
Virtual Non-Contrast versus True Non-Contrast Computed Tomography: Initial Experiences with a Photon Counting Scanner Approved for Clinical Use

 and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Population
2.2. CT Protocols and Image Acquisition
2.3. Quantitative Image Analysis
2.4. Statistical Analysis
3. Results
3.1. Comparison of TNC and VNC Images
3.1.1. TNC versus VNCv
3.1.2. TNC versus VNCa
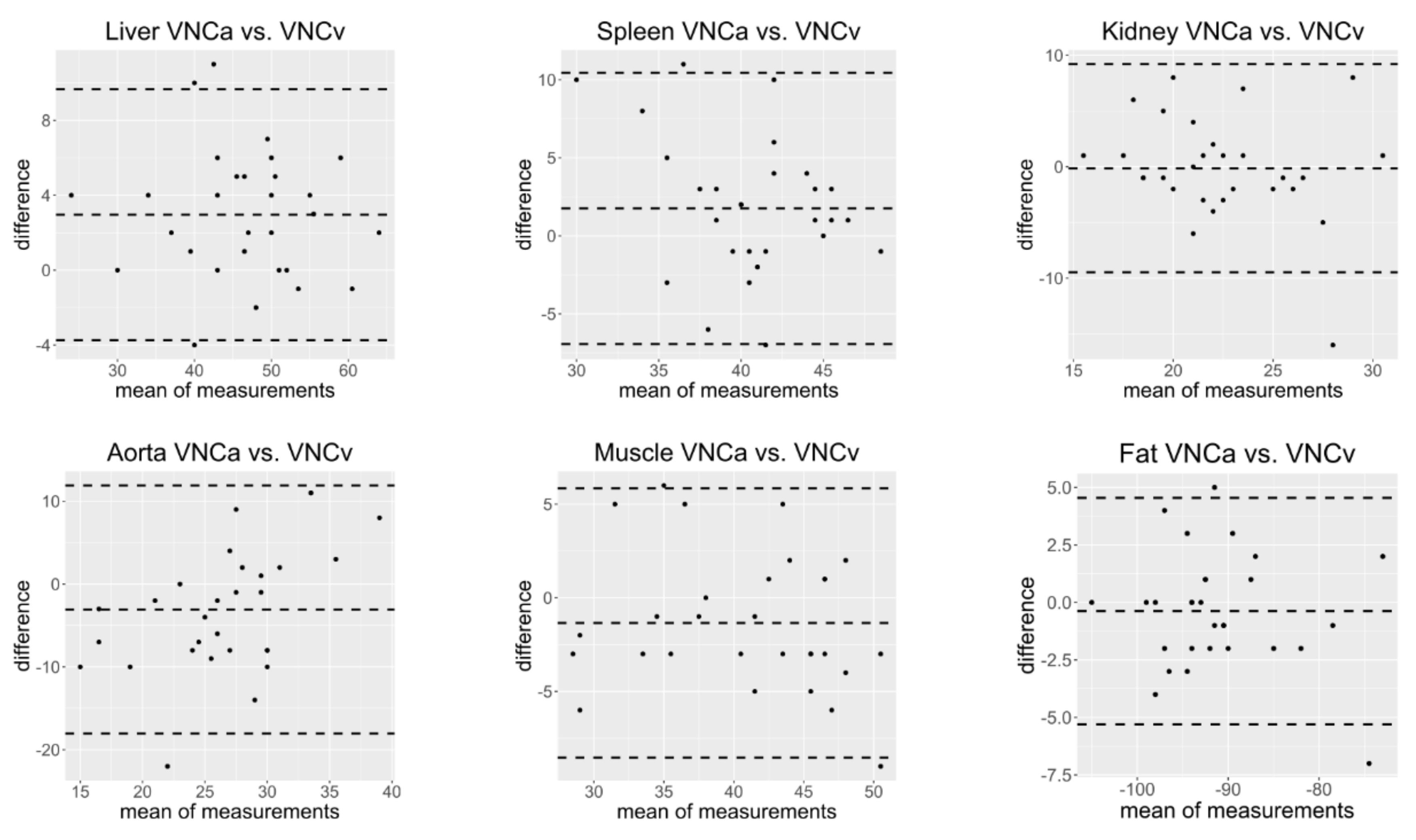
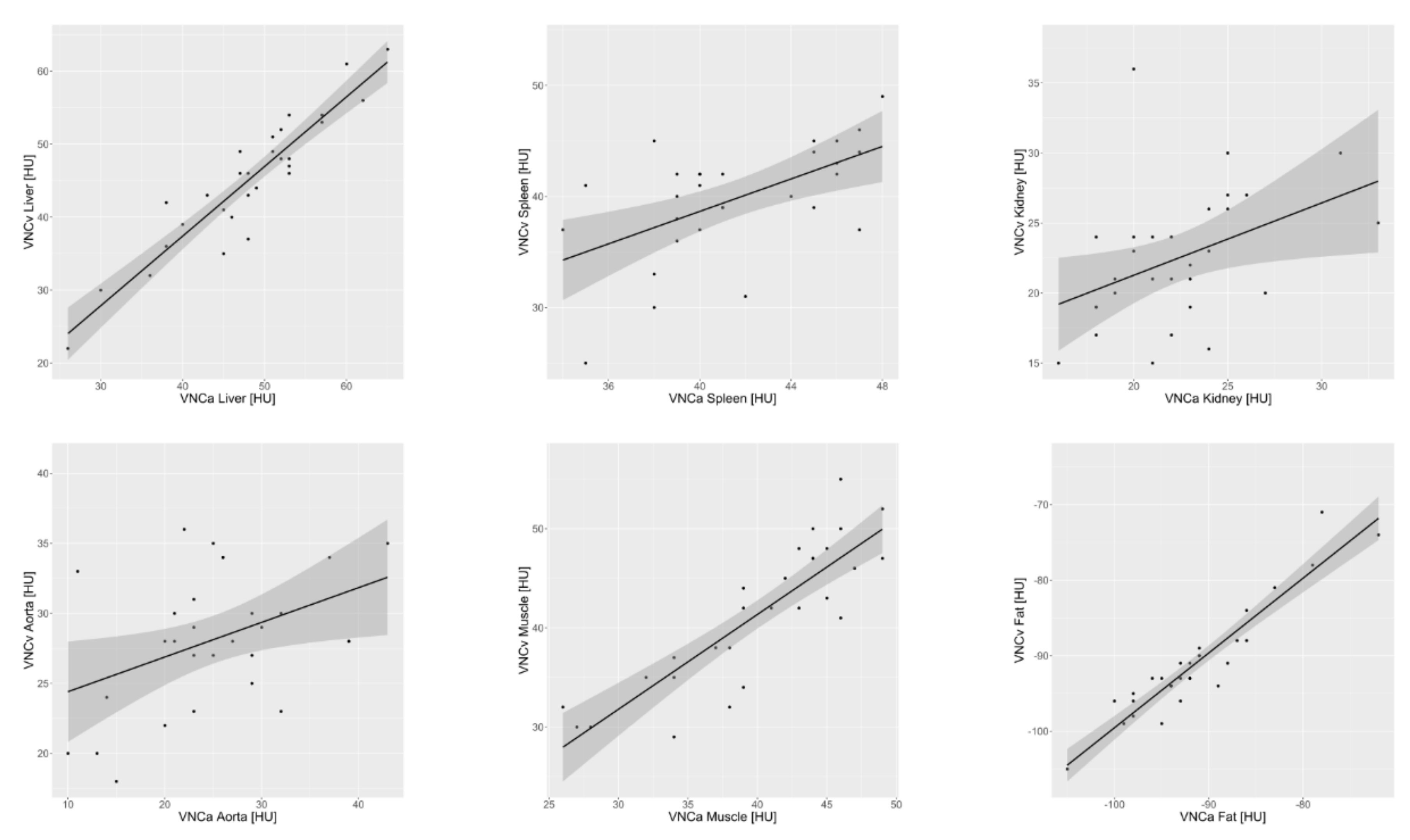
3.1.3. VNCv versus VNCa
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hamrahian, A.H.; Ioachimescu, A.G.; Remer, E.M.; Motta-Ramirez, G.; Bogabathina, H.; Levin, H.S.; Reddy, S.; Gill, I.S.; Siperstein, A.; Bravo, E.L. Clinical utility of noncontrast computed tomography attenuation value (hounsfield units) to differentiate adrenal adenomas/hyperplasias from nonadenomas: Cleveland Clinic experience. J. Clin. Endocrinol. Metab. 2005, 90, 871–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byun, J.; Lee, S.S.; Sung, Y.S.; Shin, Y.; Yun, J.; Kim, H.S.; Yu, E.S.; Lee, S.-G.; Lee, M.-G. CT indices for the diagnosis of hepatic steatosis using non-enhanced CT images: Development and validation of diagnostic cut-off values in a large cohort with pathological reference standard. Eur. Radiol. 2019, 29, 4427–4435. [Google Scholar] [CrossRef] [PubMed]
- Flohr, T.G.; McCollough, C.H.; Bruder, H.; Petersilka, M.; Gruber, K.; Süss, C.; Grasruck, M.; Stierstorfer, K.; Krauss, B.; Raupach, R.; et al. First performance evaluation of a dual-source CT (DSCT) system. Eur. Radiol. 2006, 16, 256–268. [Google Scholar] [CrossRef] [PubMed]
- Hokamp, N.G.; Maintz, D.; Shapira, N.; Chang, D.H.; Noel, P.B.; Healthcare, R.C.I.P. Technical background of a novel detector-based approach to dual-energy computed tomography. Diagn. Interv. Radiol. 2020, 26, 68. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Leng, S.; Yu, L.; Fletcher, J.G. Dual- and Multi-Energy CT: Principles, Technical Approaches, and Clinical Applications. Radiology 2015, 276, 637–653. [Google Scholar] [CrossRef] [PubMed]
- Patino, M.; Prochowski, A.; Agrawal, M.D.; Simeone, F.J.; Gupta, R.; Hahn, P.F.; Sahani, D.V. Material Separation Using Dual-Energy CT: Current and Emerging Applications. RadioGraphics 2016, 36, 1087–1105. [Google Scholar] [CrossRef] [PubMed]
- Sauter, A.P.; Muenzel, D.; Dangelmaier, J.; Braren, R.; Pfeiffer, F.; Rummeny, E.J.; Noël, P.; Fingerle, A.A. Dual-layer spectral computed tomography: Virtual non-contrast in comparison to true non-contrast images. Eur. J. Radiol. 2018, 104, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Toepker, M.; Moritz, T.; Krauss, B.; Weber, M.; Euller, G.; Mang, T.; Wolf, F.; Herold, C.J.; Ringl, H. Virtual non-contrast in second-generation, dual-energy computed tomography: Reliability of attenuation values. Eur. J. Radiol. 2012, 81, e398–e405. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, L.; Rajiah, P.; Ahn, R.; Rassouli, N.; Xi, Y.; Soesbe, T.C.; Lewis, M.A.; Lenkinski, R.; Leyendecker, J.R.; Abbara, S. Spectral detector CT-derived virtual non-contrast images: Comparison of attenuation values with unenhanced CT. Abdom. Radiol. 2017, 42, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Haji-Momenian, S.; Parkinson, W.; Khati, N.; Brindle, K.; Earls, J.; Zeman, R. Single-energy non-contrast hepatic steatosis criteria applied to virtual non-contrast images: Is it still highly specific and positively predictive? Clin. Radiol. 2018, 73, 594.e7–594.e15. [Google Scholar] [CrossRef] [PubMed]
- Laukamp, K.R.; Ho, V.; Obmann, V.C.; Herrmann, K.; Gupta, A.; Borggrefe, J.; Lennartz, S.; Hokamp, N.G.; Ramaiya, N. Virtual non-contrast for evaluation of liver parenchyma and vessels: Results from 25 patients using multi-phase spectral-detector CT. Acta Radiol. 2020, 61, 1143–1152. [Google Scholar] [CrossRef] [PubMed]
- Laukamp, K.R.; Lennartz, S.; Ho, V.; Hokamp, N.G.; Zopfs, D.; Gupta, A.; Graner, F.P.; Borggrefe, J.; Gilkeson, R.; Ramaiya, N. Evaluation of the liver with virtual non-contrast: Single institution study in 149 patients undergoing TAVR planning. Br. J. Radiol. 2020, 93, 20190701. [Google Scholar] [CrossRef] [PubMed]
- Laukamp, K.R.; Kessner, R.; Halliburton, S.; Zopfs, D.; Gupta, A.; Hokamp, N.G. Virtual Noncontrast Images from Portal Venous Phase Spectral-Detector CT Acquisitions for Adrenal Lesion Characterization. J. Comput. Assist. Tomogr. 2021, 45, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Sommer, C.M.; Schwarzwaelder, C.B.; Stiller, W.; Schindera, S.T.; Stampfl, U.; Bellemann, N.; Holzschuh, M.; Schmidt, J.; Weitz, J.; Grenacher, L.; et al. Iodine removal in intravenous dual-energy CT-cholangiography: Is virtual non-enhanced imaging effective to replace true non-enhanced imaging? Eur. J. Radiol. 2012, 81, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Holz, J.A.; Alkadhi, H.; Laukamp, K.R.; Lennartz, S.; Heneweer, C.; Püsken, M.; Persigehl, T.; Maintz, D.; Hokamp, N.G. Quantitative accuracy of virtual non-contrast images derived from spectral detector computed tomography: An abdominal phantom study. Sci. Rep. 2020, 10, 21575. [Google Scholar] [CrossRef] [PubMed]
- Willemink, M.J.; Persson, M.; Pourmorteza, A.; Pelc, N.J.; Fleischmann, D. Photon-counting CT: Technical Principles and Clinical Prospects. Radiology 2018, 289, 293–312. [Google Scholar] [CrossRef] [PubMed]
- Flohr, T.; Petersilka, M.; Henning, A.; Ulzheimer, S.; Ferda, J.; Schmidt, B. Photon-counting CT review. Phys. Med. 2020, 79, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Leng, S.; Zhou, W.; Yu, Z.; Halaweish, A.; Krauss, B.; Schmidt, B.; Yu, L.; Kappler, S.; McCollough, C. Spectral performance of a whole-body research photon counting detector CT: Quantitative accuracy in derived image sets. Phys. Med. Biol. 2017, 62, 7216–7232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, D.N.; Straka, M.; Roos, J.E.; Napel, S.; Fleischmann, D. Dual-energy CT Discrimination of Iodine and Calcium: Experimental Results and Implications for Lower Extremity CT Angiography. Acad. Radiol. 2009, 16, 160–171. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TNC | VNCv | TNC vs. VNCv | VNCa | TNC vs. VNCa | VNCv vs. VNCa | |
|---|---|---|---|---|---|---|
| Mean HU ± SD (n = 72) | Mean HU ± SD (n = 72) | Two-Sided p | Mean HU ± SD (n = 29) | Two-Sided p | Two- Sided p | |
| Liver | 58.58 ± 8.74 | 47.63 ± 9.38 | <0.001 | 48.03 ± 8.88 | <0.001 | <0.001 |
| Spleen | 53.83 ± 3.14 | 42.19 ± 5.16 | <0.001 | 41.55 ± 4.01 | <0.001 | 0.042 |
| Kidney | 36.57 ± 4.41 | 24.69 ± 4.55 | <0.001 | 22.34 ± 3.85 | <0.001 | 0.877 |
| Aorta | 44.44 ± 4.69 | 29.78 ± 5.11 | <0.001 | 25.07 ± 8.30 | <0.001 | 0.039 |
| Muscle | 49.10 ± 6.05 | 42.83 ± 5.94 | <0.001 | 40.21 ± 6.52 | <0.001 | 0.058 |
| Fat | −106.87 ± 8.56 | −89.64 ± 9.02 | <0.001 | −91.31 ± 7.05 | <0.001 | 0.423 |
| Bone | 133.44 ± 51.38 | 47.32 ± 25.70 | <0.001 | 50.97 ± 30.51 | <0.001 | 0.743 |
| TNC − VNCv | TNC − VNCa | VNCv − VNCa | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean Offset HU ± SD | Diff. >15 HU | Diff. >10 HU | Mean Offset HU ± SD | Diff. >15 HU | Diff. >10 HU | Mean Offset HU ± SD | Diff. >15 HU | Diff. >10 HU | |
| Liver | 10.96 ± 4.55 | 10/72 (14%) | 40/72 (56%) | 8.90 ± 3.11 | 0/29 (0%) | 7/29 (24%) | −2.97 ± 3.42 | 0/29 (0%) | 1/29 (3%) |
| Spleen | 11.64 ± 5.19 | 16/72 (22%) | 42/72 (58%) | 11.70 ± 4.52 | 5/29 (17%) | 22/29 (76%) | −1.76 ± 4.44 | 0/29 (0%) | 1/29 (3%) |
| Kidney | 11.88 ± 5.88 | 15/72 (21%) | 46/72 (64%) | 14.97 ± 5.39 | 13/29 (45%) | 24/29 (83%) | 0.14 ± 4.76 | 1/29 (3%) | 1/29 (3%) |
| Aorta | 14.67 ± 5.52 | 31/72 (43%) | 55/72 (76%) | 18.55 ± 8.10 | 21/29 (72%) | 26/29 (90%) | 3.07 ± 7.64 | 1/29 (3%) | 4/29 (14%) |
| Muscle | 6.26 ± 4.42 | 2/72 (3%) | 12/72 (17%) | 8.24 ± 4.25 | 1/29 (3%) | 9/29 (31%) | 1.35 ± 3.67 | 0/29 (0%) | 0/29 (0%) |
| Fat | −17.24 ± 5.81 | 46/72 (64%) | 66/72 (92%) | −16.00 ± 4.43 | 16/29 (55%) | 24/29 (83%) | 0.38 ± 2.51 | 0/29 (0%) | 0/29 (0%) |
| Total | 120/432 (28%) | 261/432 (60%) | 56/174 (32%) | 112/174 (64%) | 2/174 (1%) | 7/174 (4%) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niehoff, J.H.; Woeltjen, M.M.; Laukamp, K.R.; Borggrefe, J.; Kroeger, J.R. Virtual Non-Contrast versus True Non-Contrast Computed Tomography: Initial Experiences with a Photon Counting Scanner Approved for Clinical Use. Diagnostics 2021, 11, 2377. https://doi.org/10.3390/diagnostics11122377
Niehoff JH, Woeltjen MM, Laukamp KR, Borggrefe J, Kroeger JR. Virtual Non-Contrast versus True Non-Contrast Computed Tomography: Initial Experiences with a Photon Counting Scanner Approved for Clinical Use. Diagnostics. 2021; 11(12):2377. https://doi.org/10.3390/diagnostics11122377
Chicago/Turabian StyleNiehoff, Julius Henning, Matthias Michael Woeltjen, Kai Roman Laukamp, Jan Borggrefe, and Jan Robert Kroeger. 2021. "Virtual Non-Contrast versus True Non-Contrast Computed Tomography: Initial Experiences with a Photon Counting Scanner Approved for Clinical Use" Diagnostics 11, no. 12: 2377. https://doi.org/10.3390/diagnostics11122377
APA StyleNiehoff, J. H., Woeltjen, M. M., Laukamp, K. R., Borggrefe, J., & Kroeger, J. R. (2021). Virtual Non-Contrast versus True Non-Contrast Computed Tomography: Initial Experiences with a Photon Counting Scanner Approved for Clinical Use. Diagnostics, 11(12), 2377. https://doi.org/10.3390/diagnostics11122377