



Radiologic versus Segmentation Measurements to Quantify Wilms Tumor Volume on MRI in Pediatric Patients

 , , , ,
, , , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Magnetic Resonance Imaging
2.3. Tumor Volume Measurement
2.3.1. Radiological Tumor Volume Measurements
2.3.2. Manual Segmentation-Based Tumor Volume Measurements
- Manual indication of tumor and background on each fourth slice of the postcontrast T1-weighted scan, due to the best tumor and kidney contrast in this sequence.
- Initial tumor segmentation using the 3DSlicer algorithm “grow from seeds”, which is a 3D volume growing algorithm. After this step, each pixel was assigned either the label tumor or background.
- Because of the difference in in-slice resolution and slice thickness, the segmentation was reformatted from the T1-weighted image to the T2-weighted image using 3DSlicer’s inbuild function. These labels were extensively checked and manually corrected if needed.
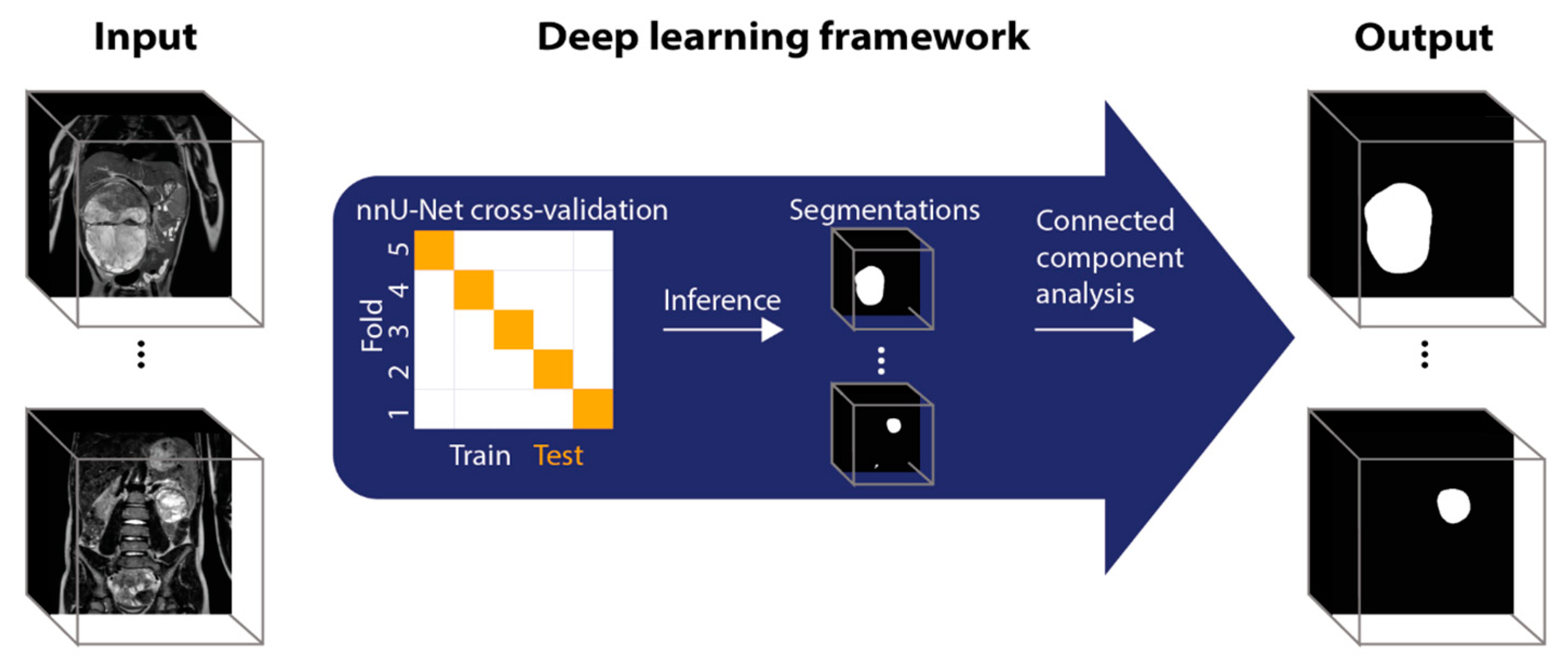
2.3.3. Deep Learning-Based Tumor Volume Measurements
2.4. Statistical Analysis
3. Results
3.1. Patients
3.1.1. Tumor Volume Measurements
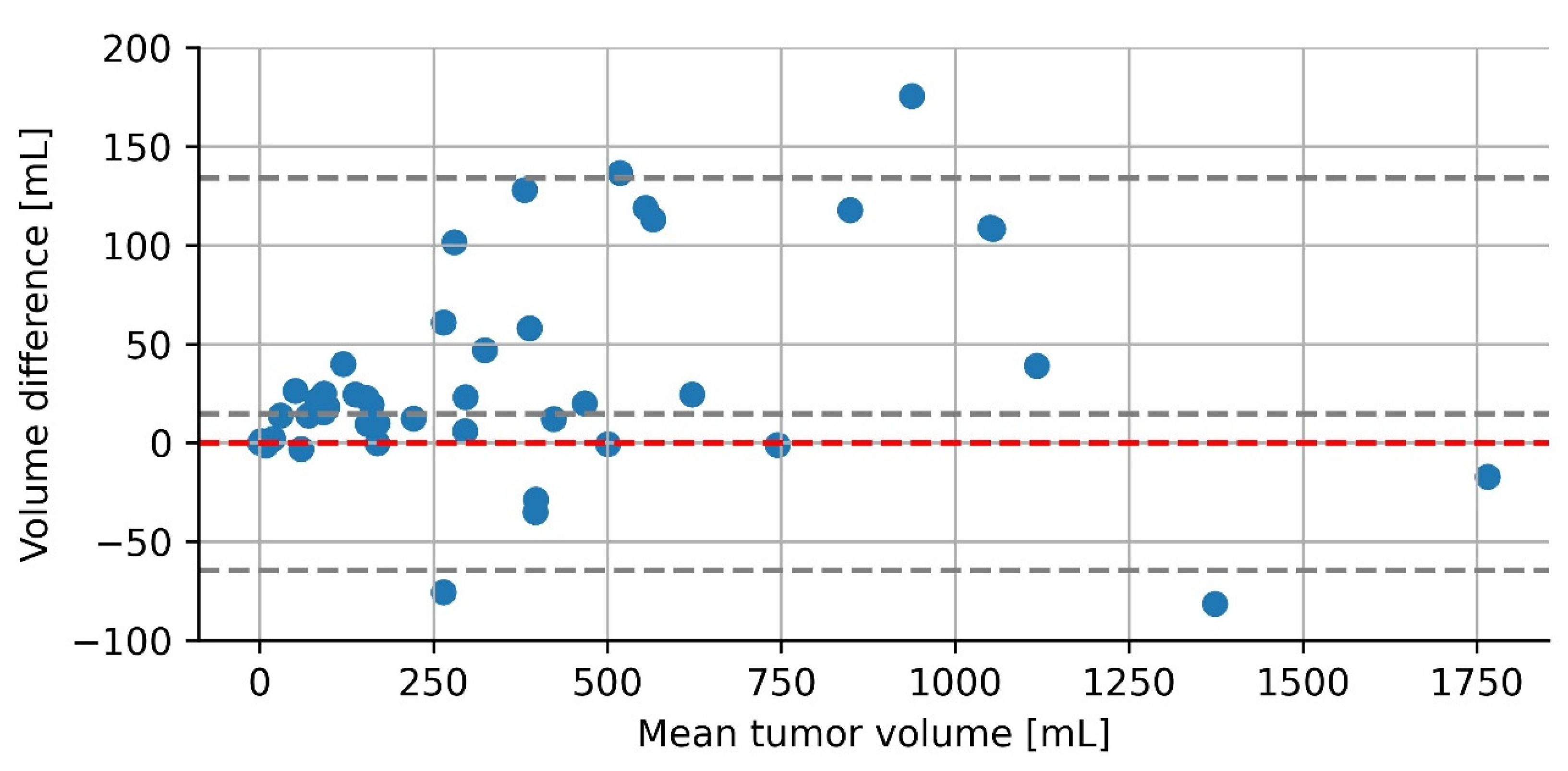
3.1.2. Radiological versus Manual Segmentation-Based Tumor Volume Measurements
3.1.3. Deep Learning-Based Segmentation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spreafico, F.; Bellani, F.F. Wilms’ tumor: Past, present and (possibly) future. Expert Rev. Anticancer Ther. 2006, 6, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Roy, P.; van Peer, S.E.; de Witte, M.M.; Tytgat, G.A.M.; Karim-Kos, H.E.; van Grotel, M.; van de Ven, C.P.; Mavinkurve-Groothuis, A.M.C.; Merks, J.H.M.; Kuiper, R.P.; et al. Characteristics and outcome of children with renal tumors in the Netherlands: The first five-year’s experience of national centralization. PLoS ONE 2022, 17, e0261729. [Google Scholar] [CrossRef] [PubMed]
- SIOP Renal Tumour Study Group. Paediatric renal tumours: Perspectives from the SIOP-RTSG. Nat. Rev. Urol. 2017, 14, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Vujanić, G.M.; Gessler, M.; Ooms, A.H.A.G.; Collini, P.; Coulomb-l’Hermine, A.; D’Hooghe, E.; de Krijger, R.R.; Perotti, D.; Pritchard-Jones, K.; Vokuhl, C.; et al. The UMBRELLA SIOP–RTSG 2016 Wilms tumour pathology and molecular biology protocol. Nat. Rev. Urol. 2018, 15, 693–701. [Google Scholar] [CrossRef] [Green Version]
- Van den Heuvel-Eibrink, M.M.; Hol, J.A.; Pritchard-Jones, K.; van Tinteren, H.; Furtwängler, R.; Verschuur, A.C.; Vujanic, G.M.; Leuschner, I.; Brok, J.; Rübe, C.; et al. Rationale for the treatment of Wilms tumour in the UMBRELLA SIOP–RTSG 2016 protocol. Nat. Rev. Urol. 2017, 14, 743–752. [Google Scholar] [CrossRef] [Green Version]
- Provenzi, V.O.; Rosa, R.F.M.; Rosa, R.C.M.; Roehe, A.V.; dos Santos, P.P.A.; Faulhaber, F.R.S.; de Oliveira, C.A.V.; Zen, P.R.G. Tumor size and prognosis in patients with Wilms tumor. Rev. Paul. Pediatr. 2015, 33, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Joseph, L.L.; Boddu, D.; Srinivasan, H.N.; Regi, S.S.; Antonisamy, B.; Matthew, L.G.; Totadri, S. Postchemotherapy tumor volume as a prognostic indicator in Wilms tumor: A single-center experience from South India. Pediatr. Blood Cancer 2022, 69, e29454. [Google Scholar] [CrossRef]
- Tirumani, S.H.; Shinagare, A.B.; O’Neill, A.C.; Nishino, M.; Rosenthal, M.H.; Ramaiya, N.H. Accuracy and Feasibility of Estimated Tumour Volumetry in Primary Gastric Gastrointestinal Stromal Tumours: Validation Using Semi-automated Technique in 127 Patients. Eur. Radiol. 2016, 26, 286–295. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J.; Kim, W. Method of tumor volume evaluation using magnetic resonance imaging for outcome prediction in cervical cancer treated with concurrent chemotherapy and radiotherapy. Radiat. Oncol. J. 2012, 30, 70–77. [Google Scholar] [CrossRef]
- Colvin, R.; Walker, D.; Hafron, J.; Seifman, B.; Nandalur, S.; Gangwish, D.; Nandalur, K.R. Which measurement method should be used for prostate volume for PI-RADS? A comparison of ellipsoid and segmentation methods. Clin. Imaging 2021, 80, 454–458. [Google Scholar] [CrossRef]
- Müller, S.; Farag, I.; Weickert, J.; Braun, Y.; Lollert, A.; Dobberstein, J.; Hötker, A.; Graf, N. Benchmarking Wilms’ tumor in multisequence MRI data: Why does current clinical practice fail? Which popular segmentation algorithms perform well? J. Med. Imaging 2019, 6, 034001. [Google Scholar] [CrossRef] [PubMed]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.W.M.; van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vujanić, G.M.; Sandstedt, B.; Kelsey, A.; Sebire, N.J. Central pathology review in multicenter trials and studies. Cancer 2009, 115, 1977–1983. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Medical Image Computing and Computer-Assisted Intervention–MICCAI 2015: 18th International Conference, Munich, Germany, 5–9 October 2015, Proceedings, Part III 18; Springer: Berlin/Heidelberg, Germany, 2015; Volume 9351, pp. 234–241. [Google Scholar]
- Berrar, D. Cross-Validation. Ref. Modul. Life Sci. 2019, 1, 542–545. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Measurement in Medicine: The Analysis of Method Comparison Studies. J. R. Stat. Soc. Ser. Stat. 1983, 32, 307–317. [Google Scholar] [CrossRef]
- Dewitte, K.; Fierens, C.; Stöckl, D.; Thienpont, L.M. Application of the Bland–Altman Plot for Interpretation of Method-Comparison Studies: A Critical Investigation of Its Practice. Clin. Chem. 2002, 48, 799–801. [Google Scholar] [CrossRef]
- Taha, A.A.; Hanbury, A. Metrics for evaluating 3D medical image segmentation: Analysis, selection, and tool. BMC Med. Imaging 2015, 15, 29. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.H.; Shu, L.; Jia, X.; Zhou, H.C.; Liu, T.T.; Liang, J.W.; Ding, Y.S.; He, M.; Shu, Q. Machine Learning-Based CT Radiomics Method for Identifying the Stage of Wilms Tumor in Children. Front Pediatr. 2022, 10, 873035. [Google Scholar] [CrossRef]
- Fitski, M.; Meulstee, J.W.; Littooij, A.S.; van der Ven, C.P.; van der Steeg, A.F.W.; Wijnen, M.H.W.A. MRI-Based 3-Dimensional Visualization Workflow for the Preoperative Planning of Nephron-Sparing Surgery in Wilms’ Tumor Surgery: A Pilot Study. J. Healthc. Eng. 2020, 2020, 8899049. [Google Scholar] [CrossRef]
- Chaussy, Y.; Vieille, L.; Lacroix, E.; Lenoir, M.; Marie, F.; Corbat, L.; Henriet, J.; Auber, F. 3D reconstruction of Wilms’ tumor and kidneys in children: Variability, usefulness and constraints. J. Pediatr. Urol. 2020, 16, 830.e1–830.e8. [Google Scholar] [CrossRef] [PubMed]
- Reinke, A.; Tizabi, M.D.; Sudre, C.; Eisenmann, M.; Rädsch, T.; Baumgartner, M.; Acion, L.; Antonelli, M.; Arbel, T.; Bakas, S.; et al. Common Limitations of Image Processing Metrics: A Picture Story. arXiv 2021, arXiv:2104.05642. [Google Scholar]
- Van Peer, S.E.; Hol, J.A.; van der Steeg, A.F.W.; van Grotel, M.; Tytgat, G.A.M.; Mavinkurve-Groothuis, A.M.C.; Janssens, G.O.R.; Littooij, A.S.; de Krijger, R.R.; Jongemans, M.C.J.; et al. Bilateral Renal Tumors in Children: The First 5 Years’ Experience of National Centralization in The Netherlands and a Narrative Review of the Literature. J. Clin. Med. 2021, 10, 5558. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | T1-Weighted with Fat Suppression | 3D T2-Weighted |
|---|---|---|
| Sequence type | Gradient Echo | Turbo Spin Echo |
| Repetition time (ms) | 5.5 | 459 |
| Echo time (ms) | 2.7 | 90 |
| Flip angle | 10° | 90° |
| Slice thickness (mm) | 3.0 | 1.15 |
| Voxel spacing (mm) | 0.74 × 0.74 mm2 | 0.83 × 0.83 mm2 |
| Characteristic | Value | |
|---|---|---|
| Median age at diagnosis in months (min–max) | 39 (7–109) | |
| Gender | Male Female | 22 (49%) 23 (51%) |
| Tumor localization | Bilateral Left Right | 6 (13%) 16 (36%) 23 (51%) |
| Characteristics | Value | |
|---|---|---|
| Histological tumor type | Regressive Non-regressive
Completely necrotic Nephrogenic rest Unknown | 14 (27%) 13 (25%) 9 (17%) 2 (4%) 1 (2%) 5 (10%) 2 (4%) 1 (2%) 5 (10%) |
| Median radiological volume [mL] (range) | 215 (0.68–1774) |
| Volume Tumor | Absolute Difference (Mean) | p-Value | Percentage Difference (Mean) | p-Value |
|---|---|---|---|---|
| 0–300 mL | 5.6 | 0.01 | 11.9 | 0.95 |
| 300–500 mL | 21.5 | 9.1 | ||
| >500 mL | 70.2 | 9.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buser, M.A.D.; van der Steeg, A.F.W.; Wijnen, M.H.W.A.; Fitski, M.; van Tinteren, H.; van den Heuvel-Eibrink, M.M.; Littooij, A.S.; van der Velden, B.H.M. Radiologic versus Segmentation Measurements to Quantify Wilms Tumor Volume on MRI in Pediatric Patients. Cancers 2023, 15, 2115. https://doi.org/10.3390/cancers15072115
Buser MAD, van der Steeg AFW, Wijnen MHWA, Fitski M, van Tinteren H, van den Heuvel-Eibrink MM, Littooij AS, van der Velden BHM. Radiologic versus Segmentation Measurements to Quantify Wilms Tumor Volume on MRI in Pediatric Patients. Cancers. 2023; 15(7):2115. https://doi.org/10.3390/cancers15072115
Chicago/Turabian StyleBuser, Myrthe A. D., Alida F. W. van der Steeg, Marc H. W. A. Wijnen, Matthijs Fitski, Harm van Tinteren, Marry M. van den Heuvel-Eibrink, Annemieke S. Littooij, and Bas H. M. van der Velden. 2023. "Radiologic versus Segmentation Measurements to Quantify Wilms Tumor Volume on MRI in Pediatric Patients" Cancers 15, no. 7: 2115. https://doi.org/10.3390/cancers15072115
APA StyleBuser, M. A. D., van der Steeg, A. F. W., Wijnen, M. H. W. A., Fitski, M., van Tinteren, H., van den Heuvel-Eibrink, M. M., Littooij, A. S., & van der Velden, B. H. M. (2023). Radiologic versus Segmentation Measurements to Quantify Wilms Tumor Volume on MRI in Pediatric Patients. Cancers, 15(7), 2115. https://doi.org/10.3390/cancers15072115