
Folate–Methionine Cycle Disruptions in ASD Patients and Possible Interventions: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
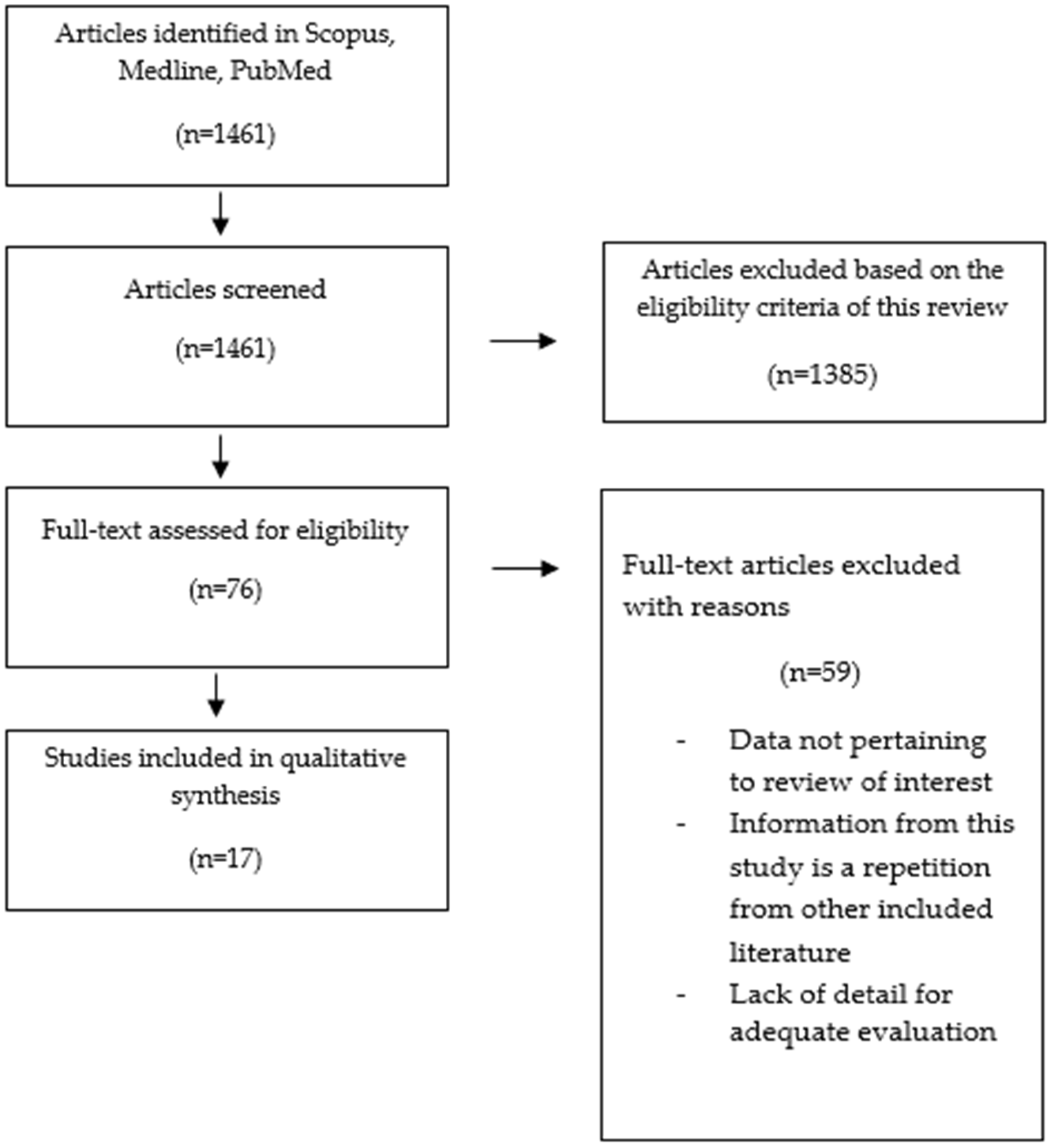
2.3. Literature Search and Selection of Articles
2.4. Data Extraction
2.5. Risk of Bias across Studies
3. Results
3.1. Overall Results
3.2. Summary of the Results Included in This Systematic Review
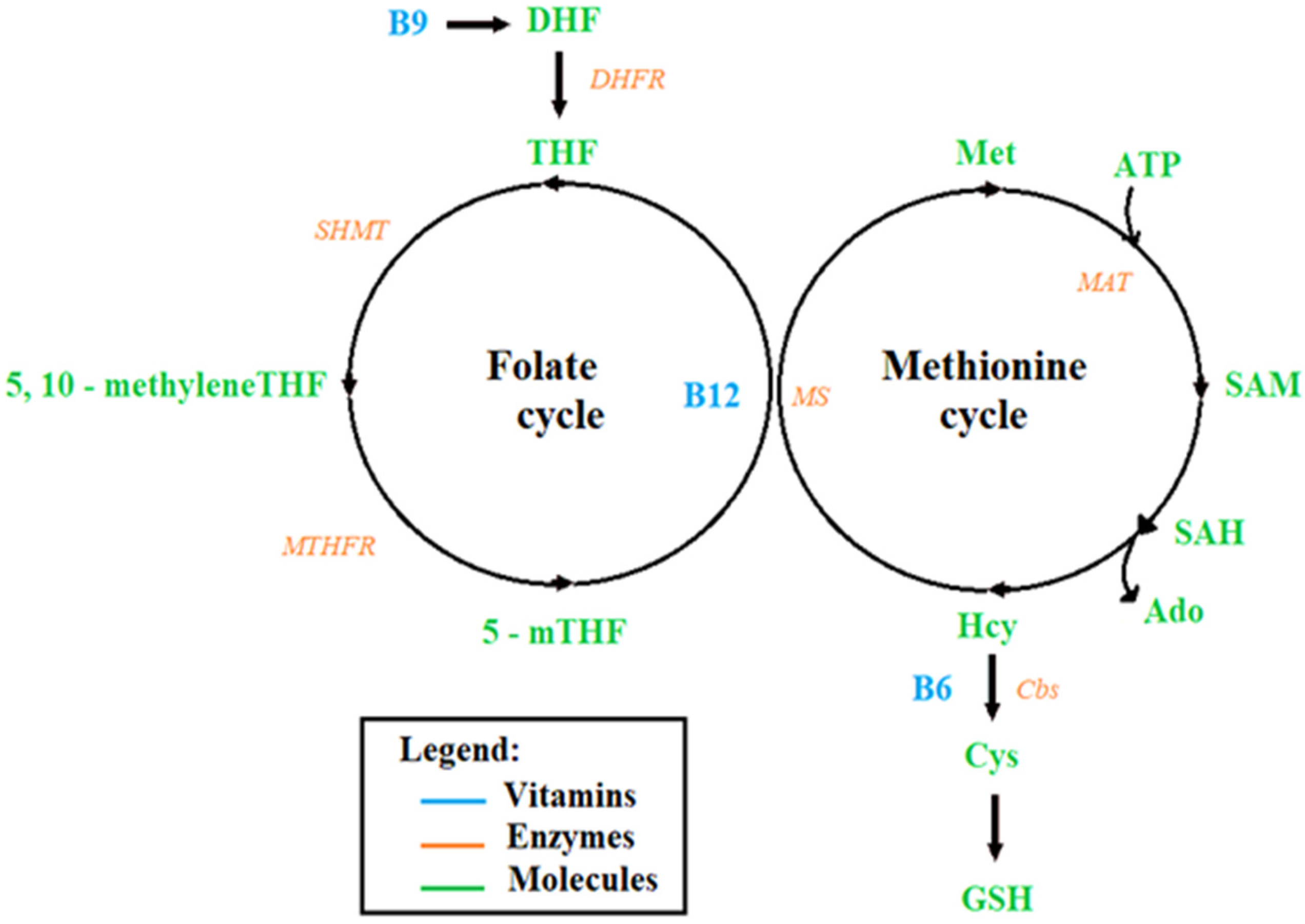
3.3. Perturbations of the Folate–Methionine Cycle in Individuals with ASD
3.3.1. Studies on the Deficiency of B Vitamins in ASD Children
3.3.2. Causes of These Perturbations
Studies on the Poor Dietary Intake of ASD Children
Studies on the Genetic Predisposition of ASD
3.3.3. Possible Interventions
Studies on the Effect of Folate and Vitamin B12 Supplementation in ASD Children
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zeidan, J.; Fombonne, E.; Scorah, J.; Ibrahim, A.; Durkin, M.S.; Saxena, S.; Yusuf, A.; Shih, A.; Elsabbagh, M. Global prevalence of autism: A systematic review update. Autism Res. 2022, 15, 778–790. [Google Scholar] [CrossRef]
- Eissa, N.; Al-Houqani, M.; Sadeq, A.; Ojha, S.K.; Sasse, A.; Sadek, B. Current Enlightenment About Etiology and Pharmacological Treatment of Autism Spectrum Disorder. Front. Neurosci. 2018, 12, 304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaaya, M.; Saab, D.; Maalouf, F.T.; Boustany, R.-M. Prevalence of Autism Spectrum Disorder in Nurseries in Lebanon: A Cross Sectional Study. J. Autism Dev. Disord. 2016, 46, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Hodges, H.; Fealko, C.; Soares, N. Autism spectrum disorder: Definition, epidemiology, causes, and clinical evaluation. Transl. Pediatr. 2020, 9, S55–S65. [Google Scholar] [CrossRef] [PubMed]
- Hnoonual, A.; Thammachote, W.; Tim-Aroon, T.; Rojnueangnit, K.; Hansakunachai, T.; Sombuntham, T.; Roongpraiwan, R.; Worachotekamjorn, J.; Chuthapisith, J.; Fucharoen, S.; et al. Chromosomal microarray analysis in a cohort of underrepresented population identifies SERINC2 as a novel candidate gene for autism spectrum disorder. Sci. Rep. 2017, 7, 12096. [Google Scholar] [CrossRef] [Green Version]
- Bitar, T.; Hleihel, W.; Marouillat, S.; Vonwill, S.; Vuillaume, M.-L.; Soufia, M.; Vourc’h, P.; Laumonnier, F.; Andres, C.R. Identification of rare copy number variations reveals PJA2, APCS, SYNPO, and TAC1 as novel candidate genes in Autism Spectrum Disorders. Mol. Genet. Genom. Med. 2019, 7, e786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soueid, J.; Kourtian, S.; Makhoul, N.J.; Makoukji, J.; Haddad, S.; Ghanem, S.S.; Kobeissy, F.; Boustany, R.-M. RYR2, PTDSS1 and AREG genes are implicated in a Lebanese population-based study of copy number variation in autism. Sci. Rep. 2016, 6, 19088. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.Y.; Son, M.J.; Son, C.Y.; Radua, J.; Eisenhut, M.; Gressier, F.; Koyanagi, A.; Carvalho, A.F.; Stubbs, B.; Solmi, M.; et al. Environmental risk factors and biomarkers for autism spectrum disorder: An umbrella review of the evidence. Lancet Psychiatry 2019, 6, 590–600. [Google Scholar] [CrossRef] [Green Version]
- Gerges, P.; Bitar, T.; Hawat, M.; Alameddine, A.; Soufia, M.; Andres, C.R.; Hleihel, W. Risk and Protective Factors in Autism Spectrum Disorders: A Case Control Study in the Lebanese Population. Int. J. Environ. Res. Public Health 2020, 17, 6323. [Google Scholar] [CrossRef]
- Ming, X.; Stein, T.P.; Barnes, V.; Rhodes, N.; Guo, L. Metabolic Perturbance in Autism Spectrum Disorders: A Metabolomics Study. Available online: https://pubs.acs.org/doi/pdf/10.1021/pr300910n (accessed on 20 June 2022).
- Bitar, T.; Mavel, S.; Emond, P.; Nadal-Desbarats, L.; Lefèvre, A.; Mattar, H.; Soufia, M.; Blasco, H.; Vourc’h, P.; Hleihel, W.; et al. Identification of metabolic pathway disturbances using multimodal metabolomics in autistic disorders in a Middle Eastern population. J. Pharm. Biomed. Anal. 2018, 152, 57–65. [Google Scholar] [CrossRef]
- Han, Y.; Xi, Q.; Dai, W.; Yang, S.; Gao, L.; Su, Y.; Zhang, X. Abnormal transsulfuration metabolism and reduced antioxidant capacity in Chinese children with autism spectrum disorders. Int. J. Dev. Neurosci. 2015, 46, 27–32. [Google Scholar] [CrossRef] [PubMed]
- James, S.J.; Cutler, P.; Melnyk, S.; Jernigan, S.; Janak, L.; Gaylor, D.W.; Neubrander, J.A. Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am. J. Clin. Nutr. 2004, 80, 1611–1617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belardo, A.; Gevi, F.; Zolla, L. The concomitant lower concentrations of vitamins B6, B9 and B12 may cause methylation deficiency in autistic children. J. Nutr. Biochem. 2019, 70, 38–46. [Google Scholar] [CrossRef]
- Orozco, J.S.; Hertz-Picciotto, I.; Abbeduto, L.; Slupsky, C.M. Metabolomics analysis of children with autism, idiopathic-developmental delays, and Down syndrome. Transl. Psychiatry 2019, 9, 243. [Google Scholar] [CrossRef] [Green Version]
- Lyon, P.; Strippoli, V.; Fang, B.; Cimmino, L. B Vitamins and One-Carbon Metabolism: Implications in Human Health and Disease. Nutrients 2020, 12, 2867. [Google Scholar] [CrossRef] [PubMed]
- Main, P.A.; Angley, M.T.; Thomas, P.; O’Doherty, C.E.; Fenech, M. Folate and methionine metabolism in autism: A systematic review. Am. J. Clin. Nutr. 2010, 91, 1598–1620. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Palfrey, H.A.; Pathak, R.; Kadowitz, P.J.; Gettys, T.W.; Murthy, S.N. The metabolism and significance of homocysteine in nutrition and health. Nutr. Metab. 2017, 14, 78. [Google Scholar] [CrossRef] [Green Version]
- Clare, C.E.; Brassington, A.H.; Kwong, W.Y.; Sinclair, K.D. One-Carbon Metabolism: Linking Nutritional Biochemistry to Epigenetic Programming of Long-Term Development. Annu. Rev. Anim. Biosci. 2019, 7, 263–287. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zou, M.; Sun, C.; Wu, L.; Chen, W.-X. Prenatal Folic Acid Supplements and Offspring’s Autism Spectrum Disorder: A Meta-analysis and Meta-regression. J. Autism Dev. Disord. 2022, 52, 522–539. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [Green Version]
- Hoxha, B.; Hoxha, M.; Domi, E.; Gervasoni, J.; Persichilli, S.; Malaj, V.; Zappacosta, B. Folic Acid and Autism: A Systematic Review of the Current State of Knowledge. Cells 2021, 10, 1976. [Google Scholar] [CrossRef]
- Alahmari, S.; Alatawi, R.; Albalawi, R.; Albalawi, R.; Alamri, E. Nutritional status among children with autism spectrum disorders in Saudi Arabia. Med. Sci. 2022, 26, e1960. [Google Scholar] [CrossRef]
- Esteban-Figuerola, P.; Canals, J.; Fernández-Cao, J.C.; Arija Val, V. Differences in food consumption and nutritional intake between children with autism spectrum disorders and typically developing children: A meta-analysis. Autism 2019, 23, 1079–1095. [Google Scholar] [CrossRef] [PubMed]
- Barnhill, K.; Gutierrez, A.; Ghossainy, M.; Marediya, Z.; Devlin, M.; Sachdev, P.; Marti, C.N.; Hewitson, L. Dietary status and nutrient intake of children with autism spectrum disorder: A case-control study. Res. Autism Spectr. Disord. 2018, 50, 51–59. [Google Scholar] [CrossRef]
- Plaza-Diaz, J.; Flores-Rojas, K.; de la Torre-Aguilar, M.J.; Gomez-Fernández, A.R.; Martín-Borreguero, P.; Perez-Navero, J.L.; Gil, A.; Gil-Campos, M. Dietary Patterns, Eating Behavior, and Nutrient Intakes of Spanish Preschool Children with Autism Spectrum Disorders. Nutrients 2021, 13, 3551. [Google Scholar] [CrossRef] [PubMed]
- Chistol, L.T.; Bandini, L.G.; Must, A.; Phillips, S.; Cermak, S.A.; Curtin, C. Sensory sensitivity and food selectivity in children with autism spectrum disorder. J. Autism Dev. Disord. 2018, 48, 583–591. [Google Scholar] [CrossRef]
- Adams, S.N.; Verachia, R.; Coutts, K. Mealtime challenges and food selectivity in children with autism spectrum disorder in South Africa. S. Afr. J. Clin. Nutr. 2022, 35, 78–84. [Google Scholar] [CrossRef]
- Molina-López, J.; Leiva-García, B.; Planells, E.; Planells, P. Food selectivity, nutritional inadequacies, and mealtime behavioral problems in children with autism spectrum disorder compared to neurotypical children. Int. J. Eat Disord. 2021, 54, 2155–2166. [Google Scholar] [CrossRef]
- Li, C.-X.; Liu, Y.-G.; Che, Y.-P.; Ou, J.-L.; Ruan, W.-C.; Yu, Y.-L.; Li, H.-F. Association between MTHFR C677T Polymorphism and Susceptibility to Autism Spectrum Disorders: A Meta-Analysis in Chinese Han Population. Front. Pediatr. 2021, 9, 598805. [Google Scholar] [CrossRef]
- El-baz, F.; El-Aal, M.A.; Kamal, T.M.; Sadek, A.A.; Othman, A.A. Study of the C677T and 1298AC polymorphic genotypes of MTHFR Gene in autism spectrum disorder. Electron. Physician 2017, 9, 5287–5293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Omari, L.M.; Hunaiti, A.A.; Beirat, M.A.; Bustanji, Y.K. Study of MTHFR C677T Polymorphism and Associated Oxidative Stress Biomarkers among Autism Spectrum Disorder Patients in Jordan. Jordan J. Biol. Sci. 2020, 13, 247–252. [Google Scholar]
- Li, Y.; Qiu, S.; Shi, J.; Guo, Y.; Li, Z.; Cheng, Y.; Liu, Y. Association between MTHFR C677T/A1298C and susceptibility to autism spectrum disorders: A meta-analysis. BMC Pediatr. 2020, 20, 449. [Google Scholar] [CrossRef] [PubMed]
- Sadeghiyeh, T.; Dastgheib, S.A.; Mirzaee-Khoramabadi, K.; Morovati-Sharifabad, M.; Akbarian-Bafghi, M.J.; Poursharif, Z.; Mirjalili, S.R.; Neamatzadeh, H. Association of MTHFR 677C>T and 1298A>C polymorphisms with susceptibility to autism: A systematic review and meta-analysis. Asian J. Psychiatry 2019, 46, 54–61. [Google Scholar] [CrossRef]
- Razi, B.; Imani, D.; Hassanzadeh Makoui, M.; Rezaei, R.; Aslani, S. Association between MTHFR gene polymorphism and susceptibility to autism spectrum disorders: Systematic review and meta-analysis. Res. Autism Spectr. Disord. 2020, 70, 101473. [Google Scholar] [CrossRef]
- Muftin, N.Q.; Jubair, S.; Hadi, S.M. Identification of MTHFR genetic polymorphism in Iraqi autistic children. Gene Rep. 2020, 18, 100585. [Google Scholar] [CrossRef]
- Sun, C.; Zou, M.; Zhao, D.; Xia, W.; Wu, L. Efficacy of Folic Acid Supplementation in Autistic Children Participating in Structured Teaching: An Open-Label Trial. Nutrients 2016, 8, 337. [Google Scholar] [CrossRef] [Green Version]
- Čorejová, A.; Fazekaš, T.; Jánošíková, D.; Repiský, J.; Pospíšilová, V.; Miková, M.; Rauová, D.; Ostatníková, D.; Kyselovič, J.; Hrabovská, A. Improvement of the Clinical and Psychological Profile of Patients with Autism after Methylcobalamin Syrup Administration. Nutrients 2022, 14, 2035. [Google Scholar] [CrossRef] [PubMed]
- Hendren, R.L.; James, S.J.; Widjaja, F.; Lawton, B.; Rosenblatt, A.; Bent, S. Randomized, Placebo-Controlled Trial of Methyl B12 for Children with Autism. J. Child Adolesc. Psychopharmacol. 2016, 26, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Altun, H.; Kurutaş, E.B.; Şahin, N.; Güngör, O.; Fındıklı, E. The Levels of Vitamin D, Vitamin D Receptor, Homocysteine and Complex B Vitamin in Children with Autism Spectrum Disorders. Clin. Psychopharmacol. Neurosci. 2018, 16, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Yektaş, Ç.; Alpay, M.; Tufan, A.E. Comparison of serum B12, folate and homocysteine concentrations in children with autism spectrum disorder or attention deficit hyperactivity disorder and healthy controls. Neuropsychiatr. Dis. Treat 2019, 15, 2213–2219. [Google Scholar] [CrossRef] [Green Version]
- Marí-Bauset, S.; Zazpe, I.; Mari-Sanchis, A.; Llopis-González, A.; Morales Suárez-Varela, M. Food Selectivity in Autism Spectrum Disorders: A Systematic Review. J. Child Neurol. 2013, 29, 1718–1727. [Google Scholar] [CrossRef]
- Al-Batayneh, K.M.; Zoubi, M.S.A.; Shehab, M.; Al-Trad, B.; Bodoor, K.; Khateeb, W.A.; Aljabali, A.A.A.; Hamad, M.A.; Eaton, G. Association between MTHFR 677C>T Polymorphism and Vitamin B12 Deficiency: A Case-control Study. J. Med. Biochem. 2018, 37, 141–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghubeer, S.; Matsha, T.E. Methylenetetrahydrofolate (MTHFR), the One-Carbon Cycle, and Cardiovascular Risks. Nutrients 2021, 13, 4562. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Zhu, Y.; Wang, T.; Zhang, X.; Zhang, K.; Zhang, Z. Genetic risk factors for autism-spectrum disorders: A systematic review based on systematic reviews and meta-analysis. J. Neural Transm. 2021, 128, 717–734. [Google Scholar] [CrossRef]
- Fan, S.; Yang, B.; Zhi, X.; Wang, Y.; Zheng, Q.; Sun, G. Combined genotype and haplotype distributions of MTHFR C677T and A1298C polymorphisms. Medicine 2016, 95, e5355. [Google Scholar] [CrossRef] [PubMed]
- Tisato, V.; Silva, J.A.; Longo, G.; Gallo, I.; Singh, A.V.; Milani, D.; Gemmati, D. Genetics and epigenetics of one-carbon metabolism pathway in autism spectrum disorder: A sex-specific brain epigenome? Genes 2021, 12, 782. [Google Scholar] [CrossRef]
- Li, Y.; Li, Y.-M.; Xiang, D. Supplement intervention associated with nutritional deficiencies in autism spectrum disorders: A systematic review. Eur. J. Nutr. 2018, 57, 2571–2582. [Google Scholar] [CrossRef]
- Al-Beltagy, S.; El-Serogy, H.; Elaziz, S.; Al-Gohary, T. A Study of Plasma Homocysteine Level in Children with Autism. Asian J. Pediatr. Res. 2022, 10, 31–37. [Google Scholar] [CrossRef]
- Frye, R.E.; DeLaTorre, R.; Taylor, H.; Slattery, J.; Melnyk, S.; Chowdhury, N.; James, S.J. Redox metabolism abnormalities in autistic children associated with mitochondrial disease. Transl. Psychiatry 2013, 3, e273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawat, S.; Nagpal, J.; Jain, T. Role of Vitamin B12 in Autistic Spectrum and Attention Deficit Hyperactivity Disorders: A Scoping Review. Indian J. Nutr. 2021, 8, 243. [Google Scholar]
- O’Leary, F.; Samman, S. Vitamin B12 in Health and Disease. Nutrients 2010, 2, 299–316. [Google Scholar] [CrossRef] [Green Version]
- Robea, M.-A.; Luca, A.-C.; Ciobica, A. Relationship between Vitamin Deficiencies and Co-Occurring Symptoms in Autism Spectrum Disorder. Medicina 2020, 56, 245. [Google Scholar] [CrossRef]
- Parra, M.; Stahl, S.; Hellmann, H. Vitamin B6 and Its Role in Cell Metabolism and Physiology. Cells 2018, 7, 84. [Google Scholar] [CrossRef] [Green Version]
- Frye, R.E.; Slattery, J.C.; Quadros, E.V. Folate metabolism abnormalities in autism: Potential biomarkers. Biomark. Med. 2017, 11, 687–699. [Google Scholar] [CrossRef] [Green Version]
- Balashova, O.A.; Visina, O.; Borodinsky, L.N. Folate Action in Nervous System Development and Disease. Dev. Neurobiol. 2018, 78, 391–402. [Google Scholar] [CrossRef]
- Zulkifli, M.N.; Kadar, M.; Fenech, M.; Hamzaid, N.H. Interrelation of food selectivity, oral sensory sensitivity, and nutrient intake in children with autism spectrum disorder: A scoping review. Res. Autism Spectr. Disord. 2022, 93, 101928. [Google Scholar] [CrossRef]
- Baraskewich, J.; von Ranson, K.M.; McCrimmon, A.; McMorris, C.A. Feeding and eating problems in children and adolescents with autism: A scoping review. Autism 2021, 25, 1505–1519. [Google Scholar] [CrossRef] [PubMed]
- Vissoker, R.E.; Latzer, Y.; Gal, E. Eating and feeding problems and gastrointestinal dysfunction in Autism Spectrum Disorders. Res. Autism Spectr. Disord. 2015, 12, 10–21. [Google Scholar] [CrossRef]
- Suman, P.; Kumar, P. Clinical Relevance of Methylenetetrahydrofolate Reductase Genetic Testing in Autism: A Case Report of Successful Clinical Outcome. Cureus 2021, 13, e12586. [Google Scholar] [CrossRef]
- Gowda, V.K.; Srinivasan, V.M. A Treatable Cause of Global Developmental Delay with Autism Spectrum Disorder Due to Cobalamin Related Remethylation Disorder. Indian J. Pediatr. 2022, 89, 832. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No | Study | Type of Study | Sample Size | Age | Aim of the Study | Study Outcomes Parameters | Outcomes |
|---|---|---|---|---|---|---|---|
| 1 | S. Alahmari et al. (2022) [23] | Case control study | 155 children (70 children with ASD and 85 children without ASD) | 7–12 years old | Compare the nutritional status of Saudi children with autism spectrum disorders (ASD) to Saudi children without ASD | Dietary consumption using a 3-day food record (daily average of energy, intake of folic acid, vitamin B12, calcium, iron, magnesium, sodium, selenium vitamin B6, vitamin C) | The daily average of energy from carbohydrates was significantly higher among children with ASD than among children without ASD. A lower intake of folic acid, vitamin B12, calcium, iron, magnesium, sodium, and selenium was detected among children with ASD, while vitamin B6, vitamin C, and potassium were significantly higher among children with ASD compared to children without ASD [23]. |
| 2 | Esteban-Figuerola et al. (2020) [24] | Meta-analysis | - | - | Determine the overall differences in nutritional intake and food consumption between children with autism spectrum disorder and control (typical development) children | Food record (calcium, vitamin B12, vitamin D, vitamin E, calcium, selenium, phosphorus, thiamine, riboflavin | Children with ASD consume less protein, vitamin D, vitamin B12, omega-3, calcium, phosphorus, selenium, thiamine and riboflavin than controls [24] |
| 3 | K Barnhill et al. (2018) [25] | Case control study | 86 children with ASD aged 57 age-matched peers without ASD. | 2–8 years old | Compare dietary intake in 2-to-8-year-old US children with and without an ASD diagnosis | Food record (energy, protein, carbohydrate, vitamin B6, vitamin B, vitamin A, vitamin D, folic acid) | Children with ASD consumed lower levels of protein and calcium and were deficient in a number of B vitamins, including B1, B2, B3, B6, and folate, compared to similarly-aged children without ASD [25] |
| 4 | J Plaza-Diaz et al. (2021) [26] | Case control study | 54 children with ASD and 57 typically developing children | 2–6 years old | Determine the feeding behavior, dietary patterns, and macro-and micronutrient intakes in a sample of Spanish preschool children with ASD compared to typically developing control children of the same age | Food frequency questionnaire and 24 h dietary registrations | High energy and fat intakes and a low intake of vegetables and fruits. The usual individual intakes of vitamins B6, B12, and folate were below the recommended doses in children with ASD when compared with the control children [26] |
| No | Study | Type of Study | Sample Size | Age | Aim of the Study | Study Outcomes Parameters | Outcomes |
|---|---|---|---|---|---|---|---|
| 1 | Chistol et al. (2018) [27] | Cross-sectional study | 53 children with ASD and 58 children without ASD | 3–11 years old | Compare oral sensory processing function between children with and without ASD, examine the relationship between atypical oral sensory processing and food selectivity in children with ASD, and examine the relationship between atypical oral sensory processing and fruit and vegetable consumption | Food frequency questionnaire and 3 days food record | Children with ASD exhibit more atypical sensory processing than children without ASD. They tend to refuse more types of food and consume fewer vegetables than those with typical oral sensory sensitivity [27] |
| 2 | Adams et al. (2022) [28] | Cross-sectional quantitative research design | 40 caregivers of ASD children | 3–10 years old | Determine the types of feeding difficulties prevalent in children with ASD, the food items that children in South Africa prefer, and the relationship between age and ASD severity on food preferences | Behavioral Pediatric Feeding Assessment Scale and food preference questionnaire | Common feeding difficulties in children with ASD. A preference for starches and snack items compared with fruits and vegetables. Significant correlations between ASD severity and ASD age on food preferences [28] |
| 3 | J Molina-López et al. (2021) [29] | Cross-sectional case-control study | 144 children (N = 55 with ASD; N = 91 with neurotypical children) | 6–18 years old | Evaluate body composition, nutritional status through food selectivity and degree of inadequate intake, and mealtime behavior in children with autism spectrum disorder (ASD) compared to neurotypical children. | Body composition, nutritional intake, food consumption frequency (FFQ), and mealtime behavior | A greater presence of children with a low weight and obesity in the ASD group. The presence of obesity in ASD children compared to the comparison group was even higher when considering the fat component. ASD children had greater intake inadequacy, high food selectivity by FFQ, and more eating problems (food rejection, limited variety, disruptive behavior), compared to neurotypical children [29] |
| No | Study | Type of Study | Sample Size | Age | Aim of the Study | Study Outcomes Parameters | Outcomes |
|---|---|---|---|---|---|---|---|
| 1 | Chen-Xi Li et al. (2021) [30] | Meta-analysis | - | - | Evaluate the association of MTHFR C677T polymorphism with autism susceptibility among a Chinese Han population | Genetic analyses: MTHFR C677T as predictors of autism risk. | MTHFR C677T was strongly associated with the increased risk of autism in China, especially in Northern Han subgroup [30] |
| 2 | F. El-baz, et al. (2017) [31] | Case control study | 31 ASD children and 39 TD children | 1.5 to 18 years | Identify C677T and A1298C polymorphic genotypes of MTHFR gene among Egyptian ASD children | Identification of C677T and 1298AC polymorphic genotypes of MTHFR gene | There is a significant association between severity and occurrence of autism with MTHFR gene polymorphisms [31] |
| 3 | L. M. Al-Omari et al. (2020) [32] | Case control study | 25 ASD children and 25 TD children | 7 to 18 years | Investigate MTHFR C677T polymorphism (rs1801133) in autistic children | Frequency of genotype MTHFR C677T in children | MTHFR C677T frequency was significantly higher in autistic as compared to non-autistic children. The homozygous genotype CC of the MTHFR C677T was lower in patients with autism than in the control group (28% vs. 52%), while heterozygous CT genotype of the MTHFR C677T and the homozygous TT genotype were higher in patients with autism compared to control group (52%, 44%) and (20%, 4%), respectively [32] |
| 4 | Y. Li et al. (2020) [33] | Meta-analysis | - | Authenticate correlations between MTHFR polymorphism (C677T/A1298C) and susceptibility to ASD | Genetic analyses: MTHFR C677T, MTHFR A1298C as predictors of autism risk. | MTHFR C677T polymorphism is a susceptibility factor for ASD, and MTHFR. A1298C polymorphism is not associated with ASD susceptibility [33] | |
| 5 | T. Sadeghiyeh et al. (2019) [34] | Systematic and meta-analysis | - | - | Evaluate association of MTHFR 677C > T and 1298A > C polymorphisms with risk of autism | Genetic analyses: MTHFR C677T, MTHFR A1298C as predictors of autism risk. | MTHFR 677C > T polymorphism was significantly associated with an increased risk of autism in overall population and by ethnicity, while MTHFR 1298A > C polymorphism was not associated with autism risk overall [34] |
| 6 | B. Razi et al. (2020) [35] | Systematic review and meta-analysis | - | - | Assess candidate genes associated with ASD risk | Genetic analyses: MTHFR C677T, MTHFR A1298C as predictors of autism risk. | A strong association between MTHFR C677T gene polymorphism and autism spectrum disorders risk in Caucasians. There is no significant association between MTHFR A1298C gene polymorphism and ASD risk [35] |
| 7 | N. Q. Muftin et al. (2020) [36] | Review | - | - | Examined the correlation of the common polymorphism (A1298C) and risk of autism on Iraqi autistic children | The correlation of the common polymorphism (A1298C) and risk of autism | All three alleles (AA, AC, CC) were non-significantly correlated with the risk of autism (O.R = 1.23, p = 0.75) and the A1298C polymorphism is not associated with autism in Iraqi population [36] |
| No | Study | Type of Study | Sample Size | Age | Supplement Used | Period of Intake | Study Outcomes Parameters | Outcomes |
|---|---|---|---|---|---|---|---|---|
| 1 | C. Sun, et al. (2016) [37] | Open-Label Trial | 66 ASD children and 22 TD children | 4.5 ± 1.1 years old | Folic acid tablets (400 µg) ren | Twice daily/3 months | There is a significant association between severity and occurrence of autism with MTHFR gene polymorphisms C677T and A1298C. Further studies are needed on a larger scale to explore other gene polymorphisms that may be associated with autism to correlate the genetic basis of autism. There is a significant association between the severity and occurrence of autism with MTHFR gene polymorphisms. C677T and A1298C. Further studies are needed on a larger scale to explore other gene polymorphisms that may be associated with autism to correlate the genetic basis of autism. Plasma levels of FA homocysteine glutathione metabolism before and after treatment. Improvement of autism symptoms | Taking supplements of folic acid reduced the symptoms of autism in terms of sociability, cognitive verbal/preverbal, receptive language, and affective expression and communication. It increased the concentrations of folic acid, homocysteine, and normalized glutathione redox metabolism [37] |
| 2 | A. Čorejová et al. (2022) [38] | Case control study | 25 ASD children | 4–20 years old | Methylcobalamin syrup (500 µg dose) | Daily/200 days | Levels of vitamin B12 and homocysteine after supplementation. Impact on the overall oxidative status | Methylcobalamin treatment increased the levels of vitamin B12 in ASD children, but no significant changes were observed in homocysteine levels. Moreover, methylcobalamin treatment had an important impact on the overall oxidative status, expressed as GSH/GSSG. Methylcobalamin treatment increased the levels of vitamin B12 in ASD children, but no significant changes were observed in homocysteine levels. Methylcobalamin treatment had an important impact on the overall oxidative status, expressed as GSH/GSSG [38] |
| 3 | R. L. Hendren et al. (2016) [39] | Randomized, Placebo-Controlled Trial | 57 ASD children | 3–7 years | Methyl B12 (75 μg/kg) or saline placebo every 3 days in a subcutaneous injection | 8 weeks of treatment | Plasma Plasma levels of methionine, S-adenosyl-L-homocysteine, and the ratio of S-adenosylmethionine (SAM) to SAH | An increase in plasma methionine (p = 0.05), a decrease in S-adenosyl-L-homocysteine (SAH) (p = 0.007), and an improvement in the ratio of S-adenosylmethionine (SAM) to SAH (p = 0.007), thus leading to the improvement of cellular methylation capacity [39] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roufael, M.; Bitar, T.; Sacre, Y.; Andres, C.; Hleihel, W. Folate–Methionine Cycle Disruptions in ASD Patients and Possible Interventions: A Systematic Review. Genes 2023, 14, 709. https://doi.org/10.3390/genes14030709
Roufael M, Bitar T, Sacre Y, Andres C, Hleihel W. Folate–Methionine Cycle Disruptions in ASD Patients and Possible Interventions: A Systematic Review. Genes. 2023; 14(3):709. https://doi.org/10.3390/genes14030709
Chicago/Turabian StyleRoufael, Melissa, Tania Bitar, Yonna Sacre, Christian Andres, and Walid Hleihel. 2023. "Folate–Methionine Cycle Disruptions in ASD Patients and Possible Interventions: A Systematic Review" Genes 14, no. 3: 709. https://doi.org/10.3390/genes14030709
APA StyleRoufael, M., Bitar, T., Sacre, Y., Andres, C., & Hleihel, W. (2023). Folate–Methionine Cycle Disruptions in ASD Patients and Possible Interventions: A Systematic Review. Genes, 14(3), 709. https://doi.org/10.3390/genes14030709