
The Association of Body Mass Index with COVID-19 Complications and Survival Rate at a Tertiary Hospital

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. BMI Calculation
2.3. Statistical Analyses
3. Results
3.1. Demographic Characteristics of the Study Sample
3.2. Assessing the Relationship between Demographics, Comorbidities, COVID-19 Outcomes, and BMI Category
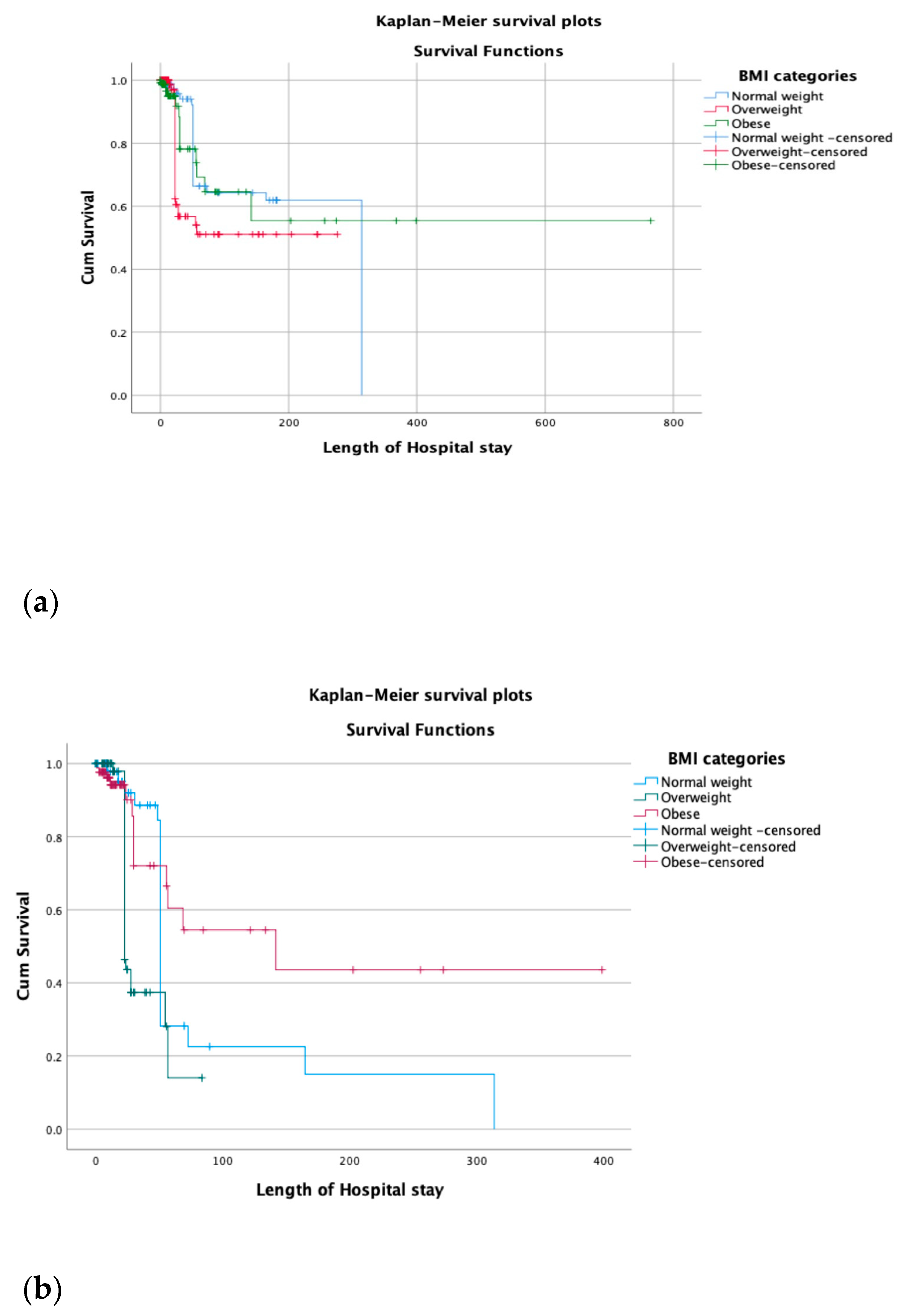
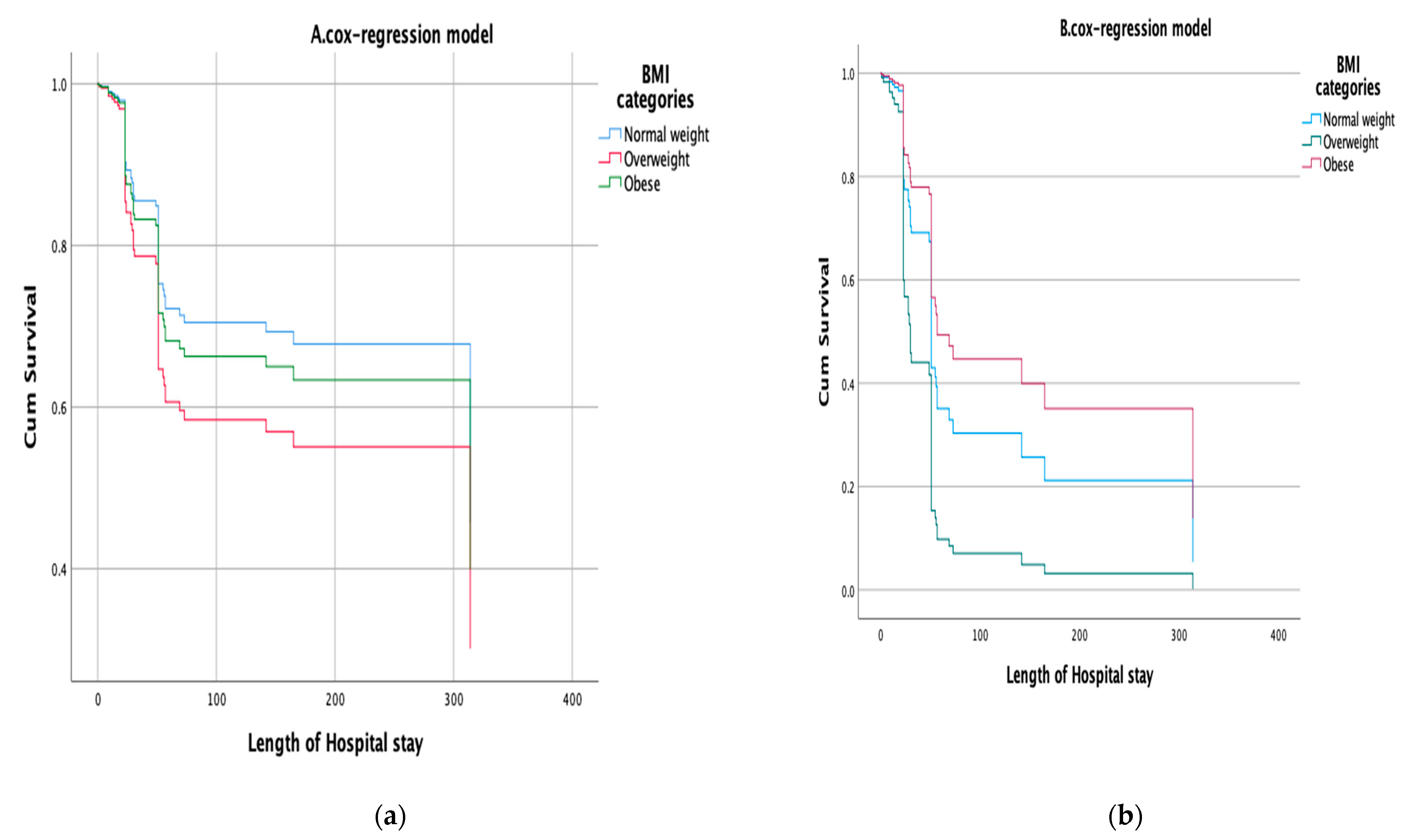
3.3. Estimated Relationship between BMI Categories as The independent Variable with COVID-19 Complication Outcomes and Mortality in Hospitalized and ICU Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Watanabe, M.; Caruso, D.; Tuccinardi, D.; Risi, R.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Tarallo, M.; Strigari, L.; Manfrini, S.; et al. Visceral fat shows the strongest association with the need of intensive care in patients with COVID-19. Metabolism 2020, 111, 154319. [Google Scholar] [CrossRef]
- AlKhafaji, D.; Al Argan, R.; Albahrani, S.; Al Elq, A.; Albaker, W.; Al-Hariri, M.; Alwaheed, A.; Alqatari, S.; Alzaki, A.; Alsaid, A.; et al. The impact of obesity on hospitalized patients with COVID-19 infection in the Eastern Province of Saudi Arabia. J. Med. Life 2022, 15, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, WHO. World Health Organisation Diabetes Country Profiles: Saudi Arabia. 2016. Available online: https://www.who.int/diabetes/country-profiles/sau_en.pdf (accessed on 31 May 2021).
- Cho, Y.; Cho, Y.; Choi, H.J.; Lee, H.; Lim, T.H.; Kang, H.; Ko, B.S.; Oh, J. The effect of BMI on COVID-19 outcomes among older patients in South Korea: A nationwide retrospective cohort study. Ann. Med. 2021, 53, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.D.; Meng, K.; Guan, H.Q.; Leng, L.; Zhu, R.R.; Wang, B.Y.; He, M.A.; Cheng, L.X.; Huang, K.; Zeng, Q.T. Clinical characteristics and outcomes of 112 cardiovascular disease patients infected by 2019-nCoV. Zhonghua Xin Xue Guan Bing Za Zhi 2020, 48, E004. [Google Scholar]
- Földi, M.; Farkas, N.; Kiss, S.; Zádori, N.; Váncsa, S.; Szakó, L.; Dembrovszky, F.; Solymár, M.; Bartalis, E.; Szakács, Z.; et al. Obesity is a risk factor for developing critical condition in COVID-19 patients: A systematic review and meta-analysis. Obes. Rev. 2020, 21, e13095. [Google Scholar] [CrossRef]
- Sjögren, L.; Stenberg, E.; Thuccani, M.; Martikainen, J.; Rylander, C.; Wallenius, V.; Olbers, T.; Kindblom, J.M. Impact of obesity on intensive care outcomes in patients with COVID-19 in Sweden—A cohort study. PLoS ONE 2021, 16, e0257891. [Google Scholar] [CrossRef]
- Zangeneh, M.; Valeh, T.; Sharifi, A. Survival analysis based on body mass index in patients with COVID-19 admitted to the intensive care unit of Amir Al-Momenin Hospital in Arak–2021. Obes. Med. 2022, 32, 100420. [Google Scholar] [CrossRef]
- Chandarana, H.; Dane, B.; Mikheev, A.; Taffel, M.; Feng, Y.; Rusinek, H. Visceral adipose tissue in patients with COVID-19: Risk stratification for severity. Abdom. Radiol. 2021, 46, 818–825. [Google Scholar] [CrossRef]
- Wu, J.; Li, W.; Shi, X. Early antiviral treatment contributes to alleviate the severity and improve the prognosis of patients with novel coronavirus disease (COVID-19). J. Intern. Med. 2020, 288, 128–138. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Lu, Y.; Huang, Y.-M. Obesity in patients with COVID-19: A systematic review and meta-analysis. Metabolism 2020, 113, 154378. [Google Scholar] [CrossRef] [PubMed]
- Barron, E.; Bakhai, C.; Kar, P.; Weaver, A.; Bradley, D.; Ismail, H.; Knighton, P.; Holman, N.; Khunti, K.; Sattar, N.; et al. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: A whole-population study. Lancet Diabetes Endocrinol. 2020, 8, 813–822. [Google Scholar] [CrossRef] [PubMed]
- O’brien, J.M.; Phillips, G.S.; Ali, N.A.; Lucarelli, M.; Marsh, C.B.; Lemeshow, S. Body mass index is independently associated with hospital mortality in mechanically ventilated adults with acute lung injury. Crit. Care Med. 2006, 34, 738–744. [Google Scholar] [CrossRef]
- Lindgren, M.; Toska, T.; Alex, C.; Lundberg, C.E.; Cronie, O.; Rosengren, A.; Adiels, M.; Sjöland, H. BMI, sex and outcomes in hospitalised patients in western Sweden during the COVID-19 pandemic. Sci. Rep. 2022, 12, 4918. [Google Scholar] [CrossRef]
- Popkin, B.M.; Du, S.; Green, W.D.; Beck, M.A.; Algaith, T.; Herbst, C.H.; Alsukait, R.F.; Alluhidan, M.; Alazemi, N.; Shekar, M. Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships. Obes. Rev. 2020, 21, e13128. [Google Scholar] [CrossRef]
- Griffith, G.J.; Morris, T.T.; Tudball, M.J.; Herbert, A.; Mancano, G.; Pike, L.; Sharp, G.C.; Sterne, J.; Palmer, T.M.; Smith, G.D.; et al. Collider bias undermines our understanding of COVID-19 disease risk and severity. Nat. Commun. 2020, 11, 5749. [Google Scholar] [CrossRef] [PubMed]
- Alyami, M.H.; Naser, A.Y.; Orabi, M.A.A.; Alwafi, H.; Alyami, H.S. Epidemiology of COVID-19 in the Kingdom of Saudi Arabia: An Ecological Study. Front. Public Health 2020, 8, 506. [Google Scholar] [CrossRef]
- Denova-Gutiérrez, E.; Lopez-Gatell, H.; Alomia-Zegarra, J.L.; López-Ridaura, R.; Zaragoza-Jimenez, C.A.; Dyer-Leal, D.D.; Cortés-Alcala, R.; Villa-Reyes, T.; Gutiérrez-Vargas, R.; Rodríguez-González, K.; et al. The Association of Obesity, Type 2 Diabetes, and Hypertension with Severe Coronavirus Disease 2019 on Admission Among Mexican Patients. Obesity 2020, 28, 1826–1832. [Google Scholar] [CrossRef]
- Rietman, M.L.; Van Der A, D.L.; Van Oostrom, S.H.; Picavet, H.S.J.; Dollé, M.E.T.; Van Steeg, H.; Verschuren, W.M.M.; Spijkerman, A.M.W. The association between BMI and different frailty domains: A U-shaped curve? J. Nutr. Health Aging 2018, 22, 8–15. [Google Scholar] [CrossRef]
- Owen, W.F.; Carmona, R.; Pomeroy, C. Failing Another National Stress Test on Health Disparities. JAMA 2020, 323, 1905–1906. [Google Scholar] [CrossRef] [Green Version]
- Townsend, M.J.; Kyle, T.K.; Stanford, F.C. Outcomes of COVID-19: Disparities in obesity and by ethnicity/race. Int. J. Obes. 2020, 44, 1807–1809. [Google Scholar] [CrossRef]
- Clift, A.K.; Coupland, C.A.C.; Keogh, R.H.; Diaz-Ordaz, K.; Williamson, E.; Harrison, E.M.; Hayward, A.; Hemingway, H.; Horby, P.; Mehta, N.; et al. Living risk prediction algorithm (QCOVID) for risk of hospital admission and mortality from coronavirus 19 in adults: National derivation and validation cohort study. BMJ 2020, 371, m3731. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Ho, F.K.; Gill, J.M.; Ghouri, N.; Gray, S.R.; Celis-Morales, C.A.; Katikireddi, S.V.; Berry, C.; Pell, J.P.; McMurray, J.J.; et al. BMI and future risk for COVID-19 infection and death across sex, age and ethnicity: Preliminary findings from UK biobank. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1149–1151. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Young, D.; Coupland, C.; Channon, K.M.; Tan, P.S.; A Harrison, D.; Rowan, K.; Aveyard, P.; Pavord, I.D.; Watkinson, P.J. Risk of severe COVID-19 disease with ACE inhibitors and angiotensin receptor blockers: Cohort study including 8.3 million people. Heart 2020, 106, 1503–1511. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, J.; Carter, B.; Vilches-Moraga, A.; Quinn, T.J.; Braude, P.; Verduri, A.; Pearce, L.; Stechman, M.; Short, R.; Price, A.; et al. The effect of frailty on survival in patients with COVID-19 (COPE): A multicentre, European, observational cohort study. Lancet Public Health 2020, 5, e444–e451. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, S.M.; O’Rahilly, S. When two pandemics meet: Why is obesity associated with increased COVID-19 mortality? Medicine 2020, 1, 33–42. [Google Scholar] [CrossRef]
- Battisti, S.; Pedone, C.; Napoli, N.; Russo, E.; Agnoletti, V.; Nigra, S.G.; Dengo, C.; Mughetti, M.; Conte, C.; Pozzilli, P.; et al. Computed Tomography Highlights Increased Visceral Adiposity Associated With Critical Illness in COVID-19. Diabetes Care 2020, 43, e129–e130. [Google Scholar] [CrossRef]
- Umbrello, M.; Fumagalli, J.; Pesenti, A.; Chiumello, D. Pathophysiology and Management of Acute Respiratory Distress Syndrome in Obese Patients. Semin. Respir. Crit. Care Med. 2019, 40, 40–56. [Google Scholar] [CrossRef]
- Ni, Y.-N.; Luo, J.; Yu, H.; Wang, Y.-W.; Hu, Y.-H.; Liu, D.; Liang, B.-M.; Liang, Z.-A. Can body mass index predict clinical outcomes for patients with acute lung injury/acute respiratory distress syndrome? A meta-analysis. Crit. Care 2017, 21, 36. [Google Scholar] [CrossRef] [Green Version]
- Dietz, W.; Santos-Burgoa, C. Obesity and its Implications for COVID-19 Mortality. Obesity 2020, 28, 1005. [Google Scholar] [CrossRef] [Green Version]
- Melebari, S.; ElBahrawy, A.; Aljahdali, A.; Hussain, N.; Bahwaireth, L.; Alahmadi, G.; Alharbi, R.; Alghamdi, J.; Alzahrani, O. The prevalence of obesity in hospitalized COVID-19 patients at King Abdullah Medical City, Makkah, Saudi Arabia. Int. J. Med. Dev. Ctries. 2020, 5, 1579–1582. [Google Scholar] [CrossRef]
- Gao, F.; Zheng, K.I.; Wang, X.-B.; Sun, Q.-F.; Pan, K.-H.; Wang, T.-Y.; Chen, Y.-P.; Targher, G.; Byrne, C.D.; George, J.; et al. Obesity Is a Risk Factor for Greater COVID-19 Severity. Diabetes Care 2020, 43, e72–e74. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total = 600 | Normal Weight = 157 | Overweight = 188 | Obese 255 | (p-Value) |
|---|---|---|---|---|---|
| (1) Demographical | |||||
| (a) Age group | <0.001 * | ||||
| <20 | 26 (4.3%) | 14 (8.9 %) | 9 (4.8%) | 3 (1.2%) | |
| 20–40 | 158 (26.3%) | 44 (28 %) | 42 (22.3%) | 72 (28.2%) | |
| 41–60 | 248 (41.3%) | 53 (33.8 %) | 82 (43.6%) | 113 (44.3%) | |
| 61–80 | 145 (24.2%) | 36 (22.9 %) | 45 (23.9%) | 64 (25.1%) | |
| >80 | 23 (3.8%) | 10 (6.4 %) | 10 (5.3%) | 3 (1.2%) | |
| (b) Gender | 0.005 * | ||||
| Female | 219 (36.5%) | 50 (28%) | 64 (34 %) | 111 (43.5 %) | |
| Male | 381 (63.5%) | 132 (72 %) | 123 (66%) | 144 (56.5 %) | |
| (2) comorbidities | Total =600 | Normal weight =157 | Overweight =188 | Obese 255 | (p-Value) |
| (a) Diabetes mellitus | |||||
| Yes | 285 (47.5%) | 100 (55.4 %) | 82 (43.6 %) | 116 (45.5 %) | |
| No | 315 (52.5%) | 82 (44.6%) | 105 (56.4%) | 139 (54.5 %) | 0.064 |
| (b) Cardiovascular disease | |||||
| Yes | 110 (18.3%) | 26 (16.6 %) | 49 (26.1%) | 35 (13.7%) | |
| No | 490 (81.7%) | 131 (83.4 %) | 139 (73.9%) | 220 (86.3%) | 0.003 * |
| (c)Respiratory Diseases (RD) | 0.013 * | ||||
| Yes | 72 (12%) | 27 (17.2%) | 13 (6.9 %) | 32 (12.5%) | |
| No | 528 (88%) | 130 (82.8 %) | 175 (93.1 %) | 223 (87.5%) | |
| End-Stage Renal Disease (ESRD) | 0.021 * | ||||
| Yes | 33 (5.5%) | 15 (5.1%) | 4 (2.1 %) | 14 (8.9%) | |
| NO | 567 (94.5%) | 240 (94.1 %) | 184 (97.9 %) | 143 (91.1%) | |
| (3) The outcomes | Total = 600 | Normal weight = 157 | Overweight = 188 | Obese 255 | (p-value) |
| (a) Admission to ICU | 0.418 | ||||
| Yes | 203 (33.8%) | 48 (30.6 %) | 70 (37.2 %) | 85 (33.3 %) | |
| No | 397 (66.16%) | 109 (69.4 %) | 118 (62.8%) | 170 (66.7 %) | |
| (b) O2<93% | 0.002 * | ||||
| Yes | 307 (51.2%) | 68 (43.3 %) | 87 (46.3%) | 152 (59.6 %) | |
| NO | 293 (48.8%) | 89 (56.7 %) | 101 (53.7%) | 103 (40.4 %) | |
| (c) Mechanical ventilation | <0.001 * | ||||
| Yes | 83 (13.8%) | 10 (6.4 %) | 39 (20.7 %) | 34 (13.3 %) | |
| No | 517 (86.2%) | 147 (93.6%) | 149 (79.3 %) | 221 (86.7 %) | |
| (d)lung infiltrate | <0.001 * | ||||
| Yes | 364 (60.7%) | 85 (54.1 %) | 90 (47.9%) | 189 (74.1%) | |
| No | 236 (39.3%) | 72 (45.9 %) | 98 (52.1%) | 66 (25.9 %) | |
| (f) Death | 0.004 * | ||||
| Yes | 65 (10.8%) | 23 (14.6 %) | 27 (14.4%) | 15 (5.9%) | |
| No | 535 (89.2%) | 134 (85.4%) | 161 (85.6 %) | 240 (94.1%) |
| BMI | N = 600 | Mean Rank | df | X2 | p-Value | Post Hoc Analysis | p-Value |
|---|---|---|---|---|---|---|---|
| Normal weight 18.5–24.9 | 157 | 345.66 | 2 | 19.79 | <0.001 * | Normal weight vs. Overweight | 0.110 |
| Overweight 25–29.9 | 188 | 306.56 | Normal weight vs. Obese | <0.001 * | |||
| Obese ≥30 Kg/m2 | 255 | 268.23 | Overweight vs. Obese | 0.064 |
| Model 1. BMI Adjusted for Age, Gender, CVD, RD, and ESRD | ||||||
|---|---|---|---|---|---|---|
| Variable | O2 < 93% | Mechanical Ventilation | Lung Infiltrate | |||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR(95% CI) | p-Value | |
| Normal weight (reference group) | - | - | - | - | - | - |
| Overweight | 1.55 (0.958–2.519) | 0.074 | 3.666 (1.660–8.096) | 0.001 | 0.894 (0.555–1.439) | 0.664 |
| Obese | 2.450 (1.837–4.610) | <0.001 | 2.815 (1.261–6.285) | 0.012 | 3.384 (2.111–5.477) | <0.001 |
| Model A. BMI Adjusted for Age, Gender, CVD, RD, and ESRD | Model B. BMI Adjusted for Age, Gender, CVD, RD, and ESRD | |||||
|---|---|---|---|---|---|---|
| Variable | Death | Death | ||||
| HR | (95% CI) | p-Value | HR | (95% CI) | p-Value | |
| Normal weight (reference group) | - | - | - | - | - | - |
| Overweight | 1.535 | (0.794–2.966) | 0.202 | 2.222 | (1.204–4.098) | 0.011 |
| Obese | 1.175 | (0.570–2.421) | 0.662 | 0.675 | (0.339–1.345) | 0.263 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlBahrani, S.; Al-Maqati, T.N.; Al Naam, Y.A.; Alqahtani, J.S.; Alqahtani, A.S.; AlRabeeah, S.; Aldhahir, A.M.; Alkhalaf, F.; Alzuraiq, H.R.; Alenezi, M.H.; et al. The Association of Body Mass Index with COVID-19 Complications and Survival Rate at a Tertiary Hospital. Life 2023, 13, 1572. https://doi.org/10.3390/life13071572
AlBahrani S, Al-Maqati TN, Al Naam YA, Alqahtani JS, Alqahtani AS, AlRabeeah S, Aldhahir AM, Alkhalaf F, Alzuraiq HR, Alenezi MH, et al. The Association of Body Mass Index with COVID-19 Complications and Survival Rate at a Tertiary Hospital. Life. 2023; 13(7):1572. https://doi.org/10.3390/life13071572
Chicago/Turabian StyleAlBahrani, Salma, Thekra N. Al-Maqati, Yaser A. Al Naam, Jaber S. Alqahtani, Abdullah S. Alqahtani, Saad AlRabeeah, Abdulelah M. Aldhahir, Faisal Alkhalaf, Hind R. Alzuraiq, Maryam Hamad Alenezi, and et al. 2023. "The Association of Body Mass Index with COVID-19 Complications and Survival Rate at a Tertiary Hospital" Life 13, no. 7: 1572. https://doi.org/10.3390/life13071572
APA StyleAlBahrani, S., Al-Maqati, T. N., Al Naam, Y. A., Alqahtani, J. S., Alqahtani, A. S., AlRabeeah, S., Aldhahir, A. M., Alkhalaf, F., Alzuraiq, H. R., Alenezi, M. H., Alzahrani, A., Bakkar, M., Albahrani, Z., & Maawadh, R. M. (2023). The Association of Body Mass Index with COVID-19 Complications and Survival Rate at a Tertiary Hospital. Life, 13(7), 1572. https://doi.org/10.3390/life13071572