

The Efficacy of Manual Therapy Approaches on Pain, Maximum Mouth Opening and Disability in Temporomandibular Disorders: A Systematic Review of Randomised Controlled Trials

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
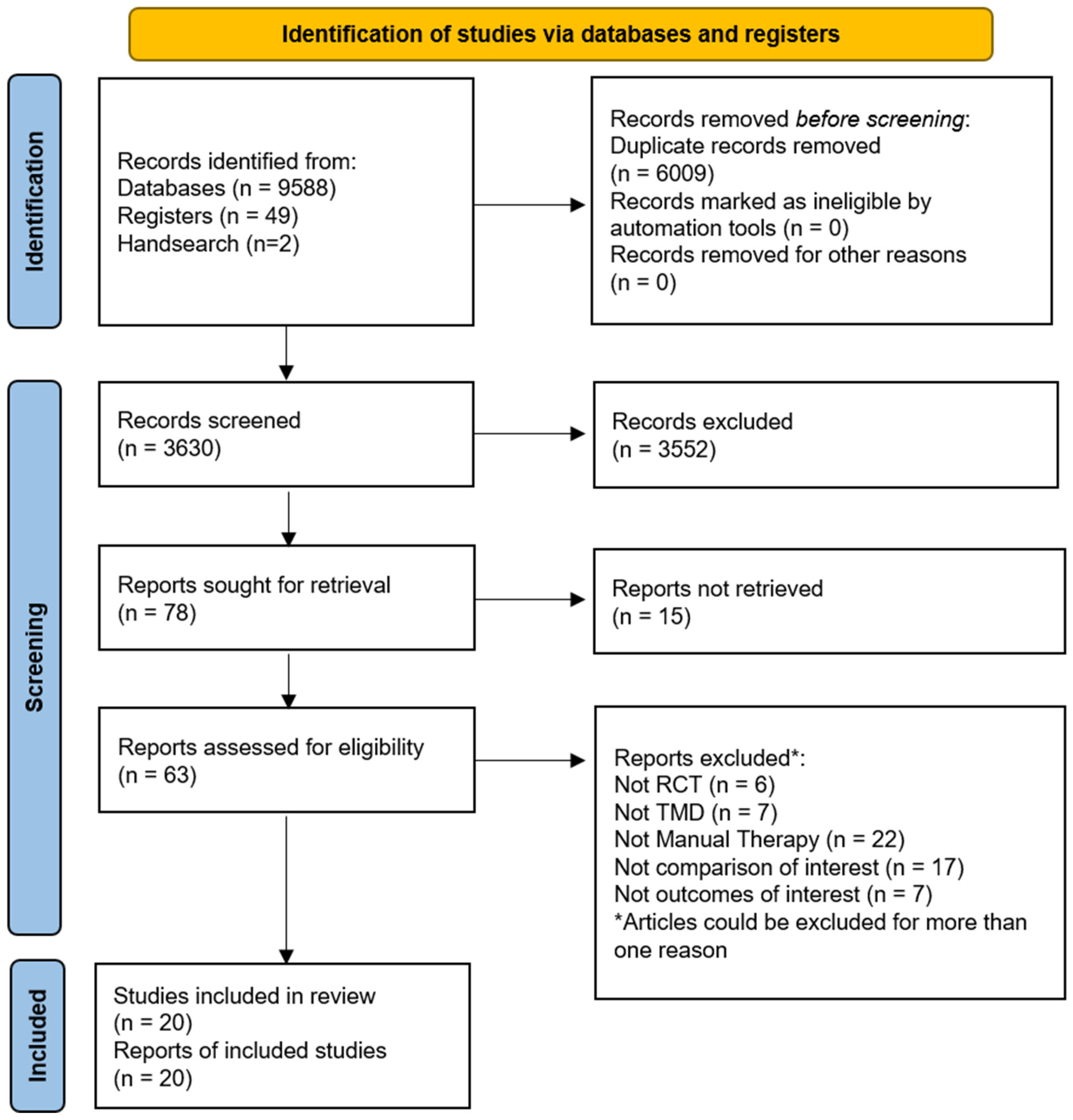
2.2. Search Strategy and Study Selection
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Analysis
3. Results
3.1. Characteristics of Included Trials and Assessment of Risk of Bias
3.2. Effects of Manual Therapy on Pain Intensity in People with Temporomandibular Disorders
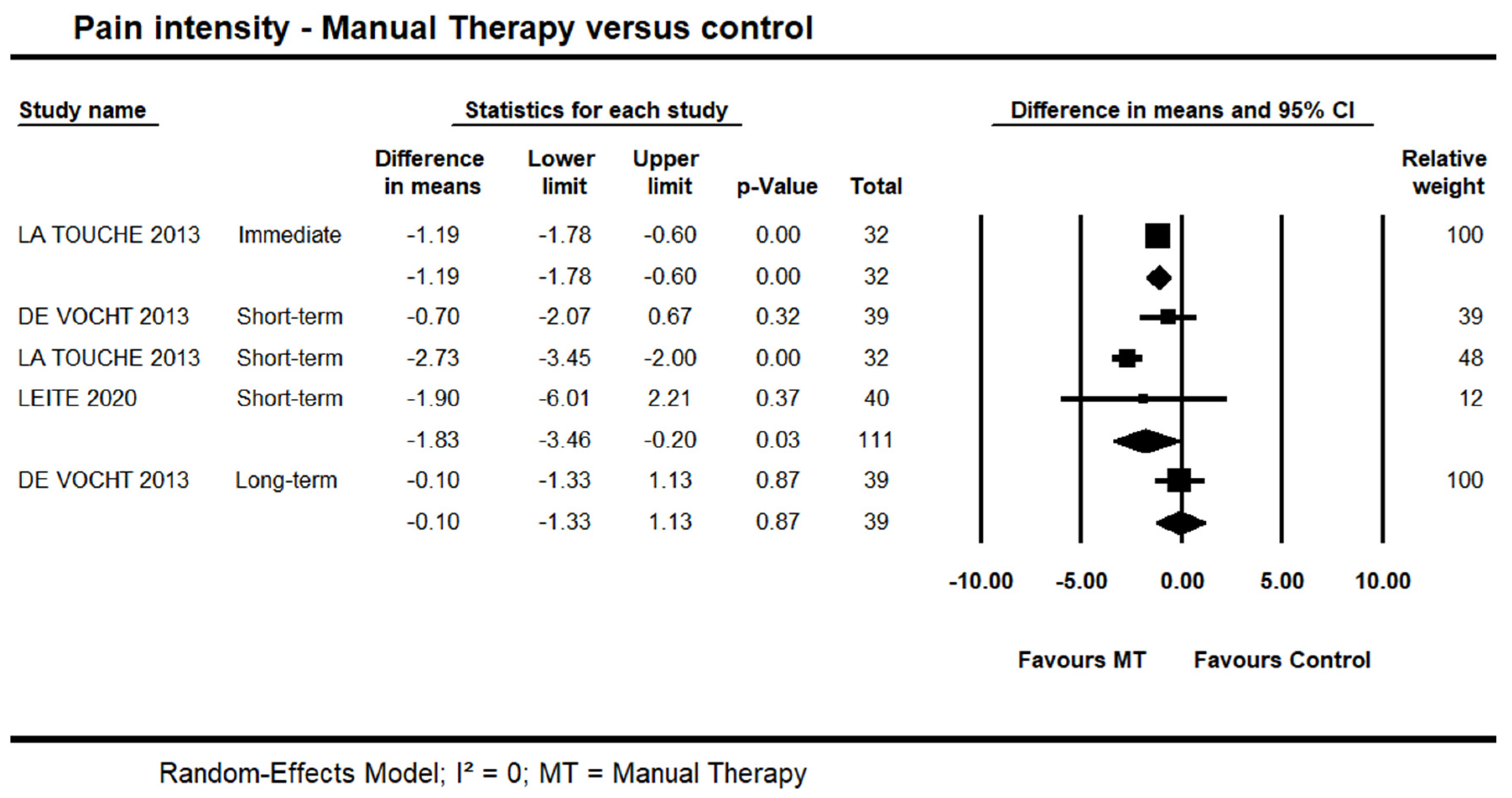
3.2.1. Manual Therapy versus Control on Pain Intensity
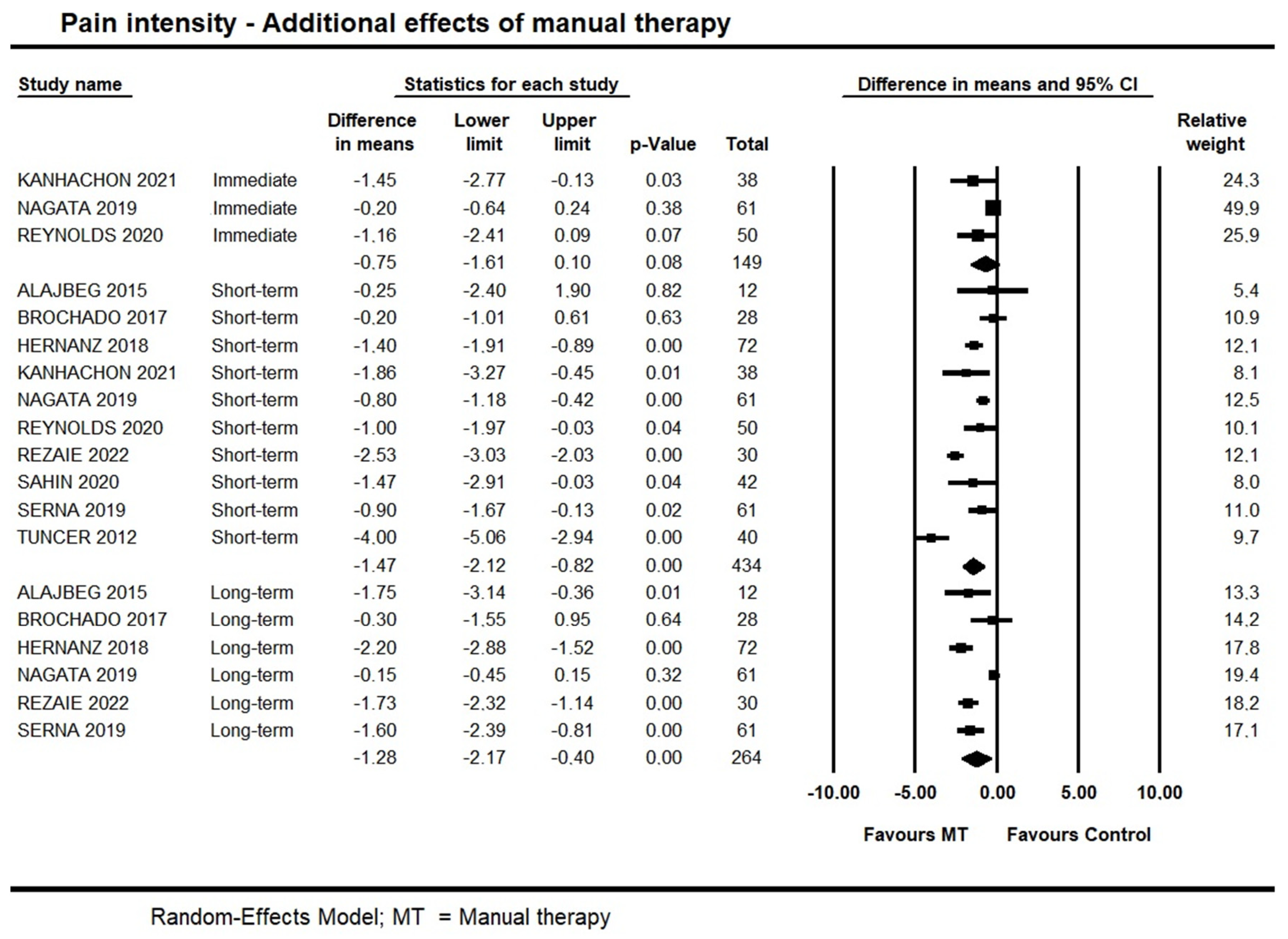
3.2.2. Additional Effects of Manual Therapy on Pain Intensity
3.3. Effects of Manual Therapy on Maximum Mouth Opening in People with Temporomandibular Disorders
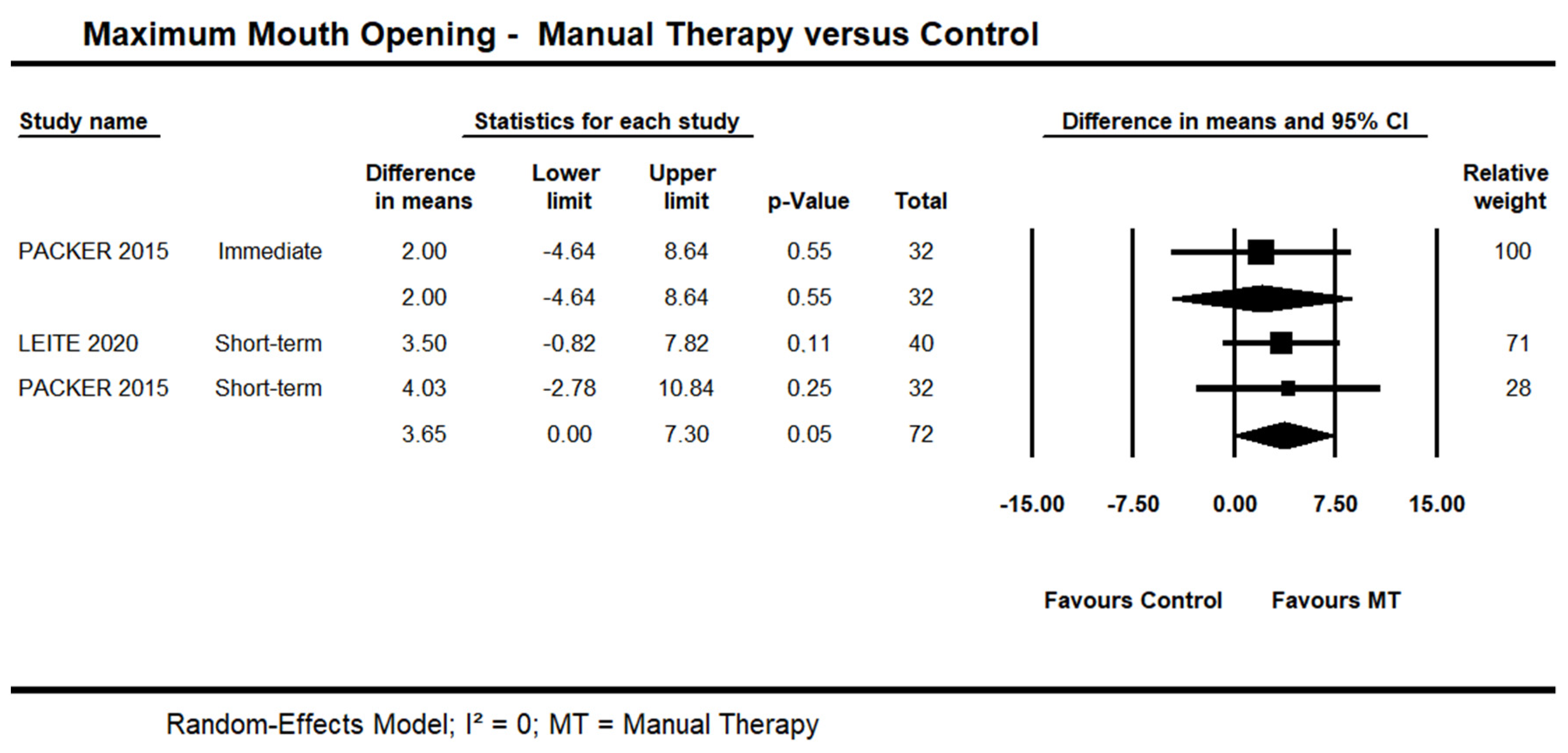
3.3.1. Manual Therapy versus Control on Maximum Mouth Opening
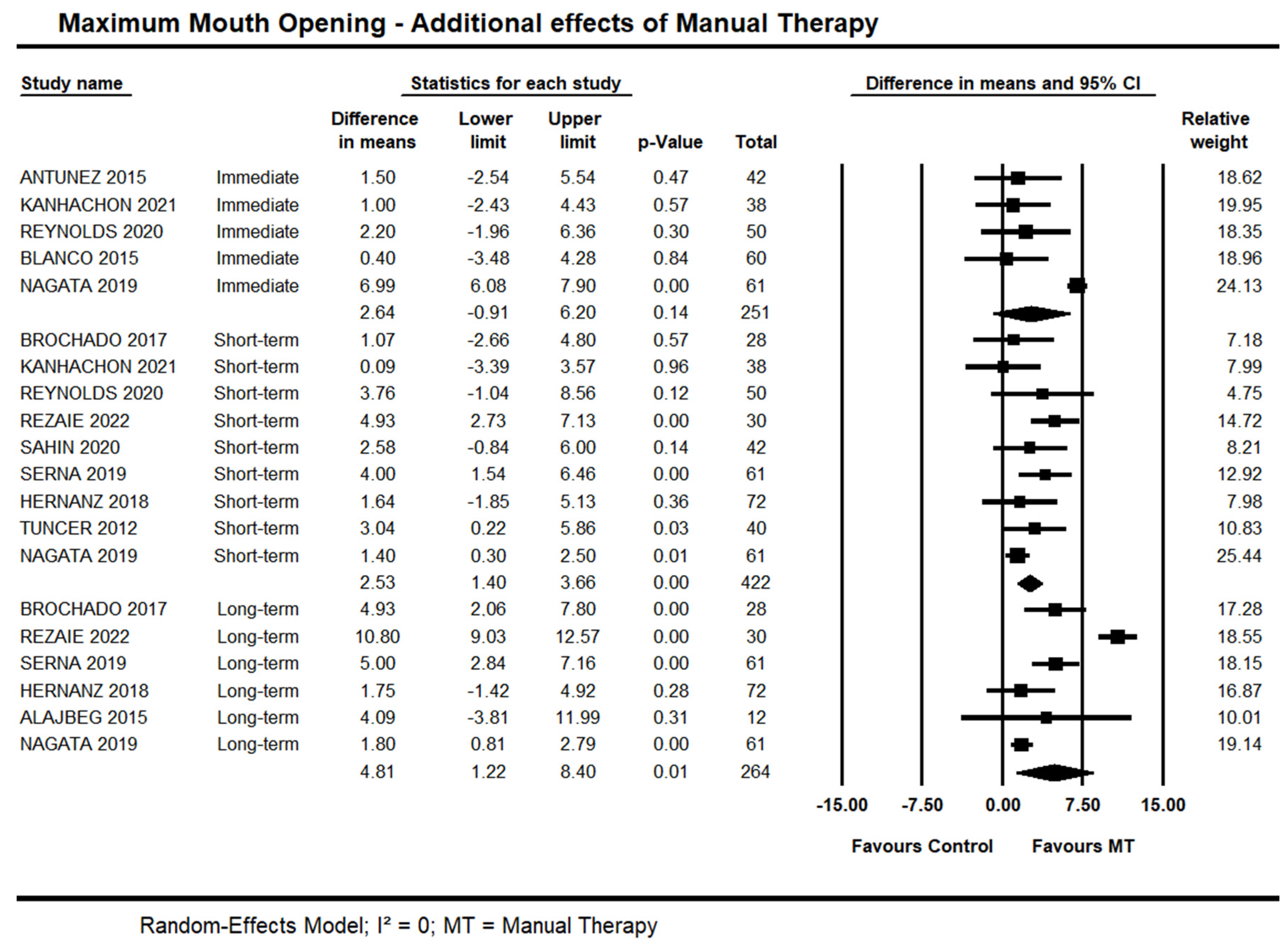
3.3.2. Additional Effects of Manual Therapy on Maximum Mouth Opening
3.4. Effects of Manual Therapy on Disability in People with Temporomandibular Disorders
3.4.1. Manual Therapy versus Control on Disability
3.4.2. Additional Effects of Manual Therapy on Disability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Definition |
| CF-PDI | Craniofacial pain and disability inventory |
| CIs | Confidence intervals |
| DC/TMD | The Diagnostic Criteria for Temporomandibular Disorders |
| FPHI | Fonseca Patient History Index |
| GRADE | Grading of Recommendations Assessment |
| JFLS | Jaw Functional Limitation Scale |
| MCID | Minimal clinical important difference |
| MDC | Minimal Detectable Change |
| MDs | Mean differences |
| MFIQ | Mandibular Function Impairment Questionnaire |
| MFIQ | Migraine Functional Impact Questionnaire |
| MMO | Maximum mouth opening |
| NRS | Numerical Rating Scale |
| PRISMA | Prospective Reporting Items for Systematic Review and Meta-Analyses |
| PROSPERO | Prospective Registry of Systematic Reviews |
| RCTs | Randomised controlled trials |
| SDs | Standard deviations |
| SMDs | Standardized mean differences |
| TMD | Temporomandibular disorders |
| VAS | Visual Analog Scale |
References
- Manfredini, D.; Chiappe, G.; Bosco, M. Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) axis I diagnoses in an Italian patient population. J. Oral Rehabil. 2006, 33, 551–558. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef]
- Minervini, G.; Mariani, P.; Fiorillo, L.; Cervino, G.; Cicciù, M.; Laino, L. Prevalence of temporomandibular disorders in people with multiple sclerosis: A systematic review and meta-analysis. Cranio 2022, 1–9. [Google Scholar] [CrossRef]
- Forssell, H.; Kauko, T.; Kotiranta, U.; Suvinen, T. Predictors for future clinically significant pain in patients with temporomandibular disorder: A prospective cohort study. Eur. J. Pain 2017, 21, 188–197. [Google Scholar] [CrossRef]
- Ohrbach, R.; Dworkin, S.F. Five-year outcomes in TMD: Relationship of changes in pain to changes in physical and psychological variables. Pain 1998, 74, 315–326. [Google Scholar] [CrossRef]
- Velly, A.M.; Elsaraj, S.M.; Botros, J.; Samim, F.; der Khatchadourian, Z.; Gornitsky, M. The contribution of pain and disability on the transition from acute to chronic pain-related TMD: A 3-month prospective cohort study. Front. Pain Res. 2022, 3, 956117. [Google Scholar] [CrossRef]
- Nilsson, I.-M.; List, T. Does adolescent self-reported TMD pain persist into early adulthood? A longitudinal study. Acta Odontol. Scand. 2020, 78, 377–383. [Google Scholar] [CrossRef]
- Barry, F.; Chai, F.; Chijcheapaza-Flores, H.; Garcia-Fernandez, M.J.; Blanchemain, N.; Nicot, R. Systematic review of studies on drug-delivery systems for management of temporomandibular-joint osteoarthritis. J. Stomatol. Oral Maxillofac. Surg. 2021, 123, e336–e341. [Google Scholar] [CrossRef]
- Seo, H.; Jung, B.; Yeo, J.; Kim, K.-W.; Cho, J.-H.; Lee, Y.J.; Ha, I.-H. Healthcare utilisation and costs for temporomandibular disorders: A descriptive, cross-sectional study. BMJ Open 2020, 10, e036768. [Google Scholar] [CrossRef]
- Riley, P.; Glenny, A.-M.; Worthington, H.V.; Jacobsen, E.; Robertson, C.; Durham, J.; Davies, S.; Petersen, H.; Boyers, D. Oral splints for patients with temporomandibular disorders or bruxism: A systematic review and economic evaluation. Health Technol. Assess. 2020, 24, 1–224. [Google Scholar] [CrossRef] [Green Version]
- Prodoehl, J.; Kraus, S.; Stein, A.B. Predicting the number of physical therapy visits and patient satisfaction in individuals with temporomandibular disorder: A cohort study. J. Oral Rehabil. 2022, 49, 22–36. [Google Scholar] [CrossRef]
- Kothari, K.; Jayakumar, N.; Razzaque, A. Multidisciplinary management of temporomandibular joint ankylosis in an adult: Journey from arthroplasty to oral rehabilitation. BMJ Case Rep. 2021, 14, e245120. [Google Scholar] [CrossRef]
- Penlington, C.; Bowes, C.; Taylor, G.; Otemade, A.A.; Waterhouse, P.; Durham, J.; Ohrbach, R. Psychological therapies for temporomandibular disorders (TMDs). Cochrane Database Syst. Rev. 2022, 2022, CD013515. [Google Scholar] [CrossRef]
- de Souza, R.F.; da Silva, C.H.L.; Nasser, M.; Fedorowicz, Z.; A Al-Muharraqi, M. Interventions for managing temporomandibular joint osteoarthritis. Cochrane Database Syst. Rev. 2012, 2018, CD007261. [Google Scholar] [CrossRef]
- Mujakperuo, H.R.; Watson, M.; Morrison, R.; Macfarlane, T.V. Pharmacological interventions for pain in patients with temporomandibular disorders. Cochrane Database Syst. Rev. 2010, 10, CD004715. [Google Scholar] [CrossRef]
- Ferrillo, M.; Nucci, L.; Giudice, A.; Calafiore, D.; Marotta, N.; Minervini, G.; D’Apuzzo, F.; Ammendolia, A.; Perillo, L.; de Sire, A. Efficacy of conservative approaches on pain relief in patients with temporomandibular joint disorders: A systematic review with network meta-analysis. Cranio 2022, 1–17. [Google Scholar] [CrossRef]
- Minervini, G.; Fiorillo, L.; Russo, D.; Lanza, A.; D’Amico, C.; Cervino, G.; Meto, A.; Di Francesco, F. Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature. Prosthesis 2022, 4, 253–262. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Pitance, L.; Singh, V.; Neto, F.; Thie, N.; Michelotti, A. Effectiveness of Manual Therapy and Therapeutic Exercise for Temporomandibular Disorders: Systematic Review and Meta-Analysis. Phys. Ther. 2016, 96, 9–25. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Schuenemann, H.J.; Tugwell, P.; Knottnerus, A. GRADE guidelines: A new series of articles in the Journal of Clinical Epidemiology. J. Clin. Epidemiol. 2011, 64, 380–382. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions. 2021. Available online: https://training.cochrane.org/cochrane-handbook-systematic-reviews-interventions (accessed on 7 December 2020).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Katz, J.; Melzack, R. Measurement of Pain. Surg. Clin. North Am. 1999, 79, 231–252. [Google Scholar] [CrossRef]
- Wood, G.D.; A Branco, J. A comparison of three methods of measuring maximal opening of the mouth. J. Oral Surg. (Am. Dent. Assoc. 1965) 1979, 37, 175–177. [Google Scholar]
- Ohrbach, R.; Larsson, P.; List, T. The jaw functional limitation scale: Development, reliability, and validity of 8-item and 20-item versions. J. Orofac. Pain 2008, 22, 219–230. [Google Scholar]
- Stegenga, B.; De Bont, L.G.; De Leeuw, R.; Boering, G. Assessment of mandibular function impairment associated with temporomandibular joint osteoarthrosis and internal derangement. J. Orofac. Pain 1993, 7, 183–195. [Google Scholar]
- Macedo, L.G.; Elkins, M.R.; Maher, C.G.; Moseley, A.M.; Herbert, R.D.; Sherrington, C. There was evidence of convergent and construct validity of Physiotherapy Evidence Database quality scale for physiotherapy trials. J. Clin. Epidemiol. 2010, 63, 920–925. [Google Scholar] [CrossRef]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Kropmans, T.; Dijkstra, P.; Stegenga, B.; Stewart, R.; De Bont, L. Smallest detectable difference in outcome variables related to painful restriction of the temporomandibular joint. J. Dent. Res. 1999, 78, 784–789. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Mueller, P.S.; Montori, V.; Bassler, D.; Koenig, B.A.; Guyatt, G.H. Ethical Issues in Stopping Randomized Trials Early Because of Apparent Benefit. Ann. Intern. Med. 2007, 146, 878–881. [Google Scholar] [CrossRef]
- Foley, N.C.; Teasell, R.W.; Bhogal, S.K.; Speechley, M.R. Stroke Rehabilitation Evidence-Based Review: Methodology. Top. Stroke Rehabil. 2003, 10, 1–7. [Google Scholar] [CrossRef]
- Ioannidis, J.P.; Trikalinos, T.A. The appropriateness of asymmetry tests for publication bias in meta-analyses: A large survey. Can. Med. Assoc. J. 2007, 176, 1091–1096. [Google Scholar] [CrossRef]
- Alajbeg, I.; Gikić, M.; Peruzović, M.V. Mandibular Range of Movement and Pain Intensity in Patients with Anterior Disc Displacement without Reduction. Acta Stomatol. Croat. 2015, 49, 119–127. [Google Scholar] [CrossRef]
- Espejo-Antúnez, L.; Castro-Valenzuela, E.; Ribeiro, F.; Albornoz-Cabello, M.; Silva, A.; Rodríguez-Mansilla, J. Immediate effects of hamstring stretching alone or combined with ischemic compression of the masseter muscle on hamstrings extensibility, active mouth opening and pain in athletes with temporomandibular dysfunction. J. Bodyw. Mov. Ther. 2016, 20, 579–587. [Google Scholar] [CrossRef]
- Rodriguez-Blanco, C.; Cocera-Morata, F.M.; Heredia-Rizo, A.M.; Ricard, F.; Almazán-Campos, G.; Oliva-Pascual-Vaca, Á. Immediate Effects of Combining Local Techniques in the Craniomandibular Area and Hamstring Muscle Stretching in Subjects with Temporomandibular Disorders: A Randomized Controlled Study. J. Altern. Complement. Med. 2015, 21, 451–459. [Google Scholar] [CrossRef]
- Brochado, F.T.; De Jesus, L.H.; Carrard, V.C.; Freddo, A.L.; Chaves, K.D.; Martins, M.D. Comparative effectiveness of photobiomodulation and manual therapy alone or combined in TMD patients: A randomized clinical trial. Braz. Oral Res. 2018, 32, e50. [Google Scholar] [CrossRef] [Green Version]
- DeVocht, J.W.; Goertz, C.M.; Hondras, M.A.; Long, C.R.; Schaeffer, W.; Thomann, L.; Spector, M.; Stanford, C.M. A pilot study of a chiropractic intervention for management of chronic myofascial temporomandibular disorder. J. Am. Dent. Assoc. 2013, 144, 1154–1163. [Google Scholar] [CrossRef] [Green Version]
- Gomes, C.A.F.D.P.; El Hage, Y.; Amaral, A.P.; Politti, F.; Biasotto-Gonzalez, D.A. Effects of massage therapy and occlusal splint therapy on electromyographic activity and the intensity of signs and symptoms in individuals with temporomandibular disorder and sleep bruxism: A randomized clinical trial. Chiropr. Man. Ther. 2014, 22, 43. [Google Scholar] [CrossRef] [Green Version]
- Hernanz, G.S.; Angulo-Carrere, T.; Ardizone-García, I.; Svensson, P.; Álvarez-Méndez, A.M. Pressure Release Technique Versus Placebo Applied to Cervical and Masticatory Muscles in Patients with Chronic Painful Myofascial Temporomandibular Disorder. A Randomized Clinical Trial 2020, PREPRINT (Version 1) available at Research Square. Available online: https://www.researchsquare.com/article/rs-51085/v1 (accessed on 7 December 2020).
- Kalamir, A.; Bonello, R.; Graham, P.; Vitiello, A.L.; Pollard, H. Intraoral Myofascial Therapy for Chronic Myogenous Temporomandibular Disorder: A Randomized Controlled Trial. J. Manip. Physiol. Ther. 2012, 35, 26–37. [Google Scholar] [CrossRef]
- Kanhachon, W.; Boonprakob, Y. Modified-Active Release Therapy in Patients with Scapulocostal Syndrome and Masticatory Myofascial Pain: A Stratified-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 8533. [Google Scholar] [CrossRef]
- La Touche, R.; Paris-Alemany, A.; Mannheimer, J.S.; Angulo-Díaz-Parreño, S.; Bishop, M.; Centeno, A.L.-V.; von Piekartz, H.; Fernandez-Carnero, J. Does Mobilization of the Upper Cervical Spine Affect Pain Sensitivity and Autonomic Nervous System Function in Patients With Cervico-craniofacial Pain? Clin. J. Pain 2013, 29, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Leite, W.B.; Oliveira, M.L.; Ferreira, I.C.; Anjos, C.F.; Barbosa, M.A.; Barbosa, A.C. Effects of 4-Week Diacutaneous Fibrolysis on Myalgia, Mouth Opening, and Level of Functional Severity in Women With Temporomandibular Disorders: A Randomized Controlled Trial. J. Manip. Physiol. Ther. 2020, 43, 806–815. [Google Scholar] [CrossRef]
- Lucas, C.; Branco, I.; Silva, M.; Alves, P.; Pereira, Â.M. Benefits of manual therapy in temporomandibular joint dysfunction treatment. In 2nd International Congress of CiiEM-Translational Research and Innovation in Human and Health Science; Campus Egas Moniz: Monte de Caparica, Portugal, 2017. [Google Scholar]
- Nagata, K.; Hori, S.; Mizuhashi, R.; Yokoe, T.; Atsumi, Y.; Nagai, W.; Goto, M. Efficacy of mandibular manipulation technique for temporomandibular disorders patients with mouth opening limitation: A randomized controlled trial for comparison with improved multimodal therapy. J. Prosthodont. Res. 2019, 63, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Packer, A.C.; Pires, P.F.; Dibai-Filho, A.V.; Rodrigues-Bigaton, D. Effect of Upper Thoracic Manipulation on Mouth Opening and Electromyographic Activity of Masticatory Muscles in Women With Temporomandibular Disorder: A Randomized Clinical Trial. J. Manip. Physiol. Ther. 2015, 38, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Puentedura, E.J.; Kolber, M.J.; Cleland, J.A. Effectiveness of Cervical Spine High-Velocity, Low-Amplitude Thrust Added to Behavioral Education, Soft Tissue Mobilization, and Exercise for People With Temporomandibular Disorder With Myalgia: A Randomized Clinical Trial. J. Orthop. Sport. Phys. Ther. 2020, 50, 455–465. [Google Scholar] [CrossRef]
- Rezaie, K.; Amiri, A.; Takamjani, E.E.; Shirani, G.; Salehi, S.; Alizadeh, L. The Efficacy of Neck and Temporomandibular Joint (TMJ) Manual Therapy in Comparison With a Multimodal Approach in the Patients with TMJ Dysfunction: A Blinded Randomized Controlled Trial. Med. J. Islam. Repub. Iran 2022, 36, 328–337. [Google Scholar] [CrossRef]
- Şahin, D.; Mutlu, E.K.; Şakar, O.; Ateş, G.; Inan, Ş.; Taşkıran, H. The effect of the ischaemic compression technique on pain and functionality in temporomandibular disorders: A randomised clinical trial. J. Oral Rehabil. 2021, 48, 531–541. [Google Scholar] [CrossRef]
- de la Serna, P.D.; Plaza-Manzano, G.; Cleland, J.; Fernández-De-Las-Peñas, C.; Martín-Casas, P.; Díaz-Arribas, M.J. Effects of Cervico-Mandibular Manual Therapy in Patients with Temporomandibular Pain Disorders and Associated Somatic Tinnitus: A Randomized Clinical Trial. Pain Med. 2020, 21, 613–624. [Google Scholar] [CrossRef]
- Tuncer, A.; Ergun, N.; Tuncer, A.H.; Karahan, S. Effectiveness of manual therapy and home physical therapy in patients with temporomandibular disorders: A randomized controlled trial. J. Bodyw. Mov. Ther. 2013, 17, 302–308. [Google Scholar] [CrossRef]
- Yoshida, H.; Fukumura, Y.; Suzuki, S.; Fujita, S.; Kenzo, O.; Yoshikado, R.; Nakagawa, M.; Inoue, A.; Sako, J.; Yamada, K.; et al. Simple manipulation therapy for temporomandibular joint internal derangement with closed lock. J. Oral. Maxillofac. Surg. 2005, 17, 256–260. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Conti, P.C.R.; Alyahya, A.; Alkebsi, K.; Elsharkawy, A.; Christidis, N. The hierarchy of different treatments for myogenous temporomandibular disorders: A systematic review and network meta-analysis of randomized clinical trials. Oral Maxillofac. Surg. 2022, 26, 519–533. [Google Scholar] [CrossRef] [PubMed]
- Dinsdale, A.; Costin, B.; Dharamdasani, S.; Page, R.; Purs, N.; Treleaven, J. What conservative interventions improve bite function in those with temporomandibular disorders? A systematic review using self-reported and physical measures. J. Oral Rehabil. 2022, 49, 456–475. [Google Scholar] [CrossRef] [PubMed]
- Asquini, G.; Pitance, L.; Michelotti, A.; Falla, D. Effectiveness of manual therapy applied to craniomandibular structures in temporomandibular disorders: A systematic review. J. Oral Rehabil. 2022, 49, 442–455. [Google Scholar] [CrossRef]
- Calixtre, L.B.; Moreira, R.F.C.; Franchini, G.H.; Alburquerque-Sendín, F.; Oliveira, A.B. Manual therapy for the management of pain and limited range of motion in subjects with signs and symptoms of temporomandibular disorder: A systematic review of randomised controlled trials. J. Oral Rehabil. 2015, 42, 847–861. [Google Scholar] [CrossRef]
- Ferrillo, M.; Ammendolia, A.; Paduano, S.; Calafiore, D.; Marotta, N.; Migliario, M.; Fortunato, L.; Giudice, A.; Michelotti, A.; de Sire, A. Efficacy of rehabilitation on reducing pain in muscle-related temporomandibular disorders: A systematic review and meta-analysis of randomized controlled trials. J. Back Musculoskelet. Rehabil. 2022, 35, 921–936. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Local | Participants | Intervention | Outcome Time-Points |
|---|---|---|---|---|
| Alajbeg et al., 2015 [35] | Croatia | 12 participants (M = 3; F = 9), mean age of 30.5 ± 14 y/o, with TMJ disc displacement based on DC/TMD and MRI. | EG = Joint mobilization + Massage + Stabilization occlusal splint CG = Stabilization occlusal splint | Pain intensity (0–100 VAS); MMO Short and long-term. |
| Antunez et al., 2015 [36] | Spain | 42 participants (M = 14; F = 28), mean age of 21.2 ± 1.6 y/o; TMD (myofascial pain) based on DC/TMD, for ≥6 months. | EG = Ischemic compression technique on the masseter muscle + stretching of hamstrings CG = PNF stretching of hamstrings | Pain intensity (0–10 VAS); MMO (Caliper); Immediate effects |
| Blanco et al., 2015 [37] | Spain | 60 participants (M = 19; F = 41), mean age 35.2 ± 12 y/o, with TMD (myofascial pain) for ≥6 months based on DC/TMD; restricted cervical mobility. | EG = Suboccipital muscle inhibition + Pressure release massage + stretching. CG = Pressure release massage + stretching | MMO (Caliper); Immediate effects |
| Brochado et al., 2017 [38] | Brazil | 28 participants (M = 1; F = 27), mean age 44.5 ± 17 y/o, with TMD (myogenic and arthrogenic) based on DC/TMD. | EG = Pressure Release Massage + Joint Mobilization + Photobiomodulation. CG = Photobiomodulation | Pain intensity (0–10 VAS) Short and long-term. |
| Devocht et al., 2013 [39] | USA | 39 amateur athletes (M = 8; F = 31), mean age of 33 y/o, with TMD (myofascial pain) based on DC/TMD, for at ≥6 months. | EG = Mechanically assisted manipulation (hand-held spring-loaded instrument)—12 sessions for 2 months. CG = Sham Device | Pain intensity (0–10 NRS) Short and Long-term |
| Gomes et al., 2014 [40] | Brazil | 30 participants (M = 4; F = 26), mean age of 27 ± 1.6 y/o, with severe TMD and bruxism. | EG = Massage + Occlusal splint—3 times week, for 4 weeks. CG = Occlusal splint | Oral Disability (0–100 FPHI) Short-term |
| Hernanz et al., 2018 [41] | Spain | 72 participants (M = 12; F = 60), mean age 42 y/o, with TMD (myofascial pain) based on DC/TMD for ≥6 months. | EG = Pressure Release Technique + Occlusal splint + education CG = Sham + Occlusal splint and education | Pain intensity (0–10 VAS). MMO Short and long-term |
| Kalamir et al., 2011 [42] | Australia | 60 participants (M = 26; F = 34), age between 18–50 y/o, with TMD based on DC/TMD for ≥3 months. | EG = Intraoral manual pressure—2 times week for 5 weeks CG = Waitlist | Pain intensity (0–10 NRS); MMO (caliper); Short and Long-term |
| Kanhachon et al., 2021 [43] | Thailand | 38 academics (M = 4; F = 34), mean age of 25 ± 5 y/o, with pain on the neck, scapular, and jaw for more than 3 months, with a referral pattern. | EG = Active Stretching Release Therapy + hot pack on jaw and scapular areas + education CG = Hot pack on jaw and scapular areas + education | Pain intensity (0–10 VAS); MMO (therabite device)® Immediate, short-term |
| La Touche et al., 2013 [44] | Spain | 32 patients (M = 11; F = 21), mean age 34 y/o, with TMD (myofascial pain)—DC/TMD. | EG = Upper cervical mobilization—3 sessions over 2 weeks. CG = Sham | Pain intensity (0–100 VAS) Immediate, short-term |
| Leite et al., 2020 [45] | Brazil | 48 women, age between 18–45 y/o, with TMD (pain dysfunction) based on DC/TMD, for ≥6 months. | EG = Diacutaneous Fibrolysis—2 sessions week for 4 weeks CG = Sham | Pain intensity (0–100 VAS); MMO (Calliper); Disability (0–68 MFIQ) Short-term |
| Lucas et al., 2017 [46] | Portugal | 20 participants with pain on masticatory muscles and/or TMJ according to DC/TMD. | EG = Manual Therapy + Therapeutic Exercises—2 sessions week for 6 weeks CG = Therapeutic Exercises | Pain intensity (0–10 NRS); MMO Immediate effects |
| Nagata et al., 2019 [47] | Japan | 61 participants (M = 11; F = 50), mean age of 49.6 ± 25 y/o, with TMD based on DC/TMD and MRI. | EG = Joint manipulation + self-exercise + CBT + education. CG = Self-exercise + CBT + education. | Pain intensity (0–10 NRS). MMO (caliper). Immediate, short and long-term |
| Packer et al., 2015 [48] | Brazil | 32 women, mean age 24 ± 5 y/o, with TMD based on DC/TMD | EG = Upper thoracic manipulation CG = Sham | MMO (caliper). Immediate, short-term |
| Reynolds et al., 2020 [49] | USA | 50 participants (M = 7; F = 43), mean age of 24.78 ± 5.4 y/o, with TMD according to DC/TMD. | EG = Cervical HVLAT + suboccipital release + education + home exercises CG = Sham HVLAT + suboccipital release + education + home exercises | Pain intensity (0–10 NRS); MMO (ROM scale). Disability (0–20 JFLS) Immediate, short-term |
| Rezaie et al., 2022 [50] | Iran | 30 participants (M = 13; F = 17), mean age of 28 y/o, with TMD according to DC/TMD, for ≥3 months. | EG = Joint and soft-tissue mobilization on TMJ and cervical spine + Massage + UST + TENS CG: Massage + UST + TENS | Pain intensity (0–10 NRS); MMO (Calliper); Short and long-term |
| Sahin et al., 2020 [51] | Turkey | 42 participants (M = 10; F = 32), mean age of 26.2 y/o, with TMD according to DC/TMD and trigger-point in the masseter muscle. | EG = Ischemic compression technique + Postural and Rocabado’s 6 × 6 exercises. CG =Postural and Rocabado’s 6 × 6 exercises | Pain intensity (0–10 VAS). MMO (Ruler). Disability (JFLS-8) Short-term |
| Serna et al., 2019 [52] | Spain | 61 participants (M = 25; F = 36), age between 18 and 65 y/o, with tinnitus symptoms and TMD according to DC/TMD. | EG = Multimodal Manual therapy + Cervical and TMJ exercises + Self-massage + education—for 5 weeks CG = Cervical and TMJ exercises + Self-massage + education | Pain intensity (0–10 NRS); MMO (Adapted-Ruler); Disability (0–63 CF-PDI) Short and long-term |
| Tuncer et al., 2012 [53] | Turkey | 40 participants (M = 9; F = 31), age between 18–72 y/o, with TMD and disc displacement based on DC/TMD for ≥3 months. | EG = Soft tissue and joint mobilization + TMJ exercises and stretching + Education CG = TMJ exercises and stretching + Education | Pain intensity (0–100 VAS); MMO (Ruler) Short-term |
| Yoshida et al., 2005 [54] | Japan | 305 participants (M = 76; F = 229), age between 18–74 y/o, with TMJ disc displacement. | EG = Jaw joint manipulation + NSAIDs CG = NSAIDs | MMO Immediate effects |
| Study | A | B | C | D | E | F | G | H | I | J | Score (0–10) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alajbeg et al., 2015 [35] | Y | N | Y | N | N | Y | Y | Y | N | Y | 6 |
| Antunez et al., 2015 [36] | Y | N | Y | N | N | Y | Y | Y | N | Y | 6 |
| Blanco et al., 2015 [37] | Y | N | Y | Y | N | Y | Y | Y | Y | Y | 8 |
| Brochado et al., 2017 [38] | Y | N | Y | N | N | Y | N | Y | Y | Y | 6 |
| Devocht et al., 2013 [39] | Y | Y | Y | N | N | N | N | Y | Y | Y | 6 |
| Gomes et al., 2014 [40] | Y | Y | N | N | N | Y | Y | Y | Y | Y | 7 |
| Hernanz et al., 2018 [41] | Y | Y | Y | Y | N | N | Y | N | Y | Y | 7 |
| Kalamir et al., 2011 [42] | Y | Y | Y | N | N | Y | Y | Y | Y | N | 7 |
| Kanhachon et al., 2021 [43] | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8 |
| La Touche et al., 2013 [44] | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | 9 |
| Leite et al., 2020 [45] | Y | N | Y | Y | N | Y | Y | Y | Y | Y | 8 |
| Lucas et al., 2017 [46] | Y | N | N | N | N | N | Y | N | N | N | 2 |
| Nagata et al., 2019 [47] | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 |
| Packer et al., 2015 [48] | Y | Y | Y | N | N | Y | Y | Y | N | Y | 7 |
| Reynolds et al., 2020 [49] | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | 9 |
| Rezaie et al., 2022 [50] | Y | Y | Y | Y | N | Y | N | N | Y | Y | 7 |
| Sahin et al., 2020 [51] | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 |
| Serna et al., 2019 [52] | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8 |
| Tuncer et al., 2012 [53] | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8 |
| Yoshida et al., 2005 [54] | Y | N | N | N | N | N | N | N | N | N | 1 |
| Population: People with Temporomandibular Disorder. Intervention: Manual Pressure Release techniques (6 trials); Joint manipulation (4 trials); Joint mobilization (1 trial); Soft-tissue mobilization (1 trial); Stretching (1 trial); Instrumental-assisted techniques (2 trials); Massage (1 trial); MTs in combination (5 trials); Not specified (1 trial). Comparison: No intervention (13 trials), sham (6 trials), wait-list (1 trial). Outcome: Pain intensity (15 trials); MMO (15 trials); Disability (5 trials). Setting: Spain (5 trials); Brazil (4 trials); Japan (2 trials); USA (2 trials); Turkey (2 trials); Australia (1 trial); Iran (1 trial); Portugal (1 trial); Thailand (1 trial); Croatia (1 trial). | ||||
| Outcome Time-Point | MD or SMD (CI 95%) | Sample Size (No. of Studies) | GRADE Assessment | Comments |
| MT vs. Control 0–10 Pain intensity Immediate-effects | −0.88 (−1.57 to −0.19) | 32 (1 study) | ⨁⨁⊝⊝ LOW a,b | The difference is statistically significant but not clinically important based on a MCID = 2. |
| MT add effects 0–10 Pain intensity Immediate-effects | −0.75 (−1.61 to 0.10) | 149 (3 studies) | ⨁⨁⨁⊝ MODERATE a | The difference is not statistically significant. |
| MT vs. Control 0–10 Pain intensity Short-term | −1.83 (−3.46 to −0.20) | 111 (3 studies) | ⨁⨁⊝⊝ LOW a,c | The difference is statistically significant but may not be clinically important based on a MCID = 2. |
| MT add effects 0–10 Pain intensity Short-term | −1.47 (−2.12 to −0.82) | 434 (10 studies) | ⨁⨁⨁⨁ HIGH | The difference is statistically significant but may not be clinically important based on a MCID = 2. |
| MT vs. Control 0–10 Pain intensity Long-term | −0.10 (−1.33 to 1.13) | 39 (1 study) | ⨁⊝⊝⊝ VERY LOW a,b,c | The difference is not statistically significant. |
| MT add effects 0–10 Pain intensity Long-term | −1.28 (−2.17 to −0.40) | 342 (6 studies) | ⨁⨁⨁⊝ MODERATE a | The difference is statistically significant but may not be clinically important based on a MCID = 2. |
| Joint Manipulation 0–10 Pain intensity Short-term | −0.83 (−1.18 to −0.47) | 111 (2 studies) | ⨁⨁⨁⊝ MODERATE a | Subgroup analysis—MT modalities The difference is statistically significant but not clinically important based on a MCID = 2. |
| Manual Pressure 0–10 Pain intensity Short-term | −1.41 (−1.89 to −0.93) | 114 (2 studies) | ⨁⨁⨁⊝ MODERATE a | Subgroup analysis—MT modalities The difference is statistically significant but not clinically important based on a MCID of 2 points. |
| Multimodal 0–10 Pain intensity Short-term | −1.65 (−2.98 to −0.32) | 171 (5 studies) | ⨁⨁⨁⊝ MODERATE a | Subgroup analysis—MT modalities The difference is statistically significant but may not be clinically important based on a MCID = 2. |
| Stretching 0–10 Pain intensity Short-term | −1.86 (−3.27 to −0.45) | 3 8(1 study) | ⨁⨁⊝⊝ LOW a,b | Subgroup analysis—MT modalities The difference is statistically significant but may not be clinically important based on a MCID = 2. |
| MT vs. Control MMO—mm Immediate-effects | 2.0 (−4.64 to 8.64) | 32 (1 study) | ⨁⨁⊝⊝ LOW a,b | The difference is not statistically significant. |
| MT add effects MMO—mm Immediate-effects | 2.64 (−0.91 to 6.20) | 251 (5 studies) | ⨁⨁⨁⊝ MODERATE a | The difference is not statistically significant. |
| MT vs. Control MMO—mm Short-term | 3.65 (0.00 to 7.30) | 72 (2 studies) | ⨁⨁⨁⊝ MODERATE a | The difference is statistically significant but may be not clinically important based on a MDC of 5 mm |
| MT add effects MMO—mm Short-term | 2.5 8(1.58 to 3.58) | 494 (9 studies) | ⨁⨁⨁⨁ HIGH | The difference is statistically significant but not clinically important based on a MDC of 5 mm |
| MT add effects MMO—mm Long-term | 4.81 (1.22 to 8.40) | 264 (6 study) | ⨁⨁⨁⊝ MODERATE a | The difference is statistically significant but may not be clinically important based on a MDC = 5 mm. |
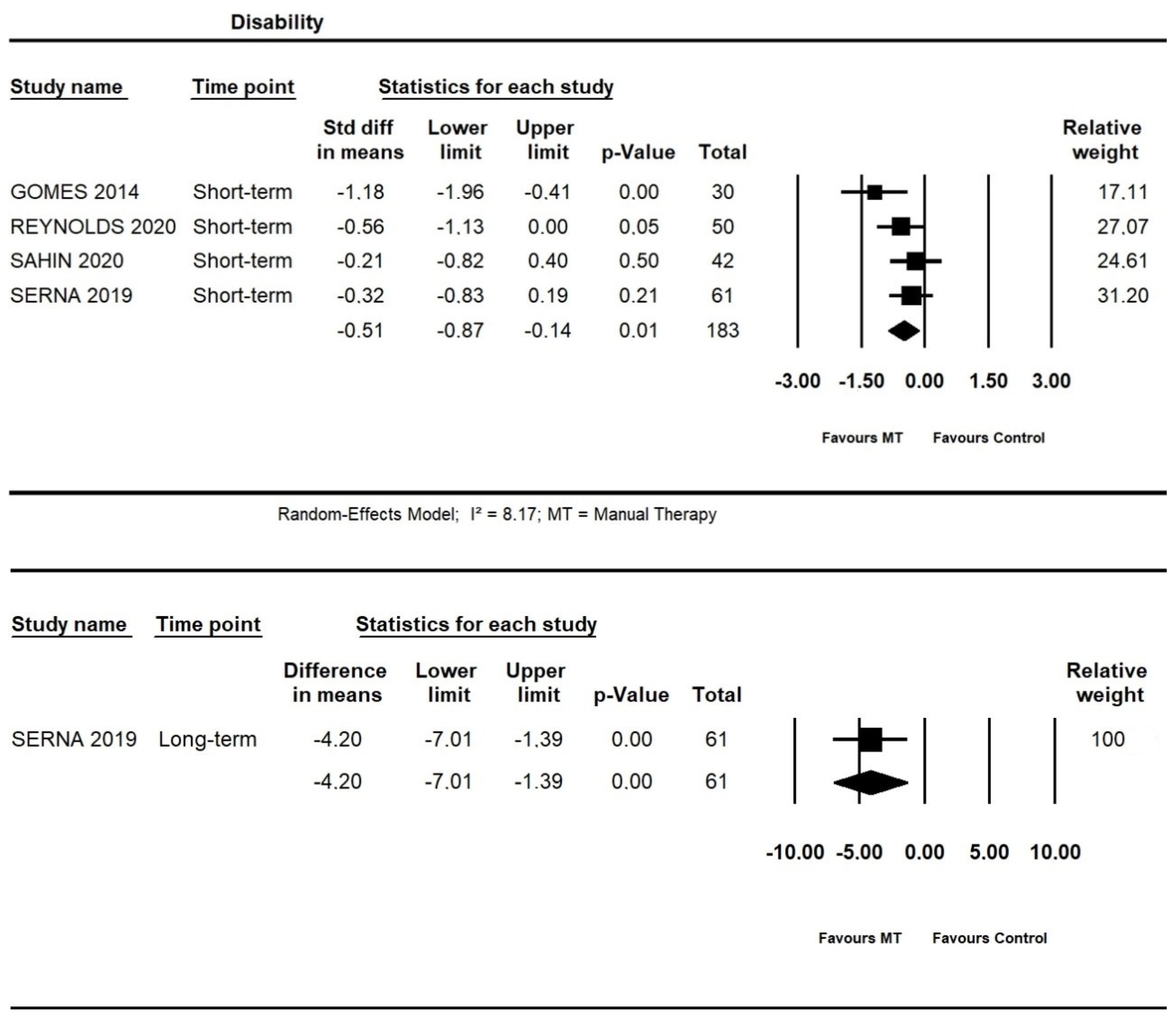
| MT add effects Disability Short-term | −0.51 (−0.87 to −0.14) * | 183 (4 studies) | ⨁⨁⨁⊝ MODERATE a | The difference is statistically significant and may have a Moderate effect size based on the Hedges’g cut-off point of 0.5. |
| MT vs. Control Disability Long-term | −4.20 (−7.01 to −1.39) | 61 (1 study) | ⨁⨁⊝⊝ LOW a,b | The difference is statistically significant but not clinically important based on a MDC = 8. |
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect; Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different; Low certainty: Confidence in the effect estimate is limited: The true effect may be substantially different from the estimated; Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect. | ||||
| Criteria for downgrade the certainty of evidence a Downgraded owing to imprecision: Sample size < 400; b Downgraded owing to inconsistence: When I² > 50% or when pooling was not possible; c Downgraded owing to risk of bias: >25% of the participants were from studies with a high risk of bias. | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vieira, L.S.; Pestana, P.R.M.; Miranda, J.P.; Soares, L.A.; Silva, F.; Alcantara, M.A.; Oliveira, V.C. The Efficacy of Manual Therapy Approaches on Pain, Maximum Mouth Opening and Disability in Temporomandibular Disorders: A Systematic Review of Randomised Controlled Trials. Life 2023, 13, 292. https://doi.org/10.3390/life13020292
Vieira LS, Pestana PRM, Miranda JP, Soares LA, Silva F, Alcantara MA, Oliveira VC. The Efficacy of Manual Therapy Approaches on Pain, Maximum Mouth Opening and Disability in Temporomandibular Disorders: A Systematic Review of Randomised Controlled Trials. Life. 2023; 13(2):292. https://doi.org/10.3390/life13020292
Chicago/Turabian StyleVieira, Leonardo Sette, Priscylla Ruany Mendes Pestana, Júlio Pascoal Miranda, Luana Aparecida Soares, Fabiana Silva, Marcus Alessandro Alcantara, and Vinicius Cunha Oliveira. 2023. "The Efficacy of Manual Therapy Approaches on Pain, Maximum Mouth Opening and Disability in Temporomandibular Disorders: A Systematic Review of Randomised Controlled Trials" Life 13, no. 2: 292. https://doi.org/10.3390/life13020292
APA StyleVieira, L. S., Pestana, P. R. M., Miranda, J. P., Soares, L. A., Silva, F., Alcantara, M. A., & Oliveira, V. C. (2023). The Efficacy of Manual Therapy Approaches on Pain, Maximum Mouth Opening and Disability in Temporomandibular Disorders: A Systematic Review of Randomised Controlled Trials. Life, 13(2), 292. https://doi.org/10.3390/life13020292