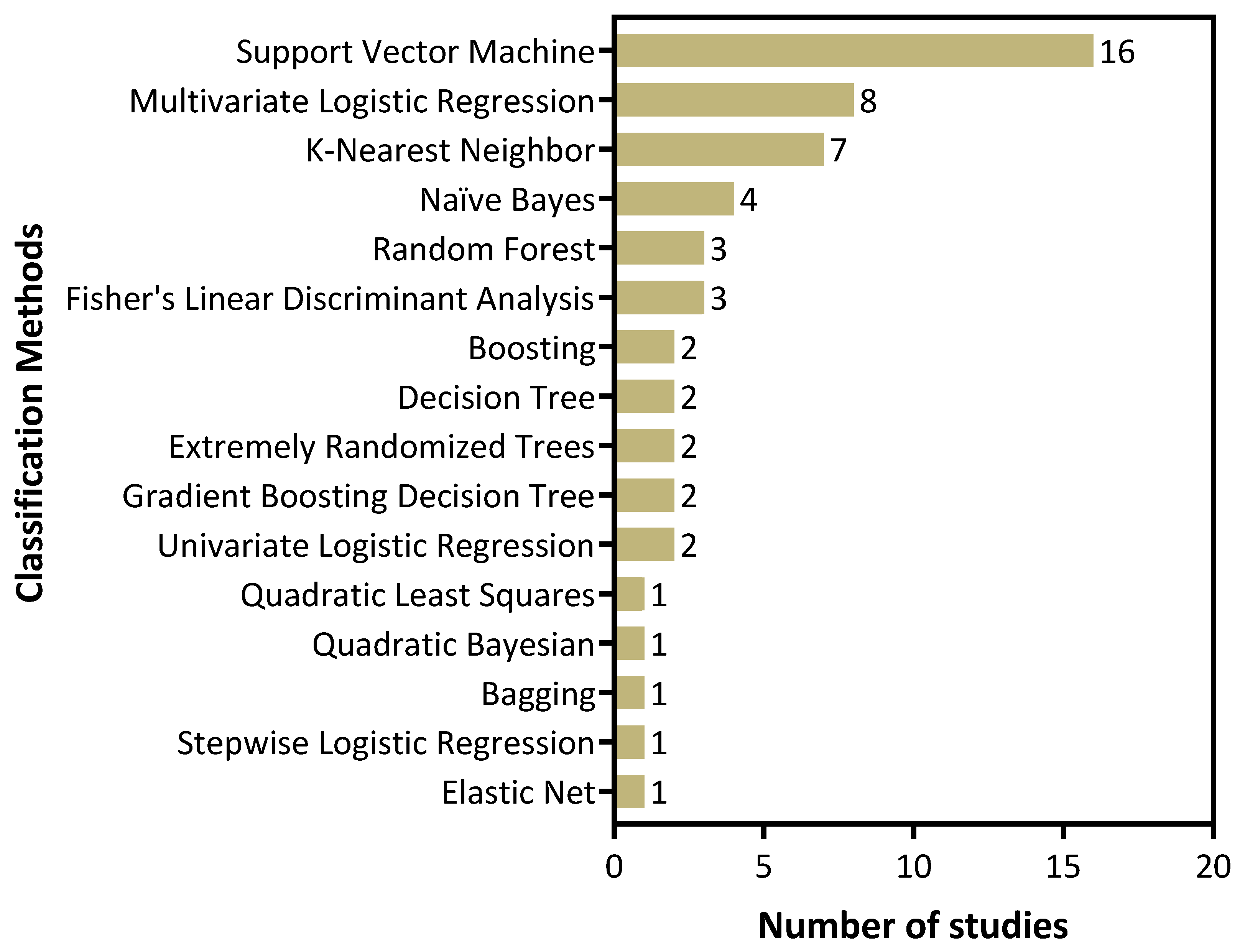
3.5. Machine Learning Methods Employed in US Radiomics Studies
3.6. Reporting Completeness and Methodologic Quality Appraisal
3.7. Performance of US Radiomic Models for Diagnostic Applications in Head and Neck Oncology
3.8. Performance of US Radiomics for Response Prediction in Head and Neck Cancer
3.9. Performance of US Radiomics for Xerostomia Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Klein Nulent, T.J.W.; Noorlag, R.; Van Cann, E.M.; Pameijer, F.A.; Willems, S.M.; Yesuratnam, A.; Rosenberg, A.J.W.P.; de Bree, R.; van Es, R.J.J. Intraoral ultrasonography to measure tumor thickness of oral cancer: A systematic review and meta-analysis. Oral Oncol. 2018, 77, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Jayachandran, S.; Sachdeva, S.K. Diagnostic accuracy of color doppler ultrasonography in evaluation of cervical lymph nodes in oral cancer patients. Indian J. Dent. Res. 2012, 23, 557. [Google Scholar] [CrossRef]
- Dudau, C.; Hameed, S.; Gibson, D.; Muthu, S.; Sandison, A.; Eckersley, R.J.; Clarke, P.; Cosgrove, D.O.; Lim, A.K. Can contrast-enhanced ultrasound distinguish malignant from reactive lymph nodes in patients with head and neck cancers? Ultrasound Med. Biol. 2014, 40, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Brito, J.P.; Gionfriddo, M.R.; Al Nofal, A.; Boehmer, K.R.; Leppin, A.L.; Reading, C.; Callstrom, M.; Elraiyah, T.A.; Prokop, L.J.; Stan, M.N.; et al. The accuracy of thyroid nodule ultrasound to predict thyroid cancer: Systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2014, 99, 1253–1263. [Google Scholar] [CrossRef]
- Gritzmann, N.; Rettenbacher, T.; Hollerweger, A.; Macheiner, P.; Hübner, E. Sonography of the salivary glands. Eur. Radiol. 2003, 13, 964–975. [Google Scholar] [CrossRef]
- Liu, Z.; Wang, S.; Dong, D.; Wei, J.; Fang, C.; Zhou, X.; Sun, K.; Li, L.; Li, B.; Wang, M.; et al. The applications of radiomics in precision diagnosis and treatment of oncology: Opportunities and challenges. Theranostics 2019, 9, 1303–1322. [Google Scholar] [CrossRef]
- Van Dijk, L.V.; Fuller, C.D. Artificial Intelligence and Radiomics in Head and Neck Cancer Care: Opportunities, Mechanics, and Challenges. Am. Soc. Clin. Oncol. Educ. Book 2021, 41, e225–e235. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Debray, T.P.A.; Vergouwe, Y.; Koffijberg, H.; Nieboer, D.; Steyerberg, E.W.; Moons, K.G.M. A new framework to enhance the interpretation of external validation studies of clinical prediction models. J. Clin. Epidemiol. 2015, 68, 279–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acharya, U.R.; Faust, O.; Sree, S.V.; Molinari, F.; Suri, J.S. ThyroScreen system: High resolution ultrasound thyroid image characterization into benign and malignant classes using novel combination of texture and discrete wavelet transform. Comput. Methods Programs Biomed. 2012, 107, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Ardakani, A.A.; Mohammadzadeh, A.; Yaghoubi, N.; Ghaemmaghami, Z.; Reiazi, R.; Jafari, A.H.; Hekmat, S.; Shiran, M.B.; Bitarafan-Rajabi, A. Predictive quantitative sonographic features on classification of hot and cold thyroid nodules. Eur. J. Radiol. 2018, 101, 170–177. [Google Scholar] [CrossRef]
- Ardakani, A.A.; Reiazi, R.; Mohammadi, A. A clinical decision support system using ultrasound textures and radiologic features to distinguish metastasis from tumor-free cervical lymph nodes in patients with papillary thyroid carcinoma. J. Ultrasound Med. 2018, 37, 2527–2535. [Google Scholar] [CrossRef]
- Bhatia, K.S.S.; Lam, A.C.L.; Pang, S.W.A.; Wang, D.; Ahuja, A.T. Feasibility study of texture analysis using ultrasound shear wave elastography to predict malignancy in thyroid nodules. Ultrasound Med. Biol. 2016, 42, 1671–1680. [Google Scholar] [CrossRef]
- Chang, Y.; Paul, A.K.; Kim, N.; Baek, J.H.; Choi, Y.J.; Ha, E.J.; Lee, K.D.; Lee, H.S.; Shin, D.; Kim, N. Computer-aided diagnosis for classifying benign versus malignant thyroid nodules based on ultrasound images: A comparison with radiologist-based assessments. Med. Phys. 2016, 43, 554. [Google Scholar] [CrossRef]
- Chen, Y.; Jiang, J.; Shi, J.; Chang, W.; Shi, J.; Chen, M.; Zhang, Q. Dual-mode ultrasound radiomics and intrinsic imaging phenotypes for diagnosis of lymph node lesions. Ann. Transl. Med. 2020, 8, 742. [Google Scholar] [CrossRef]
- Ding, J.; Cheng, H.D.; Huang, J.; Zhang, Y.; Liu, J. An improved quantitative measurement for thyroid cancer detection based on elastography. Eur. J. Radiol. 2012, 81, 800–805. [Google Scholar] [CrossRef]
- Galimzianova, A.; Siebert, S.M.; Kamaya, A.; Rubin, D.L.; Desser, T.S. Quantitative framework for risk stratification of thyroid nodules with ultrasound: A step toward automated triage of thyroid cancer. AJR Am. J. Roentgenol. 2020, 214, 885–892. [Google Scholar] [CrossRef]
- Jiang, M.; Li, C.; Tang, S.; Lv, W.; Yi, A.; Wang, B.; Yu, S.; Cui, X.; Dietrich, C.F. Nomogram Based on Shear-Wave Elastography Radiomics Can Improve Preoperative Cervical Lymph Node Staging for Papillary Thyroid Carcinoma. Thyroid 2020, 30, 885–897. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-Y.; Kim, E.-K.; Moon, H.J.; Yoon, J.H.; Kwak, J.Y. Application of texture analysis in the differential diagnosis of benign and malignant thyroid nodules: Comparison with gray-scale ultrasound and elastography. AJR Am. J. Roentgenol. 2015, 205, W343–W351. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Lee, E.; Nam, S.J.; Kim, E.K.; Moon, H.J.; Yoon, J.H.; Han, K.H.; Kwak, J.Y. Ultrasound texture analysis: Association with lymph node metastasis of papillary thyroid microcarcinoma. PLoS ONE 2017, 12, e0176103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, M.-R.; Shin, J.H.; Park, H.; Cho, H.; Kim, E.; Hahn, S.Y. Radiomics based on thyroid ultrasound can predict distant metastasis of follicular thyroid carcinoma. J. Clin. Med. 2020, 9, 2156. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Pan, D.; He, Y.; Wu, Y.; Peng, J.; Li, J.; Wang, Y.; Yang, H.; Chen, J. Using ultrasound features and radiomics analysis to predict lymph node metastasis in patients with thyroid cancer. BMC Surg. 2020, 20, 315. [Google Scholar] [CrossRef]
- Liang, J.; Huang, X.; Hu, H.; Liu, Y.; Zhou, Q.; Cao, Q.; Wang, W.; Liu, B.; Zheng, Y.; Li, X.; et al. Predicting malignancy in thyroid nodules: Radiomics score versus 2017 American College of Radiology Thyroid Imaging, Reporting and Data System. Thyroid 2018, 28, 1024–1033. [Google Scholar] [CrossRef]
- Liu, T.; Ge, X.; Yu, J.; Guo, Y.; Wang, Y.; Wang, W.; Cui, L. Comparison of the application of B-mode and strain elastography ultrasound in the estimation of lymph node metastasis of papillary thyroid carcinoma based on a radiomics approach. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 1617–1627. [Google Scholar] [CrossRef]
- Liu, T.; Zhou, S.; Yu, J.; Guo, Y.; Wang, Y.; Zhou, J.; Chang, C. Prediction of lymph node metastasis in patients with papillary thyroid carcinoma: A radiomics method based on preoperative ultrasound images. Technol. Cancer Res. Treat. 2019, 18, 1533033819831713. [Google Scholar] [CrossRef] [Green Version]
- Nam, S.J.; Yoo, J.; Lee, H.S.; Kim, E.K.; Moon, H.J.; Yoon, J.H.; Kwak, J.Y. Quantitative evaluation for differentiating malignant and benign thyroid nodules using histogram analysis of grayscale sonograms. J. Ultrasound Med. 2016, 35, 775–782. [Google Scholar] [CrossRef]
- Park, V.Y.; Han, K.; Kim, H.J.; Lee, E.; Youk, J.H.; Kim, E.K.; Moon, H.J.; Yoon, J.H.; Kwak, J.Y. Radiomics signature for prediction of lateral lymph node metastasis in conventional papillary thyroid carcinoma. PLoS ONE 2020, 15, e0227315. [Google Scholar] [CrossRef]
- Park, V.Y.; Lee, E.; Lee, H.S.; Kim, H.J.; Yoon, J.; Son, J.; Song, K.; Moon, H.J.; Yoon, J.H.; Kim, G.R.; et al. Combining radiomics with ultrasound-based risk stratification systems for thyroid nodules: An approach for improving performance. Eur. Radiol. 2021, 31, 2405–2413. [Google Scholar] [CrossRef] [PubMed]
- Prochazka, A.; Gulati, S.; Holinka, S.; Smutek, D. Classification of thyroid nodules in ultrasound images using direction-independent features extracted by two-threshold binary decomposition. Technol. Cancer Res. Treat. 2019, 18, 1533033819830748. [Google Scholar] [CrossRef] [PubMed]
- Raghavendra, U.; Acharya, U.R.; Gudigar, A.; Hong Tan, J.; Fujita, H.; Hagiwara, Y.; Molinari, F.; Kongmebhol, P.; Hoong Ng, K. Fusion of spatial gray level dependency and fractal texture features for the characterization of thyroid lesions. Ultrasonics 2017, 77, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Tong, Y.; Li, J.; Huang, Y.; Zhou, J.; Liu, T.; Guo, Y.; Yu, J.; Zhou, S.; Wang, Y.; Chang, C. Ultrasound-based radiomic nomogram for predicting lateral cervical lymph node metastasis in papillary thyroid carcinoma. Acad. Radiol. 2021, 28, 1675–1684. [Google Scholar] [CrossRef]
- Yoon, J.; Lee, E.; Kang, S.-W.; Han, K.; Park, V.Y.; Kwak, J.Y. Implications of US radiomics signature for predicting malignancy in thyroid nodules with indeterminate cytology. Eur. Radiol. 2021, 31, 5059–5067. [Google Scholar] [CrossRef]
- Zhao, C.K.; Ren, T.T.; Yin, Y.F.; Shi, H.; Wang, H.X.; Zhou, B.Y.; Wang, X.R.; Li, X.; Zhang, Y.F.; Liu, C.; et al. A comparative analysis of two machine learning-based diagnostic patterns with Thyroid Imaging Reporting and Data System for thyroid nodules: Diagnostic performance and unnecessary biopsy rate. Thyroid 2021, 31, 470–481. [Google Scholar] [CrossRef]
- Zhou, S.C.; Liu, T.T.; Zhou, J.; Huang, Y.X.; Guo, Y.; Yu, J.H.; Wang, Y.Y.; Chang, C. An ultrasound radiomics nomogram for preoperative prediction of central neck lymph node metastasis in papillary thyroid carcinoma. Front. Oncol. 2020, 10, 1591. [Google Scholar] [CrossRef]
- Dasgupta, A.; Fatima, K.; DiCenzo, D.; Bhardwaj, D.; Quiaoit, K.; Saifuddin, M.; Karam, I.; Poon, I.; Husain, Z.; Tran, W.T.; et al. Quantitative ultrasound radiomics in predicting recurrence for patients with node-positive head-neck squamous cell carcinoma treated with radical radiotherapy. Cancer Med. 2020, 10, 2579–2589. [Google Scholar] [CrossRef]
- Fatima, K.; Dasgupta, A.; DiCenzo, D.; Kolios, C.; Quiaoit, K.; Saifuddin, M.; Sandhu, M.; Bhardwaj, D.; Karam, I.; Poon, I.; et al. Ultrasound delta-radiomics during radiotherapy to predict recurrence in patients with head and neck squamous cell carcinoma. Clin. Transl. Radiat. Oncol. 2021, 28, 62–70. [Google Scholar] [CrossRef]
- Osapoetra, L.O.; Dasgupta, A.; DiCenzo, D.; Fatima, K.; Quiaoit, K.; Saifuddin, M.; Karam, I.; Poon, I.; Husain, Z.; Tran, W.T.; et al. Assessment of clinical radiosensitivity in patients with head-neck squamous cell carcinoma from pre-treatment quantitative ultrasound radiomics. Sci. Rep. 2021, 11, 6117. [Google Scholar] [CrossRef]
- Park, V.Y.; Han, K.; Lee, E.; Kim, E.K.; Moon, H.J.; Yoon, J.H.; Kwak, J.Y. Association between radiomics signature and disease-free survival in conventional papillary thyroid carcinoma. Sci. Rep. 2019, 9, 4501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, W.T.; Suraweera, H.; Quaioit, K.; Cardenas, D.; Leong, K.X.; Karam, I.; Poon, I.; Jang, D.; Sannachi, L.; Gangeh, M.; et al. Predictive quantitative ultrasound radiomic markers associated with treatment response in head and neck cancer. Future Sci. OA 2019, 6, FSO433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, W.T.; Suraweera, H.; Quiaoit, K.; DiCenzo, D.; Fatima, K.; Jang, D.; Bhardwaj, D.; Kolios, C.; Karam, I.; Poon, I.; et al. Quantitative ultrasound delta-radiomics during radiotherapy for monitoring treatment responses in head and neck malignancies. Future Sci. OA 2020, 6, FSO624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Tridandapani, S.; Beitler, J.J.; Yu, D.S.; Yoshida, E.J.; Curran, W.J.; Liu, T. Ultrasound GLCM texture analysis of radiation-induced parotid-gland injury in head-and-neck cancer radiotherapy: An in vivo study of late toxicity. Med. Phys. 2012, 39, 5732–5739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Tridandapani, S.; Beitler, J.J.; Yu, D.S.; Yoshida, E.J.; Curran, W.J.; Liu, T. Ultrasound histogram assessment of parotid gland injury following head-and-neck radiotherapy: A feasibility study. Ultrasound Med. Biol. 2012, 38, 1514–1521. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Tridandapani, S.; Beitler, J.J.; Yu, D.S.; Chen, Z.; Kim, S.; Bruner, D.W.; Curran, W.J.; Liu, T. Diagnostic accuracy of ultrasonic histogram features to evaluate radiation toxicity of the parotid glands: A clinical study of xerostomia following head-and-neck cancer radiotherapy. Acad. Radiol. 2014, 21, 1304–1313. [Google Scholar] [CrossRef] [Green Version]
- Meccariello, G.; Maniaci, A.; Bianchi, G.; Cammaroto, G.; Iannella, G.; Catalano, A.; Sgarzani, R.; De Vito, A.; Capaccio, P.; Pelucchi, S.; et al. Neck dissection and trans oral robotic surgery for oropharyngeal squamous cell carcinoma. Auris Nasus Larynx 2021. [Google Scholar] [CrossRef]
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H.J.W.L. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Jensen, S.B.; Vissink, A.; Limesand, K.H.; Reyland, M.E. Salivary Gland Hypofunction and Xerostomia in Head and Neck Radiation Patients. J. Natl. Cancer Inst. Monogr. 2019, 2019, lgz016. [Google Scholar] [CrossRef]
- Kocher, M. Artificial intelligence and radiomics for radiation oncology. Strahlenther Onkol. 2020, 196, 847. [Google Scholar] [CrossRef]
- Valdora, F.; Houssami, N.; Rossi, F.; Calabrese, M.; Tagliafico, A.S. Rapid review: Radiomics and breast cancer. Breast Cancer Res. Treat. 2018, 169, 217–229. [Google Scholar] [CrossRef] [PubMed]
- Granzier, R.W.Y.; van Nijnatten, T.J.A.; Woodruff, H.C.; Smidt, M.L.; Lobbes, M.B.I. Exploring breast cancer response prediction to neoadjuvant systemic therapy using MRI-based radiomics: A systematic review. Eur. J. Radiol. 2019, 121, 108736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chetan, M.R.; Gleeson, F.V. Radiomics in predicting treatment response in non-small-cell lung cancer: Current status, challenges and future perspectives. Eur. Radiol. 2021, 31, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, H.; Liu, X.; Rivera, S.C.; Moher, D.; Chan, A.W.; Sydes, M.R.; Calvert, M.J.; Denniston, A.K. Reporting guidelines for clinical trials of artificial intelligence interventions: The SPIRIT-AI and CONSORT-AI guidelines. Trials 2021, 22, 11. [Google Scholar] [CrossRef]
- Coppola, F.; Faggioni, L.; Regge, D.; Giovagnoni, A.; Golfieri, R.; Bibbolino, C.; Miele, V.; Neri, E.; Grassi, R. Artificial intelligence: Radiologists’ expectations and opinions gleaned from a nationwide online survey. Radiol. Med. 2021, 126, 63–71. [Google Scholar] [CrossRef]
- Chen, Y.; Stavropoulou, C.; Narasinkan, R.; Baker, A.; Scarbrough, H. Professionals’ responses to the introduction of AI innovations in radiology and their implications for future adoption: A qualitative study. BMC Health Serv. Res. 2021, 21, 813. [Google Scholar] [CrossRef]
- Huisman, M.; Ranschaert, E.; Parker, W.; Mastrodicasa, D.; Koci, M.; Pinto de Santos, D.; Coppola, F.; Morozov, S.; Zins, M.; Bohyn, C.; et al. An international survey on AI in radiology in 1,041 radiologists and radiology residents part 1: Fear of replacement, knowledge, and attitude. Eur. Radiol. 2021, 31, 7058–7066. [Google Scholar] [CrossRef]
- Kang, J.; Thompson, R.F.; Aneja, S.; Lehman, C.; Trister, A.; Zou, J.; Obcemea, C.; El Naqa, I. National Cancer Institute Workshop on Artificial Intelligence in Radiation Oncology: Training the Next Generation. Pract. Radiat. Oncol. 2021, 11, 74–83. [Google Scholar] [CrossRef]
- Wong, K.; Gallant, F.; Szumacher, E. Perceptions of Canadian radiation oncologists, radiation physicists, radiation therapists and radiation trainees about the impact of artificial intelligence in radiation oncology-national survey. J. Med. Imaging Radiat. Sci. 2021, 52, 44–48. [Google Scholar] [CrossRef]
- Van Hoek, J.; Huber, A.; Leichtle, A.; Härmä, K.; Hilt, D.; von Tengg-Kobligk, H.; Heverhagen, J.; Poellinger, A. A survey on the future of radiology among radiologists, medical students and surgeons: Students and surgeons tend to be more skeptical about artificial intelligence and radiologists may fear that other disciplines take over. Eur. J. Radiol. 2019, 121, 108742. [Google Scholar] [CrossRef] [PubMed]
- Nagendran, M.; Chen, Y.; Lovejoy, C.A.; Gordon, A.C.; Komorowski, M.; Harvey, H.; Topol, E.J.; Ioannidis, J.P.A.; Collins, G.S.; Maruthappu, M. Artificial intelligence versus clinicians: Systematic review of design, reporting standards, and claims of deep learning studies. BMJ 2020, 368, m689. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Radiomics Platform | Number of Features | Statistical Analysis/Model Performance |
|---|---|---|---|
| Acharya et al., 2012 [13] | Not reported | 5 | Malignant vs. benign thyroid nodules Training AUC: 0.99 |
| Ardakani et al., 2018 (Eur J Radiol) [14] | Not reported | 40 | Hot (hyperfunctioning) vs. cold (hypofunctioning) thyroid nodules Training AUC: 0.99 (95% CI: 0.978, 1.000) Validation AUC: 0.95 (95% CI: 0.874, 1.000) |
| Ardakani et al., 2018 (J Ultrasound Med) [15] | Not reported | 4 | LNM vs. no LNM Radiologic + textural features Training AUC: 0.99 (95% CI: 0.998, 0.999) Validation AUC: 0.95 (95% CI: 0.911, 0.993) |
| Bhatia et al., 2016 [16] | MATLAB | 15 | Malignant vs. benign thyroid nodules Training AUC: 0.97 (p < 0.0001) |
| Chang et al., 2016 [17] | Not reported | 74 | Malignant vs. benign thyroid nodules Adaboost CAD AUC: 0.98 RAD AUC: 0.98 |
| Chen et al., 2020 [18] | MATLAB | 23 | Benign vs. lymphomatous AUC: 0.95 (p < 0.001) Lymphomatous vs. metastatic AUC: 0.93 (p < 0.001) Benign vs. malignant AUC: 0.84 (p < 0.001) Benign vs. metastatic AUC: 0.72 (p < 0.001) |
| Ding et al., 2012 [19] | Not reported | Not reported | Malignant vs. benign thyroid nodules Training accuracy: 95% |
| Galimzianova et al., 2020 [20] | Not reported | 219 | Malignant vs. benign thyroid nodules Training AUC: 0.83 (95% CI: 0.715, 0.942) |
| Jiang et al., 2020 [21] | PyRadiomics | 6 | LNM vs. no LNM Training AUC: 0.85 (95% CI: 0.791, 0.912) Validation AUC: 0.83 (95% CI: 0.749, 0.916) |
| Kim et al., 2015 [22] | MATLAB | 10 | Malignant vs. benign thyroid nodules Gray-scale AUC: 0.80 Elastography AUC: 0.68 |
| Kim et al., 2017 [23] | MATLAB | 5 | LNM vs. no LNM OR: 0.98; 95% CI: 0.48-1.99, p > 0.05 |
| Kwon et al., 2020 [24] | PyRadiomics | 6 | LNM vs. no LNM Training AUC: 0.93 Validation AUC: 0.90 |
| Li et al., 2020 [25] | Ultrosomics | 690 | LNM vs. no LNM Training AUC: 0.76 Validation AUC: 0.80 |
| Liang et al., 2018 [26] | AI Kit | 19 | Malignant vs. benign thyroid nodules Training AUC: 0.92 (95% CI: 0.877, 0.965) Validation AUC: 0.93 (95% CI: 0.884, 0.977) |
| Liu et al., 2018 [27] | MATLAB | 25 | LNM vs. no LNM (B-mode + SE-US) Training AUC: 0.90 |
| Liu et al., 2019 [28] | MATLAB | 50 | LNM vs. no LNM Training AUC: 0.78 (95% CI: 0.731, 0.833) Validation AUC: 0.73 (95% CI: 0.653, 0.801) |
| Nam et al., 2016 [29] | MATLAB | 5 | Malignant vs. benign thyroid nodules Skewness AUC: 0.61 (95% CI: 0.563, 0.647) Kurtosis AUC: 0.65 (95% CI: 0.607, 0.691) Entropy AUC: 0.64 (95% CI: 0.596, 0.681) |
| Park et al., 2020 [30] | MATLAB | 14 | LNM vs. no LNM Training AUC: 0.71 (95% CI: 0.649, 0.770) Validation AUC: 0.62 (95% CI: 0.560, 0.682) |
| Park et al., 2021 [31] | MATLAB | 66 | Malignant vs. benign thyroid nodules Training AUC: 0.85 (95% CI: 0.830, 0.870) Validation AUC: 0.75 (95% CI: 0.690, 0.810) |
| Prochazka et al., 2019 [32] | MATLAB | Not reported | Malignant vs. benign thyroid nodules Accuracy: 94% |
| Raghavendra et al., 2017 [33] | Not reported | Not reported | Malignant vs. benign thyroid nodules Training AUC: 0.94 |
| Tong et al., 2020 [34] | MATLAB | 21 | LNM vs. no LNM US radiomics nomogram Training AUC: 0.94 (95% CI: 0.911, 0.982) Validation AUC: 0.91 (95% CI: 0.842, 0.987) |
| Yoon et al., 2021 [35] | MATLAB | 15 | Malignant vs. benign thyroid nodules Radiomics score + clinical variables AUC: 0.84 (95% CI: 0.775, 0.897) Clinical variables alone AUC: 0.58 (95% CI: 0.435, 0.693) |
| Zhao et al., 2021 [36] | Intelligence Foundry | 6 | Malignant vs. benign thyroid nodules ML-assisted US visual approach Training AUC: Not reported Validation AUC: 0.90 Test AUC: 0.92 |
| Zhou et al., 2020 [37] | MATLAB | 23 | LNM vs. no LNM Training AUC: 0.87 (95% CI: 0.802, 0.938) Validation AUC: 0.86 (95% CI: 0.785, 0.930) |
| Authors | Radiomics Platform | Number of Features | Statistical Analysis/Model Performance |
|---|---|---|---|
| Dasgupta et al., 2020 [38] | MATLAB | 31 | Recurrence vs. no recurrence kNN-based model a priori to treatment Training AUC: 0.74 |
| Fatima et al., 2020 [39] | MATLAB | 31 | Recurrence vs. no recurrence Pre-treatment AUC: 0.71 1-week post-treatment AUC: 0.75 4 weeks post-treatment AUC: 0.81 |
| Osapoetra et al., 2021 [40] | MATLAB | 105 | Prediction of clinical outcome (early responders vs. late responders vs. progressive disease) SVM AUC: 0.91 |
| Park et al., 2019 [41] | MATLAB | 40 | Estimation of disease-free survival C-index: 0.78 (95% CI: 0.735, 0.829) |
| Tran et al., 2019 [42] | MATLAB | 41 | Complete vs. partial responders Univariate models kNN AUC: 0.81 (95% CI: 0.640, 0.980) naive-Bayes AUC: 0.87 (95% CI: 0.730, 1.010) |
| Tran et al., 2020 [43] | MATLAB | 31 | Complete vs. partial response Univariate kNN classifier 24 h post-RT AUC: 0.74 1-week post-RT AUC: 0.81 4 weeks post-RT AUC: 0.80 |
| Authors | Radiomics Platform | Number of Features | Statistical Analysis/Model Performance |
|---|---|---|---|
| Yang et al., 2012 [44] | MATLAB | 8 | Significant differences observed for all 8 features of post-RT parotid glands compared to normal (p < 0.05) |
| Yang et al., 2012 [45] | MATLAB | 6 | Normal parotid gland R2 = 0.99 Irradiated parotid gland: R2 = 0.99 |
| Yang et al., 2014 [46] | MATLAB | 6 | Acute toxicity vs. late toxicity Peak intensity AUC: 0.90 (p < 0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
DeJohn, C.R.; Grant, S.R.; Seshadri, M. Application of Machine Learning Methods to Improve the Performance of Ultrasound in Head and Neck Oncology: A Literature Review. Cancers 2022, 14, 665. https://doi.org/10.3390/cancers14030665
DeJohn CR, Grant SR, Seshadri M. Application of Machine Learning Methods to Improve the Performance of Ultrasound in Head and Neck Oncology: A Literature Review. Cancers. 2022; 14(3):665. https://doi.org/10.3390/cancers14030665
Chicago/Turabian StyleDeJohn, Celia R., Sydney R. Grant, and Mukund Seshadri. 2022. "Application of Machine Learning Methods to Improve the Performance of Ultrasound in Head and Neck Oncology: A Literature Review" Cancers 14, no. 3: 665. https://doi.org/10.3390/cancers14030665
APA StyleDeJohn, C. R., Grant, S. R., & Seshadri, M. (2022). Application of Machine Learning Methods to Improve the Performance of Ultrasound in Head and Neck Oncology: A Literature Review. Cancers, 14(3), 665. https://doi.org/10.3390/cancers14030665