
Diabetes Mellitus in Acute Coronary Syndrome

 , ,
, , 

Abstract
:1. Introduction
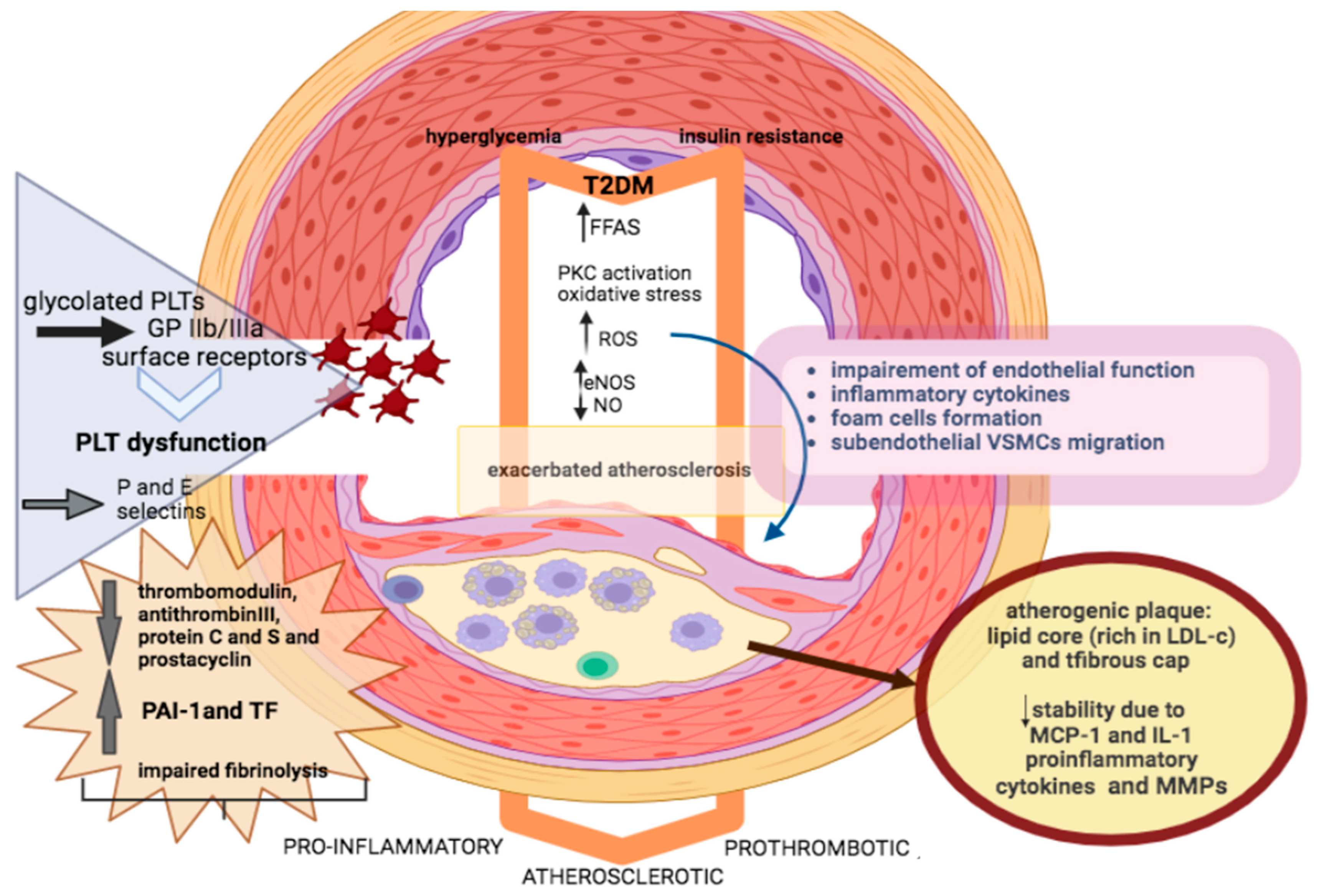
2. Pathophysiology of ACS in Patients with DM
3. Challenges in ACS Presentation and Diagnosis
4. Coronary Lesions in Patients with T2DM
5. Revascularization Strategies
6. Antithrombotic Therapy
7. Glucose Management in the Acute Phase of ACS
8. Newer Antidiabetic Agents for the Post-Acute Phase of ACS
8.1. Sodium Glucose Transporter 2 Inhibitors and Acute Myocardial Infarction
8.2. Mechanism of SGLT2i Beneficial Effects
8.3. Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl-Peptidase-4 Inhibitors in Acute Coronary Syndrome
9. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Standl, E.; Khunti, K.; Hansen, T.B.; Schnell, O. The global epidemics of diabetes in the 21st century: Current situation and perspectives. Eur. J. Prev. Cardiol. 2019, 26, 7–14. [Google Scholar] [CrossRef]
- Task Force on Diabetes, Pre-Diabetes, and Cardiovascular Diseases of the European Society of Cardiology (ESC); Developed in Collaboration with the European Association for the Study of Diabetes (EASD). ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD—Summary. Diabetes Vasc. Dis. Res. 2014, 11, 133–173. [Google Scholar] [CrossRef] [PubMed]
- Babes, E.E.; Bustea, C.; Behl, T.; Abdel-Daim, M.M.; Nechifor, A.C.; Stoicescu, M.; Brisc, C.M.; Moisi, M.; Gitea, D.; Iovanovici, D.C.; et al. Acute coronary syndromes in diabetic patients, outcome, revascularization, and antithrombotic therapy. Biomed. Pharmacother. 2022, 148, 112772. [Google Scholar] [CrossRef]
- Tang, L.; Li, K.; Wu, C.J. Thirty-day readmission, length of stay and self-management behaviour among patients with acute coronary syndrome and type 2 diabetes mellitus: A scoping review. J. Clin. Nurs. 2020, 29, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Oktay, A.A.; Akturk, H.K.; Esenboga, K.; Javed, F.; Polin, N.M.; Jahangir, E. Pathophysiology and Prevention of Heart Disease in Diabetes Mellitus. Curr. Probl. Cardiol. 2018, 43, 68–110. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [PubMed]
- Naito, R.; Kasai, T. Coronary artery disease in type 2 diabetes mellitus: Recent treatment strategies and future perspectives. World J. Cardiol. 2015, 7, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Piga, R.; Naito, Y.; Kokura, S.; Handa, O.; Yoshikawa, T. Short-term high glucose exposure induces monocyte-endothelial cells adhesion and transmigration by increasing VCAM-1 and MCP-1 expression in human aortic endothelial cells. Atherosclerosis 2007, 193, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Sethi, S.S.; Akl, E.G.; Farkouh, M.E. Diabetes mellitus and acute coronary syndrome: Lessons from randomized clinical trials. Curr. Diabetes Rep. 2012, 12, 294–304. [Google Scholar] [CrossRef] [PubMed]
- Cortigiani, L.; Rigo, F.; Gherardi, S.; Galderisi, M.; Bovenzi, F.; Sicari, R. Prognostic meaning of coronary microvascular disease in type 2 diabetes mellitus: A transthoracic Doppler echocardiographic study. J. Am. Soc. Echocardiogr. 2014, 27, 742–748. [Google Scholar] [CrossRef]
- Khan, R.S.; Drosatos, K.; Goldberg, I.J. Creating and curing fatty hearts. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 145–149. [Google Scholar] [CrossRef]
- Alexander, Y.; Osto, E.; Schmidt-Trucksass, A.; Shechter, M.; Trifunovic, D.; Duncker, D.J.; Aboyans, V.; Back, M.; Badimon, L.; Cosentino, F.; et al. Endothelial function in cardiovascular medicine: A consensus paper of the European Society of Cardiology Working Groups on Atherosclerosis and Vascular Biology, Aorta and Peripheral Vascular Diseases, Coronary Pathophysiology and Microcirculation, and Thrombosis. Cardiovasc. Res. 2021, 117, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, E.; Siasos, G.; Tsigkou, V.; Bletsa, E.; Panoilia, M.E.; Oikonomou, I.N.; Simanidis, I.; Spinou, M.; Papastavrou, A.; Kokosias, G.; et al. Coronary Artery Disease and Endothelial Dysfunction: Novel Diagnostic and Therapeutic Approaches. Curr. Med. Chem. 2020, 27, 1052–1080. [Google Scholar] [CrossRef]
- Grandl, G.; Wolfrum, C. Hemostasis, endothelial stress, inflammation, and the metabolic syndrome. Semin. Immunopathol. 2018, 40, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Q.; Wang, D.; Li, D.; Huang, J.; Ma, F.; Zhang, H.; Sheng, Y.; Zhang, C.; Ha, X. Protein kinase C: A potential therapeutic target for endothelial dysfunction in diabetes. J. Diabetes Complicat. 2023, 37, 108565. [Google Scholar] [CrossRef]
- Chang, T.C.; Huang, C.J.; Tam, K.; Chen, S.F.; Tan, K.T.; Tsai, M.S.; Lin, T.N.; Shyue, S.K. Stabilization of hypoxia-inducible factor-1alpha by prostacyclin under prolonged hypoxia via reducing reactive oxygen species level in endothelial cells. J. Biol. Chem. 2005, 280, 36567–36574. [Google Scholar] [CrossRef] [PubMed]
- Yuan, T.; Yang, T.; Chen, H.; Fu, D.; Hu, Y.; Wang, J.; Yuan, Q.; Yu, H.; Xu, W.; Xie, X. New insights into oxidative stress and inflammation during diabetes mellitus-accelerated atherosclerosis. Redox Biol. 2019, 20, 247–260. [Google Scholar] [CrossRef]
- Forbes, J.M.; Cooper, M.E. Mechanisms of diabetic complications. Physiol. Rev. 2013, 93, 137–188. [Google Scholar] [CrossRef]
- Poznyak, A.; Grechko, A.V.; Poggio, P.; Myasoedova, V.A.; Alfieri, V.; Orekhov, A.N. The Diabetes Mellitus-Atherosclerosis Connection: The Role of Lipid and Glucose Metabolism and Chronic Inflammation. Int. J. Mol. Sci. 2020, 21, 1835. [Google Scholar] [CrossRef]
- Rabbani, N.; Godfrey, L.; Xue, M.; Shaheen, F.; Geoffrion, M.; Milne, R.; Thornalley, P.J. Glycation of LDL by methylglyoxal increases arterial atherogenicity: A possible contributor to increased risk of cardiovascular disease in diabetes. Diabetes 2011, 60, 1973–1980. [Google Scholar] [CrossRef]
- Beckman, J.A.; Creager, M.A.; Libby, P. Diabetes and atherosclerosis: Epidemiology, pathophysiology, and management. JAMA 2002, 287, 2570–2581. [Google Scholar] [CrossRef] [PubMed]
- Trichon, B.H.; Roe, M.T. Acute coronary syndromes and diabetes mellitus. Diabetes Vasc. Dis. Res. 2004, 1, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Lee, H.; Hu, L.; Lu, L.; Shen, G.X. Impact of diabetes-associated lipoproteins on generation of fibrinolytic regulators from vascular endothelial cells. J. Clin. Endocrinol. Metab. 2002, 87, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.K.; Kalra, S. The Diabetic Platelets. J. Pak. Med. Assoc. 2023, 73, 1130–1133. [Google Scholar] [CrossRef] [PubMed]
- Razmara, M.; Hjemdahl, P.; Ostenson, C.G.; Li, N. Platelet hyperprocoagulant activity in Type 2 diabetes mellitus: Attenuation by glycoprotein IIb/IIIa inhibition. J. Thromb. Haemost. 2008, 6, 2186–2192. [Google Scholar] [CrossRef]
- Patti, G.; Cavallari, I.; Andreotti, F.; Calabro, P.; Cirillo, P.; Denas, G.; Galli, M.; Golia, E.; Maddaloni, E.; Marcucci, R.; et al. Prevention of atherothrombotic events in patients with diabetes mellitus: From antithrombotic therapies to new-generation glucose-lowering drugs. Nat. Rev. Cardiol. 2019, 16, 113–130. [Google Scholar] [CrossRef] [PubMed]
- Aronson, D.; Bloomgarden, Z.; Rayfield, E.J. Potential mechanisms promoting restenosis in diabetic patients. J. Am. Coll. Cardiol. 1996, 27, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Saito, I.; Folsom, A.R.; Brancati, F.L.; Duncan, B.B.; Chambless, L.E.; McGovern, P.G. Nontraditional risk factors for coronary heart disease incidence among persons with diabetes: The Atherosclerosis Risk in Communities (ARIC) Study. Ann. Intern. Med. 2000, 133, 81–91. [Google Scholar] [CrossRef]
- Altalhi, R.; Pechlivani, N.; Ajjan, R.A. PAI-1 in Diabetes: Pathophysiology and Role as a Therapeutic Target. Int. J. Mol. Sci. 2021, 22, 3170. [Google Scholar] [CrossRef]
- Babes, E.E.; Zaha, D.C.; Tit, D.M.; Nechifor, A.C.; Bungau, S.; Andronie-Cioara, F.L.; Behl, T.; Stoicescu, M.; Munteanu, M.A.; Rus, M.; et al. Value of Hematological and Coagulation Parameters as Prognostic Factors in Acute Coronary Syndromes. Diagnostics 2021, 11, 850. [Google Scholar] [CrossRef]
- Mak, K.H.; Faxon, D.P. Clinical studies on coronary revascularization in patients with type 2 diabetes. Eur. Heart J. 2003, 24, 1087–1103. [Google Scholar] [CrossRef] [PubMed]
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Prevalence of cardiovascular disease in type 2 diabetes: A systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc. Diabetol. 2018, 17, 83. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, B.; Shah, G.K.; Randhawa, M.; Ellis, S.G.; Lincoff, A.M.; Menon, V. Utility of Glycated Hemoglobin for Assessment of Glucose Metabolism in Patients With ST-Segment Elevation Myocardial Infarction. Am. J. Cardiol. 2016, 117, 749–753. [Google Scholar] [CrossRef]
- Marx, N.; Federici, M.; Schutt, K.; Muller-Wieland, D.; Ajjan, R.A.; Antunes, M.J.; Christodorescu, R.M.; Crawford, C.; Di Angelantonio, E.; Eliasson, B.; et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur. Heart J. 2023, 44, 4043–4140. [Google Scholar] [CrossRef]
- ACE Inhibitor Myocardial Infarction Collaborative Group. Indications for ACE inhibitors in the early treatment of acute myocardial infarction: Systematic overview of individual data from 100,000 patients in randomized trials. Circulation 1998, 97, 2202–2212. [Google Scholar] [CrossRef] [PubMed]
- Le Feuvre, C.; Jacqueminet, S.; Barthelemy, O. Myocardial ischemia: A silent epidemic in Type 2 diabetes patients. Future Cardiol. 2011, 7, 183–190. [Google Scholar] [CrossRef]
- Yahagi, K.; Kolodgie, F.D.; Lutter, C.; Mori, H.; Romero, M.E.; Finn, A.V.; Virmani, R. Pathology of Human Coronary and Carotid Artery Atherosclerosis and Vascular Calcification in Diabetes Mellitus. Arter. Thromb. Vasc. Biol. 2017, 37, 191–204. [Google Scholar] [CrossRef]
- Kittnar, O. Electrocardiographic changes in diabetes mellitus. Physiol. Res. 2015, 64, S559–S566. [Google Scholar] [CrossRef] [PubMed]
- Busch, N.; Jensen, M.T.; Goetze, J.P.; Schou, M.; Biering-Sorensen, T.; Fritz-Hansen, T.; Andersen, H.U.; Vilsboll, T.; Rossing, P.; Jorgensen, P.G. Prognostic and comparative performance of cardiovascular risk markers in patients with type 2 diabetes. J. Diabetes 2021, 13, 754–763. [Google Scholar] [CrossRef]
- Jehn, S.; Roggel, A.; Dykun, I.; Balcer, B.; Al-Rashid, F.; Totzeck, M.; Risse, J.; Kill, C.; Rassaf, T.; Mahabadi, A.A. Epicardial adipose tissue and obstructive coronary artery disease in acute chest pain: The EPIC-ACS study. Eur. Heart J. Open 2023, 3, oead041. [Google Scholar] [CrossRef]
- Hendricks, S.; Dykun, I.; Balcer, B.; Totzeck, M.; Rassaf, T.; Mahabadi, A.A. Epicardial adipose tissue is a robust measure of increased risk of myocardial infarction—A meta-analysis on over 6600 patients and rationale for the EPIC-ACS study. Medicine 2021, 100, e28060. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Liu, X.; Adhikari, B.K.; Chen, L.; Liu, W.; Wang, Y.; Zhang, H. The role of epicardial adipose tissue dysfunction in cardiovascular diseases: An overview of pathophysiology, evaluation, and management. Front. Endocrinol. 2023, 14, 1167952. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.B.; Shah, S.; Verma, S.; Oudit, G.Y. Epicardial adipose tissue as a metabolic transducer: Role in heart failure and coronary artery disease. Heart Fail. Rev. 2017, 22, 889–902. [Google Scholar] [CrossRef]
- Hardin, N.J. The myocardial and vascular pathology of diabetic cardiomyopathy. Coron. Artery Dis. 1996, 7, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Cassar, A.; Holmes, D.R., Jr.; Rihal, C.S.; Gersh, B.J. Chronic coronary artery disease: Diagnosis and management. Mayo Clin. Proc. 2009, 84, 1130–1146. [Google Scholar] [CrossRef]
- Matsuzawa, Y.; Lerman, A. Endothelial dysfunction and coronary artery disease: Assessment, prognosis, and treatment. Coron. Artery Dis. 2014, 25, 713–724. [Google Scholar] [CrossRef]
- Mintz, G.S.; Popma, J.J.; Pichard, A.D.; Kent, K.M.; Satler, L.F.; Chuang, Y.C.; DeFalco, R.A.; Leon, M.B. Limitations of angiography in the assessment of plaque distribution in coronary artery disease: A systematic study of target lesion eccentricity in 1446 lesions. Circulation 1996, 93, 924–931. [Google Scholar] [CrossRef]
- Chawla, A.; Chawla, R.; Jaggi, S. Microvasular and macrovascular complications in diabetes mellitus: Distinct or continuum? Indian. J. Endocrinol. Metab. 2016, 20, 546–551. [Google Scholar] [CrossRef]
- Schnell, O.; Schwarz, A.; Muhr-Becker, D.; Standl, E. Autoantibodies against autonomic nervous tissues in type 2 diabetes mellitus: No association with cardiac autonomic dysfunction. Exp. Clin. Endocrinol. Diabetes 2000, 108, 181–186. [Google Scholar] [CrossRef]
- Gimbrone, M.A., Jr.; Garcia-Cardena, G. Endothelial Cell Dysfunction and the Pathobiology of Atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef] [PubMed]
- Milzi, A.; Burgmaier, M.; Burgmaier, K.; Hellmich, M.; Marx, N.; Reith, S. Type 2 diabetes mellitus is associated with a lower fibrous cap thickness but has no impact on calcification morphology: An intracoronary optical coherence tomography study. Cardiovasc. Diabetol. 2017, 16, 152. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Yamamoto, E.; Bryniarski, K.; Xing, L.; Fracassi, F.; Lee, H.; Jang, I.K. Coronary Plaque Characteristics in Patients With Diabetes Mellitus Who Presented With Acute Coronary Syndromes. J. Am. Heart Assoc. 2018, 7, 009245. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Arora, R.; Kodumuri, V.; Khosla, S.; Jawad, E. Coronary revascularization in diabetic patients: Current state of evidence. Exp. Clin. Cardiol. 2011, 16, 16–22. [Google Scholar] [PubMed]
- Ibrahimov, F.; Yilmaz, Y.; Ismayilov, I.; Musayev, K.; Musayev, O.O.; Alasgarli, S.; Shahbazova, S.; Isgenderova, M.; Jahangirov, T. Comparing 5-year Outcomes of Aorta-Coronary Bypass Surgery and Percutaneous Coronary Intervention Performed with New-Generation Drug-Eluting Stents in Non-Diabetic Patients with Multivessel Acute Coronary Syndrome Patients and Intermediate Syntax Score. Medeni. Med. J. 2020, 35, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]
- Godoy, L.C.; Rao, V.; Farkouh, M.E. Coronary Revascularization of Patients With Diabetes Mellitus in the Setting of Acute Coronary Syndromes. Circulation 2019, 140, 1233–1235. [Google Scholar] [CrossRef]
- Lambert, D.; Mattia, A.; Hsu, A.; Manetta, F. CABG versus PCI in the Treatment of Unprotected Left Main Disease in Diabetics: A Literature Review. Int J Angiol. 2021, 30, 187–193. [Google Scholar] [CrossRef]
- Buntaine, A.J.; Shah, B.; Lorin, J.D.; Sedlis, S.P. Revascularization Strategies in Patients with Diabetes Mellitus and Acute Coronary Syndrome. Curr. Cardiol. Rep. 2016, 18, 79. [Google Scholar] [CrossRef]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Van Belle, E.; Baptista, S.B.; Raposo, L.; Henderson, J.; Rioufol, G.; Santos, L.; Pouillot, C.; Ramos, R.; Cuisset, T.; Cale, R.; et al. Impact of Routine Fractional Flow Reserve on Management Decision and 1-Year Clinical Outcome of Patients With Acute Coronary Syndromes: PRIME-FFR (Insights From the POST-IT [Portuguese Study on the Evaluation of FFR-Guided Treatment of Coronary Disease] and R3F [French FFR Registry] Integrated Multicenter Registries—Implementation of FFR [Fractional Flow Reserve] in Routine Practice). Circ. Cardiovasc. Interv. 2017, 10, e004296. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthelemy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Sorrentino, S.; Baber, U.; Claessen, B.E.; Camaj, A.; Vogel, B.; Sartori, S.; Guedeney, P.; Chandrasekhar, J.; Farhan, S.; Barman, N.; et al. Determinants of Significant Out-Of-Hospital Bleeding in Patients Undergoing Percutaneous Coronary Intervention. Thromb. Haemost. 2018, 118, 1997–2005. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.; Kaur, M.; Singh, J. Endothelial dysfunction and platelet hyperactivity in type 2 diabetes mellitus: Molecular insights and therapeutic strategies. Cardiovasc. Diabetol. 2018, 17, 121. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Patel, A.; Dharmashankar, K.; Ferreiro, J.L.; Ueno, M.; Kodali, M.; Tomasello, S.D.; Capranzano, P.; Seecheran, N.; Darlington, A.; et al. Pharmacodynamic effects of different aspirin dosing regimens in type 2 diabetes mellitus patients with coronary artery disease. Circ. Cardiovasc. Interv. 2011, 4, 180–187. [Google Scholar] [CrossRef]
- Mehta, S.R.; Tanguay, J.F.; Eikelboom, J.W.; Jolly, S.S.; Joyner, C.D.; Granger, C.B.; Faxon, D.P.; Rupprecht, H.J.; Budaj, A.; Avezum, A.; et al. Double-dose versus standard-dose clopidogrel and high-dose versus low-dose aspirin in individuals undergoing percutaneous coronary intervention for acute coronary syndromes (CURRENT-OASIS 7): A randomised factorial trial. Lancet 2010, 376, 1233–1243. [Google Scholar] [CrossRef]
- Roffi, M.; Chew, D.P.; Mukherjee, D.; Bhatt, D.L.; White, J.A.; Heeschen, C.; Hamm, C.W.; Moliterno, D.J.; Califf, R.M.; White, H.D.; et al. Platelet glycoprotein IIb/IIIa inhibitors reduce mortality in diabetic patients with non-ST-segment-elevation acute coronary syndromes. Circulation 2001, 104, 2767–2771. [Google Scholar] [CrossRef]
- Giugliano, R.P.; White, J.A.; Bode, C.; Armstrong, P.W.; Montalescot, G.; Lewis, B.S.; van’t Hof, A.; Berdan, L.G.; Lee, K.L.; Strony, J.T.; et al. Early versus delayed, provisional eptifibatide in acute coronary syndromes. N. Engl. J. Med. 2009, 360, 2176–2190. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E., Jr.; Ganiats, T.G.; Holmes, D.R., Jr.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am. Coll. Cardiol. 2014, 64, e139–e228. [Google Scholar] [CrossRef]
- Investigators, N.-S.S.; Finfer, S.; Chittock, D.R.; Su, S.Y.; Blair, D.; Foster, D.; Dhingra, V.; Bellomo, R.; Cook, D.; Dodek, P.; et al. Intensive versus conventional glucose control in critically ill patients. N. Engl. J. Med. 2009, 360, 1283–1297. [Google Scholar] [CrossRef]
- Malmberg, K.; Ryden, L.; Efendic, S.; Herlitz, J.; Nicol, P.; Waldenstrom, A.; Wedel, H.; Welin, L. Randomized trial of insulin-glucose infusion followed by subcutaneous insulin treatment in diabetic patients with acute myocardial infarction (DIGAMI study): Effects on mortality at 1 year. J. Am. Coll. Cardiol. 1995, 26, 57–65. [Google Scholar] [CrossRef]
- Malmberg, K. Prospective randomised study of intensive insulin treatment on long term survival after acute myocardial infarction in patients with diabetes mellitus. DIGAMI (Diabetes Mellitus, Insulin Glucose Infusion in Acute Myocardial Infarction) Study Group. BMJ 1997, 314, 1512–1515. [Google Scholar] [CrossRef]
- Malmberg, K.; Ryden, L.; Wedel, H.; Birkeland, K.; Bootsma, A.; Dickstein, K.; Efendic, S.; Fisher, M.; Hamsten, A.; Herlitz, J.; et al. Intense metabolic control by means of insulin in patients with diabetes mellitus and acute myocardial infarction (DIGAMI 2): Effects on mortality and morbidity. Eur. Heart J. 2005, 26, 650–661. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N.W.; Wong, V.W.; McLean, M. The Hyperglycemia: Intensive Insulin Infusion in Infarction (HI-5) study: A randomized controlled trial of insulin infusion therapy for myocardial infarction. Diabetes Care 2006, 29, 765–770. [Google Scholar] [CrossRef]
- Ceremuzynski, L.; Budaj, A.; Czepiel, A.; Burzykowski, T.; Achremczyk, P.; Smielak-Korombel, W.; Maciejewicz, J.; Dziubinska, J.; Nartowicz, E.; Kawka-Urbanek, T.; et al. Low-dose glucose-insulin-potassium is ineffective in acute myocardial infarction: Results of a randomized multicenter Pol-GIK trial. Cardiovasc. Drugs Ther. 1999, 13, 191–200. [Google Scholar] [CrossRef]
- de Koning, M.L.; van Dorp, P.; Assa, S.; Hartman, M.H.; Voskuil, M.; Anthonio, R.L.; Veen, D.; Pundziute-Do Prado, G.; Leiner, T.; van Goor, H.; et al. Rationale and Design of the Groningen Intervention Study for the Preservation of Cardiac Function with Sodium Thiosulfate after St-segment Elevation Myocardial Infarction (GIPS-IV) trial. Am. Heart J. 2022, 243, 167–176. [Google Scholar] [CrossRef]
- Mehta, S.R.; Yusuf, S.; Diaz, R.; Zhu, J.; Pais, P.; Xavier, D.; Paolasso, E.; Ahmed, R.; Xie, C.; Kazmi, K.; et al. Effect of glucose-insulin-potassium infusion on mortality in patients with acute ST-segment elevation myocardial infarction: The CREATE-ECLA randomized controlled trial. JAMA 2005, 293, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Gnaim, C.I.; McGuire, D.K. Glucose-insulin-potassium therapy for acute myocardial infarction: What goes around comes around. Am. Heart J. 2004, 148, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Siasos, G.; Stampouloglou, P.K.; Bletsa, E.; Paschou, S.A.; Oikonomou, E.; Giannopoulos, G.; Deftereos, S.; Cleman, M.W.; Tousoulis, D. SGLT-2i and Cardiovascular Prognosis. Curr. Pharm. Des. 2020, 26, 3905–3907. [Google Scholar] [CrossRef] [PubMed]
- Lan, N.S.R.; Yeap, B.B.; Fegan, P.G.; Green, G.; Rankin, J.M.; Dwivedi, G. Empagliflozin and left ventricular diastolic function following an acute coronary syndrome in patients with type 2 diabetes. Int. J. Cardiovasc. Imaging 2021, 37, 517–527. [Google Scholar] [CrossRef] [PubMed]
- Udell, J.A.; Jones, W.S.; Petrie, M.C.; Harrington, J.; Anker, S.D.; Bhatt, D.L.; Hernandez, A.F.; Butler, J. Sodium Glucose Cotransporter-2 Inhibition for Acute Myocardial Infarction: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2022, 79, 2058–2068. [Google Scholar] [CrossRef]
- White, W.B.; Cannon, C.P.; Heller, S.R.; Nissen, S.E.; Bergenstal, R.M.; Bakris, G.L.; Perez, A.T.; Fleck, P.R.; Mehta, C.R.; Kupfer, S.; et al. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N. Engl. J. Med. 2013, 369, 1327–1335. [Google Scholar] [CrossRef]
- Pfeffer, M.A.; Claggett, B.; Diaz, R.; Dickstein, K.; Gerstein, H.C.; Kober, L.V.; Lawson, F.C.; Ping, L.; Wei, X.; Lewis, E.F.; et al. Lixisenatide in Patients with Type 2 Diabetes and Acute Coronary Syndrome. N. Engl. J. Med. 2015, 373, 2247–2257. [Google Scholar] [CrossRef]
- Shimizu, W.; Kubota, Y.; Hoshika, Y.; Mozawa, K.; Tara, S.; Tokita, Y.; Yodogawa, K.; Iwasaki, Y.K.; Yamamoto, T.; Takano, H.; et al. Effects of empagliflozin versus placebo on cardiac sympathetic activity in acute myocardial infarction patients with type 2 diabetes mellitus: The EMBODY trial. Cardiovasc. Diabetol. 2020, 19, 148. [Google Scholar] [CrossRef] [PubMed]
- von Lewinski, D.; Kolesnik, E.; Tripolt, N.J.; Pferschy, P.N.; Benedikt, M.; Wallner, M.; Alber, H.; Berger, R.; Lichtenauer, M.; Saely, C.H.; et al. Empagliflozin in acute myocardial infarction: The EMMY trial. Eur. Heart J. 2022, 43, 4421–4432. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhang, J.L.; Yan, X.J.; Sun, L.; Ji, Y.; Wang, F.F. Effect of dapagliflozin on the prognosis of patients with acute myocardial infarction undergoing percutaneous coronary intervention. Cardiovasc. Diabetol. 2022, 21, 186. [Google Scholar] [CrossRef] [PubMed]
- Paolisso, P.; Bergamaschi, L.; Gragnano, F.; Gallinoro, E.; Cesaro, A.; Sardu, C.; Mileva, N.; Foa, A.; Armillotta, M.; Sansonetti, A.; et al. Outcomes in diabetic patients treated with SGLT2-Inhibitors with acute myocardial infarction undergoing PCI: The SGLT2-I AMI PROTECT Registry. Pharmacol. Res. 2023, 187, 106597. [Google Scholar] [CrossRef] [PubMed]
- Radholm, K.; Figtree, G.; Perkovic, V.; Solomon, S.D.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Barrett, T.D.; Shaw, W.; Desai, M.; et al. Canagliflozin and Heart Failure in Type 2 Diabetes Mellitus: Results From the CANVAS Program. Circulation 2018, 138, 458–468. [Google Scholar] [CrossRef]
- Kato, E.T.; Silverman, M.G.; Mosenzon, O.; Zelniker, T.A.; Cahn, A.; Furtado, R.H.M.; Kuder, J.; Murphy, S.A.; Bhatt, D.L.; Leiter, L.A.; et al. Effect of Dapagliflozin on Heart Failure and Mortality in Type 2 Diabetes Mellitus. Circulation 2019, 139, 2528–2536. [Google Scholar] [CrossRef]
- Wanner, C.; Lachin, J.M.; Inzucchi, S.E.; Fitchett, D.; Mattheus, M.; George, J.; Woerle, H.J.; Broedl, U.C.; von Eynatten, M.; Zinman, B.; et al. Empagliflozin and Clinical Outcomes in Patients With Type 2 Diabetes Mellitus, Established Cardiovascular Disease, and Chronic Kidney Disease. Circulation 2018, 137, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Peikert, A.; Chandra, A.; Kosiborod, M.N.; Claggett, B.L.; Desai, A.S.; Jhund, P.S.; Lam, C.S.P.; Inzucchi, S.E.; Martinez, F.A.; de Boer, R.A.; et al. Association of Dapagliflozin vs Placebo With Individual Kansas City Cardiomyopathy Questionnaire Components in Patients With Heart Failure With Mildly Reduced or Preserved Ejection Fraction: A Secondary Analysis of the DELIVER Trial. JAMA Cardiol. 2023, 8, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Salah, H.M.; Al’Aref, S.J.; Khan, M.S.; Al-Hawwas, M.; Vallurupalli, S.; Mehta, J.L.; Mounsey, J.P.; Greene, S.J.; McGuire, D.K.; Lopes, R.D.; et al. Efficacy and safety of sodium-glucose cotransporter 2 inhibitors initiation in patients with acute heart failure, with and without type 2 diabetes: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2022, 21, 20. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Szarek, M.; Steg, P.G.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Voors, A.A.; Metra, M.; et al. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N. Engl. J. Med. 2021, 384, 117–128. [Google Scholar] [CrossRef]
- Baird, J.K.; Sherwood, R.F.; Carr, R.J.; Atkinson, A. Enzyme purification by substrate elution chromatography from procion dye-polysaccharide matrices. FEBS Lett. 1976, 70, 61–66. [Google Scholar] [CrossRef]
- Lahnwong, S.; Palee, S.; Apaijai, N.; Sriwichaiin, S.; Kerdphoo, S.; Jaiwongkam, T.; Chattipakorn, S.C.; Chattipakorn, N. Acute dapagliflozin administration exerts cardioprotective effects in rats with cardiac ischemia/reperfusion injury. Cardiovasc. Diabetol. 2020, 19, 91. [Google Scholar] [CrossRef] [PubMed]
- Nikolaou, P.E.; Efentakis, P.; Abu Qourah, F.; Femmino, S.; Makridakis, M.; Kanaki, Z.; Varela, A.; Tsoumani, M.; Davos, C.H.; Dimitriou, C.A.; et al. Chronic Empagliflozin Treatment Reduces Myocardial Infarct Size in Nondiabetic Mice Through STAT-3-Mediated Protection on Microvascular Endothelial Cells and Reduction of Oxidative Stress. Antioxid. Redox Signal 2021, 34, 551–571. [Google Scholar] [CrossRef] [PubMed]
- Harrington, J.; Udell, J.A.; Jones, W.S.; Anker, S.D.; Bhatt, D.L.; Petrie, M.C.; Vedin, O.; Sumin, M.; Zwiener, I.; Hernandez, A.F.; et al. Empagliflozin in patients post myocardial infarction rationale and design of the EMPACT-MI trial. Am. Heart J. 2022, 253, 86–98. [Google Scholar] [CrossRef]
- Cortés, M.; Lorenzo, O.; Lumpuy-Castillo, J.; Martínez-Albaladejo, S.; Taibo-Urquía, M.; Pello, A.M.; Bollas, A.J.; Orejas, M.; Navas, M.Á.; Macia, E.; et al. Dapagliflozin Improved Cardiac Function and Structure in Diabetic Patients with Preserved Ejection Fraction: Results of a Single Centre, Observational Prospective Study. J Clin Med 2023, 23, 6698. [Google Scholar] [CrossRef]
- Kappel, B.A.; Lehrke, M.; Schutt, K.; Artati, A.; Adamski, J.; Lebherz, C.; Marx, N. Effect of Empagliflozin on the Metabolic Signature of Patients With Type 2 Diabetes Mellitus and Cardiovascular Disease. Circulation 2017, 136, 969–972. [Google Scholar] [CrossRef] [PubMed]
- Yurista, S.R.; Sillje, H.H.W.; Oberdorf-Maass, S.U.; Schouten, E.M.; Pavez Giani, M.G.; Hillebrands, J.L.; van Goor, H.; van Veldhuisen, D.J.; de Boer, R.A.; Westenbrink, B.D. Sodium-glucose co-transporter 2 inhibition with empagliflozin improves cardiac function in non-diabetic rats with left ventricular dysfunction after myocardial infarction. Eur. J. Heart Fail. 2019, 21, 862–873. [Google Scholar] [CrossRef]
- Snorek, M.; Hodyc, D.; Sedivy, V.; Durisova, J.; Skoumalova, A.; Wilhelm, J.; Neckar, J.; Kolar, F.; Herget, J. Short-term fasting reduces the extent of myocardial infarction and incidence of reperfusion arrhythmias in rats. Physiol. Res. 2012, 61, 567–574. [Google Scholar] [CrossRef]
- Horton, J.L.; Davidson, M.T.; Kurishima, C.; Vega, R.B.; Powers, J.C.; Matsuura, T.R.; Petucci, C.; Lewandowski, E.D.; Crawford, P.A.; Muoio, D.M.; et al. The failing heart utilizes 3-hydroxybutyrate as a metabolic stress defense. JCI Insight 2019, 4, e124079. [Google Scholar] [CrossRef] [PubMed]
- Mudaliar, S.; Alloju, S.; Henry, R.R. Can a Shift in Fuel Energetics Explain the Beneficial Cardiorenal Outcomes in the EMPA-REG OUTCOME Study? A Unifying Hypothesis. Diabetes Care 2016, 39, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Clanachan, A.S. Contribution of protons to post-ischemic Na(+) and Ca(2+) overload and left ventricular mechanical dysfunction. J. Cardiovasc. Electrophysiol. 2006, 17 (Suppl. S1), S141–S148. [Google Scholar] [CrossRef]
- Jennings, R.B.; Murry, C.E.; Steenbergen, C., Jr.; Reimer, K.A. Development of cell injury in sustained acute ischemia. Circulation 1990, 82, II2-12. [Google Scholar]
- Jun, S.; Aon, M.A.; Paolocci, N. Empagliflozin and HFrEF: Known and Possible Benefits of NHE1 Inhibition. JACC Basic. Transl. Sci. 2019, 4, 841–844. [Google Scholar] [CrossRef]
- Uthman, L.; Nederlof, R.; Eerbeek, O.; Baartscheer, A.; Schumacher, C.; Buchholtz, N.; Hollmann, M.W.; Coronel, R.; Weber, N.C.; Zuurbier, C.J. Delayed ischaemic contracture onset by empagliflozin associates with NHE1 inhibition and is dependent on insulin in isolated mouse hearts. Cardiovasc. Res. 2019, 115, 1533–1545. [Google Scholar] [CrossRef]
- Uthman, L.; Baartscheer, A.; Bleijlevens, B.; Schumacher, C.A.; Fiolet, J.W.T.; Koeman, A.; Jancev, M.; Hollmann, M.W.; Weber, N.C.; Coronel, R.; et al. Class effects of SGLT2 inhibitors in mouse cardiomyocytes and hearts: Inhibition of Na(+)/H(+) exchanger, lowering of cytosolic Na(+) and vasodilation. Diabetologia 2018, 61, 722–726. [Google Scholar] [CrossRef]
- Baker, H.E.; Kiel, A.M.; Luebbe, S.T.; Simon, B.R.; Earl, C.C.; Regmi, A.; Roell, W.C.; Mather, K.J.; Tune, J.D.; Goodwill, A.G. Inhibition of sodium-glucose cotransporter-2 preserves cardiac function during regional myocardial ischemia independent of alterations in myocardial substrate utilization. Basic. Res. Cardiol. 2019, 114, 25. [Google Scholar] [CrossRef]
- Trum, M.; Riechel, J.; Lebek, S.; Pabel, S.; Sossalla, S.T.; Hirt, S.; Arzt, M.; Maier, L.S.; Wagner, S. Empagliflozin inhibits Na(+) /H(+) exchanger activity in human atrial cardiomyocytes. ESC Heart Fail. 2020, 7, 4429–4437. [Google Scholar] [CrossRef]
- Uthman, L.; Li, X.; Baartscheer, A.; Schumacher, C.A.; Baumgart, P.; Hermanides, J.; Preckel, B.; Hollmann, M.W.; Coronel, R.; Zuurbier, C.J.; et al. Empagliflozin reduces oxidative stress through inhibition of the novel inflammation/NHE/[Na(+)](c)/ROS-pathway in human endothelial cells. Biomed. Pharmacother. 2022, 146, 112515. [Google Scholar] [CrossRef]
- Cesaro, A.; Gragnano, F.; Paolisso, P.; Bergamaschi, L.; Gallinoro, E.; Sardu, C.; Mileva, N.; Foa, A.; Armillotta, M.; Sansonetti, A.; et al. In-hospital arrhythmic burden reduction in diabetic patients with acute myocardial infarction treated with SGLT2-inhibitors: Insights from the SGLT2-I AMI PROTECT study. Front. Cardiovasc. Med. 2022, 9, 1012220. [Google Scholar] [CrossRef] [PubMed]
- Curtain, J.P.; Docherty, K.F.; Jhund, P.S.; Petrie, M.C.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; et al. Effect of dapagliflozin on ventricular arrhythmias, resuscitated cardiac arrest, or sudden death in DAPA-HF. Eur. Heart J. 2021, 42, 3727–3738. [Google Scholar] [CrossRef] [PubMed]
- Li, H.L.; Lip, G.Y.H.; Feng, Q.; Fei, Y.; Tse, Y.K.; Wu, M.Z.; Ren, Q.W.; Tse, H.F.; Cheung, B.Y.; Yiu, K.H. Correction to: Sodium-glucose cotransporter 2 inhibitors (SGLT2i) and cardiac arrhythmias: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2021, 20, 177. [Google Scholar] [CrossRef]
- Hu, Z.; Ju, F.; Du, L.; Abbott, G.W. Empagliflozin protects the heart against ischemia/reperfusion-induced sudden cardiac death. Cardiovasc. Diabetol. 2021, 20, 199. [Google Scholar] [CrossRef]
- Azam, M.A.; Chakraborty, P.; Si, D.; Du, B.; Masse, S.; Lai, P.F.H.; Ha, A.C.T.; Nanthakumar, K. Anti-arrhythmic and inotropic effects of empagliflozin following myocardial ischemia. Life Sci. 2021, 276, 119440. [Google Scholar] [CrossRef] [PubMed]
- Durak, A.; Olgar, Y.; Degirmenci, S.; Akkus, E.; Tuncay, E.; Turan, B. A SGLT2 inhibitor dapagliflozin suppresses prolonged ventricular-repolarization through augmentation of mitochondrial function in insulin-resistant metabolic syndrome rats. Cardiovasc. Diabetol. 2018, 17, 144. [Google Scholar] [CrossRef]
- Wan, N.; Rahman, A.; Hitomi, H.; Nishiyama, A. The Effects of Sodium-Glucose Cotransporter 2 Inhibitors on Sympathetic Nervous Activity. Front. Endocrinol. 2018, 9, 421. [Google Scholar] [CrossRef]
- Wohlfart, P.; Linz, W.; Hubschle, T.; Linz, D.; Huber, J.; Hess, S.; Crowther, D.; Werner, U.; Ruetten, H. Cardioprotective effects of lixisenatide in rat myocardial ischemia-reperfusion injury studies. J. Transl. Med. 2013, 11, 84. [Google Scholar] [CrossRef] [PubMed]
- Bao, W.; Aravindhan, K.; Alsaid, H.; Chendrimada, T.; Szapacs, M.; Citerone, D.R.; Harpel, M.R.; Willette, R.N.; Lepore, J.J.; Jucker, B.M. Albiglutide, a long lasting glucagon-like peptide-1 analog, protects the rat heart against ischemia/reperfusion injury: Evidence for improving cardiac metabolic efficiency. PLoS ONE 2011, 6, e23570. [Google Scholar] [CrossRef] [PubMed]
- Noyan-Ashraf, M.H.; Momen, M.A.; Ban, K.; Sadi, A.M.; Zhou, Y.Q.; Riazi, A.M.; Baggio, L.L.; Henkelman, R.M.; Husain, M.; Drucker, D.J. GLP-1R agonist liraglutide activates cytoprotective pathways and improves outcomes after experimental myocardial infarction in mice. Diabetes 2009, 58, 975–983. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A.; Novials, A.; Ortega, E.; Canivell, S.; La Sala, L.; Pujadas, G.; Esposito, K.; Giugliano, D.; Genovese, S. Glucagon-like peptide 1 reduces endothelial dysfunction, inflammation, and oxidative stress induced by both hyperglycemia and hypoglycemia in type 1 diabetes. Diabetes Care 2013, 36, 2346–2350. [Google Scholar] [CrossRef]
- Erdogdu, O.; Nathanson, D.; Sjoholm, A.; Nystrom, T.; Zhang, Q. Exendin-4 stimulates proliferation of human coronary artery endothelial cells through eNOS-, PKA- and PI3K/Akt-dependent pathways and requires GLP-1 receptor. Mol. Cell Endocrinol. 2010, 325, 26–35. [Google Scholar] [CrossRef]
- Lundgren, J.R.; Faerch, K.; Witte, D.R.; Jonsson, A.E.; Pedersen, O.; Hansen, T.; Lauritzen, T.; Holst, J.J.; Vistisen, D.; Jorgensen, M.E.; et al. Greater glucagon-like peptide-1 responses to oral glucose are associated with lower central and peripheral blood pressures. Cardiovasc. Diabetol. 2019, 18, 130. [Google Scholar] [CrossRef]
- Engelbrechtsen, L.; Lundgren, J.; Wewer Albrechtsen, N.J.; Mahendran, Y.; Iepsen, E.W.; Finocchietto, P.; Jonsson, A.E.; Madsbad, S.; Holst, J.J.; Vestergaard, H.; et al. Treatment with liraglutide may improve markers of CVD reflected by reduced levels of apoB. Obes. Sci. Pract. 2017, 3, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, L.A.; Mankad, S.; Sokos, G.G.; Miske, G.; Shah, A.; Elahi, D.; Shannon, R.P. Effects of glucagon-like peptide-1 in patients with acute myocardial infarction and left ventricular dysfunction after successful reperfusion. Circulation 2004, 109, 962–965. [Google Scholar] [CrossRef] [PubMed]
- Abuannadi, M.; Kosiborod, M.; Riggs, L.; House, J.A.; Hamburg, M.S.; Kennedy, K.F.; Marso, S.P. Management of hyperglycemia with the administration of intravenous exenatide to patients in the cardiac intensive care unit. Endocr. Pract. 2013, 19, 81–90. [Google Scholar] [CrossRef]
- Lonborg, J.; Kelbaek, H.; Vejlstrup, N.; Botker, H.E.; Kim, W.Y.; Holmvang, L.; Jorgensen, E.; Helqvist, S.; Saunamaki, K.; Terkelsen, C.J.; et al. Exenatide reduces final infarct size in patients with ST-segment-elevation myocardial infarction and short-duration of ischemia. Circ. Cardiovasc. Interv. 2012, 5, 288–295. [Google Scholar] [CrossRef]
- Lonborg, J.; Vejlstrup, N.; Kelbaek, H.; Botker, H.E.; Kim, W.Y.; Mathiasen, A.B.; Jorgensen, E.; Helqvist, S.; Saunamaki, K.; Clemmensen, P.; et al. Exenatide reduces reperfusion injury in patients with ST-segment elevation myocardial infarction. Eur. Heart J. 2012, 33, 1491–1499. [Google Scholar] [CrossRef]
- Chen, W.R.; Chen, Y.D.; Tian, F.; Yang, N.; Cheng, L.Q.; Hu, S.Y.; Wang, J.; Yang, J.J.; Wang, S.F.; Gu, X.F. Effects of Liraglutide on Reperfusion Injury in Patients With ST-Segment-Elevation Myocardial Infarction. Circ. Cardiovasc. Imaging 2016, 9, 005146. [Google Scholar] [CrossRef]
- Woo, J.S.; Kim, W.; Ha, S.J.; Kim, J.B.; Kim, S.J.; Kim, W.S.; Seon, H.J.; Kim, K.S. Cardioprotective effects of exenatide in patients with ST-segment-elevation myocardial infarction undergoing primary percutaneous coronary intervention: Results of exenatide myocardial protection in revascularization study. Arter. Thromb. Vasc. Biol. 2013, 33, 2252–2260. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.R.; Shen, X.Q.; Zhang, Y.; Chen, Y.D.; Hu, S.Y.; Qian, G.; Wang, J.; Yang, J.J.; Wang, Z.F.; Tian, F. Effects of liraglutide on left ventricular function in patients with non-ST-segment elevation myocardial infarction. Endocrine 2016, 52, 516–526. [Google Scholar] [CrossRef]
- Thornberry, N.A.; Gallwitz, B. Mechanism of action of inhibitors of dipeptidyl-peptidase-4 (DPP-4). Best Pract. Res. Clin. Endocrinol. Metab. 2009, 23, 479–486. [Google Scholar] [CrossRef]
- Genestreti, P.R.R.; Furtado, R.H.M.; Salsoso, R.; Dalçóquio, T.F.; Franci, A.; Menezes, F.R.; Caporrino, C.; Ferrari, A.G.; Nakashima, C.A.K.; Scanavini Filho, M.A.; et al. Effects of DPP4 Inhibitor in Platelet Reactivity and Other Cardiac Risk Markers in Patients with Type 2 Diabetes and Acute Myocardial Infarction. J. Clin. Med. 2022, 11, 5776. [Google Scholar] [CrossRef] [PubMed]
- Hage, C.; Brismar, K.; Lundman, P.; Mellbin, L.; Ryden, L. The DPP-4 inhibitor sitagliptin and endothelial function in patients with acute coronary syndromes and newly detected glucose perturbations. Diab. Vasc. Dis. Res. 2014, 11, 290–293. [Google Scholar] [CrossRef]
- Kuramitsu, S.; Miyauchi, K.; Yokoi, H.; Suwa, S.; Nishizaki, Y.; Yokoyama, T.; Nojiri, S.; Iwabuchi, M.; Shirai, S.; Ando, K.; et al. Effect of sitagliptin on plaque changes in coronary artery following acute coronary syndrome in diabetic patients: The ESPECIAL-ACS study. J. Cardiol. 2017, 69, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Scirica, B.M.; Bhatt, D.L.; Braunwald, E.; Steg, P.G.; Davidson, J.; Hirshberg, B.; Ohman, P.; Frederich, R.; Wiviott, S.D.; Hoffman, E.B.; et al. SAVOR-TIMI 53 Steering Committee and Investigators Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl. J. Med. 2013, 3, 1317–1326. [Google Scholar] [CrossRef] [PubMed]
- Zannad, F.; Cannon, C.P.; Cushman, W.C.; Bakris, G.L.; Menon, V.; Perez, A.T.; Fleck, P.R.; Mehta, C.R.; Kupfer, S.; Wilson, C.; et al. EXAMINE Investigators Heart failure and mortality outcomes in patients with type 2 diabetes taking alogliptin versus placebo in EXAMINE: A multicentre, randomised, double-blind trial. Lancet 2015, 23, 2067–2076. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical Trial, Year | Ref. | Medication | Study Type | Study Population | Intervention | Main Findings |
|---|---|---|---|---|---|---|
| EXAMINE, 2013 | [83] | Alogliptin | Double-blind, noninferiority randomized trial | Patients with T2DM and AMI or UA requiring hospitalization within previous 15–90 days | Alogliptin or placebo added to existing antidiabetic and CV therapy | Composite primary endpoint of CV death, nonfatal-MI and -stroke was 11.3% in the alogliptin group and 11.8% in the placebo (p < 0.001 in noninferiority) |
| ELIXA, 2015 | [84] | Lixisenatide | Multicenter, double-blind, randomized | Patients with T2DM and AMI or UA within the previous 180 days | Lixisenatide or placebo added to locally determined standard of care | Non-inferiority but also non-superiority of lixisenatide to placebo for the primary endpoint of MI, CV death, stroke, hospitalization for UA; similar rates of SAE |
| EMBODY, 2020 | [85] | Empagliflozin | Prospective, multicenter, double-blind, randomized | Patients with AMI and T2DM | Addition of either EMPA 10 mg or matching placebo | SDANN changes both in the EMPA (p = 0.02) and placebo groups (p = 0.06); LF/HF ratio altered in both EMPA (p = 0.01) and placebo groups (p = 0.43); improvement in HRT only in the EMPA group |
| EMMY, 2022 | [86] | Empagliflozin | Multicenter, double-blind, randomized | Patients with AMI and elevation of CK > 800 IU/L undergoing PCI | Addition of either EMPA 10 mg or matching placebo once daily within 72 h of PCI | Fifteen percent lower levels of NT-proBNP; 1.5% absolute improvement of LVEF; 6.8% greater reduction of mean E/e’; no change in adverse events |
| Zhu et al. 2022 | [87] | Dapagliflozin | Single-center, retrospective | Patients with AMI | Dapagliflozin or not at discharge | The cumulative incidence of MACE (log-rank test, p = 0.009), HF (p = 0.003), nonfatal MI (p = 0.005), and URR (p = 0.031) was higher in the DAPA-free group |
| SGLT2-I AMI PROTECT Registry, 2023 | [88] | SGLT2i | Multicenter international registry | Patients with AMI undergoing PCI between 2018 and 2021 | SGLT2i versus non-SGLT2i users | SGLT2-I users had lower rates of in-hospital CV death, arrhythmic burden, and CI-AKI (all p < 0.05); lower HF hospitalization and CV death during median follow-up of 24 ± 13 months (p < 0.04 for all) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stampouloglou, P.K.; Anastasiou, A.; Bletsa, E.; Lygkoni, S.; Chouzouri, F.; Xenou, M.; Katsarou, O.; Theofilis, P.; Zisimos, K.; Tousoulis, D.; et al. Diabetes Mellitus in Acute Coronary Syndrome. Life 2023, 13, 2226. https://doi.org/10.3390/life13112226
Stampouloglou PK, Anastasiou A, Bletsa E, Lygkoni S, Chouzouri F, Xenou M, Katsarou O, Theofilis P, Zisimos K, Tousoulis D, et al. Diabetes Mellitus in Acute Coronary Syndrome. Life. 2023; 13(11):2226. https://doi.org/10.3390/life13112226
Chicago/Turabian StyleStampouloglou, Panagiota K., Artemis Anastasiou, Evanthia Bletsa, Stavroula Lygkoni, Flora Chouzouri, Maria Xenou, Ourania Katsarou, Panagiotis Theofilis, Konstantinos Zisimos, Dimitris Tousoulis, and et al. 2023. "Diabetes Mellitus in Acute Coronary Syndrome" Life 13, no. 11: 2226. https://doi.org/10.3390/life13112226
APA StyleStampouloglou, P. K., Anastasiou, A., Bletsa, E., Lygkoni, S., Chouzouri, F., Xenou, M., Katsarou, O., Theofilis, P., Zisimos, K., Tousoulis, D., Vavuranakis, M., Siasos, G., & Oikonomou, E. (2023). Diabetes Mellitus in Acute Coronary Syndrome. Life, 13(11), 2226. https://doi.org/10.3390/life13112226