
Use of POCUS in Chest Pain and Dyspnea in Emergency Department: What Role Could It Have?

 ,
,  ,
, 
 ,
,
Abstract
:1. POCUS in Chest Pain: What Role Could It Have?
2. Cardiac Causes
3. Chest Pain and Its Respiratory Causes
4. Abdominal Causes
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gleeson, T.; Blehar, D. Point-of-Care Ultrasound in Trauma. Semin. Ultrasound CT MR 2018, 39, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Sahlani, L.; Thompson, L.; Vira, A.; Panchal, A.R. Bedside ultrasound procedures: Musculoskeletal and non-musculoskeletal. Eur. J. Trauma Emerg. Surg. 2016, 42, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Perera, P.; Mailhot, T.; Riley, D.; Mandavia, D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically lll. Emerg. Med. Clin. N. Am. 2010, 28, 29–56. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.J.; Jonas, C.E.; Carter, R.E. Point-of-Care Ultrasonography. Am. Fam. Physician 2020, 101, 275–285. [Google Scholar] [PubMed]
- Wong, A.; Vieillard-Baron, A.; Malbrain, M. Emergency bedside ultrasound: Benefits as well as caution—Part 1. General. Curr. Opin. Crit. Care 2019, 25, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Lenfant, C. Chest pain of cardiac and noncardiac origin. Metabolism 2010, 59 (Suppl. 1), S41–S46. [Google Scholar] [CrossRef]
- Chang, A.M.; Fischman, D.L.; Hollander, J.E. Evaluation of Chest Pain and Acute Coronary Syndromes. Cardiol. Clin. 2018, 36, 1–12. [Google Scholar] [CrossRef]
- Rushton, S.; Carman, M.J. Chest Pain: If It Is Not the Heart, What Is It? Nurs. Clin. N. Am. 2018, 53, 421–431. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [Green Version]
- Tang, A.; Euerle, B. Emergency department ultrasound and echocardiography. Emerg. Med. Clin. N. Am. 2005, 23, 1179–1194. [Google Scholar] [CrossRef]
- Morello, F.; Santoro, M.; Fargion, A.T.; Grifoni, S.; Nazerian, P. Diagnosis and management of acute aortic syndromes in the emergency department. Intern. Emerg. Med. 2021, 16, 171–181. [Google Scholar] [CrossRef]
- Colony, M.D.; Edwards, F.; Kellogg, D. Ultrasound assisted evaluation of chest pain in the emergency department. Am. J. Emerg. Med. 2018, 36, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Mancusi, C.; Carlino, M.V.; Sforza, A. Point-of-care ultrasound with pocket-size devices in emergency department. Echocardiography 2019, 36, 1755–1764. [Google Scholar] [CrossRef] [PubMed]
- Chenkin, J.; Atzema, C.L. Contemporary Application of Point-of-Care Echocardiography in the Emergency Department. Can. J. Cardiol. 2018, 34, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Azarbal, A.; LeWinter, M.M. Pericardial Effusion. Cardiol. Clin. 2017, 35, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Ciozda, W.; Kedan, I.; Kehl, D.W.; Zimmer, R.; Khandwalla, R.; Kimchi, A. The efficacy of sonographic measurement of inferior vena cava diameter as an estimate of central venous pressure. Cardiovasc. Ultrasound 2016, 14, 33. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [Green Version]
- Darwish, O.S.; Mahayni, A.; Kataria, S.; Zuniga, E.; Zhang, L.; Amin, A. Diagnosis of Acute Heart Failure Using Inferior Vena Cava Ultrasound: Systematic Review and Meta-analysis. J. Ultrasound Med. 2020, 39, 1367–1378. [Google Scholar] [CrossRef]
- Orso, D.; Paoli, I.; Piani, T.; Cilenti, F.L.; Cristiani, L.; Guglielmo, N. Accuracy of Ultrasonographic Measurements of Inferior Vena Cava to Determine Fluid Responsiveness: A Systematic Review and Meta-Analysis. J. Intensive Care Med. 2020, 35, 354–363. [Google Scholar] [CrossRef]
- Soar, J.; Böttiger, B.W.; Carli, P.; Couper, K.; Deakin, C.D.; Djärv, T.; Lott, C.; Olasveengen, T.; Paal, P.; Pellis, T.; et al. European Resuscitation Council Guidelines 2021: Adult advanced life support. Resuscitation 2021, 161, 115–151. [Google Scholar] [CrossRef]
- Balderston, J.R.; You, A.X.; Evans, D.P.; Taylor, L.A.; Gertz, Z.M. Feasibility of focused cardiac ultrasound during cardiac arrest in the emergency department. Cardiovasc. Ultrasound 2021, 19, 19. [Google Scholar] [CrossRef] [PubMed]
- Whitson, M.R.; Mayo, P.H. Ultrasonography in the emergency department. Crit. Care 2016, 20, 227. [Google Scholar] [CrossRef] [Green Version]
- Amini, R.; Stolz, L.A.; Kartchner, J.Z.; Thompson, M.; Stea, N.; Hawbaker, N.; Joshi, R.; Adhikari, S. Bedside echo for chest pain: An algorithm for education and assessment. Adv. Med. Educ. Pract. 2016, 7, 293–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy Hall, M.; Coffey, E.C.; Herbst, M.; Liu, R.; Pare, J.R.; Andrew Taylor, R.; Thomas, S.; Moore, C.L. The “5Es” of emergency physician-performed focused cardiac ultrasound: A protocol for rapid identification of effusion, ejection, equality, exit, and entrance. Acad. Emerg. Med. 2015, 22, 583–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrestha, A.P.; Shrestha, R.; Shrestha, S.K.; Pradhan, A. Prevalence of Dyspnea among Patients Attending the Emergency Department of a Tertiary Care Hospital: A Descriptive Cross-sectional Study. JNMA J. Nepal. Med. Assoc. 2019, 57, 302–306. [Google Scholar] [CrossRef] [Green Version]
- Bowra, J.; Duong, M.T. Point-of-care ultrasound in emergency department: Tips, tricks and controversies. Emerg. Med. Australas. 2020, 32, 155–157. [Google Scholar] [CrossRef]
- De Luca, C.; Valentino, M.; Rimondi, M.R.; Branchini, M.; Baleni, M.C.; Barozzi, L. Use of chest sonography in acute-care radiology. J. Ultrasound 2008, 11, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Pirozzi, C.; Numis, F.G.; Pagano, A.; Melillo, P.; Copetti, R.; Schiraldi, F. Immediate versus delayed integrated point-of-care-ultrasonography to manage acute dyspnea in the emergency department. Crit. Ultrasound J. 2014, 6, 5. [Google Scholar] [CrossRef] [Green Version]
- Hendin, A.; Koenig, S.; Millington, S.J. Better With Ultrasound: Thoracic Ultrasound. Chest 2020, 158, 2082–2089. [Google Scholar] [CrossRef]
- Wallbridge, P.; Steinfort, D.; Tay, T.R.; Irving, L.; Hew, M. Diagnostic chest ultrasound for acute respiratory failure. Respir. Med. 2018, 141, 26–36. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.K.; Joo, D.A.; McRae, A.D.; Takwoingi, Y.; Premji, Z.A.; Lang, E.; Wakai, A. Chest ultrasonography versus supine chest radiography for diagnosis of pneumothorax in trauma patients in the emergency department. Cochrane Database Syst. Rev. 2020, 7, Cd013031. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, A.; Yousefifard, M.; Kazemi, H.M.; Rasouli, H.R.; Asady, H.; Jafari, A.M.; Hosseini, M. Diagnostic Accuracy of Chest Ultrasonography versus Chest Radiography for Identification of Pneumothorax: A Systematic Review and Meta-Analysis. Tanaffos 2014, 13, 29–40. [Google Scholar] [PubMed]
- Eibenberger, K.L.; Dock, W.I.; Ammann, M.E.; Dorffner, R.; Hörmann, M.F.; Grabenwöger, F. Quantification of pleural effusions: Sonography versus radiography. Radiology 1994, 191, 681–684. [Google Scholar] [CrossRef]
- Maw, A.M.; Hassanin, A.; Ho, P.M.; McInnes, M.D.F.; Moss, A.; Juarez-Colunga, E.; Soni, N.J.; Miglioranza, M.H.; Platz, E.; DeSanto, K.; et al. Diagnostic Accuracy of Point-of-Care Lung Ultrasonography and Chest Radiography in Adults with Symptoms Suggestive of Acute Decompensated Heart Failure: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e190703. [Google Scholar] [CrossRef]
- Ibitoye, B.O.; Idowu, B.M.; Ogunrombi, A.B.; Afolabi, B.I. Ultrasonographic quantification of pleural effusion: Comparison of four formulae. Ultrasonography 2018, 37, 254–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montoya, J.; Stawicki, S.P.; Evans, D.C.; Bahner, D.P.; Sparks, S.; Sharpe, R.P.; Cipolla, J. From FAST to E-FAST: An overview of the evolution of ultrasound-based traumatic injury assessment. Eur. J. Trauma Emerg. Surg. 2016, 42, 119–126. [Google Scholar] [CrossRef]
- Staub, L.J.; Biscaro, R.R.M.; Kaszubowski, E.; Maurici, R. Chest ultrasonography for the emergency diagnosis of traumatic pneumothorax and haemothorax: A systematic review and meta-analysis. Injury 2018, 49, 457–466. [Google Scholar] [CrossRef]
- Wang, Y.; Shen, Z.; Lu, X.; Zhen, Y.; Li, H. Sensitivity and specificity of ultrasound for the diagnosis of acute pulmonary edema: A systematic review and meta-analysis. Med. Ultrason. 2018, 1, 32–36. [Google Scholar] [CrossRef]
- Doherty, S. Pulmonary embolism An update. Aust. Fam. Physician 2017, 46, 816–820. [Google Scholar]
- Estrada, Y.M.R.M.; Oldham, S.A. CTPA as the gold standard for the diagnosis of pulmonary embolism. Int. J. Comput. Assist. Radiol. Surg. 2011, 6, 557–563. [Google Scholar] [CrossRef]
- Nazerian, P.; Vanni, S.; Volpicelli, G.; Gigli, C.; Zanobetti, M.; Bartolucci, M.; Ciavattone, A.; Lamorte, A.; Veltri, A.; Fabbri, A.; et al. Accuracy of point-of-care multiorgan ultrasonography for the diagnosis of pulmonary embolism. Chest 2014, 145, 950–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orso, D.; Guglielmo, N.; Copetti, R. Lung ultrasound in diagnosing pneumonia in the emergency department: A systematic review and meta-analysis. Eur. J. Emerg. Med. 2018, 25, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Giannella, L.; Catania, A.; Provaroni, A.; Cerami, L.B.; Chesi, G. The value of chest ultrasound along with inflammatory biomarkers in the management of pneumonia in a non-compliant pregnant woman. J. Matern. Fetal Neonatal Med. 2012, 25, 1830–1832. [Google Scholar] [CrossRef] [PubMed]
- Piccioni, A.; Franza, L.; Rosa, F.; Cicchinelli, S.; Saviano, A.; Valletta, F.; de Cunzo, T.; Zanza, C.; Covino, M.; Ojetti, V.; et al. Patient safety recommendations and management in patients with COVID-19 pneumonia suspicion: A retrospective study. Clin. Ter. 2021, 172, 225–230. [Google Scholar] [CrossRef]
- Zanforlin, A.; Tursi, F. How Is COVID-19 Changing Lung Ultrasound? A Survey by the Thoracic Ultrasound Academy. J. Ultrasound Med. 2021, 40, 417–418. [Google Scholar] [CrossRef]
- Smith, M.J.; Hayward, S.A.; Innes, S.M.; Miller, A.S.C. Point-of-care lung ultrasound in patients with COVID-19—A narrative review. Anaesthesia 2020, 75, 1096–1104. [Google Scholar] [CrossRef] [Green Version]
- Jackson, K.; Butler, R.; Aujayeb, A. Lung ultrasound in the COVID-19 pandemic. Postgrad. Med. J. 2021, 97, 34–39. [Google Scholar] [CrossRef]
- Xue, H.; Li, C.; Cui, L.; Tian, C.; Li, S.; Wang, Z.; Liu, C.; Ge, Q. M-BLUE protocol for coronavirus disease-19 (COVID-19) patients: Interobserver variability and correlation with disease severity. Clin. Radiol. 2021, 76, 379–383. [Google Scholar] [CrossRef]
- Gil-Rodríguez, J.; de Rojas, J.P.; Aranda-Laserna, P.; Benavente-Fernández, A.; Martos-Ruiz, M.; Peregrina-Rivas, J.A.; Guirao-Arrabal, E. Ultrasound findings of lung ultrasonography in COVID-19: A systematic review. Eur. J. Radiol. 2022, 148, 110156. [Google Scholar] [CrossRef]
- Zieleskiewicz, L.; Markarian, T.; Lopez, A.; Taguet, C.; Mohammedi, N.; Boucekine, M.; Baumstarck, K.; Besch, G.; Mathon, G.; Duclos, G.; et al. Comparative study of lung ultrasound and chest computed tomography scan in the assessment of severity of confirmed COVID-19 pneumonia. Intensive Care Med. 2020, 46, 1707–1713. [Google Scholar] [CrossRef]
- Song, G.; Qiao, W.; Wang, X.; Yu, X. Association of Lung Ultrasound Score with Mortality and Severity of COVID-19: A Meta-Analysis and Trial Sequential Analysis. Int. J. Infect. Dis. 2021, 108, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Boccardi, L.; Bisconti, C.; Camboni, C.; Chieffi, M.; Putini, R.L.; Macali, L.; Spina, A.; Lukic, V.; Ciferri, E. Chest pain in women: A multicenter study of the National Association of Hospital Cardiologists (ANMCO) of the Lazio Region. Ital. Heart J. Suppl. 2002, 3, 1034–1041. [Google Scholar] [PubMed]
- Ohtani, N.; Kiyokawa, K.; Asada, H.; Kawakami, T. Stanford type A acute dissection developing acute myocardial infarction. Jpn. J. Thorac. Cardiovasc. Surg. 2000, 48, 69–72. [Google Scholar] [CrossRef]
- Cakmakci, E.; Ucan, B.; Colak, B.; Cinar, H.G. Novel Sonographic Clues for Diagnosis of Antral Gastritis and Helicobacter pylori Infection. J. Ultrasound Med. 2014, 33, 1605–1610. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, A.; Sadreddini, M.; Sepehrvand, N.; Pedram, A.; Yarmohammadi, N.; Mladkova, N.; Ghasemi-Rad, M. Lack of utility of transabdominal ultrasound in the detection of gastroesophageal reflux disease-induced esophagitis in comparison with endoscopy. Ultrasound Q. 2011, 27, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Mádi-Szabó, L.; Kocsis, G. Examination of gastroesophageal reflux by transabdominal ultrasound: Can a slow, trickling form of reflux be responsible for reflux esophagitis? Can. J. Gastroenterol. 2000, 14, 588–592. [Google Scholar] [CrossRef] [Green Version]
- Derr, C.; Drake, J.M. Esophageal rupture diagnosed with bedside ultrasound. Am. J. Emerg. Med. 2012, 30, 2093.e1–2093.e3. [Google Scholar] [CrossRef]
- Coppolino, F.F.; Gatta, G.; Di Grezia, G.; Reginelli, A.; Iacobellis, F.; Vallone, G.; Giganti, M.; Genovese, E.A. Gastrointestinal perforation: Ultrasonographic diagnosis. Crit. Ultrasound J. 2013, 5, S4. [Google Scholar] [CrossRef] [Green Version]
- Gustafsson, C.; McNicholas, A.; Sondén, A.; Törngren, S.; Järnbert-Pettersson, H.; Lindelius, A. Accuracy of Surgeon-Performed Ultrasound in Detecting Gallstones: A Validation Study. World J. Surg. 2016, 40, 1688–1694. [Google Scholar] [CrossRef]
- Littlefield, A.; Lenahan, C. Cholelithiasis: Presentation and Management. J. Midwifery Womens Health 2019, 64, 289–297. [Google Scholar] [CrossRef]
- Borzellino, G.; Motton, A.P.M.; Minniti, F.; Montemezzi, S.; Tomezzoli, A.; Genna, M. Sonographic diagnosis of acute cholecystitis in patients with symptomatic gallstones. J. Clin. Ultrasound 2016, 44, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Burrowes, D.P.; Choi, H.H.; Rodgers, S.K.; Fetzer, D.T.; Kamaya, A. Utility of ultrasound in acute pancreatitis. Abdom. Radiol. 2020, 45, 1253–1264. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, A.; Braun, M.M.; Khayat, M. Kidney Disease: Kidney Stones. FP Essent. 2021, 509, 33–38. [Google Scholar] [PubMed]
- Hanita, M. Self-report measures of patient utility: Should we trust them? J. Clin. Epidemiol. 2000, 53, 469–476. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IVC Diameter | Inspiratory Collapse | Right Atrium Pressure |
|---|---|---|
| <2.1 cm | >50% | 3 mm Hg (range 0–5 mm Hg) |
| >2.1 cm | <50% | 15 mm Hg (range 10–20 mm Hg) |
| Uses of Cardiac POCUS in the Emergency Department | |
|---|---|
| Disease | Assessment |
| Pulmonary embolism | Ejection fraction |
| Heart failure | Inferior vena cava filling |
| Aortic pathologies | |
| Pericardial effusion and cardiac tamponade | |
| Findings | Description | Interpretation |
| Physiological findings | ||
| A-Lines | Hyperechoic horizontal lines parallel to the pleural line | Normal findings |
| Sliding sign | Physiological sliding of the pleural layers during respiratory acts | Normal findings, excluding the presence of PNX |
| Pathological findings | ||
| Liver sign | The lung has the same consistency as the liver | Consolidation |
| B-Lines (Figure 4) | Vertical artifacts perpendicular to the pleural line | Presence of interstitial infiltrate, suggestive of acute pulmonary edema or COVID-19 pneumonia |
| Signs in motion mode (M-mode) | ||
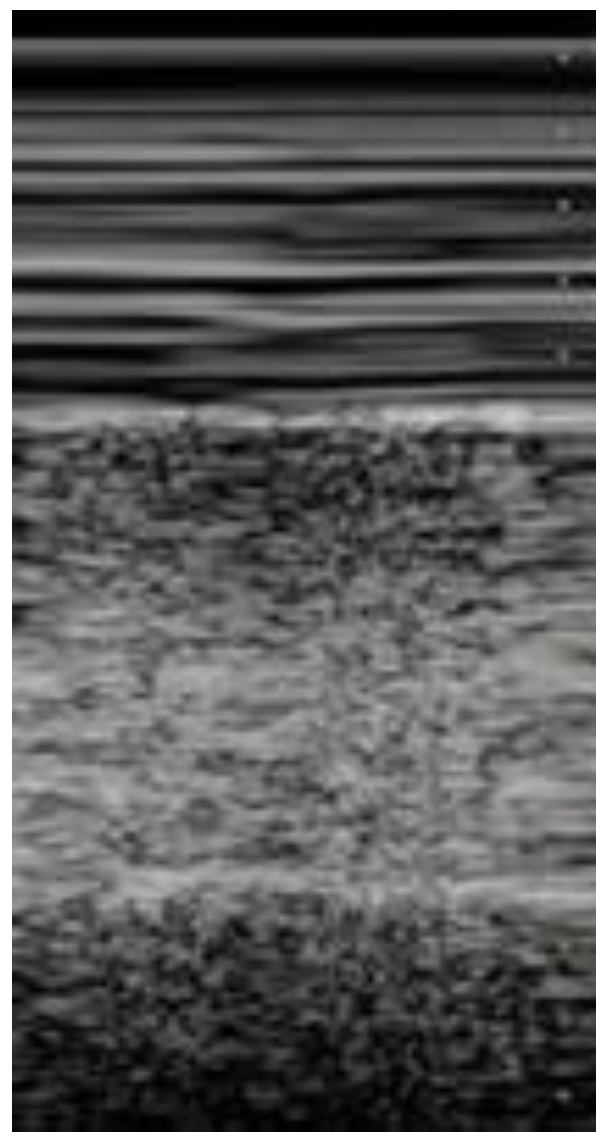
| Seashore sign (Figure 5) | The pleura is represented by horizontal artifacts and the underlying lung has a sandy pattern. | Normal finding |
| Barcode sign (sign of the stratosphere) (Figure 6) | Both the pleura and the lung appear as horizontal artifacts | PNX |
| Clinical Pattern | Ultrasound Findings |
|---|---|
| PNX | Absence of B-lines and lung sliding, barcode/stratosphere sign in M-mode |
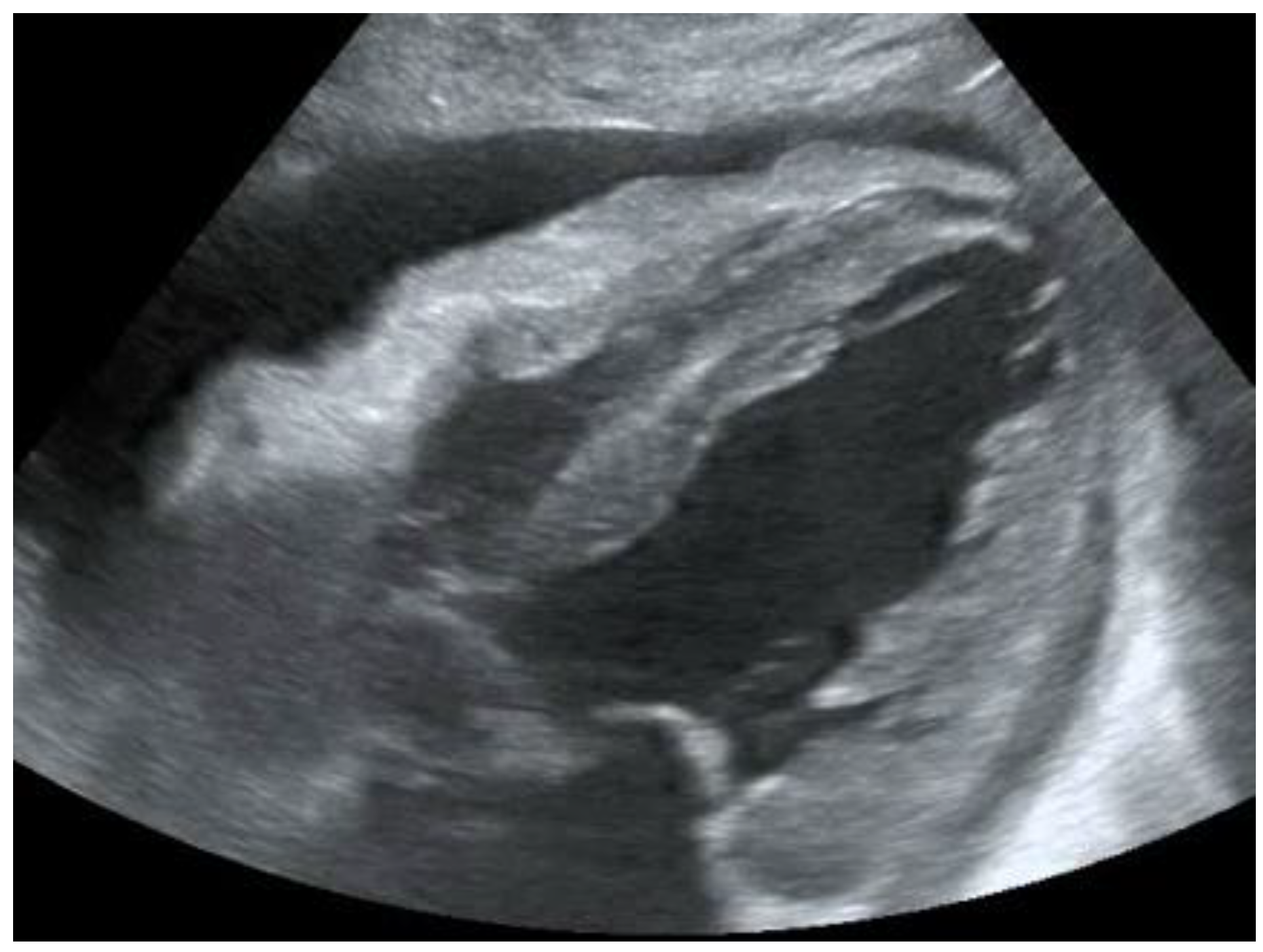
| Pleural effusion | Detection of hypoechoic material in the pleural cavity (Figure 7) |
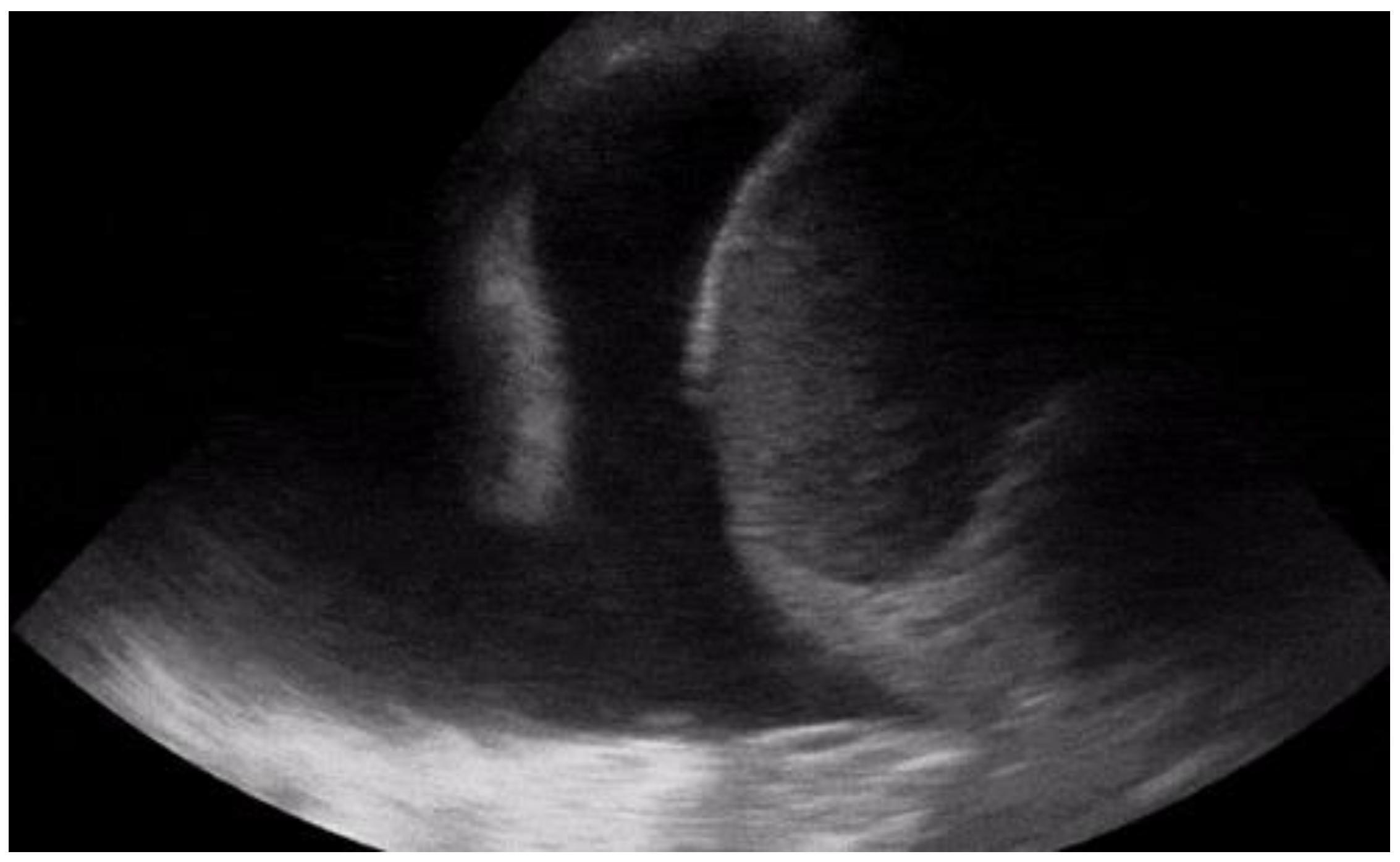
| Pneumonia | Consolidation, air bronchogram sign (Figure 8) |
| Pulmonary embolism | Dilation of the right heart cavities or the presence of blood clots within them, and the presence of deep vein thrombosis |
| Acute pulmonary edema | Presence of diffuse B-lines (Figure 9) |
| Applications of Thoracic Ultrasound |
|---|
| Acute pulmonary edema Pneumothorax Hemothorax Pleural effusion Pulmonary embolism COVID-19 Exacerbation of asthma and COPD |
| Clinical Pattern | Ultrasound Findings |
|---|---|
| Gastritis | Thickening of antral walls and mucosal layers |
| Oesophagitis | Thickening of oesophageal wall; slow, trickling reflux of gastric content |
| Oesophageal perforation | Non-visualization of the heart on ultrasound, free fluid may also be present in the upper abdominal quadrants |
| Gastric perforation | Free fluid in the upper abdominal quadrants; hyper echogenicity of the right anterior extrarenal tissue (renal rind sign) |
| Cholelithiasis | Gallstone with a shadow cone; possible bile duct dilatation. |
| Cholecystitis | Gallbladder distension, wall oedema, and pericholecystic fluid collection. |
| Pancreatitis | Enlarged and oedematous pancreas, peripancreatic fluid collections, venous thrombosis, arterial pseudoaneurysm, the presence of gallstones, or dilatation of the biliary tree |
| Nephrolithiasis | Kidney stone with a shadow cone, dilatation above the stone. |
| Patients Who Came to Emergency Department for Chest Pain and Dyspnea | |
|---|---|
| Diagnostic Suspicion | Role of Diagnostic Tests and POCUS |
| Acute coronary syndrome (ACS) | Performing ECG and troponin assay |
| Aortic dissection | The gold standard is represented by CT angiography or trans-oesophageal echocardiography, while POCUS can help in cases where these tests cannot be performed |
| Pericardial effusion and cardiac tamponade | POCUS is one of the tests that allows diagnosis |
| Pulmonary embolism | The gold standard is represented by CT angiography, and POCUS can select which patients should undergo this examination |
| Acute pulmonary edema | POCUS is one of the tests that allows diagnosis |
| PNX | Chest X-ray is the first-level examination, and thoracic ultrasound is quite accurate. E-FAST is the first choice for the trauma patient. |
| Pleural effusion or hemothorax | Chest X-ray is the first-level examination, and thoracic ultrasound is quite accurate. E-FAST is the first choice for the trauma patient. |
| Pneumonia | Blood tests with inflammatory indices and a chest X-ray comprise the first level of examination, and thoracic ultrasound is quite accurate. |
| COVID-19 pneumonia | The findings of ultrasound changes suggestive of infection can be isolated early; chest CT remains the most accurate examination. |
| Exacerbation of asthma and COPD | In this case, the finding of a normal type A pattern without pleural or parenchymal changes can be suggestive of these pathologies. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piccioni, A.; Franza, L.; Rosa, F.; Manca, F.; Pignataro, G.; Salvatore, L.; Simeoni, B.; Candelli, M.; Covino, M.; Franceschi, F. Use of POCUS in Chest Pain and Dyspnea in Emergency Department: What Role Could It Have? Diagnostics 2022, 12, 1620. https://doi.org/10.3390/diagnostics12071620
Piccioni A, Franza L, Rosa F, Manca F, Pignataro G, Salvatore L, Simeoni B, Candelli M, Covino M, Franceschi F. Use of POCUS in Chest Pain and Dyspnea in Emergency Department: What Role Could It Have? Diagnostics. 2022; 12(7):1620. https://doi.org/10.3390/diagnostics12071620
Chicago/Turabian StylePiccioni, Andrea, Laura Franza, Federico Rosa, Federica Manca, Giulia Pignataro, Lucia Salvatore, Benedetta Simeoni, Marcello Candelli, Marcello Covino, and Francesco Franceschi. 2022. "Use of POCUS in Chest Pain and Dyspnea in Emergency Department: What Role Could It Have?" Diagnostics 12, no. 7: 1620. https://doi.org/10.3390/diagnostics12071620
APA StylePiccioni, A., Franza, L., Rosa, F., Manca, F., Pignataro, G., Salvatore, L., Simeoni, B., Candelli, M., Covino, M., & Franceschi, F. (2022). Use of POCUS in Chest Pain and Dyspnea in Emergency Department: What Role Could It Have? Diagnostics, 12(7), 1620. https://doi.org/10.3390/diagnostics12071620