Detection and Diagnosis of Breast Cancer Using Artificial Intelligence Based Assessment of Maximum Intensity Projection Dynamic Contrast-Enhanced Magnetic Resonance Images

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. DCE Breast MRI Examinations
2.3. Data Set
2.4. AI System
2.5. Readout
2.6. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Kolb, T.M.; Lichy, J.; Newhouse, J.H. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology 2002, 225, 165–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, N.H.; Borel Rinkes, I.H.; Zuithoff, N.P.; Mali, W.P.; Moons, K.G.; Peeters, P.H. Meta-analysis of MR imaging in the diagnosis of breast lesions. Radiology 2008, 246, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Spick, C.; Szolar, D.H.M.; Preidler, K.W.; Tillich, M.; Reittner, P.; Baltzer, P.A. Breast MRI used as a problem-solving tool reliably excludes malignancy. Eur. J. Radiol. 2015, 84, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Saslow, D.; Boetes, C.; Burke, W.; Harms, S.; Leach, M.O.; Lehman, C.D.; Morris, E.; Pisano, E.; Schnall, M.; Sener, S.; et al. American Cancer Society guidelines for breast screening with MRI as an adjunct mammography. CA Cancer J. Clin. 2007, 57, 75–89. [Google Scholar] [CrossRef] [Green Version]
- Machida, Y.; Shimauchi, A.; Kanemaki, Y.; Igarashi, T.; Harada, M.; Fukuma, E. Feasibility and potential limitations of abbreviated breast MRI: an observer study using an enriched cohort. Breast Cancer 2017, 24, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, C.K.; Schrading, S.; Strobel, K.; Schild, H.H.; Hilgers, R.D.; Bieling, H.B. Abbreviated breast magnetic resonance imaging (MRI): first postcontrast subtracted images and maximum-intensity projection-a novel approach to breast cancer screening with MRI. J. Clin. Oncol. 2014, 32, 2304–2310. [Google Scholar] [CrossRef]
- Mendelson, E.B. Artificial intelligence in breast imaging: Potentials and limitations. AJR Am. J. Roentgenol. 2019, 212, 293–299. [Google Scholar] [CrossRef]
- Le, E.P.V.; Wang, Y.; Huang, Y.; Hickman, S.; Gilbert, F.J. Artificial intelligence in breast imaging. Clin. Radiol. 2019, 74, 357–366. [Google Scholar] [CrossRef]
- Fujioka, T.; Mori, M.; Kubota, K.; Kikuchi, Y.; Katsuta, L.; Adachi, M.; Oda, G.; Nakagawa, T.; Kitazume, Y.; Tateishi, U. Breast Ultrasound Image Synthesis using Deep Convolutional Generative Adversarial Networks. Diagnostics (Basel) 2019, 6, 176. [Google Scholar] [CrossRef] [Green Version]
- Yi, X.; Walia, E.; Babyn, P. Generative adversarial network in medical imaging: A review. Med. Image Anal. 2019, 58, 101552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujioka, T.; Kubota, K.; Mori, M.; Kikuchi, Y.; Katsuta, L.; Kasahara, M.; Oda, G.; Ishiba, T.; Nakagawa, T.; Tateishi, U. Distinction between benign and malignant breast masses at breast ultrasound using deep learning method with convolutional neural network. Jpn. J. Radiol. 2019, 37, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.; Kim, B.; Lee, I.; Yoo, M.; Lee, J.; Ham, S.; Woo, O.; Kang, J. Detection of masses in mammograms using a one-stage object detector based on a deep convolutional neural network. PLoS ONE 2018, 13, e0203355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardezi, S.J.S.; Elazab, A.; Lei, B.; Wang, T. Breast Cancer Detection and Diagnosis Using Mammographic Data: Systematic Review. J. Med. Internet Res. 2019, 21, e14464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheth, D.; Giger, M.L. Artificial intelligence in the interpretation of breast cancer on MRI. J. Magn. Reson. Imaging. 2019. [Google Scholar] [CrossRef] [PubMed]
- Reig, B.; Heacock, L.; Geras, K.J.; Moy, L. Machine learning in breast MRI. J. Magn. Reson. Imaging. 2019. [Google Scholar] [CrossRef]
- Herent, P.; Schmauch, B.; Jehanno, P.; Dehaene, O.; Saillard, C.; Balleyguier, C.; Arfi-Rouche, J.; Jégou, S. Detection and characterization of MRI breast lesions using deep learning. Diagn. Interv. Imaging. 2019, 100, 219–225. [Google Scholar] [CrossRef]
- Antropova, N.; Abe, H.; Giger, M.L. Use of clinical MRI maximum intensity projections for improved breast lesion classification with deep convolutional neural networks. J. Med. Imaging (Bellingham) 2018, 5, 014503. [Google Scholar] [CrossRef]
- Truhn, D.; Schrading, S.; Haarburger, C.; Schneider, H.; Merhof, D.; Kuhl, C. Radiomic versus Convolutional Neural Networks Analysis for Classification of Contrast-enhancing Lesions at Multiparametric Breast MRI. Radiology. 2019, 290, 290–297. [Google Scholar] [CrossRef]
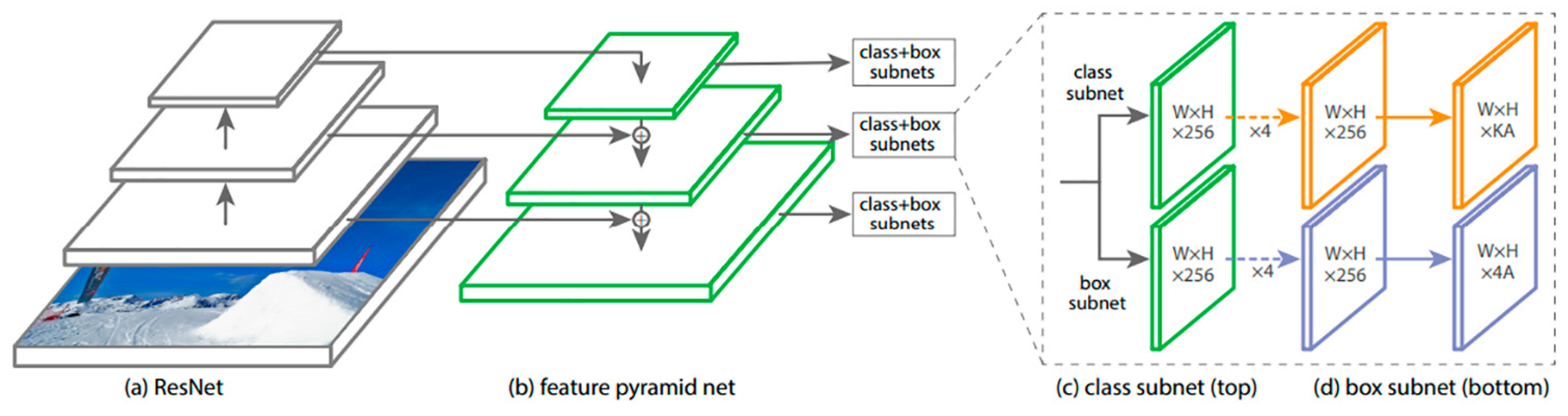
- Lin, T.Y.; Goyal, P.; Girshick, R.; He, K.; Dollár, P. Focal Loss for Dense Object Detection. ICCV 2017, 2980–2988. [Google Scholar] [CrossRef] [Green Version]
- Lin, T.Y.; Dolla, P.; Girshick, R.; He, K.; Hariharan, B.; Belongie, S. Feature pyramid networks for object detection. 2016. Available online: https://arxiv.org/abs/1612.03144 (accessed on 16 April 2020).
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. 2016, 770–778. Available online: https://arxiv.org/abs/1512.03385 (accessed on 16 April 2020).
- D’Orsi, C.; Sickles, E.; Mendelson, E.; Morris, E. Breast Imaging Reporting And Data System, 5th ed.; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. ImageNet large scale visual recognition challenge. Int. J. Comp. Sci. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.; Yun, J.; Cho, Y.; Shin, K.; Jang, R.; Bae, H.J.; Kim, N. Deep learning in medical imaging. Neurospine 2019, 16, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Fanizzi, A.; Basile, T.M.A.; Losurdo, L.; Bellotti, R.; Bottigli, U.; Dentamaro, R.; Didonna, V.; Fausto, A.; Massafra, R.; Moschetta, M.; et al. A machine learning approach on multiscale texture analysis for breast microcalcification diagnosis. BMC Bioinform. 2020, 21, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berrar, D. Cross-validation. Encyclopedia of Bioinformatics and Computational Biology. 2019, pp. 542–545. Available online: https://www.researchgate.net/profile/Daniel_Berrar/publication/324701535_Cross-Validation/links/5cb4209c92851c8d22ec4349/Cross-Validation.pdf (accessed on 16 April 2020).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Data | Validation Data | Test Data | |||
|---|---|---|---|---|---|
| Benign (n = 49) | Malignant (n = 135) | Benign (n = 20) | Malignant (n = 45) | Benign (n = 20) | Malignant (n = 52) |
| Fibroadenoma 8 | Ductal Carcinoma In Situ 22 | Fibroadenoma 4 | Ductal Carcinoma In Situ 2 | Fibroadenoma 4 | Ductal Carcinoma In Situ 3 |
| Papilloma 9 | Invasive Ductal Carcinoma 91 | Papilloma 3 | Invasive Ductal Cancer 29 | Papilloma 3 | Invasive Ductal Carcinoma 38 |
| Mastopathy 4 | Mucinous Carcinoma 3 | Mastopathy 3 | Mucinous Carcinoma 2 | Mastopathy 3 | Mucinous Carcinoma 1 |
| Benign Phyllodes Tumor 2 | Invasive Lobular Carcinoma 7 | Non-Specific Benign Lesion 2 | Invasive Lobular Carcinoma 5 | Non-Specific Benign Lesion 2 | Invasive Lobular Carcinoma 1 |
| Non-Specific Benign Lesion 4 | Apocrine Carcinoma 2 | Not Known * 8 | Apocrine Carcinoma 1 | Not Known * 8 | Apocrine Carcinoma 1 |
| Not Known * 22 | Malignant Phyllodes Tumor 1 | Malignant Phyllodes Tumor 1 | Malignant Phyllodes Tumor 2 | ||
| Unclassifiable 9 | Unclassifiable 5 | Unclassifiable 6 | |||
| Normal | Benign | Malignant | ||
|---|---|---|---|---|
| Training Data | Patients (n) | 30 | 49 | 135 |
| Age (years) | 38–72 | 38–74 | 26–86 | |
| Range, Mean ± SD | 52.9 ± 11.1 | 46.3 ± 11.0 | 58.6 ±12.8 | |
| Breasts (n) | 201 a | 88 | 139 | |
| Mass/Non-mass (n) | 77/11 | 114/25 | ||
| Size at MRI (mm) | 3–105 | 6–95 | ||
| Range, Mean ± SD | 14.9 ± 15.0 | 23.6 ± 16.9 | ||
| Validation Data | Test Data (n) | 7 | 20 | 45 |
| Age (years) | 40–54 | 28–79 | 26–78 | |
| Range, Mean ± SD | 46.0 ± 5.6 | 50.0 ± 12.5 | 55.6 ± 13.1 | |
| Breasts (n) | 64 a | 30 | 50 | |
| Mass/Non-mass (n) | 22/8 | 38/12 | ||
| Size at MRI (mm) | 3–62 | 6–123 | ||
| Range, Mean ± SD | 17.5 ± 15.2 | 35.0 ± 26.8 | ||
| Test Data | Patients (n) | 13 | 20 | 52 |
| Age (years) | 21–77 | 20–79 | 30–85 | |
| Range, Mean ± SD | 47.2 ± 12.6 | 47.2 ± 11.1 | 58.3 ±13.6 | |
| Breasts (n) | 92 a | 24 | 54 | |
| Mass/Non-mass (n) | 19/5 | 47/7 | ||
| Size at MRI (mm) | 5–33 | 7–106 | ||
| Range, Mean ± SD | 13.6 ± 8.8 | 25.6 ± 22.0 |
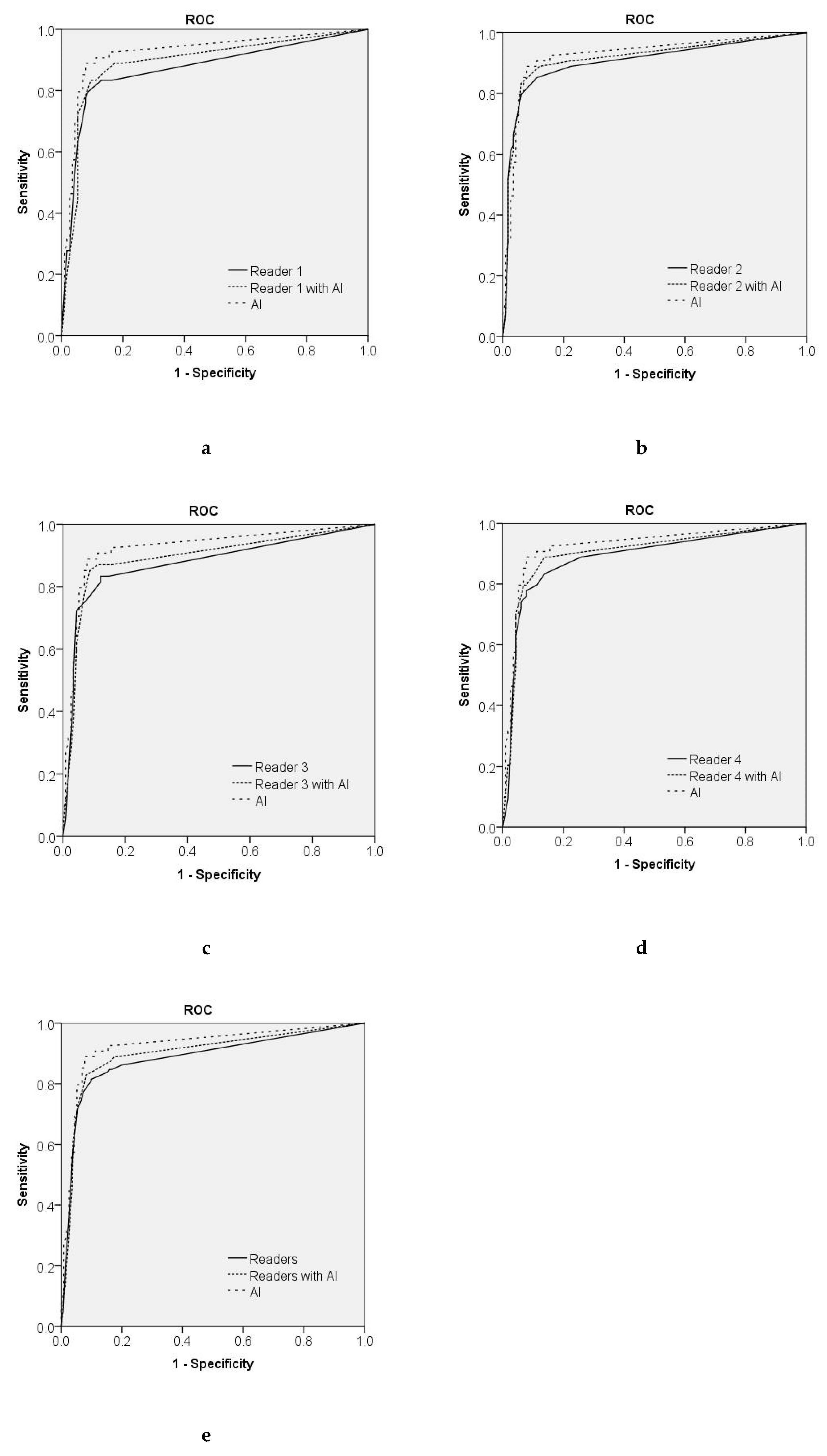
| Sensitivity | Specificity | AUC (95% CI) | |
|---|---|---|---|
| AI | 0.926 | 0.828 | 0.925 (0.878–0.971) |
| Reader 1 | 0.833 | 0.836 | 0.872 (0.811–0.933) |
| Reader 1 with AI system | 0.889 | 0.802 | 0.893 (0.837–0.948) |
| Reader 2 | 0.889 | 0.776 | 0.904 (0.849–0.959) |
| Reader 2 with AI system | 0.907 | 0.759 | 0.915 (0.863–0.967) |
| Reader 3 | 0.833 | 0.853 | 0.876 (0.816–0.936) |
| Reader 3 with AI system | 0.874 | 0.844 | 0.893 (0.847–0.956) |
| Reader 4 | 0.862 | 0.833 | 0.887 (0.829–0.945) |
| Reader 4 with AI system | 0.889 | 0.845 | 0.902 (0.847–0.956) |
| All Human Readers | 0.847 | 0.841 | 0.884 (0.854–0.920) |
| All Human Readers with AI system | 0.889 | 0.823 | 0.899 (0.872–0.929) |
| Reader without AI System | p-Value (vs. AI System) | p-Value (vs. Reader with AI System) |
|---|---|---|
| Reader 1 | 0.038 | 0.203 |
| Reader 2 | 0.414 | 0.200 |
| Reader 3 | 0.076 | 0.393 |
| Reader 4 | 0.143 | 0.203 |
| Readers | 0.002 | 0.039 |
| No | Size (mm)/Mass or Non-Mass | Possibility of Malignancy (%) | Pathology | ||||
|---|---|---|---|---|---|---|---|
| AI | Reader 1 | Reader 2 | Reader 3 | Reader 4 | |||
| False Positive | |||||||
| 1 | 27 mm/mass | 66.2 | 10 | 0 | 0 | 30 | Observation |
| 2 | No findings | 57.9 | 0 | 10 | 0 | 0 | Normal |
| 3 | No findings | 90.0 | 0 | 0 | 1 | 0 | Normal |
| 4 | 19 mm/mass | 99.9 | 80 | 60 | 10 | 90 | Fibroadenoma |
| 5 | 9 mm/mass | 83.5 | 2 | 20 | 0 | 1 | IDP |
| 6 | 9 mm/mass | 97.7 | 60 | 20 | 0 | 10 | Observation |
| 7 | 14 mm/mass | 99.9 | 95 | 40 | 5 | 95 | Fibroadenoma |
| False Negative | |||||||
| 1 | 10 mm/mass | 0 | 0 | 50 | 0 | 90 | IDC |
| 2 | 11 mm/mass | 0 | 0 | 0 | 0 | 0 | IDC |
| 3 | 17 m/non-mass | 0 | 0 | 0 | 0 | 0 | DCIS |
| 4 | 7 mm/mass | 0 | 50 | 10 | 1 | 20 | IDC |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adachi, M.; Fujioka, T.; Mori, M.; Kubota, K.; Kikuchi, Y.; Xiaotong, W.; Oyama, J.; Kimura, K.; Oda, G.; Nakagawa, T.; et al. Detection and Diagnosis of Breast Cancer Using Artificial Intelligence Based Assessment of Maximum Intensity Projection Dynamic Contrast-Enhanced Magnetic Resonance Images. Diagnostics 2020, 10, 330. https://doi.org/10.3390/diagnostics10050330
Adachi M, Fujioka T, Mori M, Kubota K, Kikuchi Y, Xiaotong W, Oyama J, Kimura K, Oda G, Nakagawa T, et al. Detection and Diagnosis of Breast Cancer Using Artificial Intelligence Based Assessment of Maximum Intensity Projection Dynamic Contrast-Enhanced Magnetic Resonance Images. Diagnostics. 2020; 10(5):330. https://doi.org/10.3390/diagnostics10050330
Chicago/Turabian StyleAdachi, Mio, Tomoyuki Fujioka, Mio Mori, Kazunori Kubota, Yuka Kikuchi, Wu Xiaotong, Jun Oyama, Koichiro Kimura, Goshi Oda, Tsuyoshi Nakagawa, and et al. 2020. "Detection and Diagnosis of Breast Cancer Using Artificial Intelligence Based Assessment of Maximum Intensity Projection Dynamic Contrast-Enhanced Magnetic Resonance Images" Diagnostics 10, no. 5: 330. https://doi.org/10.3390/diagnostics10050330
APA StyleAdachi, M., Fujioka, T., Mori, M., Kubota, K., Kikuchi, Y., Xiaotong, W., Oyama, J., Kimura, K., Oda, G., Nakagawa, T., Uetake, H., & Tateishi, U. (2020). Detection and Diagnosis of Breast Cancer Using Artificial Intelligence Based Assessment of Maximum Intensity Projection Dynamic Contrast-Enhanced Magnetic Resonance Images. Diagnostics, 10(5), 330. https://doi.org/10.3390/diagnostics10050330