Diagnostic Value of Initial Chest CT Findings for the Need of ICU Treatment/Intubation in Patients with COVID-19

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Population
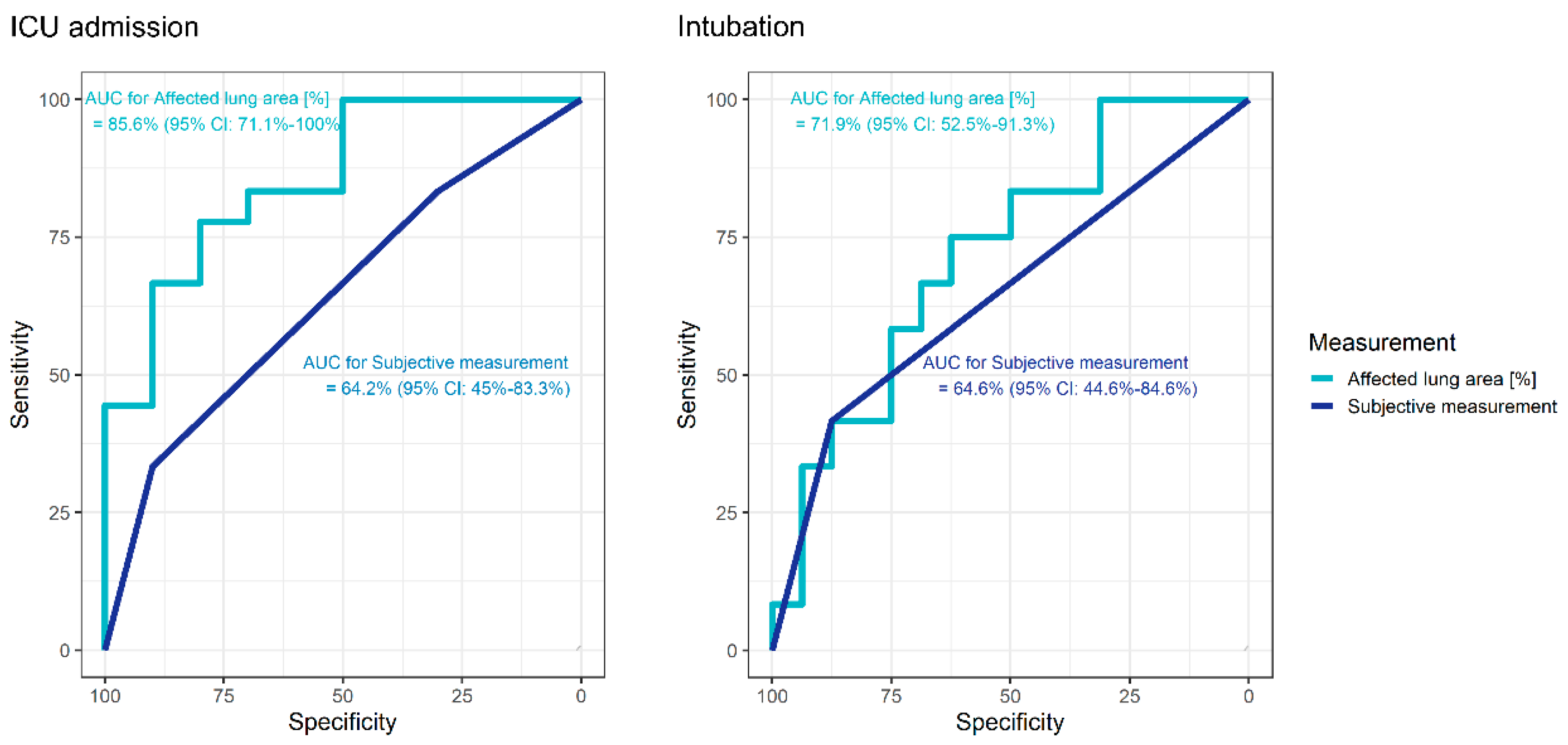
3.2. Subjective Estimation of Pulmonary Involvement
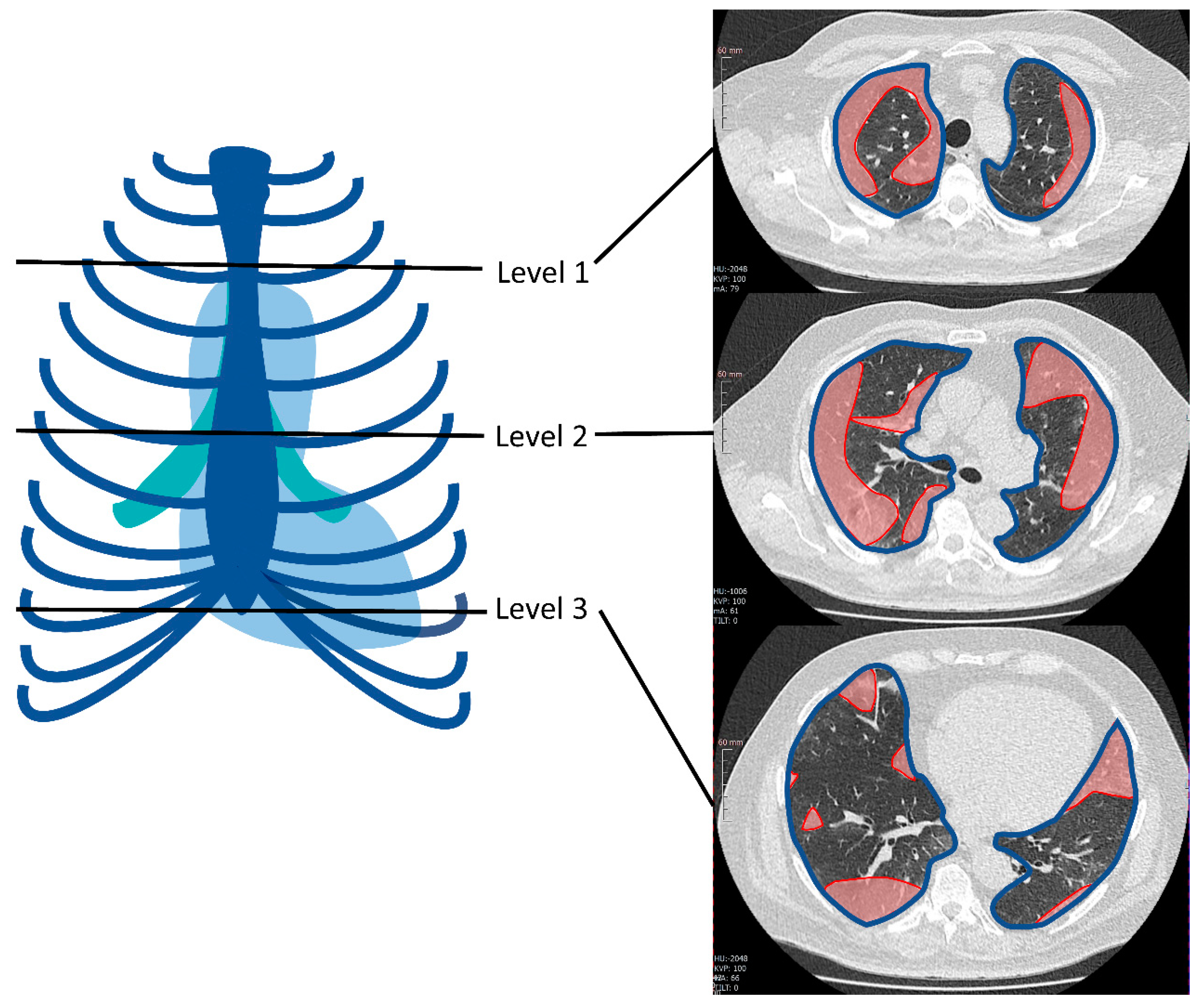
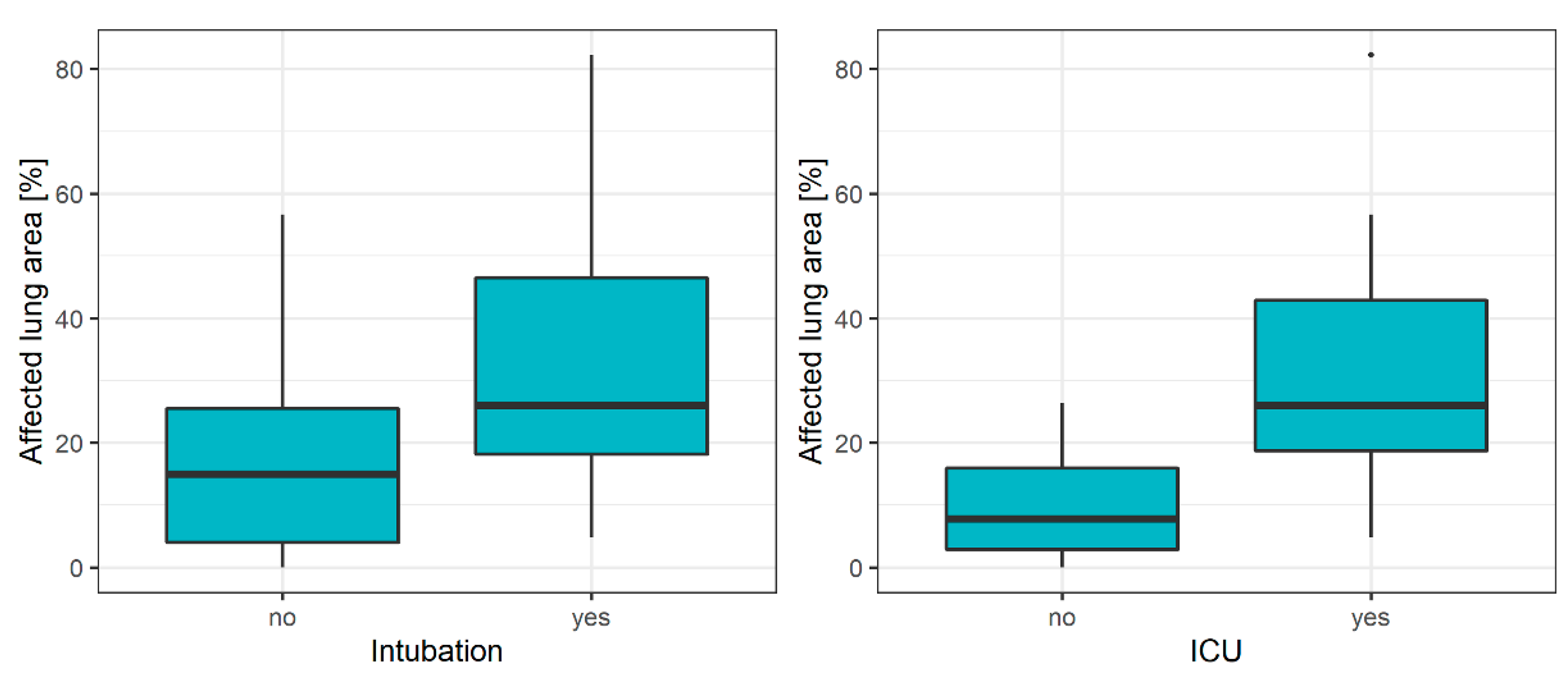
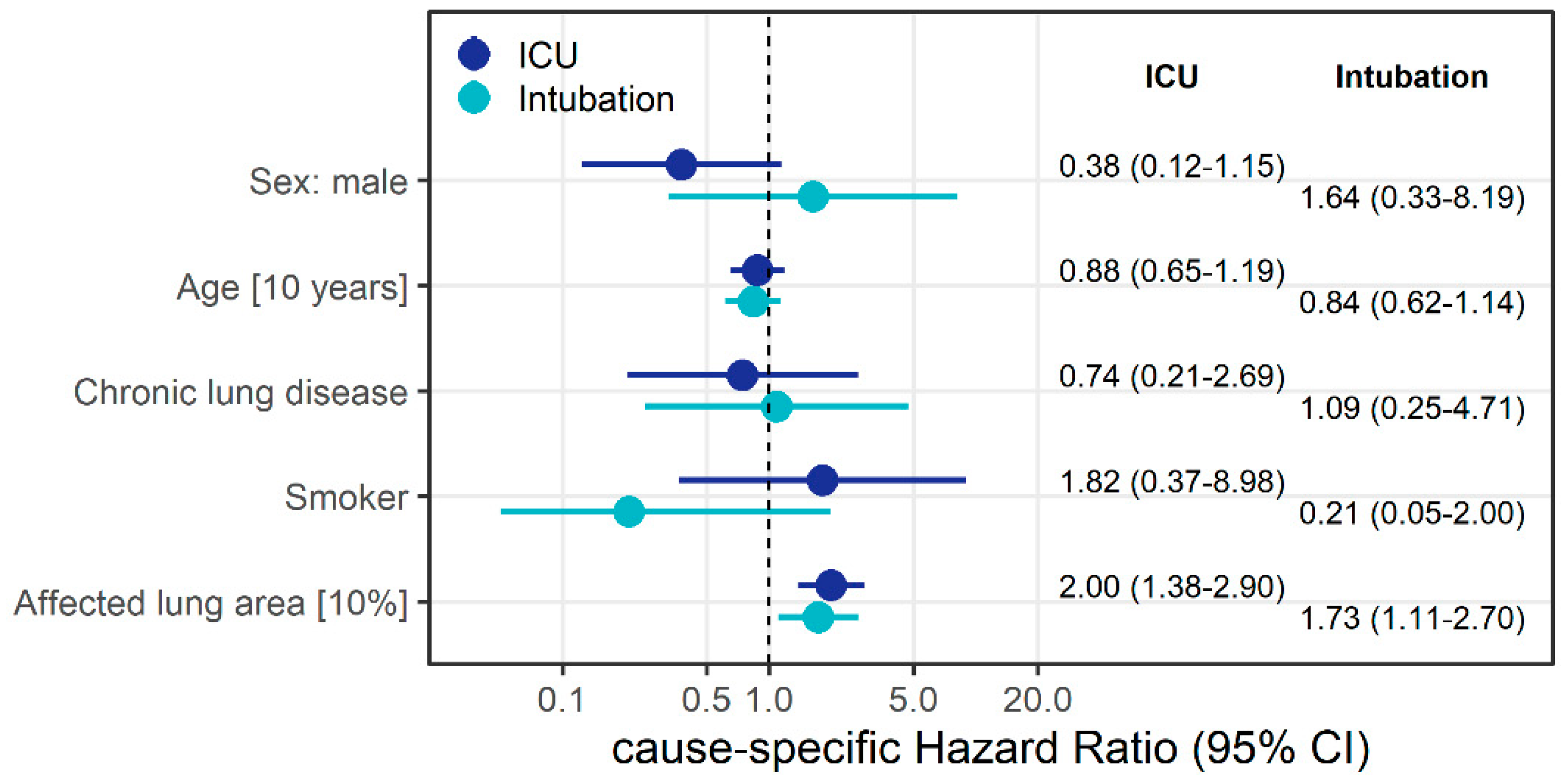
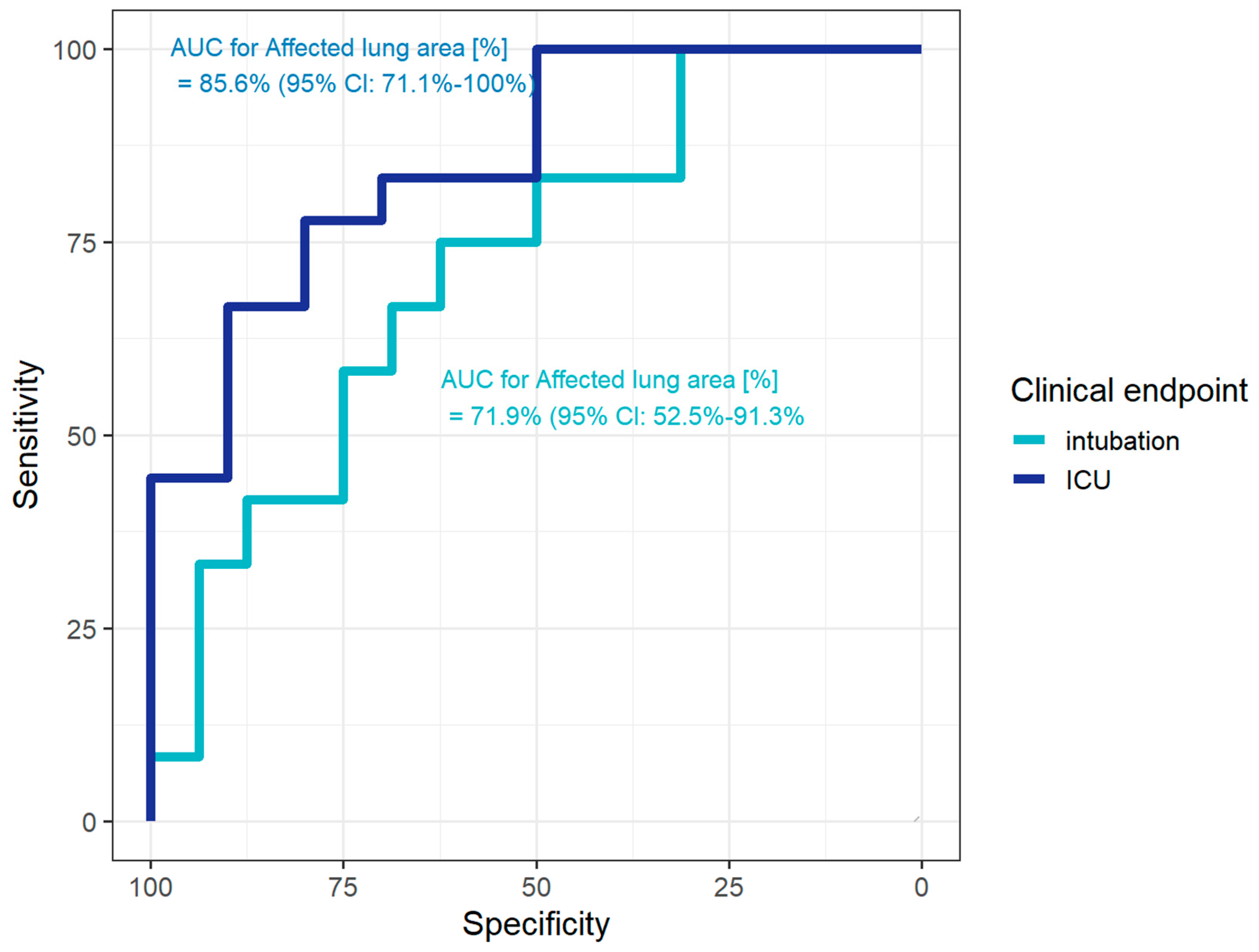
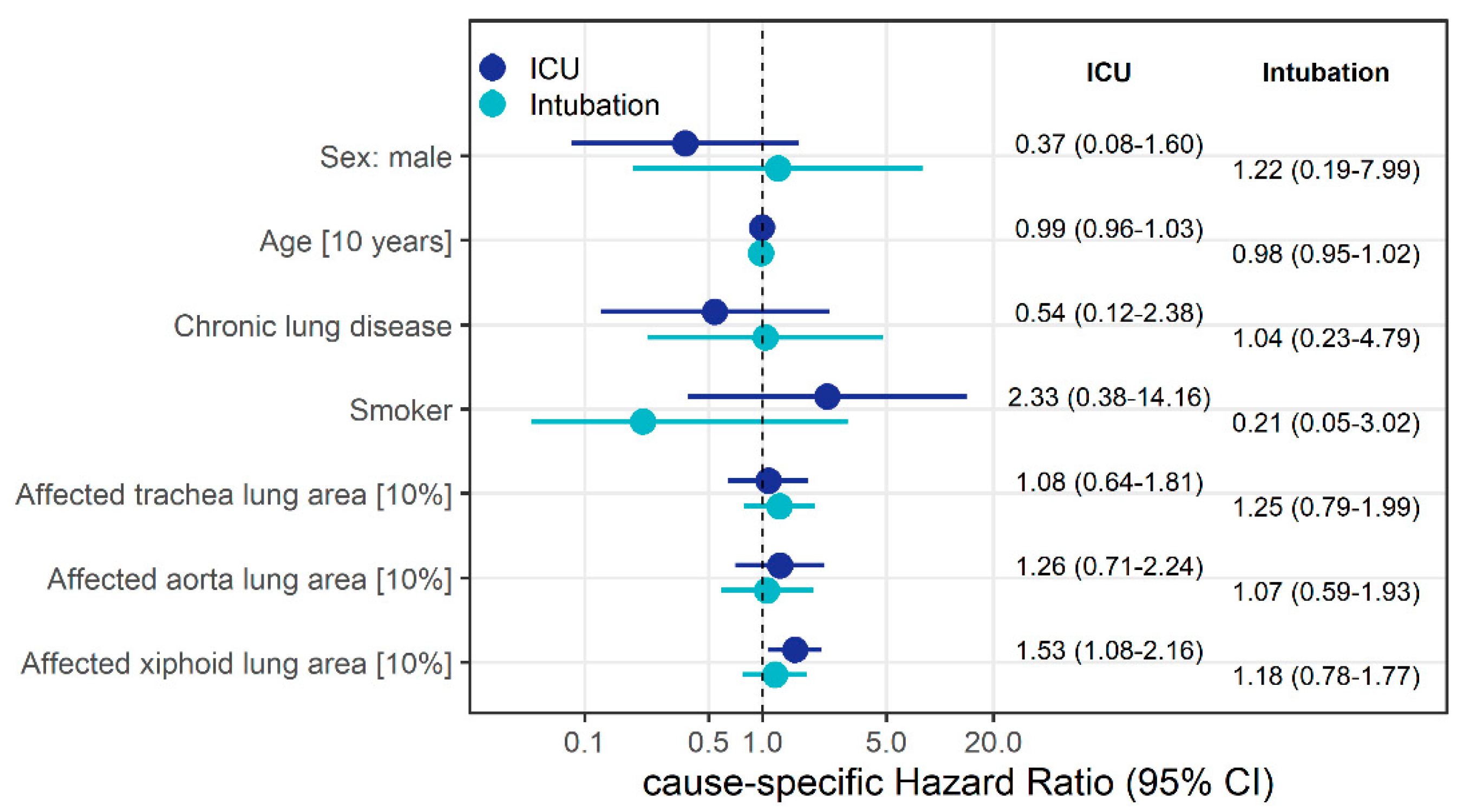
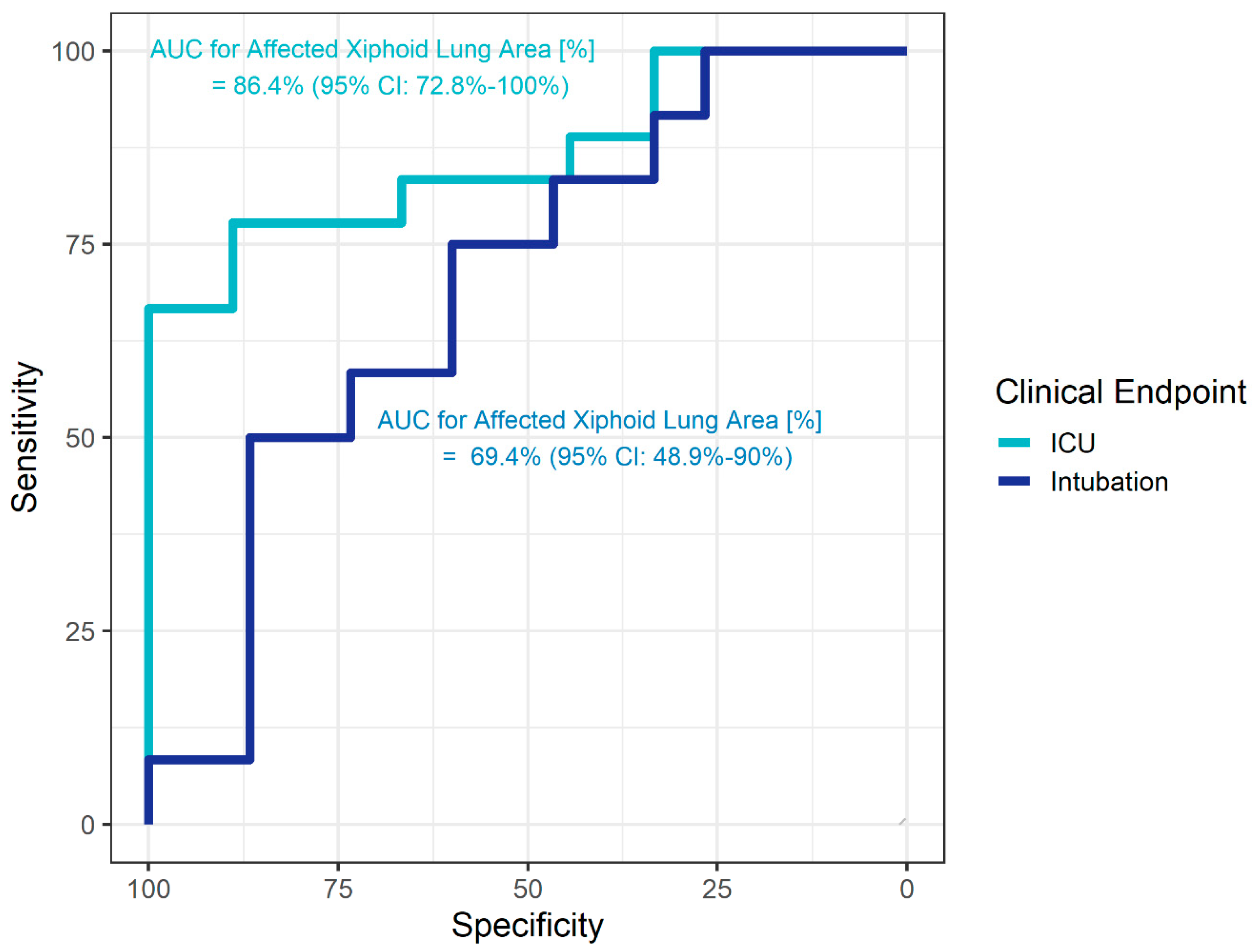
3.3. Semi-Quantitative Measurement of Pulmonary Involvement
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A


References
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological Findings from 81 Patients with Covid-19 Pneumonia in Wuhan, China: A Descriptive Study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Wu, Y.C.; Chen, C.S.; Chan, Y.J. Overview of the 2019 Novel Coronavirus (2019-nCoV): The Pathogen of Severe Specific Contagious Pneumonia (SSCP). J. Chin. Med. Assoc. 2020. [Google Scholar] [CrossRef]
- WHO. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19); World Health Organization (WHO): Geneva, Switzerland, 2020. [Google Scholar]
- RKI—Robert Koch Institut. Sars-Cov-2 Steckbrief Zur Coronavirus-Krankheit-2019 (Covid-19). Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Steckbrief.html#doc13776792bodyText1 (accessed on 13 April 2020).
- Huang, L.; Han, R.; Ai, T.; Yu, P.; Kang, H.; Tao, Q.; Xia, L. Serial Quantitative Chest CT Assessment of COVID-19: Deep-Learning Approach. Radiol. Cardiothorac. Imaging 2020, 2, e200075. [Google Scholar] [CrossRef] [Green Version]
- Phua, J.; Weng, L.; Ling, L.; Egi, M.; Lim, C.-M.; Divatia, J.V.; Shrestha, B.R.; Arabi, Y.M.; Ng, J.; Gomersall, C.D.; et al. Intensive care management of coronavirus disease 2019 (COVID-19): Challenges and recommendations. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef]
- Chen, Z.; Fan, H.; Cai, J.; Li, Y.; Wu, B.; Hou, Y.; Xu, S.; Zhou, F.; Liu, Y.; Xuan, W.; et al. High-resolution computed tomography manifestations of COVID-19 infections in patients of different ages. Eur. J. Radiol. 2020, 126, 108972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombi, D.; Bodini, F.C.; Petrini, M.; Maffi, G.; Morelli, N.; Milanese, G.; Silva, M.; Sverzellati, N.P.; Michieletti, E. Well-aerated Lung on Admitting Chest CT to Predict Adverse Outcome in COVID-19 Pneumonia. Radiology 2020, 201433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bong, C.L.; Brasher, C.; Chikumba, E.; McDougall, R.; Mellin-Olsen, J.; Enright, A. The COVID-19 Pandemic: Effects on Low- and Middle-Income Countries. Anesth. Analg. 2020, 131, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Hamper, C.M.; Fleckenstein, F.N.; Büttner, L.; Hamm, B.; Thieme, N.; Thiess, H.-M.; Scholz, O.; Döllinger, F.; Böning, G. Submillisievert Chest-CT in patients with COVID-19- experiences of a German level I center. Eur. J. Radiol. Open 2020, 100283. [Google Scholar] [CrossRef]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.A.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- R-Core-Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 25 April 2020).
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinformatics 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Therneau, T. A Package for Survival Analysis in S_. version 2.38. Available online: https://CRAN.R-project.org/package=survival (accessed on 25 April 2020).
- Kanne, J.P. Chest CT Findings in 2019 Novel Coronavirus (2019-nCoV) Infections from Wuhan, China: Key Points for the Radiologist. Radiology 2020, 295, 16–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology 2020, 200463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- WHO. Laboratory Testing for 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Dietz, W.; Santos-Burgoa, C. Obesity and its Implications for COVID-19 Mortality. Obesity (Silver Spring) 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mossa-Basha, M.; Meltzer, C.C.; Kim, D.C.; Tuite, M.J.; Kolli, K.P.; Tan, B.S. Radiology Department Preparedness for COVID-19: Radiology Scientific Expert Panel. Radiology 2020, 200988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients without ICU Admission (n = 10) | Patients Requiring ICU Admission (n = 18) | Patients without Intubation (n = 16) | Patients with Intubation (n = 12) | Total (n = 28) | |
|---|---|---|---|---|---|
| Sex | |||||
| Female | 2 (20.0%) | 7 (38.9%) | 6 (37.5%) | 3 (25.0%) | 9 (32.1%) |
| Male | 8 (80.0%) | 11 (61.1%) | 10 (62.5%) | 9 (75.0%) | 19 (67.9%) |
| Age (median, IQR) | 65.9 (54.0–71.5) | 58.2 (39.6–74.9) | 65.9 (53.9–72.4) | 56.2 (34.8–68.0) | 61.0 (49.1–72.0) |
| Comorbidities | |||||
| Diabetes | 3 (30.0%) | 3 (16.7%) | 3 (18.8%) | 3 (25.0%) | 6 (21.4%) |
| Smoking | 3 (30.0%) | 3 (16.7%) | 5 (31.2%) | 1 (8.3%) | 6 (21.4%) |
| Alcohol abuse | 2 (20.0%) | 0 (0.0%) | 2 (12.5%) | 0 (0.0%) | 2 (7.1%) |
| Hypertension | 5 (50.0%) | 9 (50.0%) | 6 (37.5%) | 8 (66.7%) | 14 (50.0%) |
| CAD | 1 (10.0%) | 0 (0.0%) | 1 (6.2%) | 0 (0.0%) | 1 (3.6%) |
| Chronic heart failure | 1 (10.0%) | 1 (5.6%) | 1 (6.2%) | 1 (8.3%) | 2 (7.1%) |
| Obesity | 1 (10.0%) | 4 (22.2%) | 1 (6.2%) | 4 (33.3%) | 5 (17.9%) |
| Chronic lung disease | 5 (50.0%) | 10 (55.6%) | 9 (56.2%) | 6 (50.0%) | 15 (53.6%) |
| Bronchiectasis | 1 (10.0%) | 3 (16.7%) | 2 (12.5%) | 2 (16.7%) | 4 (14.3%) |
| Emphysema | 4 (40.0%) | 5 (27.8%) | 6 (37.5%) | 3 (25.0%) | 9 (32.1%) |
| Fibrosis | 0 (0.0%) | 2 (11.1%) | 1 (6.2%) | 1 (8.3%) | 2 (7.1%) |
| Symptoms | |||||
| Weakness | 7 (70.0%) | 10 (55.6%) | 9 (56.2%) | 8 (66.7%) | 17 (60.7%) |
| Limb pain | 3 (30.0%) | 8 (44.4%) | 5 (31.2%) | 6 (50.0%) | 11 (39.3%) |
| Fever | 5 (50.0%) | 15 (83.3%) | 9 (56.2%) | 11 (91.7%) | 20 (71.4%) |
| Cough | 8 (80.0%) | 12 (66.7%) | 11 (68.8%) | 9 (75.0%) | 20 (71.4%) |
| Dyspnea | 7 (70.0%) | 14 (77.8%) | 10 (62.5%) | 11 (91.7%) | 21 (75.0%) |
| Abdominal symptoms 1 | 1 (10.0%) | 5 (27.8%) | 2 (12.5%) | 4 (33.3%) | 6 (21.4%) |
| Cardiac symptoms | 3 (30.0%) | 2 (11.1%) | 4 (25.0%) | 1 (8.3%) | 5 (17.9%) |
| Type of ventilation | |||||
| No | 4 (40.0%) | 0 (0.0%) | 4 (25.0%) | 0 (0.0%) | 4 (14.3%) |
| Oxygen | 6 (60.0%) | 0 (0.0%) | 6 (37.5%) | 0 (0.0%) | 6 (21.4%) |
| Noninvasive 2 | 0 (0.0%) | 6 (33.3%) | 6 (37.5%) | 0 (0.0%) | 6 (21.4%) |
| Invasive 3 | 0 (0.0%) | 8 (44.4%) | 0 (0.0%) | 8 (66.7%) | 8 (28.6%) |
| ECMO | 0 (0.0%) | 4 (22.2%) | 4 (33.3%) | 4 (14.3%) | |
| Patients without ICU Admission (n = 10) | Patients Requiring ICU Admission (n = 18) | Patients without Intubation (n = 16) | Patients with Intubation (n = 12) | Total (n = 28) | |
|---|---|---|---|---|---|
| Subjective estimate of extent of pulmonary involvement | |||||
| None | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Minor | 3 (30.0%) | 3 (16.7%) | 4 (25.0%) | 2 (16.7%) | 6 (21.4%) |
| Moderate | 6 (60.0%) | 9 (50.0%) | 10 (62.5%) | 5 (41.7%) | 15 (53.6%) |
| Major | 1 (10.0%) | 6 (33.3%) | 2 (12.5%) | 5 (41.7%) | 7 (25.0%) |
| Semi-quantitative measurement of pulmonary involvement | |||||
| Aortic arch (%) | 5.4 (2.7–14.5) | 13.2 (2.2–42.9) | 6.7 (1.9–15.6) | 22.3 (3.4–43.5) | 11.3 (2.1–32.9) |
| Tracheal bifurcation (%) | 2.9 (2.1–10.8) | 18.2 (10.6–48.6) | 8.0 (2.6–18.3) | 18.7 (8.9–49.6 | 12.0 (2.7–34.8) |
| Inferior end of the xiphoid (%) | 12.8 (2.7–21.4) | 35.1 (26.5–51.0) | 21.4 (7.2–33.7) | 34.5 (25.1–46.2) | 26.6 (10.9–37.5) |
| Affected lung area (%) | 7.8 (2.8–15.9) | 26.0 (18.7–42.9) | 15.0 (4.0–25.5) | 26.0 (18.2–46.5) | 20.4 (6.1–32.6) |
| CT findings | |||||
| Consolidations | |||||
| None | 3 (30%) | 1(5.6%) | 3 (18.8%) | 1 (8.3%) | 4 (14.3%) |
| Minor 1 | 4 (40.0%) | 1 (5.6%) | 7 (43.8%) | 4 (33.3%) | 11 (39.3%) |
| Moderate 1 | 2 (20.0%) | 7 (38.9%) | 5 (31.3%) | 4 (44.4%) | 9 (32.1%) |
| Major 1 | 1 (10.0%) | 3 (16.7%) | 1 (6.3%) | 3 (25.0%) | 4 (14.3%) |
| Ground-glass opacities | |||||
| None | 0 (0.0%) | 2 (11.1%) | 1 (6.3%) | 1 (8.3%) | 2 (7.1%) |
| Minor 1 | 7 (53.8%) | 6 (46.2%) | 8 (50.0%) | 5 (38.5%) | 13 (100.0%) |
| Moderate | 3 (30.0%) | 9 (50.0%) | 7 (43.8%) | 5 (41.7%) | 12 (42.9%) |
| Major | 0 (0.0%) | 1 (5.6%) | 0 (0.0%) | 1 (8.3%) | 1 (3.6%) |
| Pleural effusions | |||||
| None | 9 (90.0%) | 15 (83.3%) | 14 (87.5%) | 10 (83.3%) | 24 (85.7%) |
| Minor 1 | 0 (0.0%) | 2 (11.1%) | 1 (6.3%) | 1 (8.3%) | 2 (7.1%) |
| Moderate 1 | 1 (10.0%) | 0 (0.0%) | 1 (6.3%) | 0 (0.0%) | 1 (3.6%) |
| Major 1 | 0 (0.0%) | 1 (5.6%) | 0 (0.0%) | 1 (8.3%) | 1 (3.6%) |
| Lymphadenopathy | 2 (20.0%) | 2 (11.1%) | 3 (18.8%) | 1 (8.3%) | 4 (14.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Büttner, L.; Aigner, A.; Fleckenstein, F.N.; Hamper, C.M.; Jonczyk, M.; Hamm, B.; Scholz, O.; Böning, G. Diagnostic Value of Initial Chest CT Findings for the Need of ICU Treatment/Intubation in Patients with COVID-19. Diagnostics 2020, 10, 929. https://doi.org/10.3390/diagnostics10110929
Büttner L, Aigner A, Fleckenstein FN, Hamper CM, Jonczyk M, Hamm B, Scholz O, Böning G. Diagnostic Value of Initial Chest CT Findings for the Need of ICU Treatment/Intubation in Patients with COVID-19. Diagnostics. 2020; 10(11):929. https://doi.org/10.3390/diagnostics10110929
Chicago/Turabian StyleBüttner, Laura, Annette Aigner, Florian Nima Fleckenstein, Christina Maria Hamper, Martin Jonczyk, Bernd Hamm, Oriane Scholz, and Georg Böning. 2020. "Diagnostic Value of Initial Chest CT Findings for the Need of ICU Treatment/Intubation in Patients with COVID-19" Diagnostics 10, no. 11: 929. https://doi.org/10.3390/diagnostics10110929
APA StyleBüttner, L., Aigner, A., Fleckenstein, F. N., Hamper, C. M., Jonczyk, M., Hamm, B., Scholz, O., & Böning, G. (2020). Diagnostic Value of Initial Chest CT Findings for the Need of ICU Treatment/Intubation in Patients with COVID-19. Diagnostics, 10(11), 929. https://doi.org/10.3390/diagnostics10110929