
Correlation of Electrically Evoked Compound Action Potential Amplitude Growth Function Slope and Anamnestic Parameters in Cochlear Implant Patients—Identification of Predictors for the Neuronal Health Status



Abstract
:1. Introduction
2. Materials and Methods
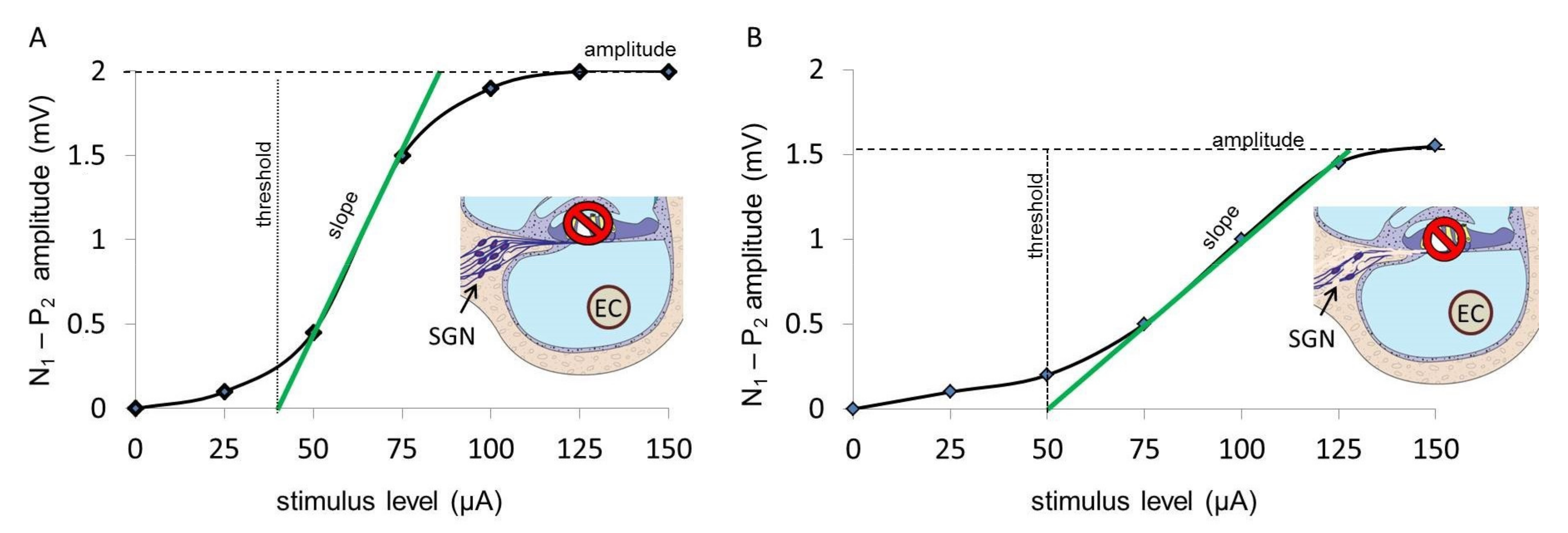
2.1. ECAP AGF Slope
2.2. ECAP Measurement
- Whole array: electrodes 1–12
- Apical region: electrodes 1–3
- Medial region: electrodes 4–9
- Basal region: electrodes 10–12
- Single apical electrode no. 1
- Single apical electrode no. 2
- Single apical electrode no. 3
2.3. Anamnestic Parameters
- unknown (N = 39)
- not documented (N = 39)
- acute (N = 50)
- progressive (N = 11)
- unknown (N = 7)
- not documented (N = 40)
- sudden idiopathic hearing loss, acute hearing loss (N = 42)
- infection (N = 12)
- syndrome, hereditary (N = 15)
- trauma, ototoxins (N = 23)
- presbyacusis (N = 0)
3. Results
3.1. ECAP AGF Slope
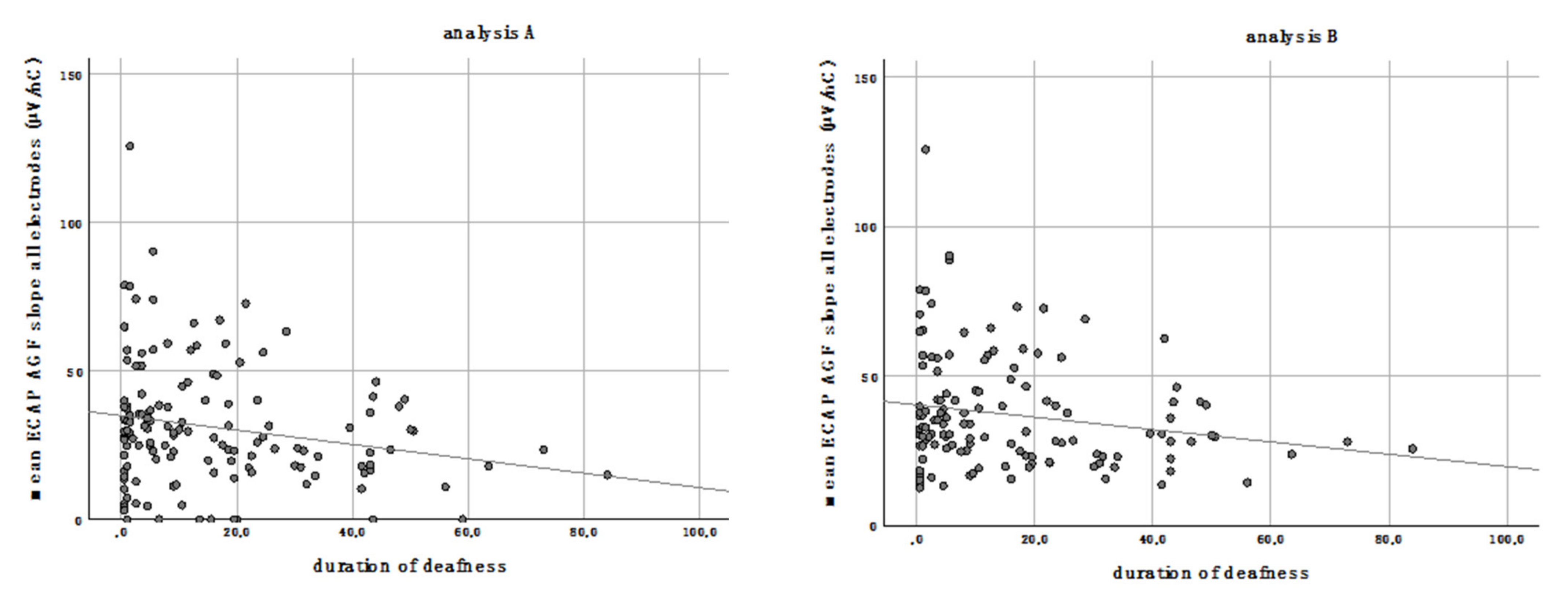
3.2. Duration of Deafness
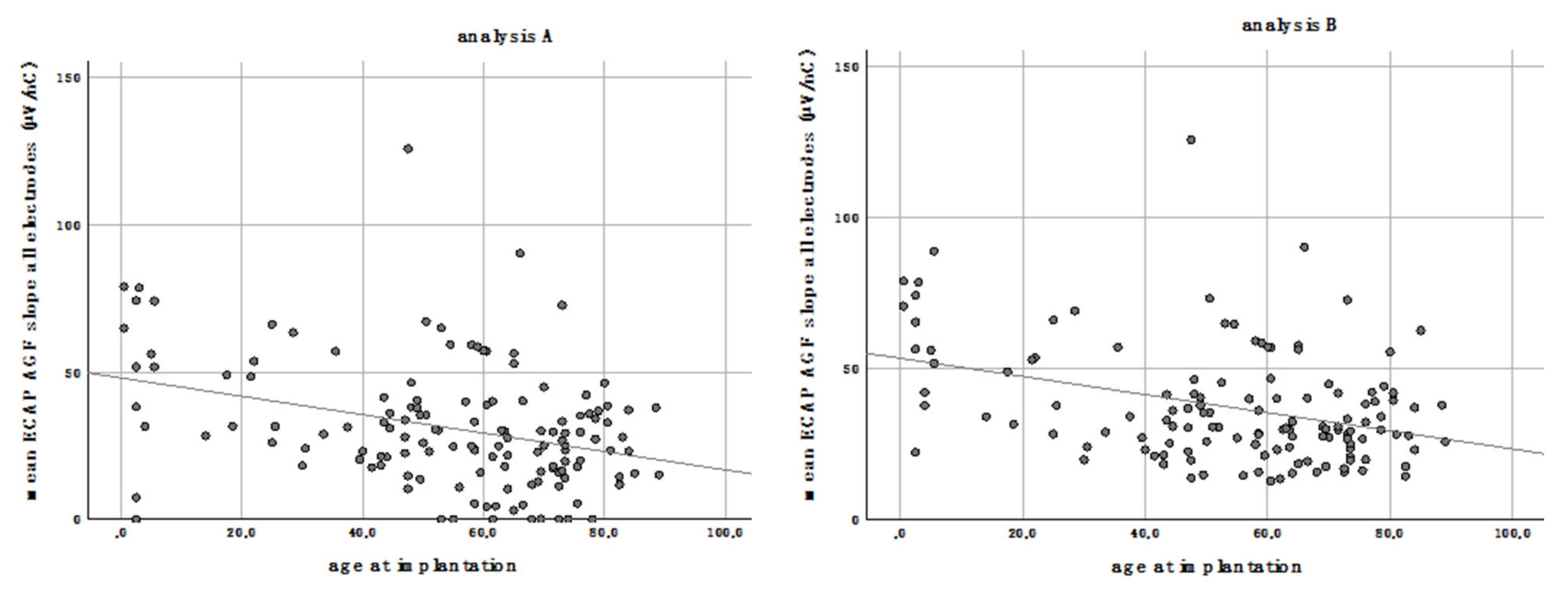
3.3. Age at Implantation
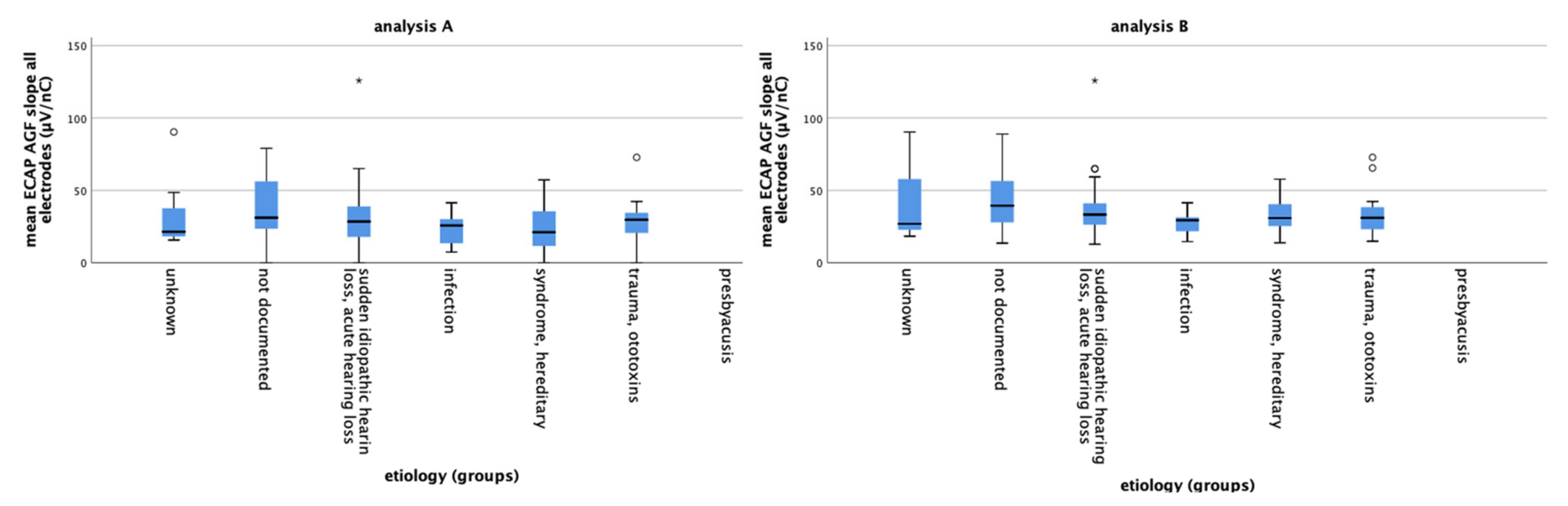
3.4. Etiology
3.5. Etiology Grouped by Occurrence of Hearing Loss
3.6. Residual Hearing
3.7. Multivariate Analysis
3.8. Electrode Array Length
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board and Informed Consent Statements
Data Availability Statement
Conflicts of Interest
References
- WHO. Deafness and Hearing Loss. Fact Sheet. Available online: http://www.who.int/mediacentre/factsheets/fs300/en/ (accessed on 1 February 2021).
- Hoppe, U.; Hocke, T.; Hast, A.; Iro, H. Maximum preimplantation monosyllabic score as predictor of cochlear implant outcome. HNO 2019, 67, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Shearer, A.E.; Eppsteiner, R.W.; Frees, K.; Tejani, V.; Sloan-Heggen, C.M.; Brown, C.; Abbas, P.; Dunn, C.; Hansen, M.R.; Gantz, B.J.; et al. Genetic variants in the peripheral auditory system significantly affect adult cochlear implant performance. Hear. Res. 2017, 348, 138–142. [Google Scholar] [CrossRef] [Green Version]
- Hall, R.D. Estimation of surviving spiral ganglion cells in the deaf rat using the electrically evoked auditory brainstem response. Hear. Res. 1990, 49, 155–168. [Google Scholar] [CrossRef]
- Vink, H.A.; van Dorp, W.C.; Thomeer, H.G.X.M.; Versnel, H.; Ramekers, D. BDNF Outperforms TrkB Agonist 7,8,3′-THF in Preserving the Auditory Nerve in Deafened Guinea Pigs. Brain Sci. 2020, 10, 787. [Google Scholar] [CrossRef]
- Dziemba, O.C.; Aristeidou, A.; Brill, S. Slope of electrically evoked compound action potential amplitude growth function is site-dependent. Cochlear Implants Inter. 2020, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mlynski, R.; Lusebrink, A.; Oberhoffner, T.; Langner, S.; Weiss, N.M. Mapping cochlear duct length to electrically evoked compound action potentials in cochlear implantation. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2021, 42, e254–e260. [Google Scholar]
- Brill, S.; Muller, J.; Hagen, R.; Moltner, A.; Brockmeier, S.-J.; Stark, T.; Helbig, S.; Maurer, J.; Zahnert, T.; Zierhofer, C.; et al. Site of cochlear stimulation and its effect on electrically evoked compound action potentials using the MED-EL standard electrode array. Biomed. Eng. Online 2009, 8, 40. [Google Scholar] [CrossRef] [Green Version]
- Jahn, K.N.; Arenberg, J.G. Identifying cochlear implant channels with relatively poor electrode-neuron interfaces using the electrically evoked compound action potential. Ear Hearing 2020, 41, 961–973. [Google Scholar] [CrossRef]
- Pfingst, B.E.; Hughes, A.P.; Colesa, D.J.; Watts, M.M.; Strahl, S.B.; Raphael, Y. Insertion trauma and recovery of function after cochlear implantation: Evidence from objective functional measures. Hearing Res. 2015, 330, 98–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spoendlin, H. Retrograde degeneration of the cochlear nerve. Acta Otolaryngol. 1975, 79, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Versnel, H.; Agterberg, M.J.; de Groot, J.C.; Smoorenburg, G.F.; Klis, S.F. Time course of cochlear electrophysiology and morphology after combined administration of kanamycin and furosemide. Hear. Res. 2007, 231, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glueckert, R.; Pfaller, K.; Kinnefors, A.; Rask-Andersen, H.; Schrott-Fischer, A. The human spiral ganglion: New insights into ultrastructure, survival rate and implications for cochlear implants. Audiol. Neurotol. 2005, 10, 258–273. [Google Scholar] [CrossRef]
- Nadol, J.B.; Young, Y.S.; Glynn, R.J. Survival of spiral ganglion-cells in profound sensorineural hearing-loss—Implications for cochlear implantation. Annals. Otol. Rhinol. Laryngol. 1989, 98, 411–416. [Google Scholar] [CrossRef]
- Landry, T.G.; Fallon, J.B.; Wise, A.K.; Shepherd, R.K. Chronic neurotrophin delivery promotes ectopic neurite growth from the spiral ganglion of deafened cochleae without compromising the spatial selectivity of cochlear implants. J. Comp. Neurol. 2013, 521, 2818–2832. [Google Scholar] [CrossRef] [Green Version]
- Seyyedi, M.; Nadol, J.B. Intracochlear Inflammatory response to cochlear implant electrodes in humans. Otol. Neurotol. 2014, 35, 1545–1551. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, R.K.; Coco, A.; Epp, S.B.; Crook, J.M. Chronic depolarization enhances the trophic effects of brain-derived neurotrophic factor in rescuing auditory neurons following a sensorineural hearing loss. J. Comp. Neurol 2005, 486, 145–158. [Google Scholar] [CrossRef] [Green Version]
- Shibata, S.B.; Cortez, S.R.; Beyer, L.A.; Wiler, J.A.; Di Polo, A.; Pfingst, B.E.; Raphael, Y. Transgenic BDNF induces nerve fiber regrowth into the auditory epithelium in deaf cochleae. Exp. Neurol. 2010, 223, 464–472. [Google Scholar] [CrossRef] [Green Version]
- Fayad, J.N.; Linthicum, F.H., Jr. Multichannel cochlear implants: Relation of histopathology to performance. Laryngoscope 2006, 116, 1310–1320. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.X.; Kim, G.H.; Snissarenko, E.P.; Cureoglu, S.; Paparella, M.M. Multi-channel cochlear implant histopathology: Are fewer spiral ganglion cells really related to better clinical performance? Acta Otol.-Laryngol. 2012, 132, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.J.; Abbas, P.J.; Gantz, B.J. Preliminary experience with neural response telemetry in the nucleus CI24M cochlear implant. Am. J. Otol. 1998, 19, 320–327. [Google Scholar] [PubMed]
- He, S.; Teagle, H.F.B.; Buchman, C.A. The Electrically Evoked Compound Action Potential: From Laboratory to Clinic. Front. Neurosci. 2017, 11, 339. [Google Scholar] [CrossRef]
- Jakobsen, J.C.; Gluud, C.; Wetterslev, J.; Winkel, P. When and how should multiple imputation be used for handling missing data in randomised clinical trials—A practical guide with flowcharts. BMC Med. Res. Method. 2017, 17, 162. [Google Scholar] [CrossRef] [Green Version]
- Scheper, V.; Schmidtheisler, M.; Lasch, F.; von der Leyen, H.; Koch, A.; Schwieger, J.; Büchner, A.; Lesinski-Schiedat, A.; Lenarz, T. Randomized placebo-controlled clinical trial investigating the effect of antioxidants and a vasodilator on overall safety and residual hearing preservation in cochlear implant patients. Trials 2020, 21, 643. [Google Scholar] [CrossRef]
- Finley, C.C.; Holden, T.A.; Holden, L.K.; Whiting, B.R.; Chole, R.A.; Neely, G.J.; Hullar, T.E.; Skinner, M.W. Role of electrode placement as a contributor to variability in cochlear implant outcomes. Otol. Neurotol.: Official Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Academy Otol. Neurotol. 2008, 29, 920–928. [Google Scholar] [CrossRef] [Green Version]
- Van der Marel, K.S.; Briaire, J.J.; Wolterbeek, R.; Snel-Bongers, J.; Verbist, B.M.; Frijns, J.H.M. Diversity in cochlear morphology and its influence on cochlear implant electrode position. Ear Hearing 2014, 35, e9–e20. [Google Scholar] [CrossRef] [PubMed]
- Holden, L.K.; Finley, C.C.; Firszt, J.B.; Holden, T.A.; Brenner, C.; Potts, L.G.; Gotter, B.D.; Vanderhoof, S.S.; Mispagel, K.; Heydebrand, G.; et al. Factors affecting open-set word recognition in adults with cochlear implants. Ear Hearing 2013, 34, 342–360. [Google Scholar] [CrossRef] [Green Version]
- Blamey, P.; Artieres, F.; Baskent, D.; Bergeron, F.; Beynon, A.; Burke, E.; Dillier, N.; Dowell, R.; Fraysse, B.; Gallego, S.; et al. Factors affecting auditory performance of postlinguistically deaf adults using cochlear implants: An update with 2251 patients. Audiol. Neurootol. 2013, 18, 36–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Würfel, W.; Lanfermann, H.; Lenarz, T.; Majdani, O. Cochlear length determination using Cone Beam Computed Tomography in a clinical setting. Hear. Res. 2014, 316, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Yukawa, K.; Cohen, L.T.; Blamey, P.; Pyman, B.C.; Tungvachirakul, V.; O’Leary, S. Effects of insertion depth of cochlear implant electrodes upon speech perception. Audiol Neurootol 2004, 9, 163–172. [Google Scholar] [CrossRef]
- Mangado, N.; Pons-Prats, J.; Coma, M.; Mistrik, P.; Piella, G.; Ceresa, M.; Gonzalez Ballester, M.A. Computational Evaluation of Cochlear Implant Surgery Outcomes Accounting for Uncertainty and Parameter Variability. Front. Physiol. 2018, 9, 498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritzsch, B.; Pirvola, U.; Ylikoski, J. Making and breaking the innervation of the ear: Neurotrophic support during ear development and its clinical implications. Cell Tissue Res. 1999, 295, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Zilberstein, Y.; Liberman, M.C.; Corfas, G. Inner hair cells are not required for survival of spiral ganglion neurons in the adult cochlea. J. Neurosci. Off. J. Soc. Neurosci. 2012, 32, 405–410. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, R.K.; Javel, E. Electrical stimulation of the auditory nerve. I. Correlation of physiological responses with cochlear status. Hear. Res. 1997, 108, 112–144. [Google Scholar] [CrossRef]
- Maruyama, J.; Miller, J.M.; Ulfendahl, M. Glial cell line-derived neurotrophic factor and antioxidants preserve the electrical responsiveness of the spiral ganglion neurons after experimentally induced deafness. Neurobiol Dis. 2008, 29, 14–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agterberg, M.J.; Versnel, H.; van Dijk, L.M.; de Groot, J.C.; Klis, S.F. Enhanced survival of spiral ganglion cells after cessation of treatment with brain-derived neurotrophic factor in deafened guinea pigs. J. Assoc. Res. Otol. 2009, 10, 355–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramekers, D.; Versnel, H.; Strahl, S.B.; Smeets, E.M.; Klis, S.F.L.; Grolman, W. Auditory-nerve responses to varied inter-phase gap and phase duration of the electric pulse stimulus as predictors for neuronal degeneration. J. Association Res. Otolaryngol. JARO 2014, 15, 187–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grill, W.M.; Norman, S.E.; Bellamkonda, R.V. Implanted neural interfaces: Biochallenges and engineered solutions. Annu. Rev. Biomed. Eng. 2009, 11, 1–24. [Google Scholar] [CrossRef]
- Zimmermann, C.E.; Burgess, B.J.; Nadol, J.B., Jr. Patterns of degeneration in the human cochlear nerve. Hearing Res. 1995, 90, 192–201. [Google Scholar] [CrossRef]
- Miura, M.; Sando, I.; Hirsch, B.E.; Orita, Y. Analysis of spiral ganglion cell populations in children with normal and pathological ears. Ann. Otol. Rhinol. Laryngol. 2002, 111, 1059–1065. [Google Scholar] [CrossRef]
- Lenarz, T. Cochlear implant—State of the art. GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 2017, 16, Doc04. [Google Scholar] [CrossRef] [Green Version]
- Jahn, K.N.; Arenberg, J.G. Electrophysiological estimates of the electrode-neuron interface differ between younger and older listeners with cochlear implants. Ear Hearing 2020, 41, 948–960. [Google Scholar] [CrossRef]
- Büchner, A.; Illg, A.; Majdani, O.; Lenarz, T. Investigation of the effect of cochlear implant electrode length on speech comprehension in quiet and noise compared with the results with users of electro-acoustic-stimulation, a retrospective analysis. PLoS ONE 2017, 12, e0174900. [Google Scholar] [CrossRef]
- Salcher, R.; Boruchov, A.; Timm, M.; Steffens, M.; Giesemann, A.; Lenarz, T.; Warnecke, A. On the intracochlear location of straight electrode arrays after cochlear implantation: How lateral are lateral wall electrodes? Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2020. [Google Scholar] [CrossRef]
- Schurzig, D.; Timm, M.E.; Batsoulis, C.; John, S.; Lenarz, T. Analysis of different approaches for clinical cochlear coverage evaluation after cochlear implantation. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2018, 39, e642–e650. [Google Scholar] [CrossRef] [PubMed]
- Buchman, C.A.; Dillon, M.T.; King, E.R.; Adunka, M.C.; Adunka, O.F.; Pillsbury, H.C. Influence of cochlear implant insertion depth on performance: A prospective randomized trial. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2014, 35, 1773–1779. [Google Scholar] [CrossRef] [PubMed]
- Kurz, A.; Grubenbecher, M.; Rak, K.; Hagen, R.; Kuhn, H. The impact of etiology and duration of deafness on speech perception outcomes in SSD patients. Eur. Arch. Oto-Rhino-Laryngol. Off. J. Eur. Fed. Oto-Rhino-Laryngol. Soc. (EUFOS) Affil. Ger. Soc. Oto-Rhino-Laryngol. Head Neck Surg. 2019, 276, 3317–3325. [Google Scholar] [CrossRef] [PubMed]
- Brochier, T.; McKay, C.M.; Carlyon, R.P. Interpreting the Effect of Stimulus Parameters on the Electrically Evoked Compound Action Potential and on Neural Health Estimates. J. Assoc. Res. Otolaryngol. 2020, 27, 020–00774. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Duration of Deafness | Age at Implantation | |||||||
|---|---|---|---|---|---|---|---|---|
| Analysis A | Analysis B | Analysis A | Analysis B | |||||
| electrodes | p-value | r2 | p-value | r2 | p-value | r2 | p-value | r2 |
| 1–12 | 0.017 | 0.041 | 0.032 | 0.035 | <0.001 | 0.119 | <0.001 | 0.134 |
| Grouped electrodes | ||||||||
| 1–3 (apical) | 0.115 | 0.018 | 0.038 | 0.035 | 0.020 | 0.039 | 0.018 | 0.045 |
| 4–9 (middle) | 0.013 | 0.044 | 0.014 | 0.047 | <0.001 | 0.136 | <0.001 | 0.156 |
| 10–12 (basal) | 0.008 | 0.051 | 0.012 | 0.053 | <0.001 | 0.195 | <0.001 | 0.287 |
| Regression Coefficient B | Std.-Error | Beta | Significance | |
|---|---|---|---|---|
| Constant | 42.356 | 7.034 | <0.001 | |
| Not documented | 1.207 | 7.671 | 0.029 | 0.875 |
| Acute hearing loss | −5.328 | 7.639 | −0.130 | 0.487 |
| Infection | −15.441 | 8.851 | −0.238 | 0.084 |
| Syndromal/hereditary | −9.018 | 8.725 | −0.144 | 0.303 |
| Trauma/ototoxins | −8.078 | 8.122 | −0.158 | 0.322 |
| Analysis A | Analysis B | |||||
|---|---|---|---|---|---|---|
| Regression coefficient B | Regression coefficient B | |||||
| Electrodes | 1–3 | 4–9 | 10–12 | 1–3 | 4–9 | 10–12 |
| Constant | 64.095 | 27.714 | 17.095 | 64.095 | 32.333 | 26.900 |
| Not documented | −10.104 | 8.390 | 5.355 | −0.186 | 8.121 | 2.314 |
| Acute hearing loss | −16.111 | 1.333 | 1.341 | −6.456 | 1.932 | −2.817 |
| Infection | −27.540 | −5.700 | −3.262 | −24.220 | −7.481 | −10.233 |
| Syndromal/hereditary | −30.806 | −2.803 | −4.651 | −21.845 | 0.217 | 0.100 |
| Trauma/ototoxins | −24.776 | 0.206 | 0.383 | −17.127 | −0.459 | −3.855 |
| Analysis A | Analysis B | |||||||
|---|---|---|---|---|---|---|---|---|
| Regression coefficient B | Regression coefficient B | |||||||
| Electrodes | all | 1–3 | 4–9 | 10–12 | all | 1–3 | 4–9 | 10–12 |
| Constant | 27.132 | 41.641 | 26.350 | 14.188 | 32.246 | 42.987 | 28.624 | 18.372 |
| Not documented | 10.344 | 12.949 | 10.021 | 8.385 | 8.444 | 13.581 | 9.098 | 7.393 |
| Acute | 2.569 | 2.972 | 1.613 | 4.079 | 1.053 | 4.093 | 1.807 | 2.155 |
| Progressive | 1.724 | 2.207 | 0.362 | 3.963 | −0.335 | 2.073 | −0.760 | 0.689 |
| Analysis A (Implant Model 20 mm) | Analyse B (IMPLANTATMODEL 24 mm) | ||
|---|---|---|---|
| Electrodes | 1–3 | 2 | 3 |
| Residual hearing | |||
| 125 Hz | / | 0.035 | / |
| 250 Hz | / | 0.030 | 0.041 |
| 500 Hz | 0.037 | 0.034 | / |
| Multivariate Analysis of Significant Variables for the Mean ECAP AGF slope of All Electrodes | ||||||
|---|---|---|---|---|---|---|
| Analysis A | Analysis B | |||||
| Regression coefficient B | Std. Error | Sig. | Regression coefficient B | Std. Error | Sig. | |
| Constant | 49.805 | 4.330 | <0.001 | 54.899 | 4.039 | <0.001 |
| Duration of deafness | −0.183 | 0.097 | 0.060 | −0.148 | 0.091 | 0.105 |
| Age at implantation | −0.291 | 0.073 | <0.001 | −0.282 | 0.068 | <0.001 |
| Multivariate analysis of significant variables for the mean ECAP AGF slope of electrodes 1–3 | ||||||
| Analysis A | Analysis B | |||||
| Regression coefficient B | Std. Error | Sig. | Regression coefficient B | Std. Error | Sig. | |
| Constant | / | / | / | 73.482 | 7.318 | <0.001 |
| Duration of deafness | / | / | / | −0.298 | 0.167 | 0.077 |
| Age at implantation | / | / | / | −0.264 | 0.124 | 0.036 |
| Multivariate analysis of significant variables for the mean ECAP AGF slope of electrodes 4–9 | ||||||
| Analysis A | Analysis B | |||||
| Regression coefficient B | Std. Error | Sig. | Regression coefficient B | Std. Error | Sig. | |
| Constant | 49.522 | 4.252 | <0.001 | 53.610 | 3.932 | <0.001 |
| Duration of deafness | −0.188 | 0.095 | 0.049 | −0.185 | 0.089 | 0.039 |
| Age at implantation | −0.309 | 0.071 | <0.001 | −0.304 | 0.066 | <0.001 |
| Multivariate analysis of significant variables for the mean ECAP AGF slope of electrodes 10–12 | ||||||
| Analysis A | Analysis B | |||||
| Regression coefficient B | Std. Error | Sig. | Regression coefficient B | Std. Error | Sig. | |
| Constant | 34.933 | 2.917 | <0.001 | 43.275 | 2.721 | <0.001 |
| Duration of deafness | −0.137 | 0.065 | 0.037 | −0.143 | 0.065 | 0.029 |
| Age at implantation | −0.266 | 0.049 | <0.001 | −0.305 | 0.046 | <0.001 |
| Electrode Array Length (mm) | ||||||
|---|---|---|---|---|---|---|
| 16 (N = 2) | 20 (N = 13) | 24 (N = 14) | 28 (N = 59) | 31.5 (N = 51) | ||
| electrodes | mean ECAP AGF slope | |||||
| Data set A | 1–12 | 20.75 | 24.15 | 32.40 | 35.17 | 28.20 |
| 1–3 | 44.33 | 32.77 | 45.86 | 52.45 | 43.43 | |
| 4–9 | 16.33 | 25.71 | 31.87 | 33.45 | 26.50 | |
| 10–12 | 6.0 | 12.41 | 20.02 | 21.32 | 16.37 | |
| Data set B | 1–12 | 32.94 | 28.53 | 41.98 | 39.37 | 36.53 |
| 1–3 | 44.33 | 35.81 | 57.74 | 59.51 | 54.09 | |
| 4–9 | 25.33 | 27.32 | 39.01 | 36.67 | 32.93 | |
| 10–12 | 12.00 | 21.20 | 26.08 | 26.03 | 24.85 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gärtner, L.; Klötzer, K.; Lenarz, T.; Scheper, V. Correlation of Electrically Evoked Compound Action Potential Amplitude Growth Function Slope and Anamnestic Parameters in Cochlear Implant Patients—Identification of Predictors for the Neuronal Health Status. Life 2021, 11, 203. https://doi.org/10.3390/life11030203
Gärtner L, Klötzer K, Lenarz T, Scheper V. Correlation of Electrically Evoked Compound Action Potential Amplitude Growth Function Slope and Anamnestic Parameters in Cochlear Implant Patients—Identification of Predictors for the Neuronal Health Status. Life. 2021; 11(3):203. https://doi.org/10.3390/life11030203
Chicago/Turabian StyleGärtner, Lutz, Katharina Klötzer, Thomas Lenarz, and Verena Scheper. 2021. "Correlation of Electrically Evoked Compound Action Potential Amplitude Growth Function Slope and Anamnestic Parameters in Cochlear Implant Patients—Identification of Predictors for the Neuronal Health Status" Life 11, no. 3: 203. https://doi.org/10.3390/life11030203
APA StyleGärtner, L., Klötzer, K., Lenarz, T., & Scheper, V. (2021). Correlation of Electrically Evoked Compound Action Potential Amplitude Growth Function Slope and Anamnestic Parameters in Cochlear Implant Patients—Identification of Predictors for the Neuronal Health Status. Life, 11(3), 203. https://doi.org/10.3390/life11030203