

A Dietary and Lifestyle Intervention Improves Treatment Adherence and Clinical Outcomes in Overweight and Obese Patients with Obstructive Sleep Apnea: A Randomized, Controlled Trial

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
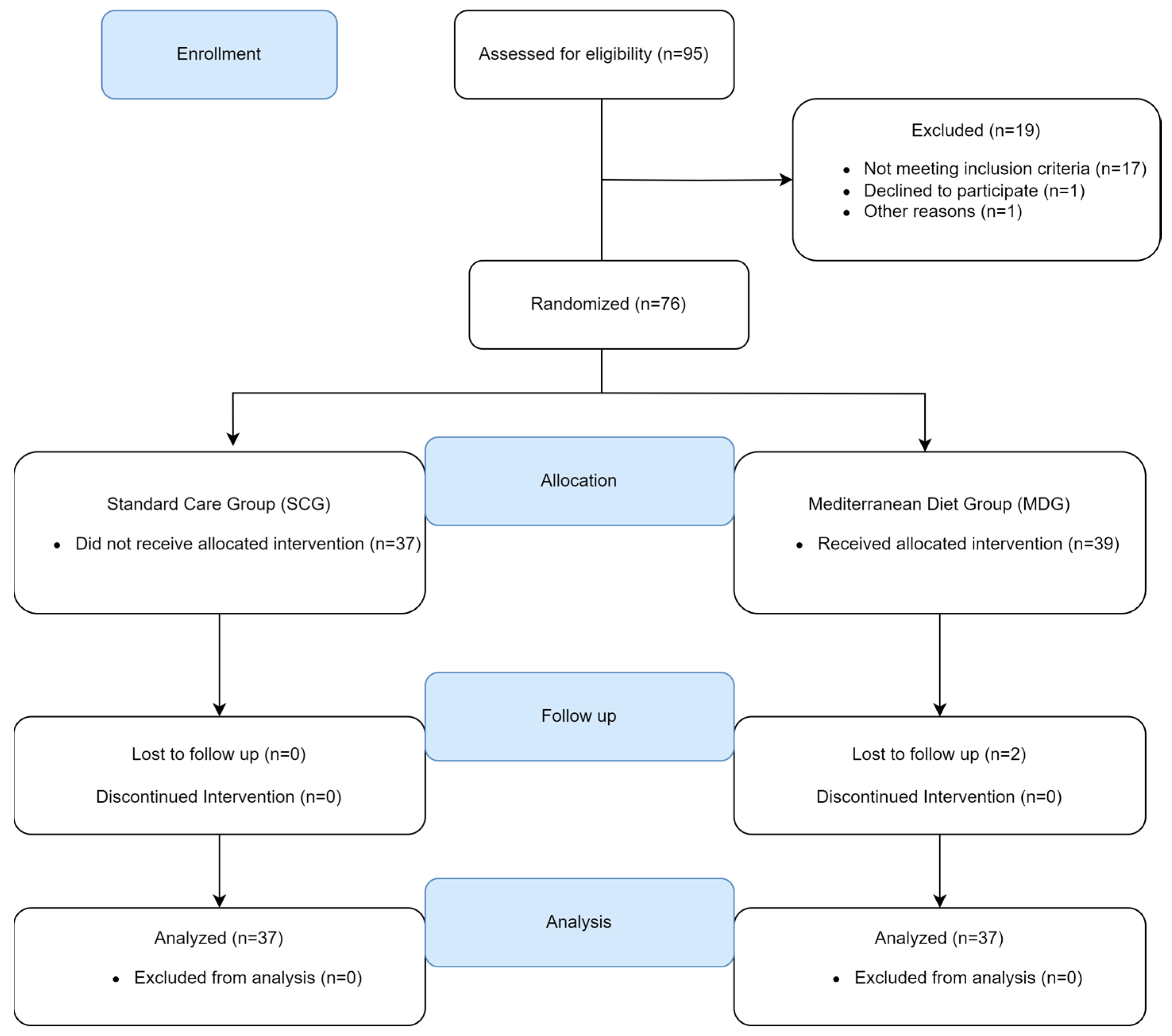
2.1. Study Patients
2.2. Data Collection
2.2.1. Epworth Sleepiness Scale (ESS)
2.2.2. Beck Depression Inventory (BDI)
2.3. Follow-Up—Usual (Standard) Care Group
2.4. Follow-Up—Intervention Group
2.4.1. Food Frequency Questionnaire
2.4.2. Mediterranean Diet Score
2.5. PAP Adherence
2.6. Statistical Analysis
3. Results
3.1. Comparison of Baseline Characteristics between the SCG and the MDG
3.2. PAP Adherence
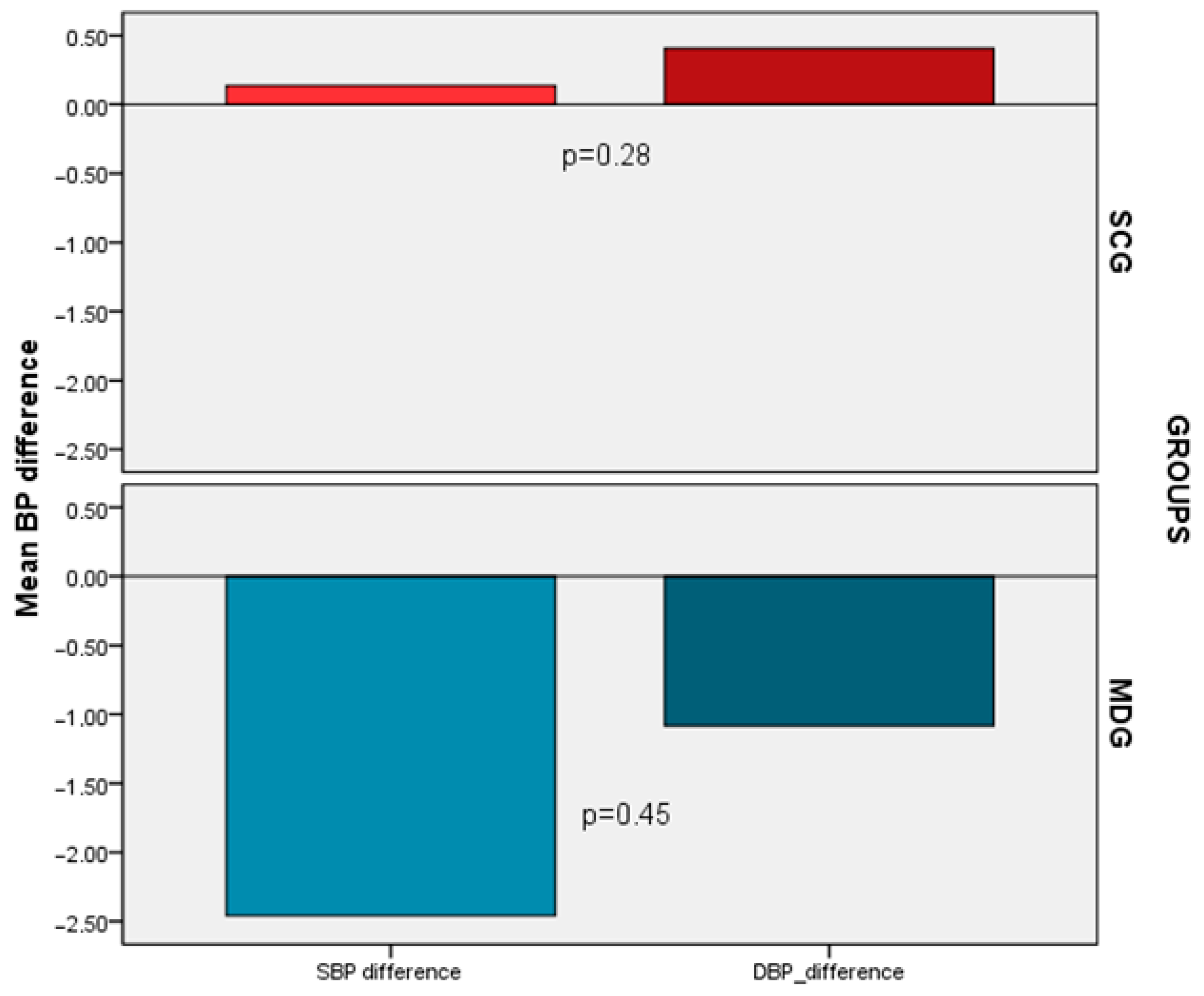
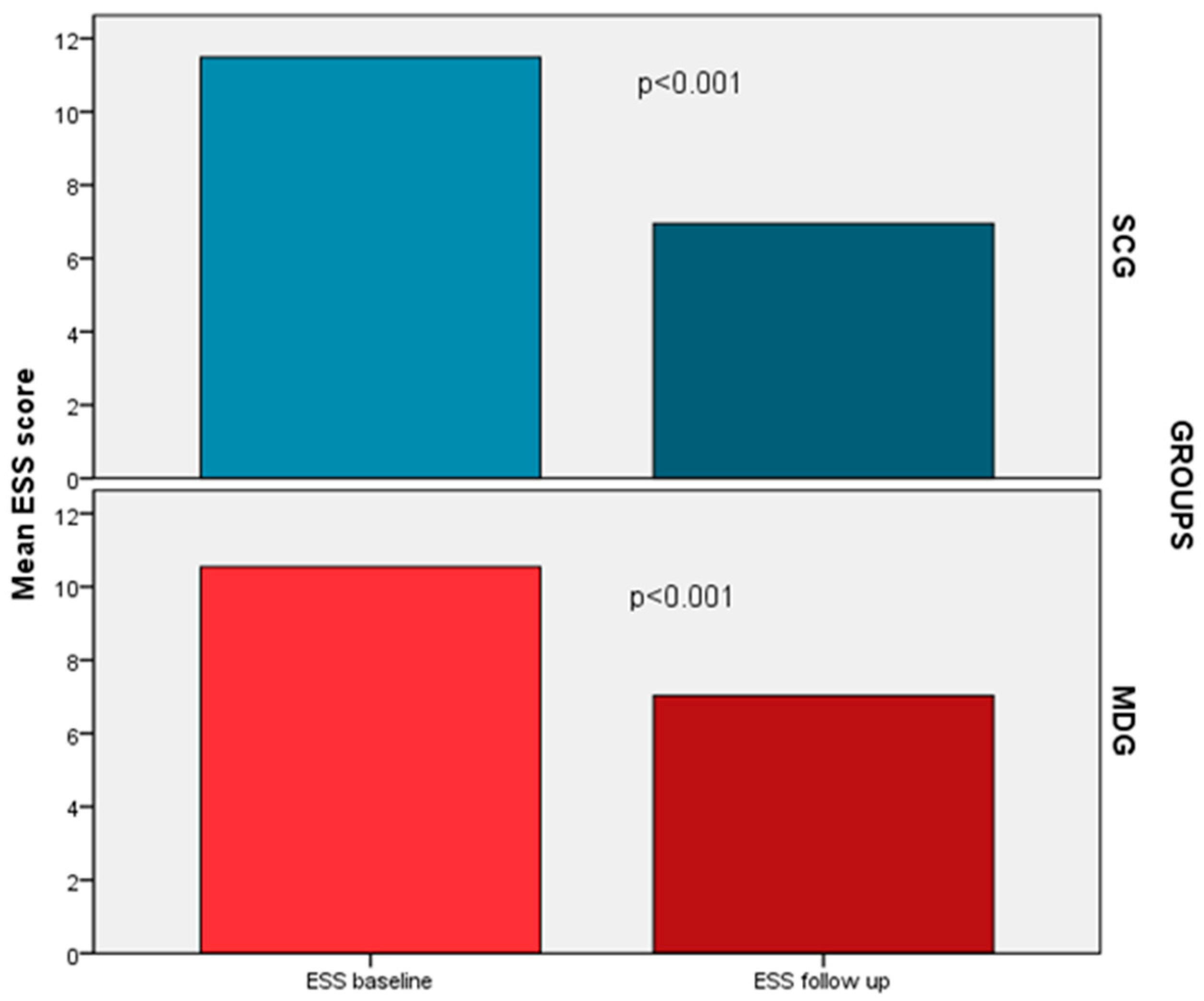
3.3. Effect of Diet Intervention on Anthropometric and Daytime Symptoms Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Resp. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Yeghiazarians, Y.; Jneid, H.; Tietjens, J.R.; Redline, S.; Brown, D.L.; El-Sherif, N.; Mehra, R.; Bozkurt, B.; Ndumele, C.E.; Somers, V.K. Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e56–e67. [Google Scholar] [CrossRef] [PubMed]
- Frost & Sullivan; American Academy of Sleep Medicine. Hidden Health Crisis Costing America billions: Underdiagnosing and Undertreating Obstructive Sleep Apnea Draining Health Care System. Published 8 August 2016. Available online: https://aasm.org/resources/pdf/sleep-apnea-economic-crisis.pdf (accessed on 22 March 2023).
- Knauert, M.; Naik, S.; Gillespie, M.B.; Kryger, M. Clinical consequences and economic costs of untreated obstructive sleep apnea syndrome. World J. Otorhinolaryngol. Head Neck Surg. 2015, 1, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.R. The complex relationship between weight and sleep apnoea. Thorax 2015, 70, 205–206. [Google Scholar] [CrossRef]
- Sareli, A.E.; Cantor, C.R.; Williams, N.N.; Korus, G.; Raper, S.E.; Pien, G.; Hurley, S.; Maislin, G.; Schwab, R.J. Obstructive sleep apnea in patients undergoing bariatric surgery—A tertiary center experience. Obes. Surg. 2011, 21, 316–327. [Google Scholar] [CrossRef]
- Giles, T.L.; Lasserson, T.J.; Smith, B.J.; White, J.; Wright, J.; Cates, C.J. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst. Rev. 2006, 1, CD001106. [Google Scholar]
- Pepperell, J.C.; Ramdassingh-Dow, S.; Crosthwaite, N.; Mullins, R.; Jenkinson, C.; Stradling, J.R.; Davies, R.J. Ambulatory blood pressure after therapeutic and subtherapeutic nasal continuous positive airway pressure for obstructive sleep apnoea: A randomised parallel trial. Lancet 2002, 359, 204–210. [Google Scholar] [CrossRef]
- Walia, H.K.; Thompson, N.R.; Pascoe, M.; Faisal, M.; Moul, D.E.; Katzan, I.; Mehra, R.; Foldvary-Schaefer, N. Effect of Positive Airway Pressure Therapy on Drowsy Driving in a Large Clinic-Based Obstructive Sleep Apnea Cohort. J. Clin. Sleep Med. 2019, 15, 1613–1620. [Google Scholar] [CrossRef]
- Weaver, T.E.; Grunstein, R.R. Adherence to continuous positive airway pressure therapy: The challenge to effective treatment. Proc. Am. Thorac. Soc. 2008, 5, 173–178. [Google Scholar] [CrossRef]
- Pepin, J.L.; Baillieul, S.; Tamisier, R. Reshaping sleep apnea care: Time for value-based strategies. Ann. Am. Thorac. Soc. 2019, 16, 1501–1503. [Google Scholar] [CrossRef]
- Johansson, K.; Neovius, M.; Lagerros, Y.T.; Harlid, R.; Rössner, S.; Granath, F.; Hemmingsson, E. Effect of a very low energy diet on moderate and severe obstructive sleep apnoea in obese men: A randomised controlled trial. BMJ 2009, 339, b4609. [Google Scholar] [CrossRef] [PubMed]
- Tuomilehto, H.P.; Seppä, J.M.; Partinen, M.M.; Peltonen, M.; Gylling, H.; Tuomilehto, J.O.; Vanninen, E.J.; Kokkarinen, J.; Sahlman, J.K.; Martikainen, T.; et al. Lifestyle intervention with weight reduction: First-line treatment in mild obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2009, 179, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Stelmach-Mardas, M.; Brajer-Luftmann, B.; Kuśnierczak, M.; Batura-Gabryel, H.; Piorunek, T.; Mardas, M. Body Mass Index Reduction and Selected Cardiometabolic Risk Factors in Obstructive Sleep Apnea: Meta-Analysis. J. Clin. Med. 2021, 10, 1485. [Google Scholar] [CrossRef]
- Georgoulis, M.; Yiannakouris, N.; Kechribari, I.; Lamprou, K.; Perraki, E.; Vagiakis, E.; Kontogianni, M.D. Cardiometabolic Benefits of a Weight-Loss Mediterranean Diet/Lifestyle Intervention in Patients with Obstructive Sleep Apnea: The “MIMOSA” Randomized Clinical Trial. Nutrients 2020, 12, 1570. [Google Scholar] [CrossRef]
- Georgoulis, M.; Yiannakouris, N.; Tenta, R.; Fragopoulou, E.; Kechribari, I.; Lamprou, K.; Perraki, E.; Vagiakis, E.; Kontogianni, M.D. A weight-loss Mediterranean diet/lifestyle intervention ameliorates inflammation and oxidative stress in patients with obstructive sleep apnea: Results of the “MIMOSA” randomized clinical trial. Eur. J. Nutr. 2021, 60, 3799–3810. [Google Scholar] [CrossRef] [PubMed]
- Georgoulis, M.; Yiannakouris, N.; Kechribari, I.; Lamprou, K.; Perraki, E.; Vagiakis, E.; Kontogianni, M.D. Dose-response relationship between weight loss and improvements in obstructive sleep apnea severity after a diet/lifestyle interventions: Secondary analyses of the “MIMOSA” randomized clinical trial. J. Clin. Sleep Med. 2022, 18, 1251–1261. [Google Scholar] [CrossRef]
- Georgoulis, M.; Yiannakouris, N.; Kechribari, I.; Lamprou, K.; Perraki, E.; Vagiakis, E.; Kontogianni, M.D. Sustained improvements in the cardiometabolic profile of patients with obstructive sleep apnea after a weight-loss Mediterranean diet/lifestyle intervention: 12-month follow-up (6 months post-intervention) of the “MIMOSA” randomized clinical trial. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 1019–1028. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness:the Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Garbin, M.G. Psychometric properties of the Beck depression inventory: Twenty-five years of evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Bouloukaki, I.; Giannadaki, K.; Mermigkis, C.; Tzanakis, N.; Mauroudi, E.; Moniaki, V.; Michelakis, S.; Siafakas, N.M.; Schiza, S.E. Intensive versus standard follow-up to improve continuous positive airway pressure compliance. Eur. Respir. J. 2014, 44, 1262–1274. [Google Scholar] [CrossRef]
- Bayram, S.Ş.; Aktaş, N. Mediterranean diet and frequently used indexes for measuring Mediterranean diet quality. In Proceedings of the International Eurasian Congress on “Natural Nutrition and Healthy Life”, Ankara, Turkey, 12–15 July 2018; Karaman, M.R., Artık, N., Şanlıer, N., Eds.; Ankara University Institute of Food Safety “Pelin Ofset”: Ankara, Turkey, 2018. [Google Scholar]
- Bountziouka, V.; Bathrellou, E.; Giotopoulou, A.; Katsagoni, C.; Bonou, M.; Vallianou, N.; Barbetseas, J.; Avgerinos, P.C.; Panagiotakos, D.B. Development, repeatability and validity regarding energy and macronutrient intake of a semi-quantitative food frequency questionnaire: Methodological considerations. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Arvaniti, F.; Stefanadis, C. Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesterolemia, diabetes and obesity, among healthy adults; the accuracy of the MedDietScore. Prev. Med. 2007, 44, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Kribbs, N.B.; Pack, A.I.; Kline, L.R.; Smith, P.L.; Schwartz, A.R.; Schubert, N.M.; Redline, S.; Henry, J.N.; Getsy, J.E.; Dinges, D.F. Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 1993, 147, 887–895. [Google Scholar] [CrossRef]
- Weaver, T.E.; Maislin, G.; Dinges, D.F.; Bloxham, T.; George, C.F.; Greenberg, H.; Kader, G.; Mahowald, M.; Younger, J.; Pack, A.I. Relationship between hours of CPAP use and achieving normal levels of sleepiness and daily functioning. Sleep 2007, 30, 711–719. [Google Scholar] [CrossRef]
- Carneiro-Barrera, A.; Amaro-Gahete, F.J.; Guillén-Riquelme, A.; Jurado-Fasoli, L.; Sáez-Roca, G.; Martín-Carrasco, C.; Buela-Casal, G.; Ruiz, J.R. Effect of an Interdisciplinary Weight Loss and Lifestyle Intervention on Obstructive Sleep Apnea Severity: The INTERAPNEA Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e228212. [Google Scholar] [CrossRef] [PubMed]
- Igelström, H.; Åsenlöf, P.; Emtner, M.; Lindberg, E. Improvement in obstructive sleep apnea after a tailored behavioural sleep medicine intervention targeting healthy eating and physical activity: A randomised controlled trial. Sleep Breath. 2018, 22, 653–661. [Google Scholar] [CrossRef]
- Spörndly-Nees, S.; Åsenlöf, P.; Lindberg, E.; Emtner, M.; Igelström, H. Effects on obstructive sleep apnea severity following a tailored behavioral sleep medicine intervention aimed at increased physical activity and sound eating: An 18-month follow-up of a randomized controlled trial. J. Clin. Sleep Med. 2020, 16, 705–713. [Google Scholar] [CrossRef]
- Schiavo, L.; Pierro, R.; Asteria, C.; Calabrese, P.; Di Biasio, A.; Coluzzi, I.; Severino, L.; Giovanelli, A.; Pilone, V.; Silecchia, G. Low-Calorie Ketogenic Diet with Continuous Positive Airway Pressure to Alleviate Severe Obstructive Sleep Apnea Syndrome in Patients with Obesity Scheduled for Bariatric/Metabolic Surgery: A Pilot, Prospective, Randomized Multicenter Comparative Study. Obes. Surg. 2022, 32, 634–642. [Google Scholar] [CrossRef]
- McEvoy, R.D.; Antic, N.A.; Heeley, E.; Luo, Y.; Ou, Q.; Zhang, X.; Mediano, O.; Chen, R.; Drager, L.F.; Liu, Z.; et al. SAVE Investigators and Coordinators CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea. N. Engl. J. Med. 2016, 375, 919–931. [Google Scholar] [CrossRef]
- Batool-Anwar, S.; Goodwin, J.L.; Kushida, C.A.; Walsh, J.A.; Simon, R.D.; Nichols, D.A.; Quan, S.F. Impact of continuous positive airway pressure (CPAP) on quality of life in patients with obstructive sleep apnea (OSA). J. Sleep Res. 2016, 25, 731–738. [Google Scholar] [CrossRef]
- Hudgel, D.W.; Patel, S.R.; Ahasic, A.M.; Bartlett, S.J.; Bessesen, D.H.; Coaker, M.A.; Fiander, P.M.; Grunstein, R.R.; Gurubhagavatula, I.; Kapur, V.K.; et al. The role of weight management in the treatment of adult obstructive sleep apnea. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e70–e87. [Google Scholar] [CrossRef]
- Rokou, A.; Eleftheriou, A.; Tsigalou, C.; Apessos, I.; Nena, E.; Dalamaga, M.; Voulgaris, A.; Steiropoulos, P. Effect of the Implementation of a Structured Diet Management Plan on the Severity of Obstructive Sleep Apnea: A Systematic Review. Curr. Nutr. Rep. 2023, 12, 26–38. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. Obesity Society. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014, 129, S102–S138. [Google Scholar] [CrossRef]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. Obesity Management Task Force of the European Association for the Study of Obesity. European Guidelines for obesity management in adults. Obes Facts 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, C.; Schiza, S.E.; Bouloukaki, I.; Hatzis, C.M.; Kafatos, A.G.; Siafakas, N.M.; Tzanakis, N.E. Effect of Mediterranean diet versus prudent diet combined with physical activity on: A randomised trial. Eur. Respir. J. 2012, 39, 1398–1404. [Google Scholar] [CrossRef]
- Georgoulis, M.; Yiannakouris, N.; Kechribari, I.; Lamprou, K.; Perraki, E.; Vagiakis, E.; Kontogianni, M.D. The effectiveness of a weight-loss Mediterranean diet/lifestyle intervention in the management of obstructive sleep apnea: Results of the “MIMOSA” randomized clinical trial. Clin. Nutr. 2021, 40, 850–859. [Google Scholar] [CrossRef] [PubMed]
- Lankford, D.A.; Proctor, C.D.; Richard, R. Continuous positive airway pressure (CPAP) changes in bariatric surgery patients undergoing rapid weight loss. Obes. Surg. 2005, 15, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Ghadiri, M.; Grunstein, R.R. Clinical side effects of continuous positive airway pressure in patients with obstructive sleep apnoea. Respirology 2020, 25, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, E.; Benediktsdottir, B.; Franklin, K.A.; Holm, M.; Johannessen, A.; Jögi, R.; Gislason, T.; Real, F.G.; Schlünssen, V.; Janson, C. Women with symptoms of sleep-disordered breathing are less likely to be diagnosed and treated for sleep apnea than men. Sleep Med. 2017, 35, 17–22. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All OSA Patients (n = 74) | OSA SCGroup (n = 37) | OSA MDGroup (n = 37) | p Value | |
|---|---|---|---|---|
| Demographics | ||||
| Gender, males (%) | 58 (78%) | 36 (97%) | 22 (60%) | <0.001 |
| Age (years) | 53 ± 11 | 53 ± 10 | 53 ± 13 | 0.79 |
| Age ≥ 60 years | 24 (32%) | 10 (27%) | 14 (38%) | 0.32 |
| BMI (kg/m2) | 36 ± 8 | 35 ± 8 | 38 ± 9 | 0.16 |
| BMI ≥ 30 | 57 (77%) | 28 (76%) | 29 (78%) | 0.78 |
| Neck circumference (cm) | 42 ± 4 | 42 ± 3 | 43 ± 4 | 0.54 |
| Waist circumference (cm) | 120 ± 16 | 120 ± 17 | 121± 15 | 0.65 |
| Hip circumference (cm) | 120 ± 17 | 118 ± 16 | 123 ± 18 | 0.16 |
| Waist/hip circumference ratio | 1.0 ± 0.07 | 1.0 ± 0.06 | 0.99 ± 0.07 | 0.07 |
| Educational Level | ||||
| Primary level or less | 10 (13%) | 7 (19%) | 3 (8%) | |
| Secondary level | 38 (52%) | 18 (49%) | 20 (54%) | |
| Tertiary level or higher | 26 (35%) | 12 (32%) | 14 (38%) | 0.75 |
| Smoking status | ||||
| Never, n (%) | 26 (36%) | 11 (30%) | 15 (40%) | |
| Currently smoking, n (%) | 21 (28%) | 10 (27%) | 11 (30%) | |
| Former, n (%) | 26 (36%) | 16 (43%) | 11 (30%) | 0.36 |
| Pack-years | 15 (0, 39) | 15 (0, 40) | 13 (0, 39) | 0.49 |
| Co-morbidities | ||||
| Hypertension | 36 (49%) | 19 (51%) | 17 (46%) | 0.64 |
| Coronary heart disease | 5 (7%) | 1 (3%) | 4 (11%) | 0.17 |
| Atrial fibrillation | 8 (11%) | 2 (5%) | 6 (16%) | 0.13 |
| Cardiovascular disease | 20 (27%) | 5 (14%) | 15 (41%) | 0.009 |
| Diabetes type II | 11 (15%) | 5 (14%) | 6 (16%) | 0.74 |
| COPD | 16 (22%) | 9 (24%) | 7 (19%) | 0.57 |
| Bronchial asthma | 10 (14%) | 5 (14%) | 5 (14%) | 1.00 |
| Hypothyroidism | 11 (15%) | 4 (11%) | 7 (19%) | 0.33 |
| Dyslipidemia | 29 (39%) | 17 (46%) | 12 (32%) | 0.23 |
| Depression | 8 (11%) | 2 (5%) | 6 (16%) | 0.13 |
| BP measurements | ||||
| SBP (mmHg) | 126 ± 14 | 127 ± 16 | 124 ± 13 | 0.37 |
| DBP (mmHg) | 78 ± 10 | 78 ± 11 | 77 ± 9 | 0.60 |
| All OSA Patients (n = 74) | OSA SCGroup (n = 37) | OSA MDGroup (n = 37) | p Value | |
|---|---|---|---|---|
| Total recording time (min) | 406 ± 40 | 404 ± 47 | 410 ± 31 | 0.53 |
| Total sleep time (min) | 276 ± 52 | 274 ± 52 | 280 ± 52 | 0.65 |
| Sleep efficiency, % | 68 ± 12 | 68 ± 12 | 68 ± 12 | 0.95 |
| Wake after sleep onset time (min) | 91 ± 36 | 95 ± 40 | 89 ± 33 | 0.53 |
| Sleep latency | 35 (24, 62) | 33 (25, 57) | 35 (24, 67) | 0.75 |
| REM latency | 232 ± 79 | 231 ± 76 | 232 ± 83 | 0.96 |
| NREM (%) | 91 ± 3 | 91 ± 3 | 91 ± 3 | 0.75 |
| REM (%) | 9 ± 3 | 9 ± 3 | 9 ± 3 | 0.75 |
| AHI | 47 ± 24 | 46 ± 22 | 49 ± 27 | 0.60 |
| REM AHI | 54 ± 26 | 54 ± 26 | 55 ± 27 | 0.89 |
| Arousal index | 45 ± 17 | 46 ± 13 | 46 ± 20 | 0.95 |
| Oxygen desaturation index | 44 (29, 65) | 46 (32, 66) | 43 (29, 82) | 0.83 |
| Mean SaO2 | 92 ± 3 | 92 ± 2 | 91 ± 3 | 0.39 |
| Lowest SaO2 | 80 (71, 83) | 80 (72, 83) | 79 (69, 83) | 0.58 |
| TST90 (min) | 77 (34, 137) | 74 (29, 114) | 81 (36, 166) | 0.53 |
| Severity of OSA (%) | ||||
| 15 ≤ AHI < 30 | 18 (24%) | 8 (22%) | 10 (27%) | |
| AHI ≥ 30 | 56 (76%) | 29 (78%) | 27 (73%) | 0.59 |
| All OSA Patients (n = 74) | OSA SCGroup (n = 37) | OSA MDGroup (n = 37) | p Value | |
|---|---|---|---|---|
| Nocturnal Symptoms | ||||
| Snoring | 74 (100%) | 37 (100%) | 37 (100%) | 1 |
| Witnessed apneas | 73 (99%) | 36 (97%) | 37 (100%) | 0.31 |
| Frequent awakenings | 39 (53%) | 15 (41%) | 24 (65%) | 0.04 |
| Nocturia | 67 (91%) | 33 (89%) | 34 (92%) | 0.69 |
| Diurnal symptoms | ||||
| ESS score | 11 ± 5 | 12 ± 5 | 11 ± 5 | 0.43 |
| ESS > 10 | 43 (58%) | 23 (62%) | 20 (54%) | 0.48 |
| Morning headache | 51 (69%) | 25 (68%) | 26 (70%) | 0.80 |
| Driving problems | 1 (1%) | 0 (0%) | 1 (3%) | 0.31 |
| BDI score | 8 (3, 14) | 5 (3, 18) | 9 (5, 12) | 0.25 |
| BDI ≥ 10 | 25 (39%) | 10 (31%) | 15 (47%) | 0.20 |
| Variable | B | S.E. | p-Value | OR (95% CI) |
|---|---|---|---|---|
| Females vs. males | −0.70 | 1.024 | 0.945 | 0.932 (0.125–26.036) |
| Age (years) | 0.006 | 0.036 | 0.870 | 1.006 (0.938–1.079) |
| Baseline BMI (kg/m2) | 0.094 | 0.057 | 0.101 | 1.099 (0.982–1.229) |
| Currently smoking vs. never/formerly smoking | −1.589 | 0.811 | 0.050 | 0.204 (0.042–1.001) |
| Baseline ESS score > 10 | 1.047 | 0.694 | 0.131 | 2.850 (0.732–11.098) |
| Baseline BDI score ≥ 10 | −1.649 | 0.816 | 0.043 | 0.192 (0.039–0.951) |
| Arterial hypertension | 1.037 | 0.778 | 0.183 | 2.821 (0.614–12.968) |
| Cardiovascular disease | −1.103 | 0.813 | 0.175 | 0.332 (0.067–1.634) |
| Type 2 diabetes | 0.372 | 0.937 | 0.691 | 1.451 (0.231–9.109) |
| COPD | −0.655 | 0.917 | 0.475 | 0.519 (0.086–3.133) |
| MDG vs. SCG | 1.697 | 0.797 | 0.033 | 5.458 (1.144–26.036) |
| Severe vs. moderate OSA | −0.625 | 0.863 | 0.469 | 0.535 (0.099–2.907) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bouloukaki, I.; Daskalaki, E.; Mavroudi, E.; Moniaki, V.; Schiza, S.E.; Tsiligianni, I. A Dietary and Lifestyle Intervention Improves Treatment Adherence and Clinical Outcomes in Overweight and Obese Patients with Obstructive Sleep Apnea: A Randomized, Controlled Trial. Life 2023, 13, 1755. https://doi.org/10.3390/life13081755
Bouloukaki I, Daskalaki E, Mavroudi E, Moniaki V, Schiza SE, Tsiligianni I. A Dietary and Lifestyle Intervention Improves Treatment Adherence and Clinical Outcomes in Overweight and Obese Patients with Obstructive Sleep Apnea: A Randomized, Controlled Trial. Life. 2023; 13(8):1755. https://doi.org/10.3390/life13081755
Chicago/Turabian StyleBouloukaki, Izolde, Eleni Daskalaki, Eleni Mavroudi, Violeta Moniaki, Sophia E. Schiza, and Ioanna Tsiligianni. 2023. "A Dietary and Lifestyle Intervention Improves Treatment Adherence and Clinical Outcomes in Overweight and Obese Patients with Obstructive Sleep Apnea: A Randomized, Controlled Trial" Life 13, no. 8: 1755. https://doi.org/10.3390/life13081755
APA StyleBouloukaki, I., Daskalaki, E., Mavroudi, E., Moniaki, V., Schiza, S. E., & Tsiligianni, I. (2023). A Dietary and Lifestyle Intervention Improves Treatment Adherence and Clinical Outcomes in Overweight and Obese Patients with Obstructive Sleep Apnea: A Randomized, Controlled Trial. Life, 13(8), 1755. https://doi.org/10.3390/life13081755