Budget Impact Analysis of EGFR Mutation Liquid Biopsy for First- and Second-Line Treatment of Metastatic Non-Small Cell Lung Cancer in Greece

Abstract
:1. Introduction
- Liquid biopsy offers a minimally invasive method for molecular diagnostic testing with lower patient burden relative to tissue biopsy.
- Liquid biopsy enables more timely and frequent EGFR mutation assessment due to lower logistical burdens with a blood draw procedure compared to an invasive surgical procedure.
- Liquid biopsy enables all patients with NSCLC the opportunity to undergo EGFR mutation testing for optimal therapy selection.
2. Materials and Methods
2.1. Model Overview
- plasma testing as an alternative to tissue biopsy for all (“plasma test only”);
- primary tissue testing with plasma testing only for patients who are ineligible for tissue biopsy (“combined testing approach”); and
- primary plasma testing for all with reflex of wild-type patients to confirmatory tissue biopsy (“reflex testing approach” per U.S. Food and Drug Administration (FDA)-approved intended use for the cobas® EGFR Mutation Test v2, Roche Molecular Systems, Pleasanton, CA, USA [23]. Due to lower test concordance between plasma and tissue testing, it is recommended that patients who are EGFR mutation negative by plasma undergo confirmatory tissue testing when practicable.)
2.2. Population
2.3. Clinical Inputs
2.4. Cost Inputs
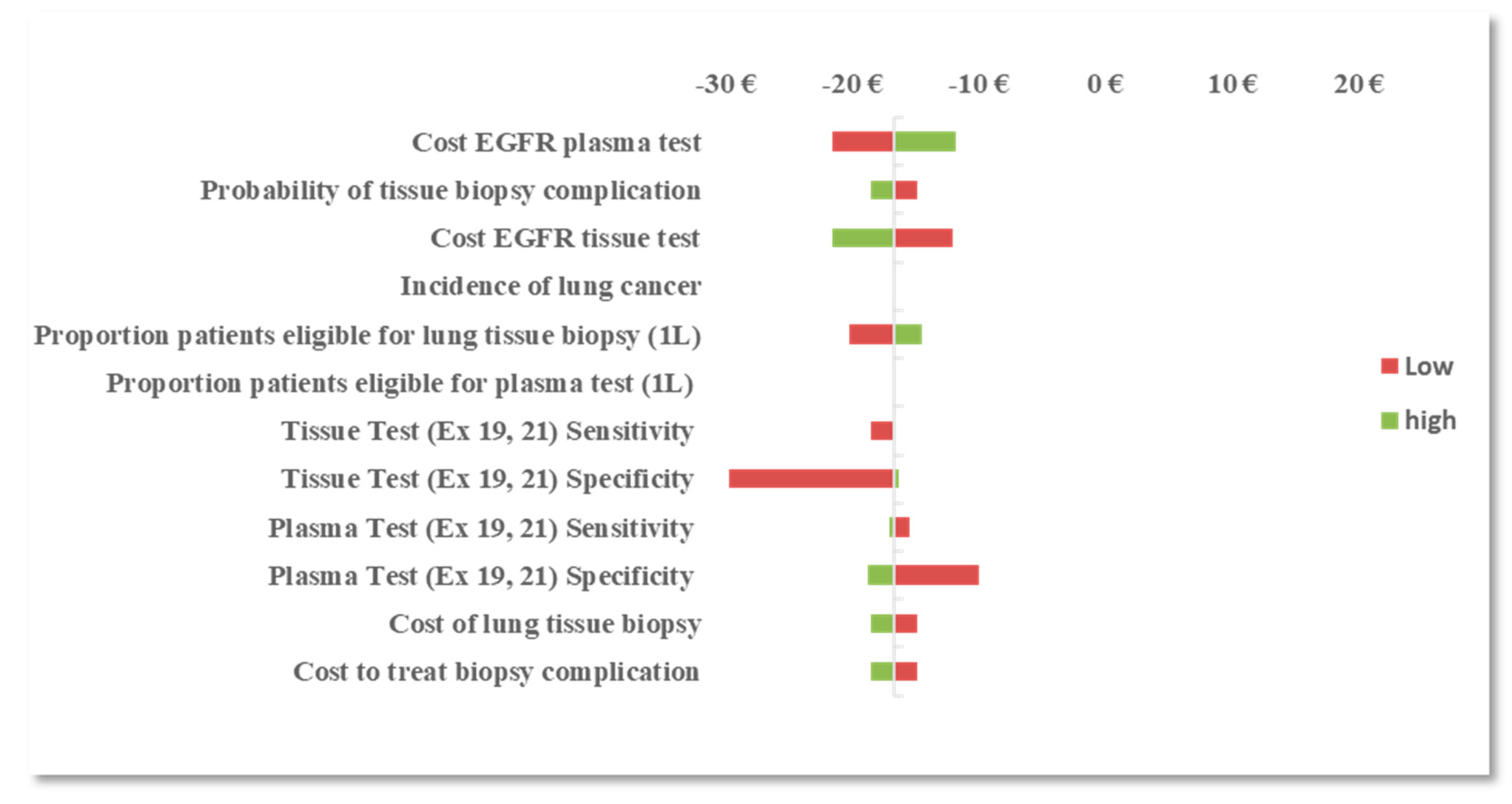
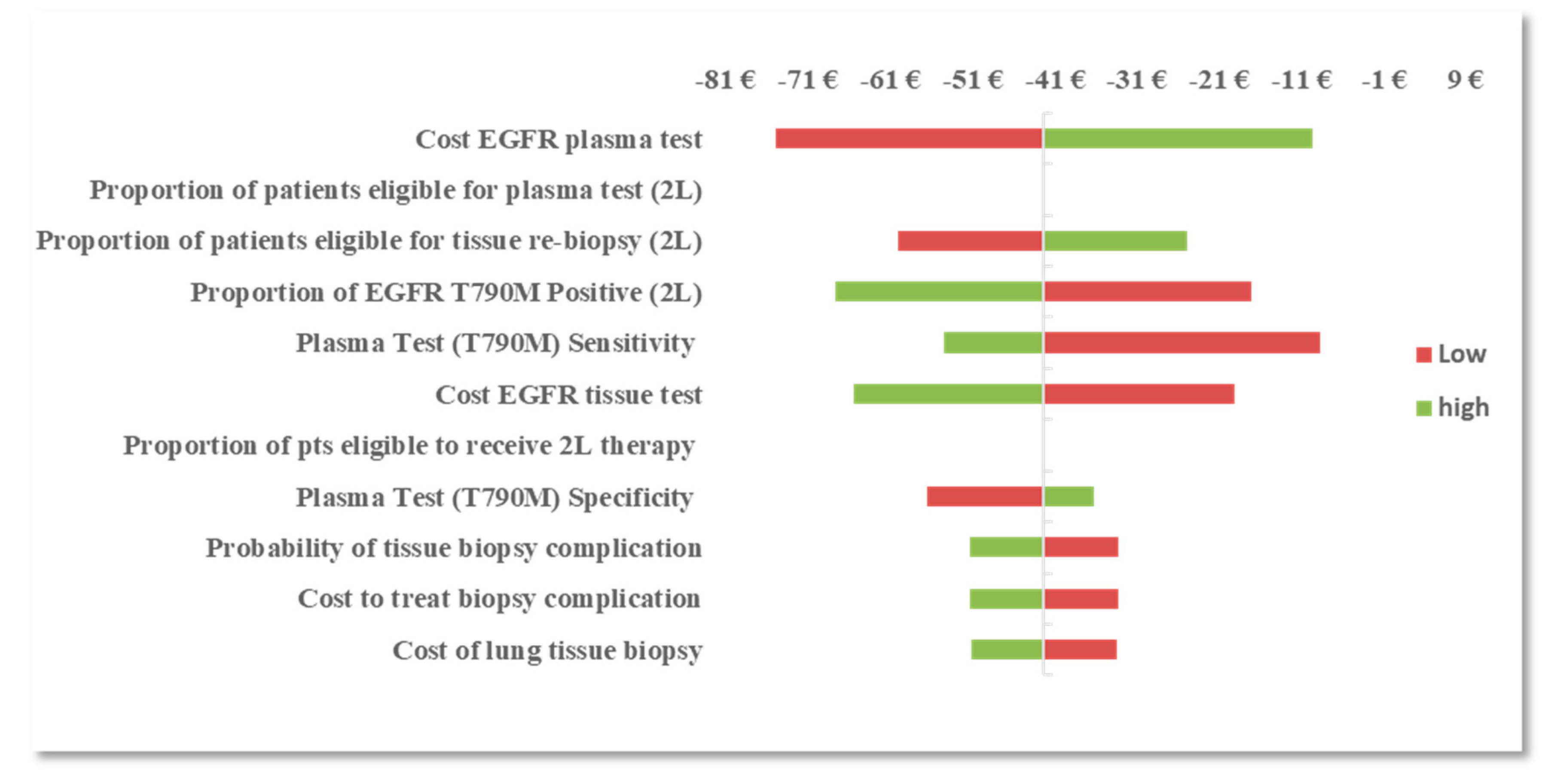
2.5. One-Way Sensitivity Analysis
3. Results
3.1. Base-Case Analysis
3.2. One-Way Sensitivity Analysis
3.3. Scenario Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.; Torre, L.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. Ca J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Didkowska, J.; Wojciechowska, U.; Manczuk, M.; Lobaszewski, J. Lung cancer epidemiology: Contemporary and future challenges worldwide. Ann. Transl. Med. 2016, 4, 150. [Google Scholar] [CrossRef] [Green Version]
- Grapatsas, K.; Leivaditis, V.; Tsilogianni, Z.; Haussmann, E.; Kaplunov, V.; Dahm, M.; Zarogoulidis, P.; Hohenforst-Schmidt, W.; Tsakiridis, K.; Foroulis, C.; et al. Epidemiology, risk factors, symptomatology, TNM classification of non small cell lung cancer. An overview while waiting the 8th TNM classification. Oncomedicine 2017, 2, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Novello, S.; Barlesi, F.; Califano, R.; Cufer, T.; Ekman, S.; Giaj Levra, M.; Kerr, K.; Popat, S.; Reck, M.; Senan, S.; et al. Metastatic non-small-cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v1–v27. [Google Scholar] [CrossRef] [PubMed]
- Syrigos, K.N.; Georgoulias, V.; Zarogoulidis, K.; Makrantonakis, P.; Charpidou, A.; Christodoulou, C. Epidemiological characteristics, EGFR status and management patterns of advanced non-small cell lung cancer patients: The Greek REASON observational registry study. Anticancer Res. 2018, 38, 3735–3744. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-L.; Yuan, J.-Q.; Wang, K.-F.; Fu, X.-H.; Han, X.-R.; Threapleton, D.; Yang, Z.-Y.; Mao, C.; Tang, J.-L. The prevalence of EGFR mutation in patients with non-small cell lung cancer: A systematic review and meta-analysis. Oncotarget 2016, 7, 78985–78993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Spanish Lung Cancer Group in collaboration with Groupe Français de Pneumo-Cancérologie and Associazione Italiana Oncologia Toracica. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicenter, open-label, randomized phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar]
- Zhou, C.; Wu, Y.-L.; Chen, G.; Feng, J.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; Lu, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Chu, D.-T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; Nishiwaki, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Mitsudomi, T.; Morita, S.; Yatabe, Y.; Negoro, S.; Okamoto, I.; Tsurutani, J.; Seto, T.; Satouchi, M.; Tada, H.; Hirashima, T.; et al. West Japan Oncology Group. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): An open label, randomized phase 3 trial. Lancet Oncol. 2010, 11, 121–128. [Google Scholar] [CrossRef]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. North-East Japan Study Group. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. NEJM 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, X.; Le, X.; Costa, D.B. The safety and efficacy of osimertinib for the treatment of EGFR T790M mutation positive non-small-cell lung cancer. Expert Rev. Anticancer Ther. 2016, 16, 383–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goss, G.; Tsai, C.-M.; Shepherd, F.A.; Bazhenova, L.; Lee, J.S.; Crino, L.; Satouchi, M.; Chu, Q.; Hida, T.; Han, J.-Y.; et al. Osimertinib for pretreated EGFR Thr790Met-positive advanced non-small-cell lung cancer (AURA2): A multicenter, open-label, single-arm, phase 2 study. Lancet Oncol. 2016, 17, 1643–1652. [Google Scholar] [CrossRef]
- Jӓnne, P.A.; Yang, J.C.-H.; Kim, D.-W.; Planchard, D.; Ohe, Y.; Ramalingam, S.; Kim, S.-W.; Su, W.-C.; Horn, L.; Haggstrom, D.; et al. AZD9291 in EGFR inhibitor-resistant non-small-cell lung cancer. NEJM 2015, 372, 1689–1699. [Google Scholar]
- Lindeman, N.I.; Cagle, P.T.; Beasley, M.B.; Chitale, D.A.; Dacic, S.; Giaccone, G.; Jenkins, R.B.; Kwiatkowski, D.; Squire, J.; Thunnissen, E.; et al. Molecular testing guideline for selection of lung cancer patients for EGFR and ALK tyrosine kinase inhibitors: Guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J. Thorac. Oncol. 2013, 8, 823–859. [Google Scholar] [PubMed] [Green Version]
- Besse, B.; Adjei, A.; Baas, P.; Nicolson, M.; Paz-Ares, L.; Reck, M.; Smit, E.; Syrigos, K.; Stahel, R.; Felip, E.; et al. 2nd ESMO consensus conference on lung cancer: Non-small-cell lung cancer first-line/second and further lines of treatment in advanced disease. Ann. Oncol. 2014, 25, 1475–1484. [Google Scholar] [CrossRef]
- Ansari, J.; Yun, J.W.; Kompelli, A.R.; Moufarrej, Y.; Alexander, J.; Herrera, G.; Shackelford, R. The liquid biopsy in lung cancer. Genes Cancer 2016, 7, 355–367. [Google Scholar] [PubMed] [Green Version]
- Chouaid, C.; Dujon, C.; Do, P.; Monnet, I.; Madroszyk, A.; Le Caer, H.; Auliac, J.B.; Berard, H.; Thomas, P.; Lena, H.; et al. Feasibility and clinical impact of re-biopsy in advanced non small-cell lung cancer: A prospective multicenter study in a real-world setting (GFPC study 12-01). Lung Cancer 2014, 86, 170–173. [Google Scholar] [CrossRef]
- Yoon, H.J.; Lee, H.Y.; Lee, K.S.; Ahn, M.-J.; Park, K.; Ahn, J.S.; Sun, J.-M.; Kim, J.; Kim, T.S.; Chung, M.J.; et al. Repeat biopsy for mutational analysis of non-small cell lung cancers resistance to previous chemotherapy: Adequacy and complications. Radiology 2012, 265, 939–948. [Google Scholar] [CrossRef]
- Boskovic, T.; Stanic, J.; Pena-Karan, S.; Karan, S.P.; Vujasinovic, G.; Dragisic, D.; Zarogoulidis, K.; Kougioumtzi, I.; Dryllis, G.; Kioumis, I.; et al. Pneumothorax after transthoracic needle biopsy of lung lesions under CT guidance. J. Thorac. Dis. 2014, 6, S99–S107. [Google Scholar]
- Leiten, E.O.; Martinsen, E.M.H.; Bakke, P.S.; Eagan, T.M.L.; Grønseth, R. Complications and discomfort of bronchoscopy: A systematic review. Eur. Clin. Respir. J. 2016, 3, 33324–33332. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-L.; Lee, V.; Liam, C.-K.; Park, K.; Srimuninnimit, V.; Wang, J.; Zhou, C.; Appius, A.; Button, P.; Hooper, G.; et al. ENSURE FASTACT-2 and ASPIRATION Investigators. Clinical utility of a blood-based EGFR mutation test in patients receiving first-line erlotinib therapy in the ENSURE, FASTACT-2, and ASPIRATION studies. Lung Cancer 2018, 126, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Cobas® EGFR Mutation Test v2 Package Insert. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf15/P150047c.pdf (accessed on 18 December 2019).
- Peters, S.; Adjei, A.A.; Gridelli, C.; Reck, M.; Kerr, K.; Felip, E. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up. Ann. Oncol. 2012, 23, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Hellenic Statistical Authority. Available online: http://www.statistics.gr/en/home/ (accessed on 14 January 2019).
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, C.; Sung, M.; Shepherd, F.A.; Nouriany, N.; Sawczak, M.; Paul, T.; Perera-Low, N.; Foster, A.; Zawisza, D.; Feld, R.; et al. Patients with Advanced Non-Small Cell Lung Cancer: Are Research Biopsies a Barrier to Participation in Clinical Trials? J. Thorac. Oncol. 2015, 11, 79–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stinchcombe, T.E.; Socinski, M.A. Considerations for second-line therapy of non-small cell lung cancer. Oncologist 2008, 13, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Hochmair, M.; Schwab, S.; Burghuber, O.; Koger, R.; Setinek, U.; Cseh, A.; Fritz, R.; Buder, A.; Filipits, M. Prevalence of EGFR T790M Mutation in NSCLC Patients after Afatinib Failure, and Subsequent Response to Osimertinib. Poster P2.03–025. In Proceedings of the IASLC 18th World Conference on Lung Cancer, Yokohama, Japan, 15–18 October 2017. [Google Scholar]
- Yu, H.A.; Arcila, M.E.; Rekhtman, N.; Sima, C.; Zakowski, M.; Pao, W.; Kris, M.; Miller, V.; Ladanyi, M.; Riely, G. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin. Cancer Res. 2013, 19, 2240–2247. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.C.-H.; Ahn, M.-J.; Kim, D.-W.; Ramalingam, S.; Sequist, L.; Kim, S.-W.; Kim, J.-H.; Planchard, D.; Felip, E.; Blackhall, F.; et al. Osimertinib in pretreated T790M-positive advanced non-small-cell lung cancer: AURA study phase II extension component. J. Clin. Oncol. 2017, 35, 1288–1296. [Google Scholar] [CrossRef]
- Benlloch, S.; Botero, M.L.; Beltran-Alamillo, J.; Mayo, C.; Gimenez-Capitan, A.; de Aguirre, I.; Queralt, C.; Ramirez, J.L.; Ramon y Cajal, S.; Klughammer, B.; et al. Clinical validation of a PCR assay for the detection of EGFR mutations in non-small cell lung cancer: Retrospective testing of specimens from the EURTAC trial. PLoS ONE 2014, 9, e89518. [Google Scholar] [CrossRef]
- Jenkins, S.; Yang, J.C.-H.; Ramalingam, S.S.; Yu, K.; Patel, S.; Weston, S.; Hodge, R.; Cantarini, M.; Jänne, P.A.; Mitsudomi, T.; et al. Plasma ctDNA analysis for detection of the EGFR T790M mutation in patients with advanced non-small cell lung cancer. J. Thorac. Oncol. 2017, 12, 1061–1070. [Google Scholar] [CrossRef] [Green Version]
- Passiglia, F.; Rizzo, S.; Di Maio, M.; Galvano, A.; Badalamenti, G.; Listì, A.; Gulotta, L.; Castiglia, M.; Fulfaro, F.; Bazan, V.; et al. The diagnostic accuracy of circulating tumor DNA for the detection of EGFR-T790M mutation in NSCLC: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 13379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Organization for the Provision of Health Services (“EOPYY”). Available online: https://www.eopyy.gov.gr/ (accessed on 11 June 2018).
- Hellenic Ministry of Health, Official Government Gazette 946. Available online: http://www.moh.gov.gr/articles/ken-eswteriko/5483-fek-kleista-enopoihmena-noshlia-2012-2017 (accessed on 11 June 2018).
- Hellenic Ministry of Health, Official Government Gazette 1511. Available online: https://www.sfee.gr/fek-1511v06-06-2014-diataxis-sintagografisis-ke-apozimiosis-ogkologikon-farmakon/ (accessed on 11 June 2018).
- Cheng, M.M.; Palma, J.F.; Scudder, S.; Poulios, N.; Liesenfeld, O. The clinical and economic impact of inaccurate EGFR mutation tests in the treatment of metastatic non-small cell lung cancer. J. Pers. Med. 2017, 7, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gancitano, G.; Ravasio, R.; Dionisi, M.; Cortinovis, D. Cost-consequence analysis of three different diagnostic strategies in the first- and second-line treatment of locally advanced or metastatic non-small-cell lung cancer. Farmaeconomia Health Econ. Ther. Pathw. 2018, 19, 27–35. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Estimate | Reference |
|---|---|---|
| Greece population per last census report (2018) | 10,741,165 | [25] |
| Lung cancer incidence | 7.5/10,000 | [26] |
| % lung cancer cases that are non-small cell (NSCLC) | 87% | [3] |
| % NSCLC that are adenocarcinoma, large cell, or unspecified histology | 55% | [3] |
| % NSCLC advanced or metastatic at diagnosis (stage IIIb or IV) | 80% | [3] |
| First-line setting (1L) | ||
| % metastatic NSCLC patients eligible for treatment upon diagnosis (1L) | 90% | Clinical opinion |
| % 1L patients eligible for lung tissue biopsy | 85% | [27] |
| % 1L patients eligible for plasma test | 100% | Assumption |
| EGFR mutation prevalence (exons 18 through 21) | 15.7% | [5] |
| Second-line setting (2L) | ||
| % mNSCLC patients eligible for treatment upon tumor progression (2L) | 50% | [28] |
| % 2L patients eligible for lung tissue re-biopsy | 80% | [18] |
| % 2L patients eligible for plasma test | 100% | Assumption |
| EGFR T790M mutation prevalence | 56% | [29,30,31] |
| Parameter | Estimate | Reference |
|---|---|---|
| Sensitivity: Tissue (exons 19 and 21) | 98.1% | [32] |
| Specificity: Tissue (exons 19 and 21) | 99.3% | [32] |
| Sensitivity: Tissue (T790M) | 88.3% | [33] |
| Specificity: Tissue (T790M) | 97.3% | [33] |
| Sensitivity: Plasma (exons 19 and 21) | 94.0% | [33] |
| Specificity: Plasma (exons 19 and 21) | 94.0% | [33] |
| Sensitivity: Plasma (T790M) | 93.0% | [33] |
| Specificity: Plasma (T790M) | 92.0% | [33] |
| Probability of adverse event or tissue biopsy complication | 11% | [20,21] |
| Parameter | Cost (€) | Reference |
|---|---|---|
| EGFR Mutation Tissue Test | ||
| Specimen collection/lung tissue biopsy (CT-guided aspiration) | 95 | [35] |
| Treat biopsy complication (assumed severe pneumothorax) | 566 | [36] |
| EGFR mutation test (procedural reimbursement) | 160 | [37] |
| EGFR Mutation Plasma Test | ||
| Specimen collection/blood draw | 0 | Blood draw procedure is not separately reimbursed |
| EGFR mutation test (procedural reimbursement) | 160 | Assumed same as EGFR mutation test with tissue specimen |
| Results | Tissue Test Only | Plasma Test Only | Combined Testing Approach | Reflex Testing Approach |
|---|---|---|---|---|
| Newly Diagnosed mNSCLC Patients in Greece (2018) | 3084 | |||
| EGFR Mutation Testing for 1L Therapy (exons 19 and 21) | ||||
| Projected Number of Patients Eligible for EGFR Mutation Testing | 2359 | 2775 | 2775 | 2775 |
| Number of Patients with Correctly Classified EGFR Mutation Status | 2338 | 2609 | 2730 | 2749 |
| Number of Identified EGFR Mutation Positive Patients | 363 | 410 | 425 | 431 |
| Total Cost of Testing Approach | €670,597 | €444,066 | €737,207 | €981,777 |
| BI per Correctly Classified Patient (projected scenario—current scenario) | Current Scenario | −€117 | −€17 | €70 |
| BI per mNSCLC Patient (projected scenario–current scenario) | Current Scenario | −€73 | €22 | €101 |
| EGFR Mutation Testing for 2L Therapy (T790M) | ||||
| Projected Number of Patients Eligible for EGFR Mutation Testing | 1234 | 1542 | 1542 | 1542 |
| Number of Patients with Correctly Classified EGFR Mutation Status | 1138 | 1463 | 1424 | 1512 |
| Number of Identified EGFR Mutation Positive Patients | 610 | 803 | 771 | 846 |
| Total Cost of Testing Approach | €350,639 | €246,703 | €399,980 | €402,387 |
| BI per Correctly Classified Patient (projected scenario—current scenario) | Current Scenario | −€139 | −€27 | −€42 |
| BI per mNSCLC patient (projected scenario–current scenario) | Current Scenario | −€34 | €16 | €17 |
| Results | Tissue Test Only | Plasma Test Only | Combined Testing Approach | Reflex Testing Approach |
|---|---|---|---|---|
| EGFR Mutation Testing for 2L Therapy (T790M) (Plasma test sensitivity 67%; specificity 80%) | ||||
| Projected Number of Patients Eligible for EGFR Mutation Testing | 1234 | 1542 | 1542 | 1542 |
| Number of Patients with Correctly Classified EGFR Mutation Status | 1138 | 1239 | 1363 | 1428 |
| Number of Identified EGFR Mutation Positive Patients | 610 | 579 | 726 | 780 |
| Total Cost of Testing Approach | €350,639 | €246,703 | €399,980 | €434,926 |
| BI per Correctly Classified Patient (projected scenario—current scenario) | Current Scenario | −€109 | −€15 | −€4 |
| BI per mNSCLC patient (projected scenario—current scenario) | Current Scenario | −€34 | €16 | €27 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, M.; Akalestos, A.; Scudder, S. Budget Impact Analysis of EGFR Mutation Liquid Biopsy for First- and Second-Line Treatment of Metastatic Non-Small Cell Lung Cancer in Greece. Diagnostics 2020, 10, 429. https://doi.org/10.3390/diagnostics10060429
Cheng M, Akalestos A, Scudder S. Budget Impact Analysis of EGFR Mutation Liquid Biopsy for First- and Second-Line Treatment of Metastatic Non-Small Cell Lung Cancer in Greece. Diagnostics. 2020; 10(6):429. https://doi.org/10.3390/diagnostics10060429
Chicago/Turabian StyleCheng, Mindy, Athanasios Akalestos, and Sidney Scudder. 2020. "Budget Impact Analysis of EGFR Mutation Liquid Biopsy for First- and Second-Line Treatment of Metastatic Non-Small Cell Lung Cancer in Greece" Diagnostics 10, no. 6: 429. https://doi.org/10.3390/diagnostics10060429
APA StyleCheng, M., Akalestos, A., & Scudder, S. (2020). Budget Impact Analysis of EGFR Mutation Liquid Biopsy for First- and Second-Line Treatment of Metastatic Non-Small Cell Lung Cancer in Greece. Diagnostics, 10(6), 429. https://doi.org/10.3390/diagnostics10060429