


From Tick to Test: A Comprehensive Review of Tick-Borne Disease Diagnostics and Surveillance Methods in the United States

Abstract
:1. Introduction
2. Tick-Borne Diseases in the United States
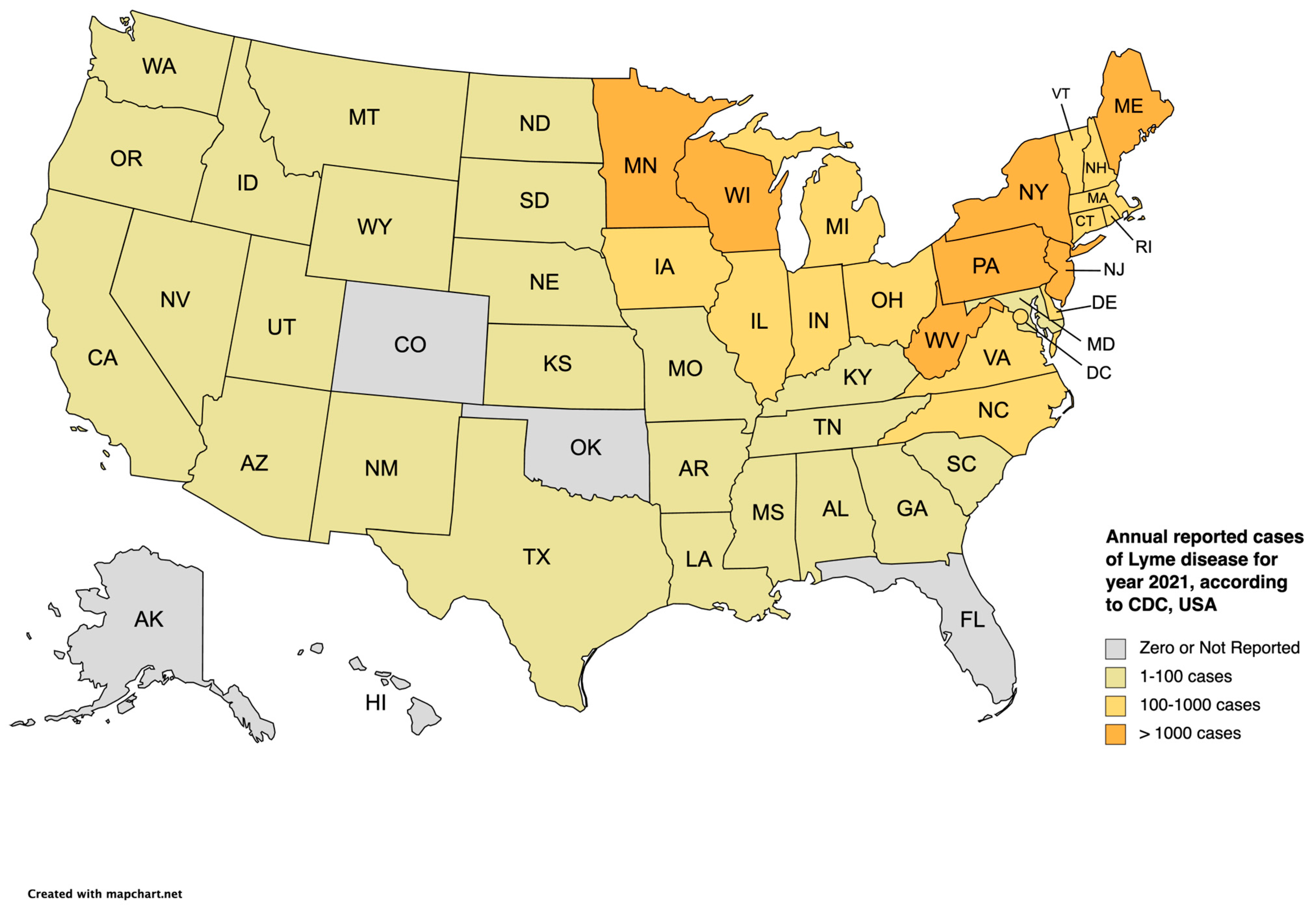
2.1. Lyme Disease
2.2. Anaplasmosis
2.3. Babesiosis
2.4. Powassan Virus Disease
2.5. Ehrlichiosis
2.6. Spotted Fever Rickettsioses
2.7. Other Tick-Borne Diseases (TBDs)
3. Surveillance Methods (Table 1)
3.1. Passive Surveillance

{kind=link}
{kind=link}
| Surveillance Method | Description | Advantages | Disadvantages |
|---|---|---|---|
| Active Surveillance | Involves actively seeking out and testing ticks or individuals for tick-borne pathogens. | Provides real-time data on tick infection rates and pathogen presence. Allows for targeted sampling in high-risk areas or populations. Can detect emerging pathogens. | Resource-intensive and time-consuming. May not capture the full range of tick species or locations. Relies on active participation of individuals or organizations. |
| Passive Surveillance | Relies on reports from healthcare providers, laboratories, or the public regarding ticks and diagnosed cases of tick-borne diseases. | Relatively low cost and effort. Provides information on human cases and associated pathogens. Can cover a large geographic area. Can capture severe or unusual cases. | Underreporting and underdiagnosis may occur. May lack comprehensive data on tick species or infection rates. Dependent on the willingness and awareness of reporting entities and individuals. |
| Sentinel Surveillance | Selects specific sites or individuals (sentinels) to provide ongoing data on tick abundance, infection rates, and disease cases. | Provides targeted data from high-risk areas or populations. Allows for long-term monitoring and trend analysis. Can identify early warning signs of disease emergence or changes in patterns. Enables collaboration and coordination between multiple stakeholders. | Limited to selected sentinel sites or populations. May not capture all tick species or locations. Requires continuous resources and commitment. Results may not be generalizable to larger areas. |
3.2. Active Surveillance
3.3. Laboratory-Based Surveillance
3.4. Sentinel Surveillance
3.5. One Health Approach (Table 2)
| Aspect | Description | Examples |
|---|---|---|
| Interconnectedness | Recognizes the interrelation of human and animal health, with the environment. | Tick-borne diseases can affect both humans and animals, and their transmission is influenced by environmental factors—climate and habitat changes. |
| Collaboration | Encourages cooperation between various disciplines and sectors, including human health, veterinary medicine, entomology, ecology, and environmental sciences. | Public health agencies, veterinary clinics, entomologists, and researchers collaborate to share data, conduct joint investigations, and develop comprehensive surveillance and control strategies. |
| Surveillance | Integrates monitoring efforts across humans, animals, and ticks to gather comprehensive data on tick-borne diseases. | Surveillance programs collect and analyze data on tick abundance, infection rates, and disease cases in both humans and animals to understand disease dynamics and identify risk factors. |
| Prevention and Control | Promotes a holistic approach to prevention and control strategies that address the various components of the disease system. | Vector control measures, such as habitat management and acaricide application, are implemented to reduce tick populations. Public education campaigns raise awareness about tick bite prevention in both humans and animals. |
| Research | Encourages interdisciplinary research to enhance understanding of tick-borne diseases, including their epidemiology, ecology, and transmission dynamics. | Research studies explore the impact of environmental factors on tick populations, investigate the efficacy of preventive measures, and develop new diagnostic tools or vaccines. |
| Policy and Regulations | Guides the development of policies and regulations that support One Health principles and facilitate coordinated efforts in tick-borne disease prevention and control. | Governments establish policies that promote collaboration between human and animal health sectors, allocate resources for surveillance and research, and regulate the use of acaricides or vaccines. |
4. Surveillance Systems
4.1. National Notifiable Diseases Surveillance System (NNDSS)
4.2. TickNET and Other Surveillance Initiatives
5. Challenges and Limitations
5.1. Underreporting and Misdiagnosis
5.2. Lack of Standardization of Surveillance in Human and Non-Human Hosts
6. Innovations and Future Directions
6.1. Molecular Surveillance Techniques
6.2. Syndromic Surveillance Networks
6.3. Prevention and Vector Management
6.4. Research Priorities and Policy Implications
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boulanger, N.; Boyer, P.; Talagrand-Reboul, E.; Hansmann, Y. Ticks and tick-borne diseases. Med. Mal. Infect. 2019, 49, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Steere, A.C.; Malawista, S.E.; Snydman, D.R.; Shope, R.E.; Andiman, W.A.; Ross, M.R.; Steele, F.M. Lyme arthritis: An epidemic of oligoarticular arthritis in children and adults in three connecticut communities. Arthritis Rheum 1977, 20, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Jongejan, F.; Uilenberg, G. The global importance of ticks. Parasitology 2004, 129, S3–S14. [Google Scholar] [CrossRef] [PubMed]
- Eisen, R.J.; Kugeler, K.J.; Eisen, L.; Beard, C.B.; Paddock, C.D. Tick-Borne Zoonoses in the United States: Persistent and Emerging Threats to Human Health. ILAR J. 2017, 58, 319–335. [Google Scholar] [CrossRef]
- Pritt, B.S.; Mead, P.S.; Johnson, D.K.H.; Neitzel, D.F.; Respicio-Kingry, L.B.; Davis, J.P.; Schiffman, E.; Sloan, L.M.; Schriefer, M.E.; Replogle, A.J.; et al. Identification of a novel pathogenic Borrelia species causing Lyme borreliosis with unusually high spirochaetaemia: A descriptive study. Lancet Infect. Dis. 2016, 16, 556–564. [Google Scholar] [CrossRef]
- Eisen, R.J.; Eisen, L. The Blacklegged Tick, Ixodes scapularis: An Increasing Public Health Concern. Trends Parasitol. 2018, 34, 295–309. [Google Scholar] [CrossRef]
- Eisen, R.J.; Paddock, C.D. Tick and Tickborne Pathogen Surveillance as a Public Health Tool in the United States. J. Med. Entomol. 2021, 58, 1490–1502. [Google Scholar] [CrossRef]
- Diuk-Wasser, M.A.; Vannier, E.; Krause, P.J. Coinfection by Ixodes Tick-Borne Pathogens: Ecological, Epidemiological, and Clinical Consequences. Trends Parasitol. 2016, 32, 30–42. [Google Scholar] [CrossRef]
- Mead, P.S. Epidemiology of Lyme disease. Infect. Dis. Clin. N. Am. 2015, 29, 187–210. [Google Scholar] [CrossRef]
- Hook, S.A.; Jeon, S.; Niesobecki, S.A.; Hansen, A.P.; Meek, J.I.; Bjork, J.K.H.; Dorr, F.M.; Rutz, H.J.; Feldman, K.A.; White, J.L.; et al. Economic Burden of Reported Lyme Disease in High-Incidence Areas, United States, 2014–2016. Emerg. Infect. Dis. 2022, 28, 1170–1179. [Google Scholar] [CrossRef]
- Marques, A.R.; Strle, F.; Wormser, G.P. Comparison of Lyme Disease in the United States and Europe. Emerg. Infect. Dis. 2021, 27, 2017–2024. [Google Scholar] [CrossRef] [PubMed]
- Chomel, B. Lyme disease. Rev. Sci. Tech. 2015, 34, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Minnesota Department of Health. About Borrelia Mayonii. Available online: https://www.health.state.mn.us/diseases/bmayonii/basics (accessed on 17 September 2023).
- CDC. Lyme Disease Surveillance Data. Available online: https://www.cdc.gov/lyme/datasurveillance/surveillance-data.html (accessed on 17 September 2023).
- Chochlakis, D.; Ioannou, I.; Tselentis, Y.; Psaroulaki, A. Human anaplasmosis and Anaplasma ovis variant. Emerg. Infect. Dis. 2010, 16, 1031–1032. [Google Scholar] [CrossRef] [PubMed]
- Ismail, N.; Bloch, K.C.; McBride, J.W. Human ehrlichiosis and anaplasmosis. Clin. Lab. Med. 2010, 30, 261–292. [Google Scholar] [CrossRef]
- Madison-Antenucci, S.; Kramer, L.D.; Gebhardt, L.L.; Kauffman, E. Emerging Tick-Borne Diseases. Clin. Microbiol. Rev. 2020, 33, e00083-18. [Google Scholar] [CrossRef]
- Dumic, I.; Jevtic, D.; Veselinovic, M.; Nordstrom, C.W.; Jovanovic, M.; Mogulla, V.; Veselinovic, E.M.; Hudson, A.; Simeunovic, G.; Petcu, E.; et al. Human Granulocytic Anaplasmosis-A Systematic Review of Published Cases. Microorganisms 2022, 10, 1433. [Google Scholar] [CrossRef]
- Russell, A.; Prusinski, M.; Sommer, J.; O’Connor, C.; White, J.; Falco, R.; Kokas, J.; Vinci, V.; Gall, W.; Tober, K.; et al. Epidemiology and Spatial Emergence of Anaplasmosis, New York, USA, 2010–2018. Emerg. Infect. Dis. 2021, 27, 2154–2162. [Google Scholar] [CrossRef]
- Schotthoefer, A.M.; Meece, J.K.; Fritsche, T.R. A clinical, diagnostic, and ecologic perspective on human anaplasmosis in the Upper Midwest. WMJ 2014, 113, 107–114. [Google Scholar]
- Bhanot, P.; Parveen, N. Investigating disease severity in an animal model of concurrent babesiosis and Lyme disease. Int. J. Parasitol. 2019, 49, 145–151. [Google Scholar] [CrossRef]
- Homer, M.J.; Aguilar-Delfin, I.; Telford, S.R., 3rd; Krause, P.J.; Persing, D.H. Babesiosis. Clin. Microbiol. Rev. 2000, 13, 451–469. [Google Scholar] [CrossRef]
- Vannier, E.G.; Diuk-Wasser, M.A.; Ben Mamoun, C.; Krause, P.J. Babesiosis. Infect. Dis. Clin. N. Am. 2015, 29, 357–370. [Google Scholar] [CrossRef] [PubMed]
- Beugnet, F.; Moreau, Y. Babesiosis. Rev. Sci. Tech. 2015, 34, 627–639. [Google Scholar] [CrossRef]
- Mc, L.D.; Donohue, W.L. Powassan virus: Isolation of virus from a fatal case of encephalitis. Can. Med. Assoc. J. 1959, 80, 708–711. [Google Scholar]
- Della-Giustina, D.; Duke, C.; Goldflam, K. Underrecognized Tickborne Illnesses: Borrelia Miyamotoi and Powassan Virus. Wilderness Environ. Med. 2021, 32, 240–246. [Google Scholar] [CrossRef]
- Kemenesi, G.; Banyai, K. Tick-Borne Flaviviruses, with a Focus on Powassan Virus. Clin. Microbiol. Rev. 2019, 32, e00106-17. [Google Scholar] [CrossRef]
- Pesko, K.N.; Torres-Perez, F.; Hjelle, B.L.; Ebel, G.D. Molecular epidemiology of Powassan virus in North America. J. Gen. Virol. 2010, 91, 2698–2705. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Foster, E.; Ribbe, F.; Hojgaard, A.; Eisen, R.J.; Paull, S.; Rich, S.M. Detection of Ehrlichia muris eauclairensis in Blacklegged Ticks (Ixodes scapularis) and White-Footed Mice (Peromyscus leucopus) in Massachusetts. Vector Borne Zoonotic Dis. 2023, 23, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Jay, R.; Armstrong, P.A. Clinical characteristics of Rocky Mountain spotted fever in the United States: A literature review. J. Vector Borne Dis. 2020, 57, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Azad, A.F.; Beard, C.B. Rickettsial pathogens and their arthropod vectors. Emerg. Infect. Dis. 1998, 4, 179–186. [Google Scholar] [CrossRef]
- Snowden, J.; Simonsen, K.A. Rocky Mountain Spotted Fever (Rickettsia rickettsii); StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Zhang, Y.Y.; Sun, Y.Q.; Chen, J.J.; Teng, A.Y.; Wang, T.; Li, H.; Hay, S.I.; Fang, L.Q.; Yang, Y.; Liu, W. Mapping the global distribution of spotted fever group rickettsiae: A systematic review with modelling analysis. Lancet Digit. Health 2023, 5, e5–e15. [Google Scholar] [CrossRef]
- Salje, J.; Weitzel, T.; Newton, P.N.; Varghese, G.M.; Day, N. Rickettsial infections: A blind spot in our view of neglected tropical diseases. PLoS Negl. Trop. Dis. 2021, 15, e0009353. [Google Scholar] [CrossRef] [PubMed]
- Herrick, K.L.; Pena, S.A.; Yaglom, H.D.; Layton, B.J.; Moors, A.; Loftis, A.D.; Condit, M.E.; Singleton, J.; Kato, C.Y.; Denison, A.M.; et al. Rickettsia parkeri Rickettsiosis, Arizona, USA. Emerg. Infect. Dis. 2016, 22, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K. Rickettsia-Host-Tick Interactions: Knowledge Advances and Gaps. Infect. Immun. 2022, 90, e0062121. [Google Scholar] [CrossRef] [PubMed]
- Pace, E.J.; O’Reilly, M. Tickborne Diseases: Diagnosis and Management. Am. Fam. Physician 2020, 101, 530–540. [Google Scholar] [PubMed]
- Yendell, S.J.; Fischer, M.; Staples, J.E. Colorado tick fever in the United States, 2002–2012. Vector Borne Zoonotic Dis. 2015, 15, 311–316. [Google Scholar] [CrossRef]
- Dworkin, M.S.; Schwan, T.G.; Anderson, D.E., Jr.; Borchardt, S.M. Tick-borne relapsing fever. Infect. Dis. Clin. N. Am. 2008, 22, 449–468. [Google Scholar] [CrossRef]
- Roscoe, C.; Epperly, T. Tick-borne relapsing fever. Am. Fam. Physician 2005, 72, 2039–2044. [Google Scholar]
- Higuita, N.I.A.; Franco-Paredes, C.; Henao-Martinez, A.F. The expanding spectrum of disease caused by the Lone Star Tick, Amblyomma americanum. Infez. Med. 2021, 29, 378–385. [Google Scholar]
- Rupani, A.; Elshabrawy, H.A.; Bechelli, J. Dermatological manifestations of tick-borne viral infections found in the United States. Virol. J. 2022, 19, 199. [Google Scholar] [CrossRef]
- Johnson, N.; Phipps, L.P.; Hansford, K.M.; Folly, A.J.; Fooks, A.R.; Medlock, J.M.; Mansfield, K.L. One Health Approach to Tick and Tick-Borne Disease Surveillance in the United Kingdom. Int. J. Environ. Res. Public Health 2022, 19, 5833. [Google Scholar] [CrossRef]
- Pasternak, A.R.; Palli, S.R. Mapping distributions of the Lyme disease vector, Ixodes scapularis, and spirochete, Borrelia burgdorferi, in Kentucky using passive and active surveillance. Ticks Tick. Borne Dis. 2022, 13, 101885. [Google Scholar] [CrossRef]
- Siegel, E.L.; Lavoie, N.; Xu, G.; Brown, C.M.; Ledizet, M.; Rich, S.M. Human-Biting Ixodes scapularis Submissions to a Crowd-Funded Tick Testing Program Correlate with the Incidence of Rare Tick-Borne Disease: A Seven-Year Retrospective Study of Anaplasmosis and Babesiosis in Massachusetts. Microorganisms 2023, 11, 1418. [Google Scholar] [CrossRef] [PubMed]
- Schillberg, E.; Lunny, D.; Lindsay, L.R.; Nelder, M.P.; Russell, C.; Mackie, M.; Coats, D.; Berry, A.; Young Hoon, K.N. Distribution of Ixodes scapularis in Northwestern Ontario: Results from Active and Passive Surveillance Activities in the Northwestern Health Unit Catchment Area. Int. J. Environ. Res. Public Health 2018, 15, 2225. [Google Scholar] [CrossRef] [PubMed]
- Mitcham, J.R.; Barrett, A.W.; Gruntmeir, J.M.; Holland, T.; Martin, J.E.; Johnson, E.M.; Little, S.E.; Noden, B.H. Active surveillance to update county scale distribution of four tick species of medical and veterinary importance in Oklahoma. J. Vector Ecol. 2017, 42, 60–73. [Google Scholar] [CrossRef] [PubMed]
- Bisanzio, D.; Fernandez, M.P.; Martello, E.; Reithinger, R.; Diuk-Wasser, M.A. Current and Future Spatiotemporal Patterns of Lyme Disease Reporting in the Northeastern United States. JAMA Netw. Open 2020, 3, e200319. [Google Scholar] [CrossRef] [PubMed]
- Kugeler, K.J.; Cervantes, K.; Brown, C.M.; Horiuchi, K.; Schiffman, E.; Lind, L.; Barkley, J.; Broyhill, J.; Murphy, J.; Crum, D.; et al. Potential quantitative effect of a laboratory-based approach to Lyme disease surveillance in high-incidence states. Zoonoses Public Health 2022, 69, 451–457. [Google Scholar] [CrossRef]
- Ogden, N.H.; Mechai, S.; Margos, G. Changing geographic ranges of ticks and tick-borne pathogens: Drivers, mechanisms and consequences for pathogen diversity. Front. Cell. Infect. Microbiol. 2013, 3, 46. [Google Scholar] [CrossRef]
- Guillot, C.; Bouchard, C.; Buhler, K.; Dumas, A.; Milord, F.; Ripoche, M.; Pelletier, R.; Leighton, P.A. Sentinel Surveillance Contributes to Tracking Lyme Disease Spatiotemporal Risk Trends in Southern Quebec, Canada. Pathogens 2022, 11, 531. [Google Scholar] [CrossRef]
- Jordan, R.A.; Egizi, A. The growing importance of lone star ticks in a Lyme disease endemic county: Passive tick surveillance in Monmouth County, NJ, 2006–2016. PLoS ONE 2019, 14, e0211778. [Google Scholar] [CrossRef]
- Gray, E.B.; Herwaldt, B.L. Babesiosis Surveillance—United States, 2011–2015. MMWR Surveill. Summ. 2019, 68, 1–11. [Google Scholar] [CrossRef]
- Baker, A.; Wang, H.H.; Mogg, M.; Derouen, Z.; Borski, J.; Grant, W.E. Increasing Incidence of Anaplasmosis in the United States, 2012 Through 2016. Vector Borne Zoonotic Dis. 2020, 20, 855–859. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention NNDSS. 2023. Available online: https://wonder.cdc.gov/nndss/static/2020/annual/2020-table1-H.pdf (accessed on 23 August 2023).
- Mead, P.; Hinckley, A.; Hook, S.; Beard, C.B. TickNET-A Collaborative Public Health Approach to Tickborne Disease Surveillance and Research. Emerg. Infect. Dis. 2015, 21, 1574–1577. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.R. Revisiting the Lyme Disease Serodiagnostic Algorithm: The Momentum Gathers. J. Clin. Microbiol. 2018, 56, e00749-18. [Google Scholar] [CrossRef] [PubMed]
- Kingry, L.C.; Anacker, M.; Pritt, B.; Bjork, J.; Respicio-Kingry, L.; Liu, G.; Sheldon, S.; Boxrud, D.; Strain, A.; Oatman, S.; et al. Surveillance for and Discovery of Borrelia Species in US Patients Suspected of Tickborne Illness. Clin. Infect. Dis. 2018, 66, 1864–1871. [Google Scholar] [CrossRef]
- CDC. Tick Surveillance. 2022. Available online: https://www.cdc.gov/ticks/surveillance/TickSurveillanceData.html (accessed on 17 September 2023).
- CDC. ArboNET. 2022. Available online: https://www.cdc.gov/mosquitoes/guidelines/west-nile/surveillance/ArboNET.html (accessed on 17 September 2023).
- Centers for Disease Control and Prevention. Lyme disease—United States, 2003–2005. MMWR Morb. Mortal. Wkly. Rep. 2007, 56, 573–576. [Google Scholar]
- Centers for Disease Control and Prevention. Effect of electronic laboratory reporting on the burden of lyme disease surveillance—New Jersey, 2001–2006. MMWR Morb. Mortal. Wkly. Rep. 2008, 57, 42–45. [Google Scholar]
- Aucott, J.; Morrison, C.; Munoz, B.; Rowe, P.C.; Schwarzwalder, A.; West, S.K. Diagnostic challenges of early Lyme disease: Lessons from a community case series. BMC Infect. Dis. 2009, 9, 79. [Google Scholar] [CrossRef]
- Webber, B.J.; Burganowski, R.P.; Colton, L.; Escobar, J.D.; Pathak, S.R.; Gambino-Shirley, K.J. Lyme disease overdiagnosis in a large healthcare system: A population-based, retrospective study. Clin. Microbiol. Infect. 2019, 25, 1233–1238. [Google Scholar] [CrossRef]
- Moncayo, A.C.; Cohen, S.B.; Fritzen, C.M.; Huang, E.; Yabsley, M.J.; Freye, J.D.; Dunlap, B.G.; Huang, J.; Mead, D.G.; Jones, T.F.; et al. Absence of Rickettsia rickettsii and occurrence of other spotted fever group rickettsiae in ticks from Tennessee. Am. J. Trop. Med. Hyg. 2010, 83, 653–657. [Google Scholar] [CrossRef]
- Tickborne Disease Working Group. Tickborne Disease Working Group 2018 Report to Congress. Available online: https://www.hhs.gov/sites/default/files/tbdwg-report-to-congress-2018.pdf (accessed on 23 August 2023).
- CDC. Surveillance for Ixodes Scapularis and Pathogens Found in this Tick Species in the United States. Available online: https://www.cdc.gov/ticks/resources/TickSurveillance_Iscapularis-P.pdf (accessed on 23 August 2023).
- Maxwell, S.P.; Brooks, C.; Kim, D.; McNeely, C.L.; Cho, S.; Thomas, K.C. Improving Surveillance of Human Tick-Borne Disease Risks: Spatial Analysis Using Multimodal Databases. JMIR Public Health Surveill. 2023, 9, e43790. [Google Scholar] [CrossRef]
- Crist, S.D.; Kopsco, H.; Miller, A.; Gronemeyer, P.; Mateus-Pinilla, N.; Smith, R.L. Knowledge, attitudes, and practices of veterinary professionals towards ticks and tick-borne diseases in Illinois. One Health 2022, 14, 100391. [Google Scholar] [CrossRef] [PubMed]
- Vayssier-Taussat, M.; Cosson, J.F.; Degeilh, B.; Eloit, M.; Fontanet, A.; Moutailler, S.; Raoult, D.; Sellal, E.; Ungeheuer, M.N.; Zylbermann, P. How a multidisciplinary ‘One Health’ approach can combat the tick-borne pathogen threat in Europe. Future Microbiol. 2015, 10, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Mizusawa, M. Updates on Rapid Diagnostic Tests in Infectious Diseases. Mo. Med. 2020, 117, 328–337. [Google Scholar] [PubMed]
- Joung, H.A.; Ballard, Z.S.; Wu, J.; Tseng, D.K.; Teshome, H.; Zhang, L.; Horn, E.J.; Arnaboldi, P.M.; Dattwyler, R.J.; Garner, O.B.; et al. Point-of-Care Serodiagnostic Test for Early-Stage Lyme Disease Using a Multiplexed Paper-Based Immunoassay and Machine Learning. ACS Nano 2020, 14, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Tokarz, R.; Mishra, N.; Tagliafierro, T.; Sameroff, S.; Caciula, A.; Chauhan, L.; Patel, J.; Sullivan, E.; Gucwa, A.; Fallon, B.; et al. A multiplex serologic platform for diagnosis of tick-borne diseases. Sci. Rep. 2018, 8, 3158. [Google Scholar] [CrossRef]
- Moore, A.; Nelson, C.; Molins, C.; Mead, P.; Schriefer, M. Current Guidelines, Common Clinical Pitfalls, and Future Directions for Laboratory Diagnosis of Lyme Disease, United States. Emerg. Infect. Dis. 2016, 22, 1169–1177. [Google Scholar] [CrossRef]
- Wormser, G.P.; Carbonaro, C.; Miller, S.; Nowakowski, J.; Nadelman, R.B.; Sivak, S.; Aguero-Rosenfeld, M.E. A limitation of 2-stage serological testing for Lyme disease: Enzyme immunoassay and immunoblot assay are not independent tests. Clin. Infect. Dis. 2000, 30, 545–548. [Google Scholar] [CrossRef]
- Mohseni, N.; Chang, M.; Garcia, K.; Weakley, M.; Do, T.; Mir, S. Development of a Syndromic Molecular Diagnostic Assay for Tick-Borne Pathogens Using Barcoded Magnetic Bead Technology. Microbiol. Spectr. 2023, 11, e0439522. [Google Scholar] [CrossRef]
- Buehler, J.W.; Hopkins, R.S.; Overhage, J.M.; Sosin, D.M.; Tong, V.; CDC Working Group. Framework for evaluating public health surveillance systems for early detection of outbreaks: Recommendations from the CDC Working Group. MMWR Recomm. Rep. 2004, 53, 1–11. [Google Scholar]
- Lock-Wah-Hoon, J.; Zheng, Y.; Braks, M.; van Asten, L.; Liu, Q.; Sushama, P.; Doreleijers, S.; Krafft, T.; van der Hoek, W.; Fanoy, E.; et al. Exploring Vector-Borne Disease Surveillance and Response Systems in Beijing, China: A Qualitative Study from the Health System Perspective. Int. J. Environ. Res. Public Health 2020, 17, 8512. [Google Scholar] [CrossRef]
- Marx, G.E.; Spillane, M.; Beck, A.; Stein, Z.; Powell, A.K.; Hinckley, A.F. Emergency Department Visits for Tick Bites—United States, January 2017-December 2019. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 612–616. [Google Scholar] [CrossRef] [PubMed]
- Esteve-Gasent, M.D.; Rodriguez-Vivas, R.I.; Medina, R.F.; Ellis, D.; Schwartz, A.; Cortes Garcia, B.; Hunt, C.; Tietjen, M.; Bonilla, D.; Thomas, D.; et al. Research on Integrated Management for Cattle Fever Ticks and Bovine Babesiosis in the United States and Mexico: Current Status and Opportunities for Binational Coordination. Pathogens 2020, 9, 871. [Google Scholar] [CrossRef] [PubMed]
- Hinckley, A.F.; Meek, J.I.; Ray, J.A.; Niesobecki, S.A.; Connally, N.P.; Feldman, K.A.; Jones, E.H.; Backenson, P.B.; White, J.L.; Lukacik, G.; et al. Effectiveness of Residential Acaricides to Prevent Lyme and Other Tick-borne Diseases in Humans. J. Infect. Dis. 2016, 214, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, M.; Muehlenbein, C.; Cartter, M.; Hayes, E.B.; Ertel, S.; Shapiro, E.D. Effectiveness of personal protective measures to prevent Lyme disease. Emerg. Infect. Dis. 2008, 14, 210–216. [Google Scholar] [CrossRef]
- Eisen, L.; Stafford, K.C. Barriers to Effective Tick Management and Tick-Bite Prevention in the United States (Acari: Ixodidae). J. Med. Entomol. 2021, 58, 1588–1600. [Google Scholar] [CrossRef]
- Kitsou, C.; Pal, U. Vaccines Against Vector-Borne Diseases. Methods Mol. Biol. 2022, 2411, 269–286. [Google Scholar]
- Hromnikova, D.; Furka, D.; Furka, S.; Santana, J.A.D.; Ravingerova, T.; Klocklerova, V.; Zitnan, D. Prevention of tick-borne diseases: Challenge to recent medicine. Biologia (Bratisl) 2022, 77, 1533–1554. [Google Scholar] [CrossRef]
- Binder, S.; Sanderson, L.M. The role of the epidemiologist in natural disasters. Ann. Emerg. Med. 1987, 16, 1081–1084. [Google Scholar] [CrossRef]
- Tiffin, H.S.; Rajotte, E.G.; Sakamoto, J.M.; Machtinger, E.T. Tick Control in a Connected World: Challenges, Solutions, and Public Policy from a United States Border Perspective. Trop. Med. Infect. Dis. 2022, 7, 388. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rowan, S.; Mohseni, N.; Chang, M.; Burger, H.; Peters, M.; Mir, S. From Tick to Test: A Comprehensive Review of Tick-Borne Disease Diagnostics and Surveillance Methods in the United States. Life 2023, 13, 2048. https://doi.org/10.3390/life13102048
Rowan S, Mohseni N, Chang M, Burger H, Peters M, Mir S. From Tick to Test: A Comprehensive Review of Tick-Borne Disease Diagnostics and Surveillance Methods in the United States. Life. 2023; 13(10):2048. https://doi.org/10.3390/life13102048
Chicago/Turabian StyleRowan, Sean, Nazleen Mohseni, Mariann Chang, Hannah Burger, Mykah Peters, and Sheema Mir. 2023. "From Tick to Test: A Comprehensive Review of Tick-Borne Disease Diagnostics and Surveillance Methods in the United States" Life 13, no. 10: 2048. https://doi.org/10.3390/life13102048
APA StyleRowan, S., Mohseni, N., Chang, M., Burger, H., Peters, M., & Mir, S. (2023). From Tick to Test: A Comprehensive Review of Tick-Borne Disease Diagnostics and Surveillance Methods in the United States. Life, 13(10), 2048. https://doi.org/10.3390/life13102048