
Colorectal Surgery in the COVID-19 Era: A Systematic Review and Meta-Analysis

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Extraction and Outcomes Evaluated and Definitions
2.2. Methodological Quality Assessment
2.3. Statistical Analysis
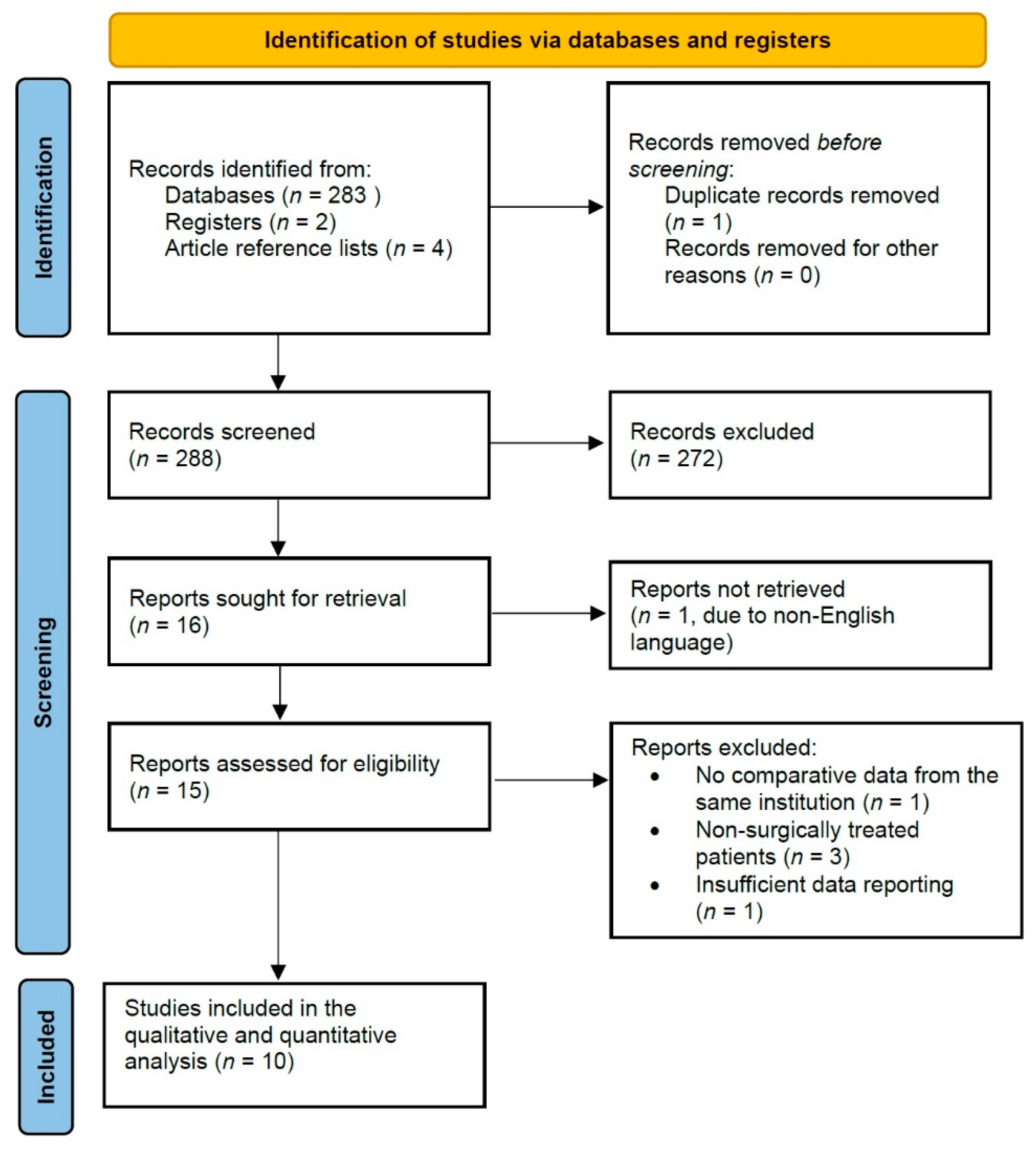
3. Results
3.1. Tumor-Related Factors
3.2. Presentation-Related Factors
3.3. Treatment-Related Factors
3.4. Treatment Outcome Factors
3.5. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Alam, W.; Bouferraa, Y.; Haibe, Y.; Mukherji, D.; Shamseddine, A. Management of colorectal cancer in the era of COVID-19: Challenges and suggestions. Sci. Prog. 2021, 104, 368504211010626. [Google Scholar] [CrossRef] [PubMed]
- Morris, E.J.A.; Goldacre, R.; Spata, E.; Mafham, M.; Finan, P.J.; Shelton, J.; Richards, M.; Spencer, K.; Emberson, J.; Hollings, S.; et al. Impact of the COVID-19 pandemic on the detection and management of colorectal cancer in England: A population-based study. Lancet Gastroenterol. Hepatol. 2021, 6, 199–208. [Google Scholar] [CrossRef]
- Donlon, N.E.; Hayes, C.; Davern, M.; Bolger, J.C.; Irwin, S.C.; Butt, W.T.; McNamara, D.A.; Mealy, K. Impact of COVID-19 on the Diagnosis and Surgical Treatment of Colorectal Cancer: A National Perspective. Dis. Colon Rectum 2021, 64, 1305–1309. [Google Scholar] [CrossRef]
- De Vincentiis, L.; Carr, R.A.; Mariani, M.P.; Ferrara, G. Cancer diagnostic rates during the 2020 “lockdown”, due to COVID-19 pandemic, compared with the 2018-2019: An audit study from cellular pathology. J. Clin. Pathol. 2021, 74, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinmouth, J.; Dong, S.; Stogios, C.; Rabeneck, L.; Rey, M.; Dubé, C. Estimating the Backlog of Colonoscopy due to Coronavirus Disease 2019 and Comparing Strategies to Recover in Ontario, Canada. Gastroenterology 2021, 160, 1400–1402.e1. [Google Scholar] [CrossRef]
- Grass, F.; Behm, K.T.; Duchalais, E.; Crippa, J.; Spears, G.M.; Harmsen, W.S.; Hübner, M.; Mathis, K.L.; Kelley, S.R.; Pemberton, J.H.; et al. Impact of delay to surgery on survival in stage I-III colon cancer. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2020, 46, 455–461. [Google Scholar] [CrossRef]
- Vecchione, L.; Stintzing, S.; Pentheroudakis, G.; Douillard, J.-Y.; Lordick, F. ESMO management and treatment adapted recommendations in the COVID-19 era: Colorectal cancer. ESMO Open 2020, 5, e000826. [Google Scholar] [CrossRef]
- O’Connor, J.M.; Esteso, F.; Chacón, M. Official French SARS-CoV-2 guidelines for cancer patients, a triage solution with precision medicine. Color. Cancer 2020, 9, CRC21. [Google Scholar] [CrossRef]
- Shinkwin, M.; Silva, L.; Vogel, I.; Reeves, N.; Cornish, J.; Horwood, J.; Davies, M.M.; Torkington, J.; Ansell, J. COVID-19 and the emergency presentation of colorectal cancer. Color. Dis. Off. J. Assoc. Coloproctol. Gt. Br. Irel. 2021, 23, 2014–2019. [Google Scholar] [CrossRef] [PubMed]
- Weiser, M.R. AJCC 8th Edition: Colorectal Cancer. Ann. Surg. Oncol. 2018, 25, 1454–1455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Mizuno, R.; Ganeko, R.; Takeuchi, G.; Mimura, K.; Nakahara, H.; Hashimoto, K.; Hinami, J.; Shimomatsuya, T.; Kubota, Y. The number of obstructive colorectal cancers in Japan has increased during the COVID-19 pandemic: A retrospective single-center cohort study. Ann. Med. Surg. 2020, 60, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Huang, Z.-H.; Zheng, C.Z.-L.; Li, C.; Zhang, Y.-Q.; Guo, T.-A.; Liu, F.-Q.; Xu, Y. The impact of COVID-19 pandemic on colorectal cancer patients: A single-center retrospective study. BMC Gastroenterol. 2021, 21, 185. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Li, Z.; An, Q.; Xiao, G. Impact of the COVID-19 Pandemic on Elective Surgery for Colorectal Cancer. J. Gastrointest. Cancer 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Park, I.J.; Lee, H.G.; Cho, E.; Kim, Y., II; Kim, C.W.; Yoon, Y.S.; Lim, S.-B.; Yu, C.S.; Kim, J.C. Impact of the COVID-19 Pandemic on Surgical Treatment Patterns for Colorectal Cancer in a Tertiary Medical Facility in Korea. Cancers 2021, 13, 2221. [Google Scholar] [CrossRef]
- Lim, J.H.; Lee, W.Y.; Yun, S.H.; Kim, H.C.; Cho, Y.B.; Huh, J.W.; Park, Y.A.; Shin, J.K. Has the COVID-19 Pandemic Caused Upshifting in Colorectal Cancer Stage? Ann. Coloproctol. 2021, 37, 253–258. [Google Scholar] [CrossRef]
- Kuryba, A.; Boyle, J.M.; Blake, H.A.; Aggarwal, A.; van der Meulen, J.; Braun, M.; Walker, K.; Fearnhead, N.S. Surgical Treatment and Outcomes of Colorectal Cancer Patients During the COVID-19 Pandemic: A National Population-based Study in England. Ann. Surg. Open Perspect. Surg. Hist. Educ. Clin. Approaches 2021, 2, e071. [Google Scholar] [CrossRef]
- Peltrini, R.; Imperatore, N.; Di Nuzzo, M.M.; D’Ambra, M.; Bracale, U.; Corcione, F. Effects of the first and second wave of the COVID-19 pandemic on patients with colorectal cancer: What has really changed in the outcomes? Br. J. Surg. 2021, 108, e365–e366. [Google Scholar] [CrossRef]
- Radulovic, R.S.; Cuk, V.V.; Juloski, J.T.; Arbutina, D.D.; Krdžic, I.D.; Milic, L.V.; Kenic, M.V.; Karamarkovic, A.R. Is Colorectal Cancer Stage Affected by COVID-19 Pandemic? Chirurgia 2021, 116, 331–338. [Google Scholar] [CrossRef]
- Moynihan, R.; Sanders, S.; Michaleff, Z.A.; Scott, A.M.; Clark, J.; To, E.J.; Jones, M.; Kitchener, E.; Fox, M.; Johansson, M.; et al. Impact of COVID-19 pandemic on utilisation of healthcare services: A systematic review. BMJ Open 2021, 11, e045343. [Google Scholar] [CrossRef]
- Mazidimoradi, A.; Tiznobaik, A.; Salehiniya, H. Impact of the COVID-19 Pandemic on Colorectal Cancer Screening: A Systematic Review. J. Gastrointest. Cancer 2021, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Issaka, R.B.; Feld, L.D.; Kao, J.; Hegarty, E.; Snailer, B.; Kalra, G.; Tomizawa, Y.; Strate, L. Real-World Data on the Impact of COVID-19 on Endoscopic Procedural Delays. Clin. Transl. Gastroenterol. 2021, 12, e00365. [Google Scholar] [CrossRef] [PubMed]
- Harber, I.; Zeidan, D.; Aslam, M.N. Colorectal Cancer Screening: Impact of COVID-19 Pandemic and Possible Consequences. Life 2021, 11, 1297. [Google Scholar] [CrossRef] [PubMed]
- Suárez, J.; Mata, E.; Guerra, A.; Jiménez, G.; Montes, M.; Arias, F.; Ciga, M.A.; Ursúa, E.; Ederra, M.; Arín, B.; et al. Impact of the COVID-19 pandemic during Spain’s state of emergency on the diagnosis of colorectal cancer. J. Surg. Oncol. 2021, 123, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Santoro, G.A.; Grossi, U.; Murad-Regadas, S.; Nunoo-Mensah, J.W.; Mellgren, A.; Di Tanna, G.L.; Gallo, G.; Tsang, C.; Wexner, S.D. DElayed COloRectal cancer care during COVID-19 Pandemic (DECOR-19): Global perspective from an international survey. Surgery 2021, 169, 796–807. [Google Scholar] [CrossRef]
- Chadi, S.A.; Guidolin, K.; Caycedo-Marulanda, A.; Sharkawy, A.; Spinelli, A.; Quereshy, F.A.; Okrainec, A. Current Evidence for Minimally Invasive Surgery During the COVID-19 Pandemic and Risk Mitigation Strategies: A Narrative Review. Ann. Surg. 2020, 272, e118–e124. [Google Scholar] [CrossRef]
- Di Saverio, S.; Khan, M.; Pata, F.; Ietto, G.; De Simone, B.; Zani, E.; Carcano, G. Laparoscopy at all costs? Not now during COVID-19 outbreak and not for acute care surgery and emergency colorectal surgery: A practical algorithm from a hub tertiary teaching hospital in Northern Lombardy, Italy. J. Trauma Acute Care Surg. 2020, 88, 715–718. [Google Scholar] [CrossRef]
- Francis, N.; Dort, J.; Cho, E.; Feldman, L.; Keller, D.; Lim, R.; Mikami, D.; Phillips, E.; Spaniolas, K.; Tsuda, S.; et al. SAGES and EAES recommendations for minimally invasive surgery during COVID-19 pandemic. Surg. Endosc. 2020, 34, 2327–2331. [Google Scholar] [CrossRef]
- De Simone, B.; Chouillard, E.; Sartelli, M.; Biffl, W.L.; Di Saverio, S.; Moore, E.E.; Kluger, Y.; Abu-Zidan, F.M.; Ansaloni, L.; Coccolini, F.; et al. The management of surgical patients in the emergency setting during COVID-19 pandemic: The WSES position paper. World J. Emerg. Surg. 2021, 16, 14. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Country | Time Interval of Data Collection | Total Patients | Age (Mean ± SD) | Sex (Male/Female) | Newcastle–Ottawa Scale Score |
|---|---|---|---|---|---|---|
| Pre-pandemic versus Pandemic cohorts, n (%) | ||||||
| Donlon [3] | Ireland | March 2019–March 2020 vs. March 2020–March 2021 | 1631 vs. 1093 | N/a | N/a | 7 |
| Peltrini [20] | Italy | October 2019–February 2020 vs. January 2021–May 2021 | 41 vs. 43 | N/a | N/a | 5 |
| Lim [18] | Korea | January–July 2017–2019 vs. January–July 2020 | 2514 vs. 715 | 61 (18–90) vs. 61 (17–97) * | 1484 (59%)/1030 (41%) vs. 415 (58%)/300(42%) | 8 |
| Shinkwin [11] | UK | January–December /2018–2019 vs. January–December 2020 | 539 vs. 267 | 70 ± 12.5 vs. 70 ± 14 | 308 (57.1%)/231 (42.9%) vs. 151 (56.6%)/116 (43.4%) | 8 |
| Kuryba [19] | UK | Six weeks before 23 March 2020 vs. nine weeks after | 11703 vs. 3227 | N/a | 6586 (56.2%)/5117 (43.8%) vs. 1793 (55.5%)/1434 (44.5%) | 9 |
| Choi [17] | Korea | March-September 2018–2019 vs. March-September 2020 | 1985 vs. 916 | 62.6 ± 12.2 vs. 61.7 ± 12.1 | 1160 (58.4%)/825 (41.6%) vs. 524 (57.2%)/392 (42.8%) | 9 |
| Radulovic [21] | Serbia | January–December 2019 vs. March 2020–April 2021 | 152 vs. 49 | 67.11 ± 11.62 vs. 67.41 ± 10.37 | 87 (57.2%)/65 (42.8%) vs. 22 (44.9%)/27 (55.1%) | 6 |
| Xu [15] | China | January–May 2019 vs. January–May 2020 | 828 vs. 710 | N/a | 518 (62.6%)/310 (37.4%) vs. 438 (61.7%)/272 (38.3%) | 7 |
| Cui [16] | China | February-May 2018–2019 vs. February-May 2020 | 205 vs. 67 | 65.6 ± 11.65 vs. 67.1 ± 11.4 | 111 (54.1%)/94 (45.9%) vs. 44 (65.7%)/23 (34.3%) | 9 |
| Mizuno [14] | Japan | December 2018–April 2020 vs. April 2020–August 2020 | 92 vs. 31 | 72.91 ± 10.58 vs. 72 ± 10.7 | 54 (58.7%)/38 (51.3%) vs. 25 (80.6%)/16 (19.4%) | 9 |
| Outcome | Number of Studies | Total Patients | Patients in the Prepandemic Cohort n(%) | Patients in the Pandemic Cohort n(%) | OR/WMD | 95% Confidence Intervals | p-Value | I2 | I2 p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Tumor-Related Factors | |||||||||
| Tis-T1 stage | 5 | 7301 | 628 (4.1) | 276 (6.3) | 1.14 | 0.87–1.48 | 0.34 | 41% | 0.15 |
| T2 stage | 5 | 7301 | 703 (4.6) | 255 (5.9) | 0.91 | 0.78–1.06 | 0.2 | 0% | 0.6 |
| T3 stage | 5 | 7301 | 2198 (14.5) | 883 (20) | 1.18 | 0.82–1.7 | 0.38 | 88% | <0.001 |
| T4 stage | 6 | 7385 | 736 (4.2) | 290 (5.7) | 1.19 | 0.79–1.8 | 0.4 | 80% | <0.001 |
| N + stage | 6 | 7385 | 1797 (10.2) | 720 (14.3) | 1 | 0.89–1.11 | 0.96 | 0% | 0.54 |
| M + stage | 6 | 19,414 | 2020 (11.8) | 711 (13.5) | 1.65 | 1.02–2.67 | 0.04 | 91% | <0.001 |
| Right-sided tumors | 7 | 19,893 | 5294 (37.5) | 1834 (37.4) | 0.88 | 0.51–1.52 | 0.66 | 99% | <0.001 |
| Left-sided tumors | 7 | 19,893 | 4946 (35) | 1759 (35.9) | 0.91 | 0.56–1.5 | 0.72 | 96% | <0.001 |
| Rectal tumors | 8 | 22,794 | 4794 (29.8) | 1934 (33.2) | 0.93 | 0.63–1.37 | 0.71 | 95% | <0.001 |
| Presentation-Related Factors | |||||||||
| Emergency presentation | 3 | 18,965 | 2851 (19.3) | 1149 (27.3) | 1.74 | 1.07–2.84 | 0.03 | 95% | <0.001 |
| Complicated tumor | 3 | 4562 | 113 (3.9) | 84 (5.1) | 1.72 | 0.78–3.78 | 0.18 | 82% | 0.004 |
| Treatment-Related Factors | |||||||||
| Neoadjuvant therapy | 3 | 7668 | 1459 (27.4) | 656 (30.6) | 1.22 | 1.09–1.37 | <0.001 | 0% | 0.4 |
| Palliative intent surgery | 4 | 4795 | 114 (6.6) | 126 (7.3) | 1.95 | 1.13–3.36 | 0.02 | 54% | 0.09 |
| Minimally Invasive Surgery | 6 | 22,584 | 7680 (48.1) | 2056 (34.9) | 0.68 | 0.37–1.24 | 0.2 | 98% | <0.001 |
| Stoma Formation | 5 | 19,683 | 1425 (10.2) | 479 (8.4) | 0.91 | 0.51–1.62 | 0.74 | 94% | <0.001 |
| Treatment Outcome Factors | |||||||||
| Mortality | 1 | 13,060 | 163 (1.6) | 74 (2.6) | N/a | N/a | N/a | N/a | N/a |
| Morbidity | 2 | 1810 | 63 (6.1) | 37 (4.8) | 0.92 | 0.55–1.55 | 0.76 | 25% | 0.25 |
| Length of hospital stay | 3 | 2011 | N/a | N/a | 0.51 | −0.93–1.94 | 0.49 | 79% | 0.008 |
| Lymph node harvest | 3 | 1894 | N/a | N/a | 1.57 | −1.99–5.13 | 0.39 | 64% | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pararas, N.; Pikouli, A.; Papaconstantinou, D.; Bagias, G.; Nastos, C.; Pikoulis, A.; Dellaportas, D.; Lykoudis, P.; Pikoulis, E. Colorectal Surgery in the COVID-19 Era: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 1229. https://doi.org/10.3390/cancers14051229
Pararas N, Pikouli A, Papaconstantinou D, Bagias G, Nastos C, Pikoulis A, Dellaportas D, Lykoudis P, Pikoulis E. Colorectal Surgery in the COVID-19 Era: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(5):1229. https://doi.org/10.3390/cancers14051229
Chicago/Turabian StylePararas, Nikolaos, Anastasia Pikouli, Dimitrios Papaconstantinou, Georgios Bagias, Constantinos Nastos, Andreas Pikoulis, Dionysios Dellaportas, Panagis Lykoudis, and Emmanouil Pikoulis. 2022. "Colorectal Surgery in the COVID-19 Era: A Systematic Review and Meta-Analysis" Cancers 14, no. 5: 1229. https://doi.org/10.3390/cancers14051229
APA StylePararas, N., Pikouli, A., Papaconstantinou, D., Bagias, G., Nastos, C., Pikoulis, A., Dellaportas, D., Lykoudis, P., & Pikoulis, E. (2022). Colorectal Surgery in the COVID-19 Era: A Systematic Review and Meta-Analysis. Cancers, 14(5), 1229. https://doi.org/10.3390/cancers14051229