

The Role of Cytokinome in the HNSCC Tumor Microenvironment: A Narrative Review and Our Experience

 ,
,  , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Review
2.2. Our Experience in the Analysis of Cytokinome in R/M HNSCC
3. Results
3.1. Literature Revision
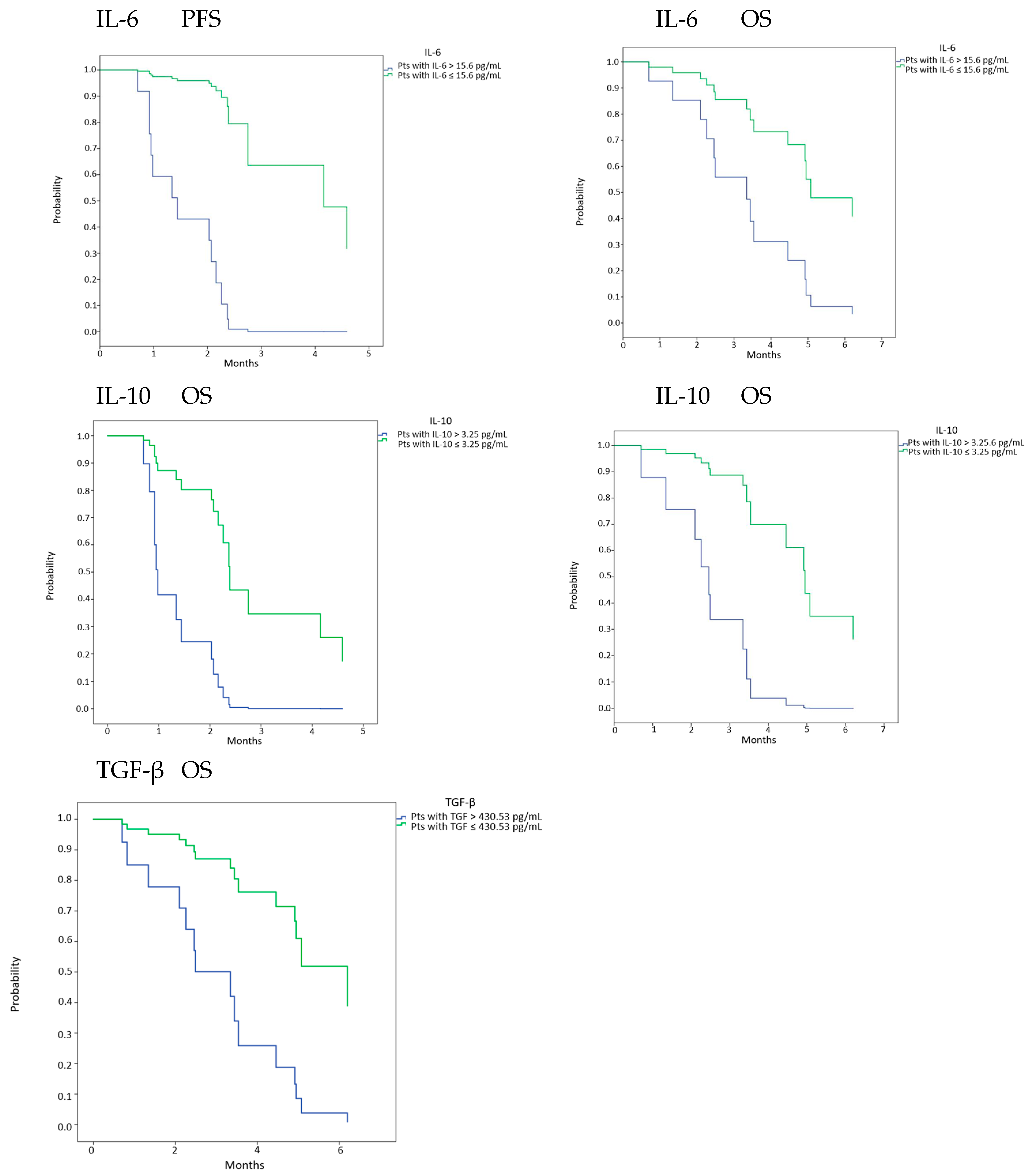
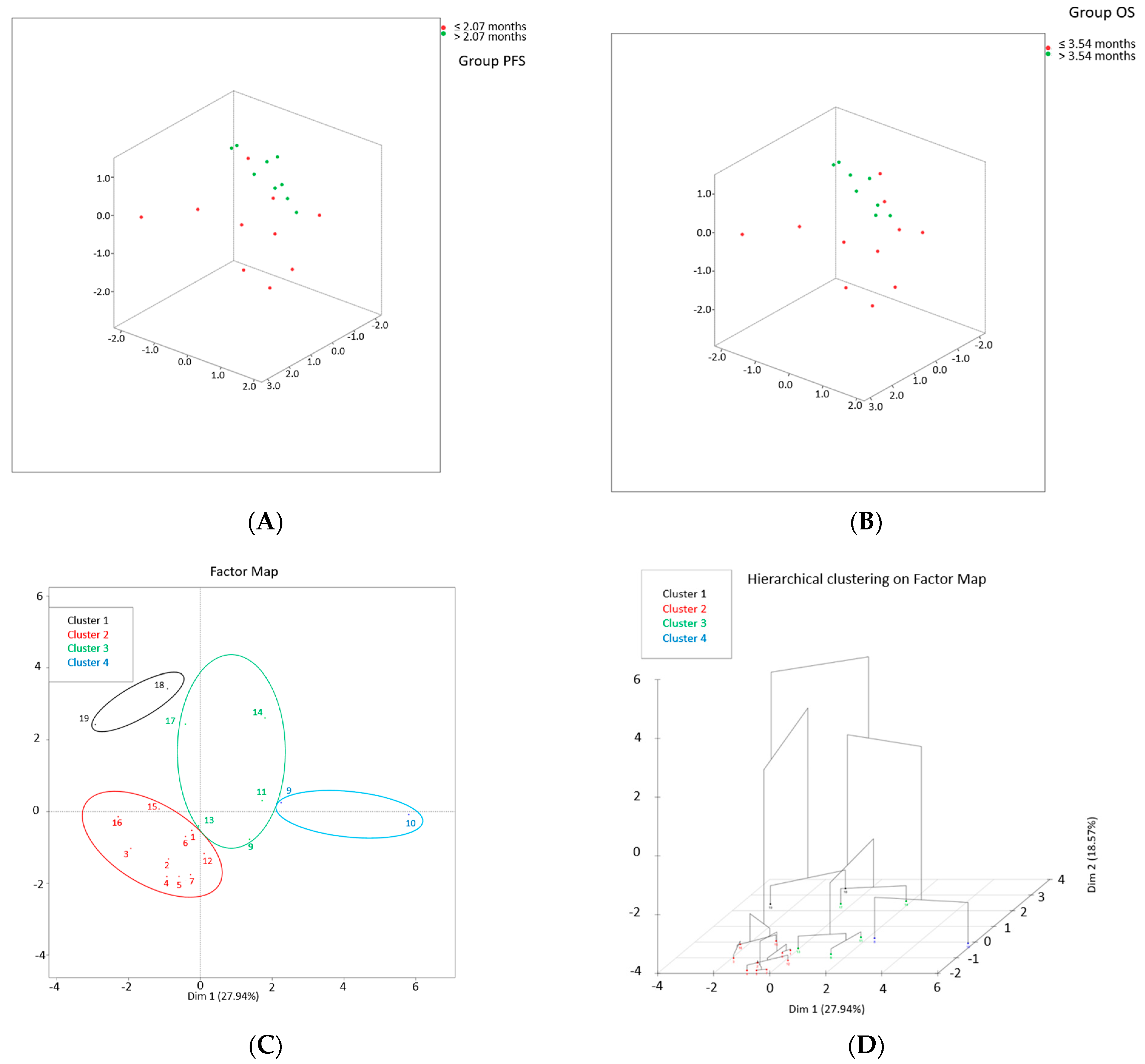
3.2. Our Experience in the Analysis of Cytokinome as an Effort to Find Prognostic Biomarkers
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Powell, S.F.; Vu, L.; Spanos, W.C.; Pyeon, D. The Key Differences between Human Papillomavirus-Positive and -Negative Head and Neck Cancers: Biological and Clinical Implications. Cancers 2021, 13, 5206. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Seruga, B.; Zhang, H.; Bernstein, L.J.; Tannock, I.F. Cytokines and their relationship to the symptoms and outcome of cancer. Nat. Cancer 2008, 8, 887–899. [Google Scholar] [CrossRef] [PubMed]
- Denaro, N.; Merlano, M.C.; Nigro, C.L. Further Understanding of the Immune Microenvironment in Head and Neck Squamous Cell Carcinoma: Implications for Prognosis. Cancer Manag. Res. 2021, 13, 3973–3980. [Google Scholar] [CrossRef] [PubMed]
- Capone, F.; Guerriero, E.; Sorice, A.; Colonna, G.; Ciliberto, G.; Costantini, S. Serum Cytokinome Profile Evaluation: A Tool to Define New Diagnostic and Prognostic Markers of Cancer Using Multiplexed Bead-Based Immunoassays. Mediat. Inflamm. 2016, 2016, 3064643. [Google Scholar] [CrossRef] [PubMed]
- Huntington, K.E.; Louie, A.; Zhou, L.; El-Deiry, W.S. A high-throughput customized cytokinome screen of colon cancer cell responses to small-molecule oncology drugs. Oncotarget 2021, 12, 1980–1991. [Google Scholar] [CrossRef]
- She, Y.; Kong, X.; Ge, Y.; Yin, P.; Liu, Z.; Chen, J.; Gao, F.; Fang, S. Immune-related gene signature for predicting the prognosis of head and neck squamous cell carcinoma. Cancer Cell Int. 2020, 20, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Dimopoulou, I.; Orfanos, S.; Kotanidou, A.; Livaditi, O.; Giamarellos-Bourboulis, E.; Athanasiou, C.; Korovesi, I.; Sotiropoulou, C.; Kopterides, P.; Ilias, I.; et al. Plasma pro-and anti-inflammatory cytokine levels and outcome prediction in unselected critically ill patients. Cytokine 2018, 41, 263–267. [Google Scholar] [CrossRef]
- Kartikasari, A.E.R.; Huertas, C.S.; Mitchell, A.; Plebanski, M. Tumor-Induced Inflammatory Cytokines and the Emerging Diagnostic Devices for Cancer Detection and Prognosis. Front. Oncol. 2021, 11, 692142. [Google Scholar] [CrossRef]
- Kaltschmidt, C.; Banz-Jansen, C.; Benhidjeb, T.; Beshay, M.; Förster, C.; Greiner, J.; Hamelmann, E.; Jorch, N.; Mertzlufft, F.; Pfitzenmaier, J.; et al. A role for NF-κB in organ specific cancer and cancer stem cells. Cancers 2019, 11, 655. [Google Scholar] [CrossRef]
- Li, J.; Xu, L.; Run, Z.-C.; Feng, W.; Liu, W.; Zhang, P.-J.; Li, Z. Multiple cytokine profiling in serum for early detection of gastric cancer. World J. Gastroenterol. 2018, 24, 2269–2278. [Google Scholar] [CrossRef]
- Kruger, D.; Yako, Y.Y.; Devar, J.; Lahoud, N.; Smith, M. Inflammatory cytokines and combined biomarker panels in pancreatic ductal adenocarcinoma: Enhancing diagnostic accuracy. PLoS ONE 2019, 14, e0221169. [Google Scholar] [CrossRef] [PubMed]
- Kampan, N.C.; Madondo, M.T.; Reynolds, J.; Hallo, J.; McNally, O.M.; Jobling, T.W.; Stephens, A.N.; Quinn, M.A.; Plebanski, M. Pre-operative sera interleukin-6 in the diagnosis of high-grade serous ovarian cancer. Sci. Rep. 2020, 10, 2213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrone, O.; Michelotti, A.; Paccagnella, M.; Montemurro, F.; Vandone, A.M.; Abbona, A.; Geuna, E.; Vanella, P.; De Angelis, C.; Nigro, C.L.; et al. Exploratory analysis of circulating cytokines in patients with metastatic breast cancer treated with eribulin: The TRANSERI-GONO (Gruppo Oncologico del Nord Ovest) study. ESMO Open 2020, 5, e000876. [Google Scholar] [CrossRef] [PubMed]
- Denaro, N.; Falletta, A.; Abbona, A.; Paccagnella, M.; Galizia, D.; Gammaitoni, L.; Fiorino, E.; De Zarlo, L.; Bossi, P.; Licitra, L.; et al. P-89 Cytokines behaviour during nivolumab treatment. A subgroup analysis of NIVACTOR study. Oral Oncol. 2021, 118, 8. [Google Scholar] [CrossRef]
- Wajant, H. The role of TNF in cancer. In Death Receptors and Cognate Ligands in Cancer; Springer: Cham, Switzerland, 2009; Volume 49, pp. 1–15. [Google Scholar]
- Pries, R.; Wollenberg, B. Cytokines in head and neck cancer. Cytokine Growth Factor Rev. 2006, 17, 141–146. [Google Scholar] [CrossRef]
- Carmeliet, P. VEGF as a Key Mediator of Angiogenesis in Cancer. Oncology 2005, 69 (Suppl. S3), 4–10. [Google Scholar] [CrossRef]
- Kumari, N.; Dwarakanath, B.S.; Das, A.; Bhatt, A.N. Role of interleukin-6 in cancer progression and therapeutic resistance. Tumor Biol. 2016, 37, 11553–11572. [Google Scholar] [CrossRef]
- Baggiolini, M.; Dewald, B.; Moser, B. Interleukin-8 and related chemotactic cytokines--CXC and CC chemokines. Adv. Immunol. 1994, 55, 97–179. [Google Scholar]
- Principe, S.; Zapater-Latorre, E.; Arribas, L.; Garcia-Miragall, E.; Bagan, J. Salivary IL-8 as a putative predictive biomarker of radiotherapy response in head and neck cancer patients. Clin. Oral Investig. 2022, 26, 437–448. [Google Scholar] [CrossRef]
- Mosman, T.R. Properties and functions of interleukin-10. Adv. Immunol. 1994, 56, 1–26. [Google Scholar]
- Bruchhage, K.-L.; Heinrichs, S.; Wollenberg, B.; Pries, R. IL-10 in the microenvironment of HNSCC inhibits the CpG ODN induced IFN-α secretion of pDCs. Oncol. Lett. 2018, 15, 3985–3990. [Google Scholar] [CrossRef] [PubMed]
- Solaymani-Mohammadi, S.; Eckmann, L.; Singer, S.M. Interleukin (IL)-21 in inflammation and immunity during parasitic diseases. Front. Cell. Infect. Microbiol. 2019, 9, 401. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Zhang, Q.; Xu, M.; Wang, L.; Chen, X.; Feng, Y.; Li, Y.; Zhang, X.; Cui, W.; Jia, X. CCL2-CCR2 axis recruits tumor associated macrophages to induce immune evasion through PD-1 signaling in esophageal carcinogenesis. Mol. Cancer 2020, 19, 41. [Google Scholar] [CrossRef] [Green Version]
- Attisano, L.; Wrana, J.L.; López-Casillas, F.; Massagué, J. TGF-beta receptors and actions. Biochim. Biophys. Acta 1994, 1222, 71–80. [Google Scholar] [CrossRef]
- Mito, I.; Takahashi, H.; Kawabata-Iwakawa, R.; Ida, S.; Tada, H.; Chikamatsu, K. Comprehensive analysis of immune cell enrichment in the tumor microenvironment of head and neck squamous cell carcinoma. Sci. Rep. 2021, 11, 16134. [Google Scholar] [CrossRef]
- Jiang, T.; Zhou, C.; Ren, S. Role of IL-2 in cancer immunotherapy. OncoImmunology 2016, 5, e1163462. [Google Scholar] [CrossRef] [Green Version]
- Thomas, G.R.; Chen, Z.; Enamorado, I.; Bancroft, C.; Van Waes, C. IL-12-and IL-2-induced tumor regression in a new murine model of oral squamous-cell carcinoma is promoted by expression of the CD80 co-stimulatory molecule and interferon-γ. Int. J. Cancer 2000, 86, 368–374. [Google Scholar] [CrossRef]
- Brown, M.A.; Hural, J. Functions of IL-4 and Control of Its Expression. Crit. Rev. Immunol. 2017, 37, 181–212. [Google Scholar] [CrossRef]
- Gitto, S.B.; Beardsley, J.M.; Nakkina, S.P.; Oyer, J.L.; Cline, K.A.; Litherland, S.A.; Copik, A.J.; Khaled, A.S.; Fanaian, N.; Arnoletti, J.P.; et al. Identification of a novel IL-5 signaling pathway in chronic pancreatitis and crosstalk with pancreatic tumor cells. Cell Commun. Signal. 2020, 18, 95. [Google Scholar] [CrossRef]
- Nguyen, K.G.; Vrabel, M.R.; Mantooth, S.M.; Hopkins, J.J.; Wagner, E.S.; Gabaldon, T.A.; Zaharoff, D.A. Localized Interleukin-12 for Cancer Immunotherapy. Front. Immunol. 2020, 11, 575597. [Google Scholar] [CrossRef] [PubMed]
- Mak, T.W.; Saunders, M.E. The Immune Response—Cytokines and Cytokine Receptors; Academic Press: Cambridge, MA, USA, 2006; pp. 463–516. [Google Scholar]
- Isvoranu, G.; Surcel, M.; Munteanu, A.N.; Bratu, O.G.; Ionita-Radu, F.; Neagu, M.T.; Chiritoiu-Butnaru, M. Therapeutic potential of interleukin-15 in cancer (Review). Exp. Ther. Med. 2021, 22, 675. [Google Scholar] [CrossRef] [PubMed]
- León, X.; Bothe, C.; García, J.; Parreño, M.; Alcolea, S.; Quer, M.; Vila, L.; Camacho, M. Expression of IL-1α correlates with distant metastasis in patients with head and neck squamous cell carcinoma. Oncotarget 2015, 6, 37398–37409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dranoff, G. Cytokines in cancer pathogenesis and cancer therapy. Nat. Cancer 2004, 4, 11–22. [Google Scholar] [CrossRef]
- Cohen, M.C.; Cohen, S. Cytokine Function: A Study in Biologic Diversity. Am. J. Clin. Pathol. 1996, 105, 589–598. [Google Scholar] [CrossRef] [Green Version]
- Lathers, D.M.; Young, M.R.I. Increased aberrance of cytokine expression in plasma of patients with more advanced squamous cell carcinoma of the head and neck. Cytokine 2004, 25, 220–228. [Google Scholar] [CrossRef]
- Liao, W.; Lin, J.-X.; Leonard, W.J. Interleukin-2 at the Crossroads of Effector Responses, Tolerance, and Immunotherapy. Immunity 2013, 38, 13–25. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.-P.; Yan, J.; Xu, J.; Pang, X.-H.; Chen, M.-S.; Li, L.; Wu, C.; Li, S.-P.; Zheng, L. Increased intratumoral IL-17-producing cells correlate with poor survival in hepatocellular carcinoma patients. J. Hepatol. 2009, 50, 980–989. [Google Scholar] [CrossRef]
- Bae, J.Y.; Kim, E.K.; Yang, D.H.; Zhang, X.; Park, Y.-J.; Lee, D.Y.; Che, C.M.; Kim, J. Reciprocal Interaction between Carcinoma-Associated Fibroblasts and Squamous Carcinoma Cells through Interleukin-1α Induces Cancer Progression. Neoplasia 2014, 16, 928–938. [Google Scholar] [CrossRef] [Green Version]
- Espinosa-Cotton, M.; Fertig, E.J.; Stabile, L.P.; Gaither-Davis, A.; Bauman, J.E.; Schmitz, S.; Gibson-Corley, K.N.; Cheng, Y.; Jensen, I.; Badovinac, V.P.; et al. A preliminary analysis of interleukin-1 ligands as potential predictive biomarkers of response to cetuximab. Biomark. Res. 2019, 7, 14. [Google Scholar] [CrossRef]
- Scheller, J.; Rose-John, S. Interleukin-6 and its receptor: From bench to bedside. Med. Microbiol. Immunol. 2006, 195, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Ralli, M.; Grasso, M.; Gilardi, A.; Ceccanti, M.; Messina, M.P.; Tirassa, P.; Fiore, M.; Altissimi, G.; Salzano, F.A.; De Vincentiis, M.; et al. The role of cytokines in head and neck squamous cell carcinoma: A review. Clin. Ter. 2020, 171, e268–e274. [Google Scholar] [CrossRef] [PubMed]
- Schett, G.; Elewaut, D.; McInnes, I.; Dayer, J.-M.; Neurath, M.F. How Cytokine Networks Fuel Inflammation: Toward a cytokine-based disease taxonomy. Nat. Med. 2013, 19, 822–824. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Descamps, G.; Seminerio, I.; Furgiuele, S.; Dequanter, D.; Mouawad, F.; Badoual, C.; Journe, F.; Saussez, S. HPV involvement in the tumor microenvironment and immune treatment in head and neck squamous cell carcinomas. Cancers 2020, 12, 1060. [Google Scholar] [CrossRef]
- Glentis, A.; Oertle, P.; Mariani, P.; Chikina, A.; El Marjou, F.; Attieh, Y.; Zaccarini, F.; Lae, M.; Loew, D.; Dingli, F.; et al. Cancer-associated fibroblasts induce metalloprotease-independent cancer cell invasion of the basement membrane. Nat. Commun. 2017, 8, 924. [Google Scholar] [CrossRef] [Green Version]
- Mao, X.; Xu, J.; Wang, W.; Liang, C.; Hua, J.; Liu, J.; Zhang, B.; Meng, Q.; Yu, X.; Shi, S. Crosstalk between cancer-associated fibroblasts and immune cells in the tumor microenvironment: New findings and future perspectives. Mol. Cancer 2021, 20, 131. [Google Scholar] [CrossRef]
- Semerano, L.; Minichiello, E.; Bessis, N.; Boissier, M.-C. Novel Immunotherapeutic Avenues for Rheumatoid Arthritis. Trends Mol. Med. 2016, 22, 214–229. [Google Scholar] [CrossRef]
- Al-Yahya, S.; Mahmoud, L.; Al-Zoghaibi, F.; Al-Tuhami, A.; Amer, H.; Almajhdi, F.N.; Polyak, S.J.; Khabar, K.S. Human cytokinome analysis for interferon response. J. Virol. 2015, 89, 7108–7119. [Google Scholar] [CrossRef] [Green Version]
- Wong, H.S.-C.; Chang, W.-C. Losses of cytokines and chemokines are common genetic features of human cancers: The somatic copy number alterations are correlated with patient prognoses and therapeutic resistance. OncoImmunology 2018, 7, e1468951. [Google Scholar] [CrossRef]
- Marzetti, E.; Picca, A.; Marini, F.; Biancolillo, A.; Coelho-Junior, H.J., Jr.; Gervasoni, J.; Bossola, M.; Cesari, M.; Onder, G.; Landi, F.; et al. Inflammatory signatures in older persons with physical frailty and sarcopenia: The frailty “cytokinome” at its core. Exp. Gerontol. 2019, 122, 129–138. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reference | Role/Action | Cytokine/Chemokine |
|---|---|---|
| [16,17] | TNF-β is secreted by T and B lymphocytes. It shares approximately 30% structural homology with TNF-α. It plays an important role in host defense against infection and the growth of some tumors. | TNF-β |
| [16] | As TNF-β, TNF-α exerts a wide variety of effects on diverse cell types through gene modulation of growth factors, cytokines, and transcription factors. In particular, like IL-1, TNF-α is a macrophage product and has the property to induce bone resorption, procoagulant activity, fibroblast growth, and expression of adhesion molecules on endothelial cells. TNF-α induces depletion of IFN-γ. Recently, TNF patterns were used to score HNSCC. High expression of TNF family members correlates with better responses. A favorable pattern is associated with p53 negative, not EGFR amplification, and HPV positive tumors. Additionally, TNF-α is correlated with CD4 and CD8 cell infiltrations. | TNF-α |
| [18] | VEGF is the key mediator of angiogenesis in cancer, in which it is upregulated by oncogene expression, a variety of growth factors, and hypoxia. It induces epithelial to mesenchymal transition. | VEGF |
| [19] | IL-6 is produced by macrophages and monocytes, fibroblasts, activated T lymphocytes, and endothelial cells (in response to IL-1 and TNF-α. IL-6 causes hepatocytes to synthesize plasma acute phase proteins and is a growth factor for malignant plasma cells and hematopoietic stem cells. | IL-6 |
| [20,21] | IL-8 is secreted by monocytes, fibroblasts, epithelial cells, astrocytes, keratinocytes, synovial cells, and various tumor cells. It has chemotactic receptor agonist property and causes neutrophils’ shape changes, chemotaxis, and exocytosis. IL-8 increases angiogenesis and correlates with high macrophage infiltrates. | IL-8 |
| [22,23] | IL-10 is secreted by activated T cells. It can inhibit both T cells and NK cells and macrophage function (reducing the secretion of cytokines from Th1 T-cell clones and macrophage functions, including microbicidal properties). It stimulates B cells. | IL-10 |
| [24] | IL-21 is secreted by activated T cells and NK cells; it regulates a wide range of immune cells, including T and B cells, NK cells, DCs, and macrophages, as well as non-immune cells, including epithelial cells and keratinocytes. It activates the Janus kinase (JAK1/3)-signal transducer and activator of transcription (STAT) signaling pathway. | IL-21 |
| [25] | CCL-2 recruits monocytes, memory T cells, and dendritic cells to the sites of inflammation produced by either tissue injury or infection. CCL-2 is implicated in the pathogenesis of several diseases characterized by monocytic infiltrates. It correlates to macrophage accumulation in cancer. | CCL-2 |
| [26,27] | TGF-β is able to induce both pro- and anti-tumoral effects. It affects proliferation and differentiation in a wide variety of cell types. It regulates extracellular matrix proteins and cell adhesion. It affects mesenchymal differentiation and is a potent chemotactic agent for various cell types, including monocytes and fibroblasts. It suppresses the activity of B and T lymphocytes, macrophages, and NK cells, regulating cytokine production by different cell types. | TGF-β |
| [28,29] | IL-2 is secreted by activated T cells, NK cells, and dendritic cells. It is known for its pleiotropic effect. It can promote T-cell and NK cell cytotoxicity activity and modulates T-cell differentiation programs in response to antigens. It has been used for the therapy of renal cell carcinoma and melanoma. In vitro IL-2 induces regression in a few HNSCC patients. | IL-2 |
| [30] | It is mainly secreted by activated T cells, NK cells, eosinophils, and basophils. Its activity is correlated to IL-13. It regulates antibody production, hematopoiesis, and inflammation and is also involved in developing effector T-cell responses. | IL-4 |
| [31] | IL-5 is produced mainly by lymphocytes, eosinophils monocytes, and macrophages. IL-5 stimulates antibody, eosinophil differentiation and proliferation and tumor cell migration and activation through STAT5 signaling. | IL-5 |
| [32] | IL-12 is a potent, pro-inflammatory cytokine. It has anti-tumor activity, and it counteracts IL-23 effect. It increases activation and cytotoxic capacities of T and NK cells and inhibits pro-tumoral macrophages and myeloid–derived suppressor cells. | IL-12 |
| [33] | IL-13 inhibits macrophage production of TNF, IL-1β, and pro-inflammatory chemokines, but can upregulate the synthesis of IL-12 by DCs and macrophages. IL-13 impairs antibody-dependent cytotoxicity. IL-13 stimulates B cell activation. IL-13 also promotes isotype switching to IgE and IgG1 and matrix expression (VCAM-1). | IL-13 |
| [34] | IL-15 is an inflammatory cytokine. It is secreted primarily by monocytes and macrophages. It stimulates TNF-α, IL-1β, inflammatory chemokines, T and B cells, and NK cells. It is regulated post-transcriptionally at the levels of translation and intracellular trafficking. | IL-15 |
| [35] | IL-1 stimulates CAFs, which produce CXCL1, CXCL8, and MMP-1. IL-1β increases neutrophils to the TME, and neutrophil accumulation has been related to poor outcomes in HNSCC. IL-12 stimulates VEGF and recruits T regulatory cells. | IL-1β |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denaro, N.; Solinas, C.; Garrone, O.; Cauchi, C.; Ruatta, F.; Wekking, D.; Abbona, A.; Paccagnella, M.; Merlano, M.C.; Lo Nigro, C. The Role of Cytokinome in the HNSCC Tumor Microenvironment: A Narrative Review and Our Experience. Diagnostics 2022, 12, 2880. https://doi.org/10.3390/diagnostics12112880
Denaro N, Solinas C, Garrone O, Cauchi C, Ruatta F, Wekking D, Abbona A, Paccagnella M, Merlano MC, Lo Nigro C. The Role of Cytokinome in the HNSCC Tumor Microenvironment: A Narrative Review and Our Experience. Diagnostics. 2022; 12(11):2880. https://doi.org/10.3390/diagnostics12112880
Chicago/Turabian StyleDenaro, Nerina, Cinzia Solinas, Ornella Garrone, Carolina Cauchi, Fiorella Ruatta, Demi Wekking, Andrea Abbona, Matteo Paccagnella, Marco Carlo Merlano, and Cristiana Lo Nigro. 2022. "The Role of Cytokinome in the HNSCC Tumor Microenvironment: A Narrative Review and Our Experience" Diagnostics 12, no. 11: 2880. https://doi.org/10.3390/diagnostics12112880
APA StyleDenaro, N., Solinas, C., Garrone, O., Cauchi, C., Ruatta, F., Wekking, D., Abbona, A., Paccagnella, M., Merlano, M. C., & Lo Nigro, C. (2022). The Role of Cytokinome in the HNSCC Tumor Microenvironment: A Narrative Review and Our Experience. Diagnostics, 12(11), 2880. https://doi.org/10.3390/diagnostics12112880