
The Role of Imaging in Portal Vein Thrombosis: From the Diagnosis to the Interventional Radiological Management

 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Etiology
- acute and chronic non-cirrhotic liver diseases or malformations and perinatal portal venous system injury
- end-stage chronic liver diseases

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Cirrhotic Systemic Causes | |
|---|---|
| Congenital Factor V Leiden mutation Factor II (prothrombin) mutation Protein C deficiency Protein S deficiency Prothrombine mutation Antithrombin deficiency | Acquired Myeloproliferative disorders Antiphospholipid syndrome Paroxysmal nocturnal hemoglobinuria Oral contraceptives Pregnancy Hyperhomocysteinemia |
| Non-cirrhotic local causes | |
| Congenital Portal vein stenosis Portal vein atresia Portal vein agenesis | Acquired Neonatal omphalitis Neonatal peritonitis Umbilical vein catheterization Diverticulitis, appendicitis Pancreatitis Duodenal ulcer Cholecystitis Tuberculous lymphadenitis Crohn’s disease, ulcerative colitis Cytomegalovirus hepatitis Liver transplantation Splenectomy GI surgery Abdominal trauma Surgical portosystemic shunting, transjugular intrahepatic portosystemic shunt, Iatrogenic |
| Cirrhotic-related diseases | |
| Genetic/Congenital Alagille syndrome Biliary atresia Primary biliary cirrhosis Primary sclerosing cholangitis Alpha-1 antitrypsin deficiency Wilson disease Hemochromatosis Nonalcoholic fatty liver disease Autoimmune hepatitis Cystic fibrosis | Acquired Chronic alcohol abuse Chronic viral hepatitis Chronic hepatotoxic drugs Schistosomiasis Sarcoidosis Cryptogenic cirrhosis Metabolic disorders |
2.1. Acute and Chronic Non-Cirrhotic Liver Diseases
- portal vein damage and subsequent obstruction such as omphalitis, umbilical vein catheterization, neonatal peritonitis, abdominal trauma, and iatrogenic operative trauma to the portal vein;
- congenital anomalies such as portal vein stenosis, portal vein atresia, or agenesis. Obstruction can occur anywhere along the line of left and right vitelline veins from which the portal vein develops. In these cases, PVT is often associated with the presence of other congenital defects, usually of the cardiovascular system;
- factors indirectly associated with PVT, such as neonatal systemic sepsis from non-intraabdominal sources, dehydration, multiple exchange transfusions, and hypercoagulable states, including myeloproliferative disorders such as polycythemia vera, inherited deficiencies of natural anticoagulants such as antithrombin III, protein C and protein S, activated protein C resistance (APCR), and prothrombin gene (G20210A) mutation [2,12].
2.2. End-Stage Chronic Liver Diseases
- the increase of resistance caused by parenchymal architectural distortion leads to increased vascular resistance, decreased flow, and in some cases to the inversion of the flow, and eventually to portal obstruction. A blood flow slower than 15 cm/s in the portal vein is associated with an increased risk of PVT [13];
- the development of hepatofugal portosystemic collateral vessels due to fibrosis and high hepatic sinusoidal pressure. Decreased portal vein inflow caused by portosystemic collateral vessel shunting may result in PVT [14];
2.3. PVT after Liver Transplantation
3. Classification
- extension (intrahepatic, extrahepatic, or both; mono- or polidistrectual);
- degree (partial or complete);
- and onset (acute or chronic).
3.1. Extension
- grade I, thrombus at main portal vein affecting less than 50% of the lumen with or without minimal extension into the superior mesenteric vein (SMV);
- grade II, thrombus at portal vein affecting more than 50%, including complete thrombosis, with or without minimal extension into the SMV;
- grade III, complete PVT plus thrombosis extending into the proximal SMV with patent distal SMV;
- intrahepatic portal vein;
- extrahepatic portal vein;
- both intrahepatic and extrahepatic portal veins;
- SMV and/or SV.
3.2. Degree
3.3. Onset
3.3.1. Cavernous Transformation
3.3.2. Portal Biliopathy
- type I: only extrahepatic bile duct;
- type II: only intrahepatic bile duct;
- type IIIa: extrahepatic and unilateral (right or left) intrahepatic bile duct;
- type IIIb: extrahepatic and bilateral intrahepatic ducts.
4. Role of Non-Invasive Imaging Modalities in Portal Vein Thrombosis
4.1. Color-Doppler Ultrasonography (CDUS) and Contrast-Enhanced Ultrasound (CEUS)
4.2. CT and MR
4.2.1. CT
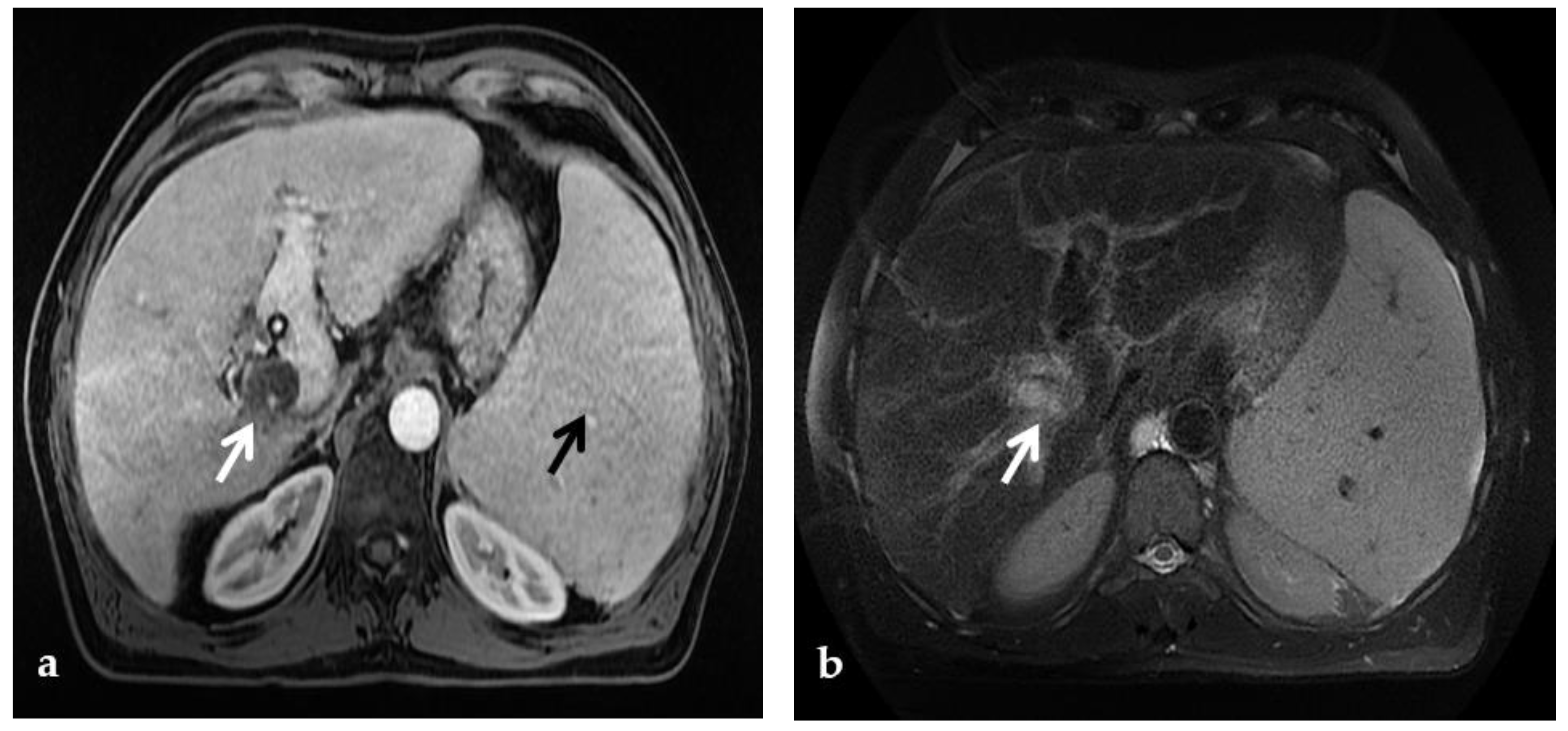
4.2.2. MR
5. Role of Invasive Imaging Modalities in Portal Vein Thrombosis
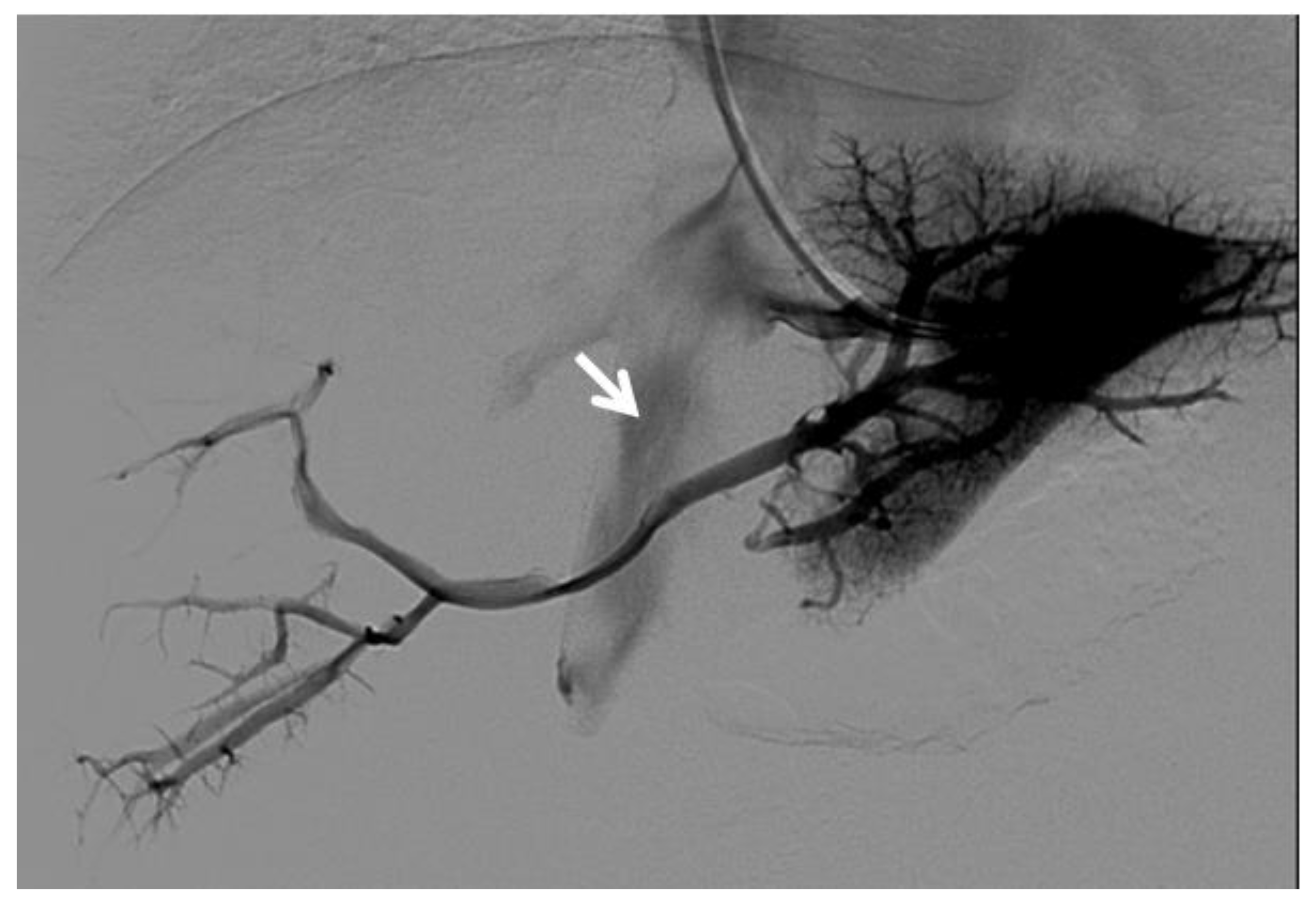
5.1. Retrograde Portography
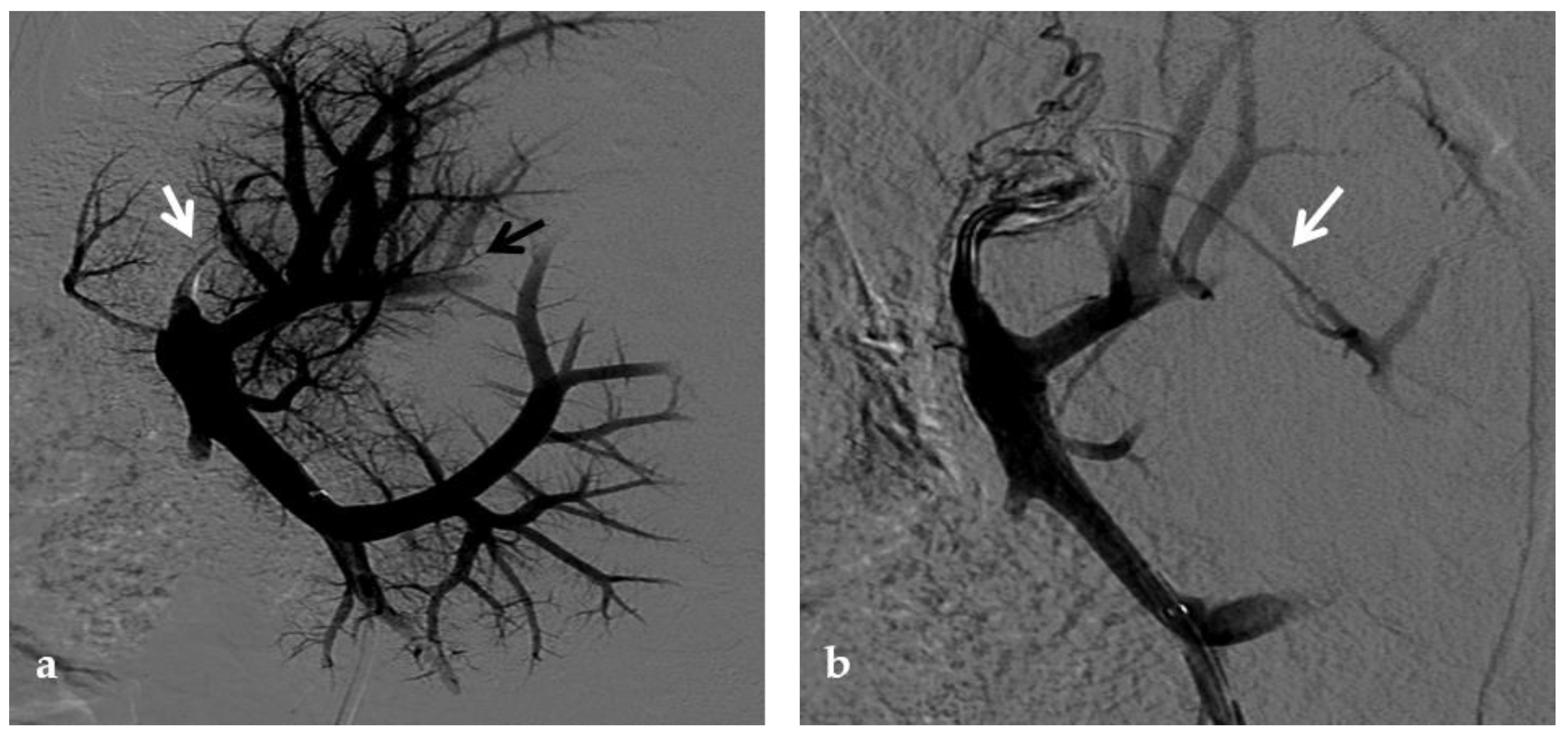
5.2. Percutaneous Direct Portography
5.2.1. Percutaneous Transhepatic Portography
5.2.2. Percutaneous Transsplenic Portography
5.2.3. Percutaneous Transmesenteric Portography
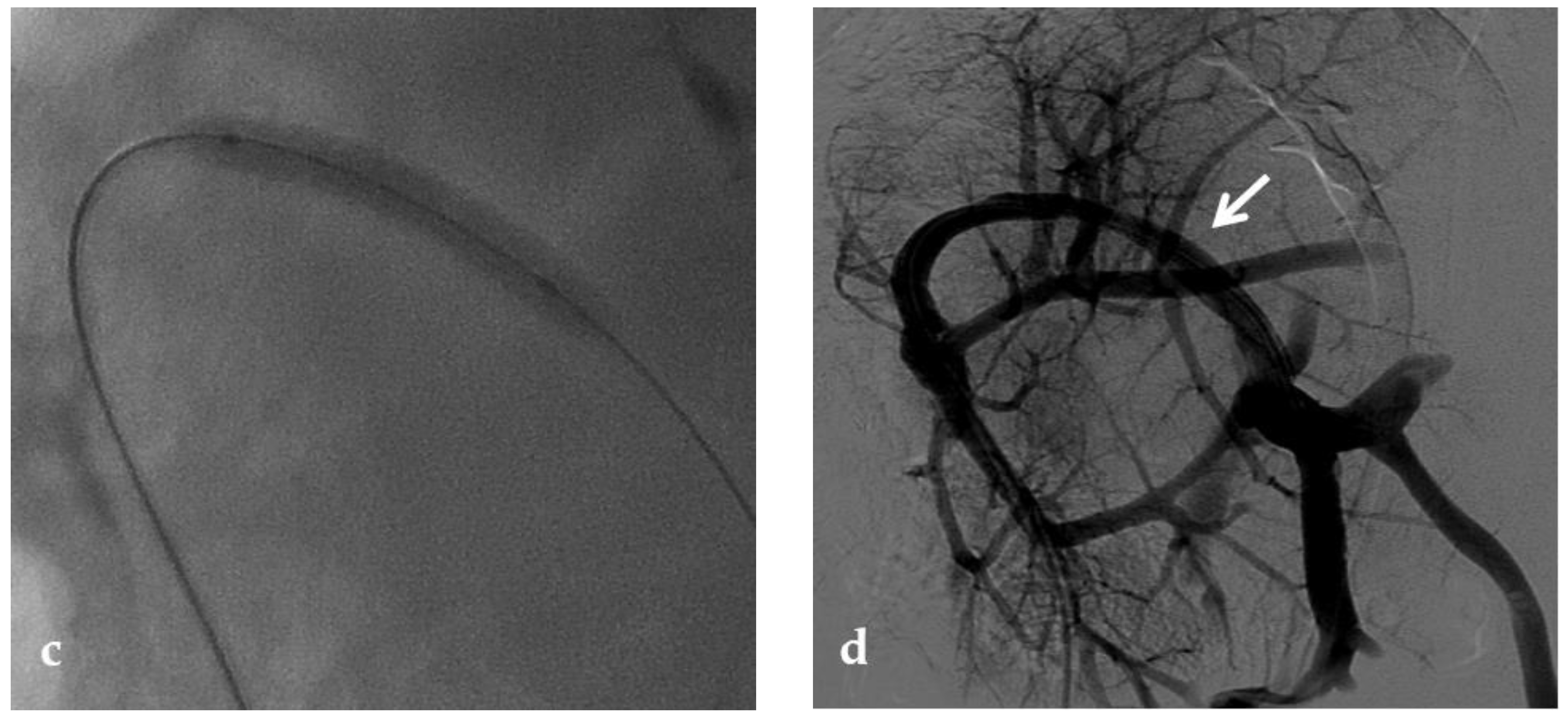
5.3. Transjugular Intrahepatic Portosystemic Shunt (TIPS)
6. Post-Surgical Assessment of Meso-Rex Shunt
7. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponziani, F.R.; Zocco, M.A.; Campanale, C.; Rinninella, E.; Tortora, A.; Di Maurizio, L.; Bombardieri, G.; De Cristofaro, R.; De Gaetano, A.M.; Landolfi, R.; et al. Portal vein thrombosis: Insight into physiopathology, diagnosis, and treatment. World J. Gastroenterol. 2010, 16, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.K.; Agarwal, S.R. Extrahepatic portal vein obstruction. Semin. Liver Dis. 2002, 22, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Turon, F.; Hernández-Gea, V.; Fuster, J.; Garcia-Criado, A.; Barrufet, M.; Darnell, A.; Fondevila, C.; Garcia-Valdecasas, J.C.; Garcia-Pagán, J.C. Nontumoral portal vein thrombosis in patients awaiting liver transplantation. Liver Transpl. 2016, 22, 352–365. [Google Scholar] [CrossRef] [Green Version]
- Koh, P.S.; Chan, S.C.; Chok, K.S.; Sharr, W.W.; Wong, T.C.; Sin, S.L.; Lo, C.M. The friendly incidental portal vein thrombus in liver transplantation. Liver Transpl. 2015, 21, 944–952. [Google Scholar] [CrossRef]
- Perez-Saborido, B.; Pacheco-Sanchez, D.; Barrera-Rebollo, A.; Asensio-Díaz, E.; Pinto-Fuentes, P.; Sarmentero-Prieto, J.C.; Rodríguez-Vielba, P.; Martínez-Díaz, R.; Gonzalo-Martín, M.; Rodríguez, M.; et al. Incidence, management, and results of vascular complications after liver transplantation. Transplant. Proc. 2011, 43, 749–750. [Google Scholar] [CrossRef]
- Millis, J.M.; Seaman, D.S.; Piper, J.B.; Alonso, E.M.; Kelly, S.; Hackworth, C.A.; Newell, K.A.; Bruce, D.S.; Woodle, E.S.; Thistlethwaite, J.R.; et al. Portal vein thrombosis and stenosis in pediatric liver transplantation. Transplantation 1996, 62, 748–754. [Google Scholar] [CrossRef]
- Patel, R.; Mahaveer, J.; Tahir, N.; Rajwal, S.; McClean, P.; Patel, J.V. Outcomes of Percutaneous Portal Vein Intervention in a Single UK Paediatric Liver Transplantation Programme. Cardiovasc. Interv. Radiol. 2018, 41, 96–103. [Google Scholar] [CrossRef] [Green Version]
- Cho, Y.P.; Kim, K.M.; Ha, T.Y.; Ko, G.Y.; Hwang, J.Y.; Park, H.; Chung, Y.S.; Yoon, T.; Hwang, S.; Jun, H.; et al. Management of late-onset portal vein complications in pediatric living-donor liver transplantation. Pediatr. Transplant. 2014, 18, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Ogren, M.; Bergqvist, D.; Bjorck, M.; Acosta, S.; Eriksson, H.; Sternby, N.H. Portal vein thrombosis: Prevalence, patient characteristics and lifetime risk: A population study based on 23,796 consecutive autopsies. World J. Gastroenterol. 2006, 12, 2115–2119. [Google Scholar] [CrossRef]
- Neto, J.S.; Fonseca, E.A.; Feier, F.H.; Pugliese, R.; Candido, H.L.; Benavides, M.R.; Porta, G.; Miura, I.K.; Danesi, V.B.; Guimaraes, T.; et al. Analysis of factors associated with portal vein thrombosis in pediatric living donor liver transplant recipients. Liver Transpl. 2014, 20, 1157–1167. [Google Scholar] [CrossRef]
- Kamran Hejazi Kenari, S.; Mirzakhani, H.; Eslami, M.; Saidi, R.F. Current state of the art in management of vascular complications after pediatric liver transplantation. Pediatr. Transplant. 2015, 19, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Di Giorgio, A.; De Angelis, P.; Cheli, M.; Vajro, P.; Iorio, R.; Cananzi, M.; Riva, S.; Maggiore, G.; Indolfi, G.; Calvo, P.L.; et al. Etiology, presenting features and outcome of children with non-cirrhotic portal vein thrombosis: A multicentre national study. Dig. Liver Dis. 2019, 51, 1179–1184. [Google Scholar] [CrossRef] [PubMed]
- Loudin, M.; Ahn, J. Portal Vein Thrombosis in Cirrhosis. J. Clin. Gastroenterol. 2017, 51, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Kita, Y.; Harihara, Y.; Sano, K.; Hirata, M.; Kubota, K.; Takayama, T.; Ohtomo, K.; Makuuchi, M.; Kita, Y. Reversible hepatofugal portal flow after liver transplantation using a small for-size graft from a living donor. Transpl. Int. 2001, 14, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Gadani, S.; Partovi, S.; Levitin, A.; Zerona, N.; Sengupta, S.; D’Amico, G.; Diago Uso, T.; Menon, K.V.N.; Quintini, C. Narrative review of portal vein thrombosis in cirrhosis: Pathophysiology, diagnosis, and management from an interventional radiology perspective. Cardiovasc. Diagn. Ther. 2022, 12, 135–146. [Google Scholar] [CrossRef]
- Alvarez, F. Portal vein complications after pediatric liver transplantation. Curr. Gastroenterol. Rep. 2012, 14, 270–274. [Google Scholar] [CrossRef]
- Shneider, B.L.; Bosch, J.; de Franchis, R.; Emre, S.H.; Groszmann, R.J.; Ling, S.C.; Lorenz, J.M.; Squires, R.H.; Superina, R.A.; Thompson, A.E.; et al. Expert panel of the Children’s Hospital of Pittsburgh of UPMC. Portal hypertension in children: Expert pediatric opinion on the report of the Baveno v Consensus Workshop on Methodology of Diagnosis and Therapy in Portal Hypertension. Pediatr. Transplant. 2012, 16, 426–437. [Google Scholar] [CrossRef]
- Cavallari, A.; Vivarelli, M.; Bellusci, R.; Jovine, E.; Mazziotti, A.; Rossi, C. Treatment of vascular complications following liver transplantation: Multidisciplinary approach. Hepatogastroenterology 2001, 48, 179–183. [Google Scholar]
- Settmacher, U.; Nussler, N.C.; Glanemann, M.; Haase, R.; Heise, M.; Bechstein, W.O.; Neuhaus, P. Venous complications after orthotopic liver transplantation. Clin. Transplant. 2000, 14, 235–241. [Google Scholar] [CrossRef]
- Heffron, T.G.; Pillen, T.; Smallwood, G.; Henry, S.; Sekar, S.; Casper, K.; Solis, D.; Tang, W.; Fasola, C.; Romero, R. Incidence, impact, and treatment of portal and hepatic venous complications following pediatric liver transplantation: A single-center 12 year experience. Pediatr. Transplant. 2010, 14, 722–729. [Google Scholar] [CrossRef]
- Ueda, M.; Egawa, H.; Ogawa, K.; Uryuhara, K.; Fujimoto, Y.; Kasahara, M.; Ogura, Y.; Kozaki, K.; Takada, Y.; Tanaka, K. Portal vein complications in the long-term course after pediatric living donor liver transplantation. Transplant. Proc. 2005, 37, 1138–1140. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, F.C.; de Tarso Machado, A.; Moreira, A.M.; dos Santos, A.C.B.; da Motta-Leal-Filho, J.M.; Suzuki, L.; Cerri, G.G.; Tannuri, U. Long-term results of the percutaneous transhepatic venoplasty of portal vein stenoses after pediatric liver transplantation. Pediatr. Transplant. 2011, 15, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Dua, A.; McElroy, L.; Wochinski, A.; Hong, J.C.; Cronin, D.C. Portal Steal Syndrome After Full-Size Deceased Donor Liver Transplantation. WMJ 2016, 115, 147–150. [Google Scholar]
- Kim, J.H.; Ko, G.Y.; Sung, K.B.; Yoon, H.K.; Kim, K.R.; Moon, D.; Lee, S.G. Transvenous variceal embolization during or after living-donor liver transplantation to improve portal venous flow. J. Vasc. Interv. Radiol. 2009, 20, 1454–1459. [Google Scholar] [CrossRef] [PubMed]
- Cavalcante, A.C.B.S.; Zurstrassen, C.E.; Carnevale, F.C.; Pugliese, R.P.S.; Fonseca, E.A.; Moreira, A.M.; Matushita, J.P.K., Jr.; Cândido, H.L.L.; Benavides, M.A.R.; Miura, I.K.; et al. Long-term outcomes of transmesenteric portal vein recanalization for the treatment of chronic portal vein thrombosis after pediatric liver transplantation. Am. J. Transplant. 2018, 18, 2220–2228. [Google Scholar] [CrossRef] [Green Version]
- Diamond, I.R.; Fecteau, A.; Millis, J.M.; Losanoff, J.E.; Ng, V.; Anand, R.; Song, C.; the SPLIT Research Group. Impact of graft type on outcome in pediatric liver transplantation: A report From Studies of Pediatric Liver Transplantation (SPLIT). Ann. Surg. 2007, 246, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Saad, W.E. Portal interventions in liver transplant recipients. Semin. Interv. Radiol. 2012, 29, 99–104. [Google Scholar] [CrossRef] [Green Version]
- DeLeve, L.D.; Valla, D.C.; Garcia-Tsao, G. American Association for the Study of Liver Diseases. Vascular disorders of the liver. Hepatology 2009, 49, 1729–1764. [Google Scholar] [CrossRef]
- Yerdel, M.A.; Gunson, B.; Mirza, D.; Karayalçin, K.; Olliff, S.; Buckels, J.; Mayer, D.; McMaster, P.; Pirenne, J. Portal vein thrombosis in adults undergoing liver transplantation: Risk factors, screening, management, and outcome. Transplantation 2000, 15, 1873–1881. [Google Scholar] [CrossRef]
- Pinelli, D.; Camagni, S.; Amaduzzi, A.; Frosio, F.; Fontanella, L.; Carioli, G.; Guizzetti, M.; Zambelli, M.F.; Giovanelli, M.; Fagiuoli, S.; et al. Liver transplantation in patients with non-neoplastic portal vein thrombosis: 20 years of experience in a single center. Clin. Transplant. 2022, 36, e14501. [Google Scholar] [CrossRef]
- Teng, F.; Sun, K.Y.; Fu, Z.R. Tailored classification of portal vein thrombosis for liver transplantation: Focus on strategies for portal vein inflow reconstruction. World J. Gastroenterol. 2020, 26, 2691–2701. [Google Scholar] [CrossRef] [PubMed]
- Bhangui, P.; Lim, C.; Levesque, E.; Salloum, C.; Lahat, E.; Feray, C.; Azoulay, D. Novel classification of non- malignant portal vein thrombosis: A guide to surgical decision-making during liver transplantation. J. Hepatol. 2019, 71, 1038–1050. [Google Scholar] [CrossRef]
- Jamieson, N.V. Changing perspectives in portal vein thrombosis and liver transplantation. Transplantation 2000, 15, 1772–1774. [Google Scholar] [CrossRef] [PubMed]
- Thatipelli, M.R.; McBane, R.D.; Hodge, D.O.; Wysokinski, W.E. Survival and recurrence in patients with splanchnic vein thromboses. Clin. Gastroenterol. Hepatol. 2010, 8, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Luca, A.; Caruso, S.; Milazzo, M.; Marrone, G.; Mamone, G.; Crinò, F.; Maruzzelli, L.; Miraglia, R.; Floridia, G.; Vizzini, G. Natural course of extrahepatic nonmalignant partial portal vein thrombosis in patients with cirrhosis. Radiology 2012, 265, 124–132. [Google Scholar] [CrossRef]
- Condat, B.; Pessione, F.; Denninger, M.H.; Hillaire, S.; Valla, D. Recent portal or mesenteric venous thrombosis: Increased recognition and frequent recanalization on anticoagulant therapy. Hepatology 2000, 32, 466–470. [Google Scholar] [CrossRef]
- Intagliata, N.M.; Caldwell, S.H.; Tripodi, A. Diagnosis, Development, and Treatment of Portal Vein Thrombosis in Patients with and Without Cirrhosis. Gastroenterology 2019, 156, 1582–1599.e1. [Google Scholar] [CrossRef]
- EASL Clinical Practice Guidelines: Vascular diseases of the liver. J. Hepatol. 2016, 64, 179–202. [CrossRef]
- Jha, R.C.; Khera, S.S.; Kalaria, A.D. Portal Vein Thrombosis: Imaging the Spectrum of Disease with an Emphasis on MRI Features. AJR Am. J. Roentgenol. 2018, 211, 14–24. [Google Scholar] [CrossRef]
- Sarin, S.K.; Philips, C.A.; Kamath, P.S.; Choudhury, A.; Maruyama, H.; Nery, F.G.; Valla, D.C. Toward a Comprehensive New Classification of Portal Vein Thrombosis in Patients with Cirrhosis. Gastroenterology 2016, 151, 574–577. [Google Scholar] [CrossRef] [Green Version]
- Chou, C.K.; Mak, C.W.; Tzeng, W.S.; Chang, J.M. CT of small bowel ischemia. Abdom. Imaging 2004, 29, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Marin, D.; Galluzzo, A.; Plessier, A.; Brancatelli, G.; Valla, D.; Vilgrain, V. Focal nodular hyperplasia-like lesions in patients with cavernous transformation of the portal vein: Prevalence, MR findings and natural history. Eur. Radiol. 2011, 21, 2074–2082. [Google Scholar] [CrossRef]
- Dilawari, J.B.; Chawla, Y.K. Pseudosclerosing cholangitis in extrahepatic portal venous obstruction. Gut 1992, 33, 272–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khuroo, M.S.; Yattoo, G.N.; Zargar, S.A.; Javid, G.; Dar, M.Y.; Khan, B.A.; Boda, M.I. Biliary abnormalities associated with extrahepatic portal venous obstruction. Hepatology 1993, 17, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Condat, B.; Vilgrain, V.; Asselah, T.; O’Toole, D.; Rufat, P.; Zappa, M.; Moreau, R.; Valla, D. Portal cavernoma-associated cholangiopathy: A clinical and MR cholangiography coupled with MR portography imaging study. Hepatology 2003, 37, 1302–1308. [Google Scholar] [CrossRef]
- Moomjian, L.N.; Winks, S.G. Portal cavernoma cholangiopathy: Diagnosis, imaging, and intervention. Abdom. Radiol. 2017, 42, 57–68. [Google Scholar] [CrossRef]
- Kalra, N.; Shankar, S.; Khandelwal, N. Imaging of portal cavernoma cholangiopathy. J. Clin. Exp. Hepatol. 2014, 4, S44–S52. [Google Scholar] [CrossRef] [Green Version]
- Chandra, R.; Kapoor, D.; Tharakan, A.; Chaudhary, A.; Sarin, S.K. Portal biliopathy. J. Gastroenterol. Hepatol. 2001, 16, 1086–1092. [Google Scholar] [CrossRef]
- Arora, A.; Sarin, S.K. Multimodality imaging of primary extrahepatic portal vein obstruction (EHPVO): What every radiologist should know. Br. J. Radiol. 2015, 88, 20150008. [Google Scholar] [CrossRef] [Green Version]
- De Gaetano, A.M.; Lafortune, M.; Patriquin, H.; De Franco, A.; Aubin, B.; Paradis, K. Cavernous transformation of the portal vein: Patterns of intrahepatic and splanchnic collateral circulation detected with Doppler sonography. AJR Am. J. Roentgenol. 1995, 165, 1151–1155. [Google Scholar] [CrossRef] [Green Version]
- Parvey, H.R.; Raval, B.; Sandler, C.M. Portal vein thrombosis: Imaging findings. AJR Am. J. Roentgenol. 1994, 162, 77–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, N.; Sasaki, A.; Tomiyama, T.; Tano, S.; Kimura, K. Color Doppler ultrasonography in the diagnosis of cavernous transformation of the portal vein. J. Clin. Ultrasound 1997, 25, 227–233. [Google Scholar] [CrossRef]
- Sacerdoti, D.; Bolognesi, M.; Bombonato, G.C.; Merkel, C.; Gatta, A. Pathophysiology of arterial Doppler parameters in portal hypertension. Ultrasound Med. Biol. 2000, 26, A120. [Google Scholar]
- Webster, G.J.; Burroughs, A.K.; Riordan, S.M. Review article: Portal vein thrombosis—New insights into aetiology and management. Aliment. Pharmacol. Ther. 2005, 1, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Goh, Y.; Neo, W.T.; Teo, Y.M.; Lim, Y.T.; Dewi, M.; Ganpathi, I.S.; Bonney, G.K.; Mali, V.; Krishnan, P.; Kapur, J. Role of contrast-enhanced ultrasound in the evaluation of post-liver transplant vasculature. Clin. Radiol. 2020, 75, 832–844. [Google Scholar] [CrossRef]
- Claudon, M.; Dietrich, C.F.; Choi, B.I.; Cosgrove, D.O.; Kudo, M.; Nolsøe, C.P.; Piscaglia, F.; Wilson, S.R.; Barr, R.G.; Chammas, M.C.; et al. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) in the liver--update 2012: A WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultraschall Med. 2013, 34, 11–29. [Google Scholar]
- Wachsberg, R.H.; Bahramipour, P.; Sofocleous, C.T.; Barone, A. Hepatofugal flow in the portal venous system: Pathophysiology, imaging findings, and diagnostic pitfalls. Radiographics 2002, 22, 123–140. [Google Scholar] [CrossRef]
- Minoda, A.M.; Cadete, R.B.F.; Teixeira, S.R.; Muglia, V.F.; Elias Junior, J.; Melo-Leite, A.F. The ABCD of portal vein thrombosis: A systematic approach. Radiol. Bras. 2020, 53, 424–429. [Google Scholar] [CrossRef]
- Qi, X.; Han, G.; He, C.; Yin, Z.; Guo, W.; Niu, J.; Fan, D. CT features of non-malignant portal vein thrombosis: A pictorial review. Clin. Res. Hepatol. Gastroenterol. 2012, 36, 561–568. [Google Scholar] [CrossRef]
- Cerri, G.G.; Habr-Gama, A.; Paranagua-Vezozzo, D.; Machado, M.C.; Pinotti, H.W.; Magalhaes, A. Doppler demonstration of cystic vein dilatation secondary to portal vein thrombosis. Surg. Endosc. 1991, 5, 92–93. [Google Scholar] [CrossRef]
- Dhiman, R.K.; Saraswat, V.A.; Valla, D.C.; Chawla, Y.; Behera, A.; Varma, V.; Agarwal, S.; Duseja, A.; Puri, P.; Kalra, N.; et al. Portal cavernoma cholangiopathy: Consensus statement of a working party of the Indian national association for study of the liver. J. Clin. Exp. Hepatol. 2014, 4, S2–S14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumortier, J.; Vaillant, E.; Boillot, O.; Poncet, G.; Henry, L.; Scoazec, J.Y.; Partensky, C.; Valette, P.J.; Paliard, P.; Ponchon, T. Diagnosis and treatment of biliary obstruction caused by portal cavernoma. Endoscopy 2003, 35, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Kathemann, S.; Lainka, E.; Ludwig, J.M.; Wetter, A.; Paul, A.; Hoyer, P.F.; Forsting, M.; Schlosser, T. Imaging of the intrahepatic portal vein in children with extrahepatic portal vein thrombosis—Comparison of magnetic resonance imaging and retrograde portography. J. Pediatr. Surg. 2019, 54, 1686–1690. [Google Scholar] [CrossRef]
- Lebrec, D.; Bataille, C.; Bercoff, E.; Valla, D. Hemodynamic changes in patients with portal venous obstruction. Hepatology 1983, 3, 550–553. [Google Scholar] [CrossRef] [PubMed]
- Alberti, D.; Colusso, M.; Cheli, M.; Ravelli, P.; Indriolo, A.; Signorelli, S.; Fagiuoli, S.; D’Antiga, L. Results of a stepwise approach to extrahepatic portal vein obstruction in children. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Carollo, V.; Marrone, G.; Cortis, K.; Mamone, G.; Caruso, S.; Milazzo, M.; Maruzzelli, L.; di Francesco, F.; Delle, M.; Miraglia, R.; et al. Multimodality imaging of the Meso-Rex bypass. Abdom. Radiol. 2019, 44, 1379–1394. [Google Scholar] [CrossRef]
- Marot, A.; Barbosa, J.V.; Duran, R.; Deltenre, P.; Denys, A. Percutaneous portal vein recanalization using self-expandable nitinol stents in patients with non-cirrhotic non-tumoral portal vein occlusion. Diagn. Interv. Imaging 2019, 100, 147–156. [Google Scholar] [CrossRef]
- Uller, W.; Knoppke, B.; Schreyer, A.G.; Heiss, P.; Schlitt, H.J.; Melter, M.; Stroszczynski, C.; Zorger, N.; Wohlgemuth, W.A. Interventional Radiological Treatment of Perihepatic Vascular Stenosis or Occlusion in Pediatric Patients After Liver Transplantation. Cardiovasc. Interv. Radiol. 2013, 36, 1562–1571. [Google Scholar] [CrossRef]
- Ueda, M.; Oike, F.; Kasahara, M.; Ogura, Y.; Ogawa, K.; Haga, H.; Takada, Y.; Egawa, H.; Tanaka, K.; Uemoto, S. Portal Vein Complications in Pediatric Living Donor Liver Transplantation Using Left-Side Grafts. Am. J. Transplant. 2008, 8, 2097–2105. [Google Scholar] [CrossRef]
- Ko, G.Y.; Sung, K.B.; Lee, S.; Yoon, H.K.; Kim, K.R.; Kim, K.M.; Lee, Y.J. Stent placement for the treatment of portal vein stenosis or occlusion in pediatric liver transplant recipients. J. Vasc. Interv. Radiol. 2007, 18, 1215–1221. [Google Scholar] [CrossRef]
- Gomez-Gutierrez, M.; Quintela, J.; Marini, M.; Gala, B.; Suarez, F.; Cao, I.; Sellés, C.C.; Aguirrezabalaga, J.; Otero, A.; Mosteiro, S. Portal vein thrombosis in patients undergoing orthotopic liver transplantation: Intraoperative endovascular radiological procedures. Transplant. Proc. 2005, 37, 3906–3908. [Google Scholar] [CrossRef] [PubMed]
- Cherukuri, R.; Haskal, Z.J.; Naji, A.; Shaked, A. Percutaneous thrombolysis and stent placement for the treatment of portal vein thrombosis after liver transplantation: Long-term follow-up. Transplantation 1998, 27, 1124–1126. [Google Scholar] [CrossRef] [PubMed]
- Funaki, B.; Rosenblum, J.D.; Leef, J.A.; Zaleski, G.X.; Farrell, T.; Lorenz, J.; Brady, L. Percutaneous treatment of portal venous stenoses in children and adolescents with segmental hepatic transplantation: Long-term results. Radiology 2000, 215, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Mathias, K.; Bolder, U.; Lohlein, D.; Jager, H. Percutaneous transhepatic angioplasty and stent implantation for prehepatic portal vein obstruction. Cardiovasc. Interv. Radiol. 1993, 16, 313–315. [Google Scholar] [CrossRef] [PubMed]
- Uflacker, R. Applications of percutaneous mechanical thrombectomy in transjugular intrahepatic portosystemic shunt and portal vein thrombosis. Tech. Vasc. Interv. Radiol. 2003, 6, 59–69. [Google Scholar] [CrossRef]
- Bertram, H.; Pfister, E.D.; Becker, T.; Schoof, S. Transsplenic endovascular therapy of portal vein stenosis and subsequent complete portal vein thrombosis in a 2-year-old child. J. Vasc. Interv. Radiol. 2010, 21, 1760–1764. [Google Scholar] [CrossRef]
- Zhu, K.; Meng, X.; Zhou, B.; Qian, J.; Huang, W.; Deng, M.; Shan, H. Percutaneous transsplenic portal vein catheterization: Technical procedures, safety, and clinical applications. J. Vasc. Interv. Radiol. 2013, 24, 518–527. [Google Scholar] [CrossRef]
- Haddad, M.M.; Fleming, C.J.; Thompson, S.M.; Reisenauer, C.J.; Parvinian, A.; Frey, G.; Toskich, B.; Andrews, J.C. Comparison of Bleeding Complications between Transplenic versus Transhepatic Access of the Portal Venous System. J. Vasc. Interv. Radiol. 2018, 29, 1383–1391. [Google Scholar] [CrossRef]
- Ohm, J.Y.; Ko, G.Y.; Sung, K.B.; Gwon, D.I.; Ko, H.K. Safety and efficacy of transhepatic and transsplenic access for endovascular management of portal vein complications after liver transplantation. Liver Transpl. 2017, 23, 1133–1142. [Google Scholar] [CrossRef] [Green Version]
- Nosaka, S.; Isobe, Y.; Kasahara, M.; Miyazaki, O.; Sakamoto, S.; Uchida, H.; Shigeta, T.; Masaki, H. Recanalization of post-transplant late-onset long segmental portal vein thrombosis with bidirectional transhepatic and transmesenteric approach. Pediatr. Transplant. 2013, 17, E71–E75. [Google Scholar] [CrossRef]
- Entezari, P.; Riaz, A.; Thornburg, B.; Salem, R. Percutaneous Ultrasound-Guided Superior and Inferior Mesenteric Vein Access for Portal Vein Recanalization-Transjugular Intrahepatic Portosystemic Shunt: A Case Series. Cardiovasc. Interv. Radiol. 2021, 44, 496–499. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, F.C.; Santos, A.C.; Seda-Neto, J.; Zurstrassen, C.E.; Moreira, A.M.; Carone, E.; Marcelino, A.S.Z.; Porta, G.; Pugliese, R.; Miura, I.; et al. Portal vein obstruction after liver transplantation in children treated by simultaneous minilaparotomy and transhepatic approaches: Initial experience. Pediatr. Transplant. 2011, 15, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Ko, G.Y.; Yoon, H.K.; Shin, J.H.; Ko, H.K.; Sung, K.B. Intraoperative stent placement in the portal vein during or after liver transplantation. Liver Transpl. 2007, 13, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.F.; Ou, H.Y.; Tsang, L.L.; Yu, C.-Y.; Huang, T.-L.; Chen, T.-Y.; Concejero, A.; Wang, C.-C.; Wang, S.-H.; Lin, T.-S.; et al. Vascular stents in the management of portal venous complications in living donor liver transplantation. Am. J. Transplant. 2010, 10, 1276–1283. [Google Scholar] [CrossRef]
- Han, G.; Qi, X.; He, C.; Yin, Z.; Wang, J.; Xia, J.; Yang, Z.; Bai, M.; Meng, X.; Niu, J.; et al. Transjugular intrahepatic portosystemic shunt for portal vein thrombosis with symptomatic portal hypertension in liver cirrhosis. J. Hepatol. 2011, 54, 78–88. [Google Scholar] [CrossRef]
- Luca, A.; Miraglia, R.; Caruso, S.; Milazzo, M.; Sapere, C.; Maruzzelli, L.; Vizzini, G.; Tuzzolino, F.; Gridelli, B.; Bosch, J. Short-and long-term effects of the transjugular intrahepatic portosystemic shunt on portal vein thrombosis in patients with cirrhosis. Gut 2011, 60, 846–852. [Google Scholar] [CrossRef]
- Valentin, N.; Korrapati, P.; Constantino, J.; Young, A.; Weisberg, I. The role of transjugular intrahepatic portosystemic shunt in the management of portal vein thrombosis: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1187–1193. [Google Scholar] [CrossRef]
- Rossle, M.; Haag, K.; Ochs, A.; Sellinger, M.; Noldge, G.; Perarnau, J.; Berger, E.; Blum, U.; Gabelmann, A.; Hauenstein, K.; et al. The transjugular intrahepatic portosystemic stent-shunt procedure for variceal bleeding. N. Engl. J. Med. 1994, 330, 165–171. [Google Scholar] [CrossRef]
- Senzolo, M.; Tibbals, J.; Cholongitas, E.; Triantos, C.K.; Burroughs, A.K.; Patch, D. Transjugular intrahepatic portosystemic shunt for portal vein thrombosis with and without cavernous transformation. Aliment. Pharm. Ther. 2006, 23, 767–775. [Google Scholar] [CrossRef]
- Qi, X.; Han, G.; Yin, Z.; He, C.; Wang, J.; Guo, W.; Niu, J.; Zhang, W.; Bai, M.; Fan, D. Transjugular Intrahepatic Portosystemic Shunt for Portal Cavernoma with Symptomatic Portal Hypertension in Non-cirrhotic Patients. Dig. Dis. Sci. 2012, 57, 1072–1082. [Google Scholar] [CrossRef]
- de Ville de Goyet, J.; Lo Zupone, C.; Grimaldi, C.; D’Ambrosio, G.; Candusso, M.; Torre, G.; Monti, L. Meso-Rex bypass as an alternative technique for portal vein reconstruction at or after liver transplantation in children: Review and perspectives. Pediatr. Transplant. 2013, 17, 19–26. [Google Scholar] [CrossRef] [PubMed]
- di Francesco, F.; Grimaldi, C.; de Ville de Goyet, J. Meso-Rex bypass–a procedure to cure prehepatic portal hypertension: The insight and the inside. J. Am. Coll. Surg. 2014, 218, e23–e36. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, H.; Pimpalwar, S.; Ashton, D.; Chau, A.; Nagaraj, A.; Hernandez, J.A. Recanalization of Chronic Portal Vein Occlusion in Pediatric Liver Transplant Patients. J. Vasc. Interv. Radiol. 2019, 30, 885–891. [Google Scholar] [CrossRef] [PubMed]
- Kallini, J.R.; Gabr, A.; Kulik, L.; Ganger, D.; Lewandowski, R.; Thornburg, B.; Salem, R. Noncirrhotic complete obliterative portal vein thrombosis: Novel management using trans-splenic transjugular intrahepatic portosystemic shunt with portal vein recanalization. Hepatology 2016, 63, 1387–1390. [Google Scholar] [CrossRef] [PubMed]
- de Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C. Baveno VII Faculty. Baveno VII—Renewing consensus in portal hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Tsao, G.; Bosch, J. Management of varices and variceal hemorrhage in cirrhosis. N. Engl. J. Med. 2010, 362, 823–832. [Google Scholar] [CrossRef]






















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marra, P.; Dulcetta, L.; Carbone, F.S.; Muglia, R.; Muscogiuri, G.; Cheli, M.; D’Antiga, L.; Colledan, M.; Fagiuoli, S.; Sironi, S. The Role of Imaging in Portal Vein Thrombosis: From the Diagnosis to the Interventional Radiological Management. Diagnostics 2022, 12, 2628. https://doi.org/10.3390/diagnostics12112628
Marra P, Dulcetta L, Carbone FS, Muglia R, Muscogiuri G, Cheli M, D’Antiga L, Colledan M, Fagiuoli S, Sironi S. The Role of Imaging in Portal Vein Thrombosis: From the Diagnosis to the Interventional Radiological Management. Diagnostics. 2022; 12(11):2628. https://doi.org/10.3390/diagnostics12112628
Chicago/Turabian StyleMarra, Paolo, Ludovico Dulcetta, Francesco Saverio Carbone, Riccardo Muglia, Giuseppe Muscogiuri, Maurizio Cheli, Lorenzo D’Antiga, Michele Colledan, Stefano Fagiuoli, and Sandro Sironi. 2022. "The Role of Imaging in Portal Vein Thrombosis: From the Diagnosis to the Interventional Radiological Management" Diagnostics 12, no. 11: 2628. https://doi.org/10.3390/diagnostics12112628
APA StyleMarra, P., Dulcetta, L., Carbone, F. S., Muglia, R., Muscogiuri, G., Cheli, M., D’Antiga, L., Colledan, M., Fagiuoli, S., & Sironi, S. (2022). The Role of Imaging in Portal Vein Thrombosis: From the Diagnosis to the Interventional Radiological Management. Diagnostics, 12(11), 2628. https://doi.org/10.3390/diagnostics12112628