
Low-Baseline PD1+ Granulocytes Predict Responses to Atezolizumab–Bevacizumab in Hepatocellular Carcinoma
 , ,
, ,  , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
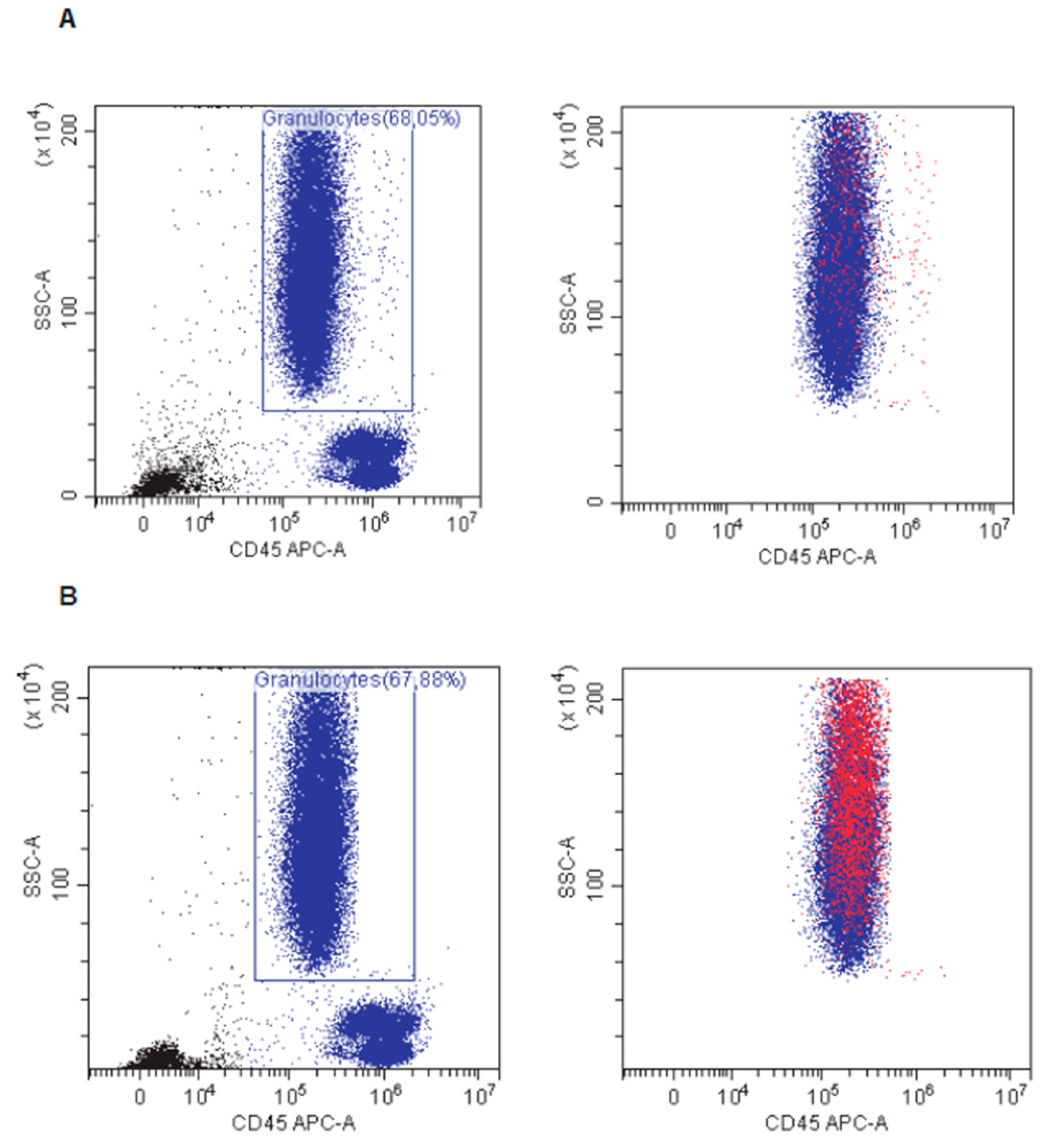
2.2. Analysis of Granulocyte Phenotype by Flow Cytometry
2.3. Statistical Analysis
3. Results
3.1. Intersample and Interday Reproducibility
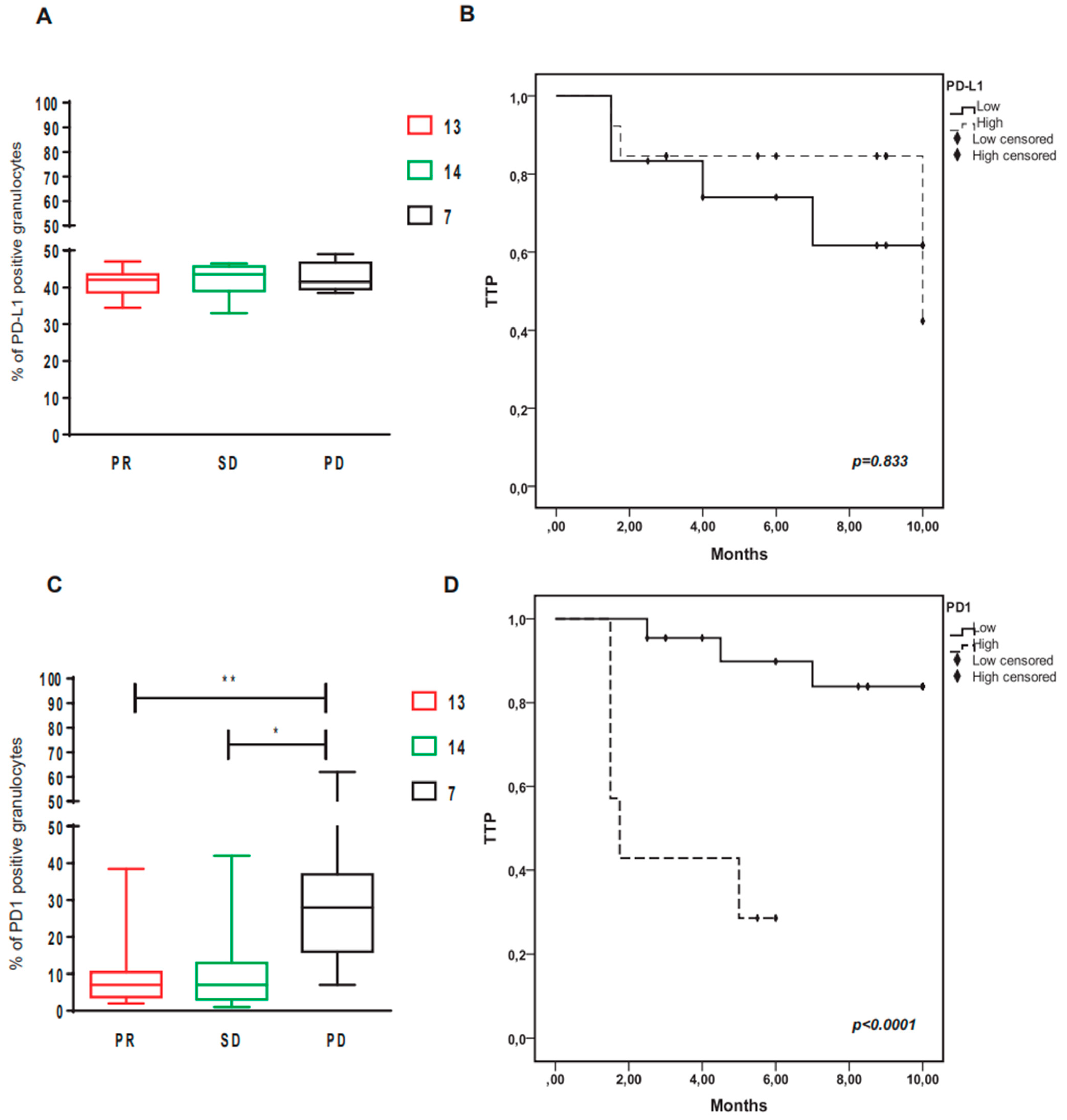
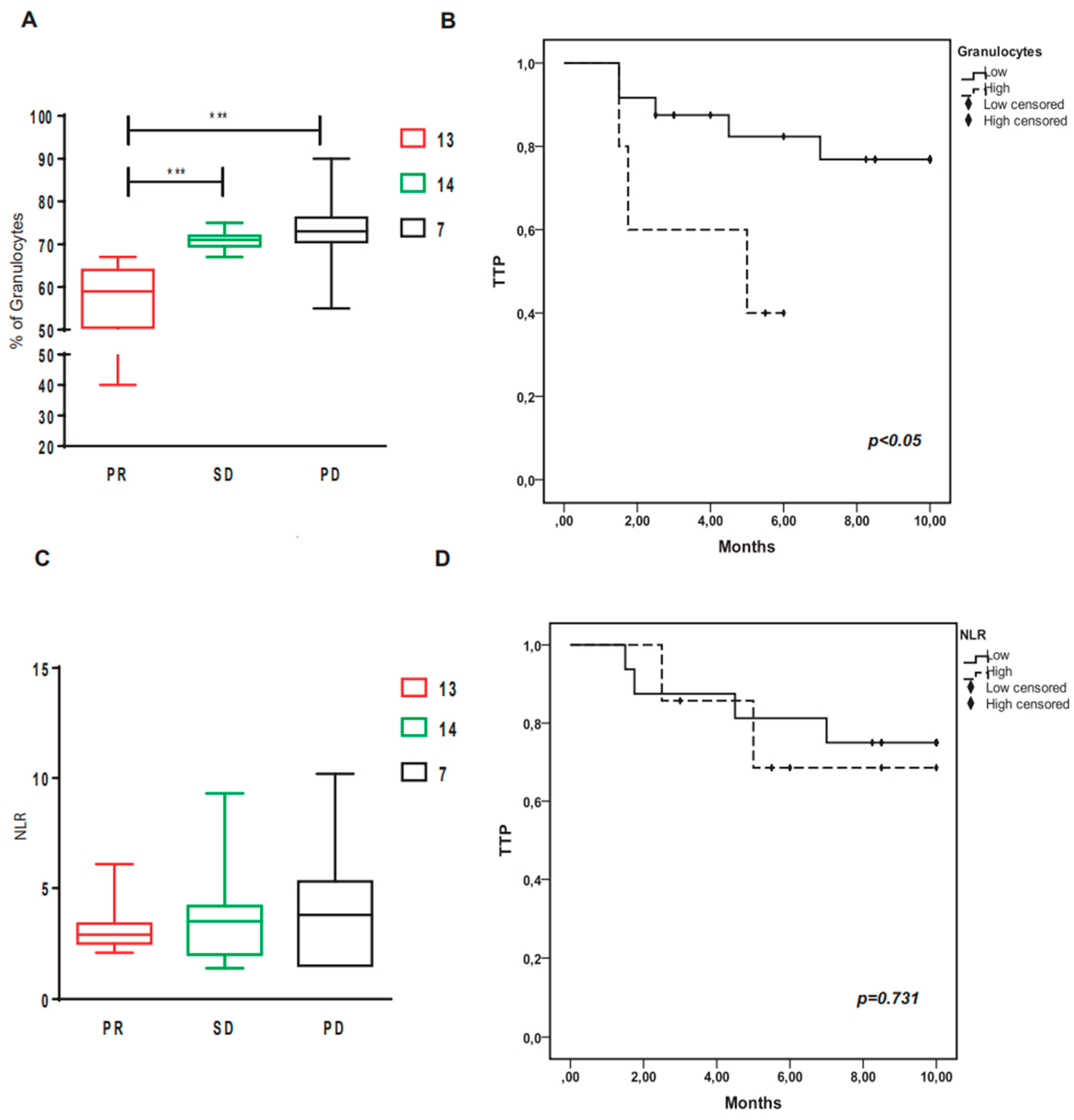
3.2. Low-Baseline PD1+ Granulocytes Predict Responses to Atezolizumab–Bevacizumb and a Longer TTP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Han, Y.; Liu, D.; Li, L. PD-1/PD-L1 pathway: Current researches in cancer. Am. J. Cancer Res. 2020, 10, 727–742. [Google Scholar] [PubMed]
- Lee, H.T.; Lee, J.Y.; Lim, H.; Lee, S.H.; Moon, Y.J.; Pyo, H.J.; Ryu, S.E.; Shin, W.; Heo, Y.S. Molecular mechanism of PD-1/PD-L1 blockade via anti-PD-L1 antibodies atezolizumab and durvalumab. Sci. Rep. 2017, 7, 5532. [Google Scholar] [CrossRef] [Green Version]
- Courau, T.; Nehar-Belaid, D.; Florez, L.; Levacher, B.; Vazquez, T.; Brimaud, F.; Bellier, B.; Klatzmann, D. TGF-beta and VEGF cooperatively control the immunotolerant tumor environment and the efficacy of cancer immunotherapies. JCI Insight 2016, 1, e85974. [Google Scholar] [CrossRef] [Green Version]
- Zhu, A.X.; Abbas, A.R.D.; de Galarreta, M.R.; Guan, Y.; Lu, S.; Koeppen, H.; Zhang, W.; Hsu, C.H.; He, A.R.; Ryoo, B.Y.; et al. Molecular correlates of clinical response and resistance to atezolizumab in combination with bevacizumab in advanced hepatocellular carcinoma. Nat. Med. 2022, 28, 1599–1611. [Google Scholar] [CrossRef]
- Giraud, J.; Chalopin, D.; Blanc, J.F.; Saleh, M. Hepatocellular Carcinoma Immune Landscape and the Potential of Immunotherapies. Front. Immunol. 2021, 12, 655697. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Jang, M.; Park, Y.N. Histopathological Variants of Hepatocellular:an update according to the 5th Edition of WHO Classifications of Digestive System tumors. J. Liver Cancer 2020, 20, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Arvanitakis, K.; Mitroulis, I.; Germanidis, G. Tumor-Associated Neutrophils in Hepatocellular Carcinoma Pathogenesis, Prognosis, and Therapy. Cancers 2021, 13, 2899. [Google Scholar] [CrossRef] [PubMed]
- Min, G.T.; Li, Y.M.; Yao, N.; Wang, J.; Wang, H.P.; Chen, W. The pretreatment neutrophil-lymphocyte ratio may predict prognosis of patients with liver cancer: A systematic review and meta-analysis. Clin. Transplant. 2018, 32, e13151. [Google Scholar] [CrossRef]
- Mouchli, M.; Reddy, S.; Gerrard, M.; Boardman, L.; Rubio, M. Usefulness of neutrophil-to-lymphocyte ratio (NLR) as a prognostic predictor after treatment of hepatocellular carcinoma. Ann. Hepatol. 2021, 22, 100249. [Google Scholar] [CrossRef]
- Eso, Y.; Takeda, H.; Taura, K.; Takai, A.; Takahashi, K.; Seno, H. Pretreatment Neutrophil-to-Lymphocyte Ratio as a Predictive Marker of Response to Atezolizumab Plus Bevacizumab for Hepatocellular Carcinoma. Curr. Oncol. 2021, 28, 4157–4166. [Google Scholar] [CrossRef]
- Dharmapuri, S.; Ozbek, U.; Lin, J.Y.; Sung, M.; Schwartz, M.; Branch, A.D.; Ang, C. Predictive value of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in advanced hepatocellular carcinoma patients treated with anti-PD-1 therapy. Cancer Med. 2020, 9, 4962–4970. [Google Scholar] [CrossRef]
- Strauss, L.; Mahmoud, M.A.A.; Weaver, J.D.; Tijaro-Ovalle, N.M.; Christofides, A.; Wang, Q.; Pal, R.; Yuan, M.; Asara, J.; Patsoukis, N.; et al. Targeted deletion of PD-1 in myeloid cells induces antitumor immunity. Sci. Immunol. 2020, 5, eaay1863. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Cagnon, L.; Costa-Nunes, C.M.; Baumgaertner, P.; Montandon, N.; Leyvraz, L.; Michielin, O.; Romano, E.; Speiser, D.E. Frequencies of circulating MDSC correlate with clinical outcome of melanoma patients treated with ipilimumab. Cancer Immunol. Immunother. CII 2014, 63, 247–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, R.; Fleming, V.; Hu, X.; Nagibin, V.; Groth, C.; Altevogt, P.; Utikal, J.; Umansky, V. Myeloid-Derived Suppressor Cells Hinder the Anti-Cancer Activity of Immune Checkpoint Inhibitors. Front. Immunol. 2018, 9, 1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwata, T.; Kondo, Y.; Kimura, O.; Morosawa, T.; Fujisaka, Y.; Umetsu, T.; Kogure, T.; Inoue, J.; Nakagome, Y.; Shimosegawa, T. PD-L1(+)MDSCs are increased in HCC patients and induced by soluble factor in the tumor microenvironment. Sci. Rep. 2016, 6, 39296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Sasikumar, P.G.; Sudarshan, N.S.; Adurthi, S.; Ramachandra, R.K.; Samiulla, D.S.; Lakshminarasimhan, A.; Ramanathan, A.; Chandrasekhar, T.; Dhudashiya, A.A.; Talapati, S.R.; et al. PD-1 derived CA-170 is an oral immune checkpoint inhibitor that exhibits preclinical anti-tumor efficacy. Commun. Biol. 2021, 4, 699. [Google Scholar] [CrossRef]
- Guo, L.; Overholser, J.; Good, A.J.; Ede, N.J.; Kaumaya, P.T.P. Preclinical Studies of a Novel Human PD-1 B-Cell Peptide Cancer Vaccine PD1-Vaxx From BALB/c Mice to Beagle Dogs and to Non-Human Primates (Cynomolgus Monkeys). Front. Oncol. 2022, 12, 826566. [Google Scholar] [CrossRef]
- Lee, C.K.; Chan, S.L.; Chon, H.J. Could We Predict the Response of Immune Checkpoint Inhibitor Treatment in Hepatocellular Carcinoma? Cancers 2022, 14, 3213. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fabrega, J.; Burrel, M.; Garcia-Criado, A.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.K.; Hubbard, M.; Jones, B.M. Use of CD45 fluorescence and side-scatter characteristics for gating lymphocytes when using the whole blood lysis procedure and flow cytometry. Cytometry 1996, 26, 16–21. [Google Scholar] [CrossRef]
- Ahmed, M.G.T.; Limmer, A.; Sucker, C.; Fares, K.M.; Mohamed, S.A.; Othman, A.H.; Berger, M.M.; Brenner, T.; Hartmann, M. Differential Regulation of CD45 Expression on Granulocytes, Lymphocytes, and Monocytes in COVID-19. J. Clin. Med. 2022, 11, 4219. [Google Scholar] [CrossRef] [PubMed]
- Fridlender, Z.G.; Albelda, S.M. Tumor-associated neutrophils: Friend or foe? Carcinogenesis 2012, 33, 949–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorch, S.K.; Kubes, P. An emerging role for neutrophil extracellular traps in noninfectious disease. Nat. Med. 2017, 23, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.Y.; Luo, Q.; Lu, L.; Zhu, W.W.; Sun, H.T.; Wei, R.; Lin, Z.F.; Wang, X.Y.; Wang, C.Q.; Lu, M.; et al. Increased neutrophil extracellular traps promote metastasis potential of hepatocellular carcinoma via provoking tumorous inflammatory response. J. Hematol. Oncol. 2020, 13, 3. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.T.; Zhao, Y.L.; Peng, L.S.; Chen, N.; Chen, W.; Lv, Y.P.; Mao, F.Y.; Zhang, J.Y.; Cheng, P.; Teng, Y.S.; et al. Tumour-activated neutrophils in gastric cancer foster immune suppression and disease progression through GM-CSF-PD-L1 pathway. Gut 2017, 66, 1900–1911. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.L.; Dai, Z.; Zhou, Z.J.; Wang, X.Y.; Yang, G.H.; Wang, Z.; Huang, X.W.; Fan, J.; Zhou, J. Overexpression of CXCL5 mediates neutrophil infiltration and indicates poor prognosis for hepatocellular carcinoma. Hepatology 2012, 56, 2242–2254. [Google Scholar] [CrossRef]
- He, G.; Zhang, H.; Zhou, J.; Wang, B.; Chen, Y.; Kong, Y.; Xie, X.; Wang, X.; Fei, R.; Wei, L.; et al. Peritumoural neutrophils negatively regulate adaptive immunity via the PD-L1/PD-1 signalling pathway in hepatocellular carcinoma. J. Exp. Clin. Cancer Res. CR 2015, 34, 141. [Google Scholar] [CrossRef] [Green Version]
- Advani, R.; Flinn, I.; Popplewell, L.; Forero, A.; Bartlett, N.L.; Ghosh, N.; Kline, J.; Roschewski, M.; LaCasce, A.; Collins, G.P.; et al. CD47 Blockade by Hu5F9-G4 and Rituximab in Non-Hodgkin’s Lymphoma. N. Engl. J. Med. 2018, 379, 1711–1721. [Google Scholar] [CrossRef]
- Zahid, K.R.; Raza, U.; Tumbath, S.; Jiang, L.; Xu, W.; Huang, X. Neutrophils: Musketeers against immunotherapy. Front. Oncol. 2022, 12, 975981. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient’s Characteristics | Atezolizumab+ Bevacizumab pts N = 34 | Response to Treatment PR/SD/PD | |
|---|---|---|---|
| Age (years old) | <65 years old ≥65 years old | 10 (29.4%) 24 (70.6%) | 4/3/3 9/11/4 |
| Gender | M F | 30 4 | 11/12/7 2/2/0 |
| ECOG PS | 0 1 | 28 (82.4%) 6 (17.6%) | 12/10/7 1/4/0 |
| Child-Pugh class | A B C | 33 (97.1%) 1 (2.9%) 0 | 12/14/7 1/0/0 0 |
| ALBI grade | 1 2 3 | 20 (58.8%) 14 (41.2%) 0 | 7/10/3 6/4/4 0 |
| BCLC stage | A B C | 0 14 20 | 0 4/7/3 9/7/4 |
| Etiology CLD | HBV active HCV cured HCV NASH/NAFLD alcohol | 3 (8.8%) 3 (8.8%) 10 (29.4%) 15 (44.1%) 3 (8.8%) | 0/1/2 2/1/0 6/2/2 3/9/3 2/1/0 |
| Nodularity | uninodular multinodular ≤3 multinodular >3 infiltrating | 9 5 10 10 | 4/3/2 1/3/1 4/4/2 4/4/2 |
| Size (main lesion in multinodular) | ≤3 cm 3–5 cm 5–10 cm >10 cm infiltrating (poorly defined) | 7 8 10 7 2 | |
| Portal vein invasion | yes no | 14 (41.2%) 20 (58.8%) | 6/4/4 7/10/3 |
| Extrahepatic spread | yes no | 11 (32.4%) 23 (67.6%) | 4/4/3 9/10/4 |
| AFP (ng/mL) | ≤20 21–400 ≥401 | 15 (44.1%) 13 (38.2%) 6 (17.6%) | 6/6/3 6/4/3 1/4/1 |
| Response to treatment | partial response stable disease progression | 13 14 7 |
| Blood Sample | PD1+% | PDL1+% | |
|---|---|---|---|
| Patient 1-T0 | A | 3% | 44% |
| Patient 1-T0 | B | 3% | 43% |
| Patient 2-T0 | A | 38% | 41% |
| Patient 2-T0 | B | 40% | 40% |
| Patient 3-T0 | A | 57% | 41% |
| Patient 3-T-1 | B | 60% | 39% |
| Patient 4-T0 | A | 15% | 36% |
| Patient 4-T-5 | B | 16% | 39% |
| Patient 5-T0 | A | 62% | 49% |
| Patient 5-T-5 | B | 58% | 46% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giovannini, C.; Suzzi, F.; Tovoli, F.; Bruccoleri, M.; Marseglia, M.; Alimenti, E.; Fornari, F.; Iavarone, M.; Piscaglia, F.; Gramantieri, L. Low-Baseline PD1+ Granulocytes Predict Responses to Atezolizumab–Bevacizumab in Hepatocellular Carcinoma. Cancers 2023, 15, 1661. https://doi.org/10.3390/cancers15061661
Giovannini C, Suzzi F, Tovoli F, Bruccoleri M, Marseglia M, Alimenti E, Fornari F, Iavarone M, Piscaglia F, Gramantieri L. Low-Baseline PD1+ Granulocytes Predict Responses to Atezolizumab–Bevacizumab in Hepatocellular Carcinoma. Cancers. 2023; 15(6):1661. https://doi.org/10.3390/cancers15061661
Chicago/Turabian StyleGiovannini, Catia, Fabrizia Suzzi, Francesco Tovoli, Mariangela Bruccoleri, Mariarosaria Marseglia, Eleonora Alimenti, Francesca Fornari, Massimo Iavarone, Fabio Piscaglia, and Laura Gramantieri. 2023. "Low-Baseline PD1+ Granulocytes Predict Responses to Atezolizumab–Bevacizumab in Hepatocellular Carcinoma" Cancers 15, no. 6: 1661. https://doi.org/10.3390/cancers15061661
APA StyleGiovannini, C., Suzzi, F., Tovoli, F., Bruccoleri, M., Marseglia, M., Alimenti, E., Fornari, F., Iavarone, M., Piscaglia, F., & Gramantieri, L. (2023). Low-Baseline PD1+ Granulocytes Predict Responses to Atezolizumab–Bevacizumab in Hepatocellular Carcinoma. Cancers, 15(6), 1661. https://doi.org/10.3390/cancers15061661