
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Post-COVID Syndrome: A Common Neuroimmune Ground?
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
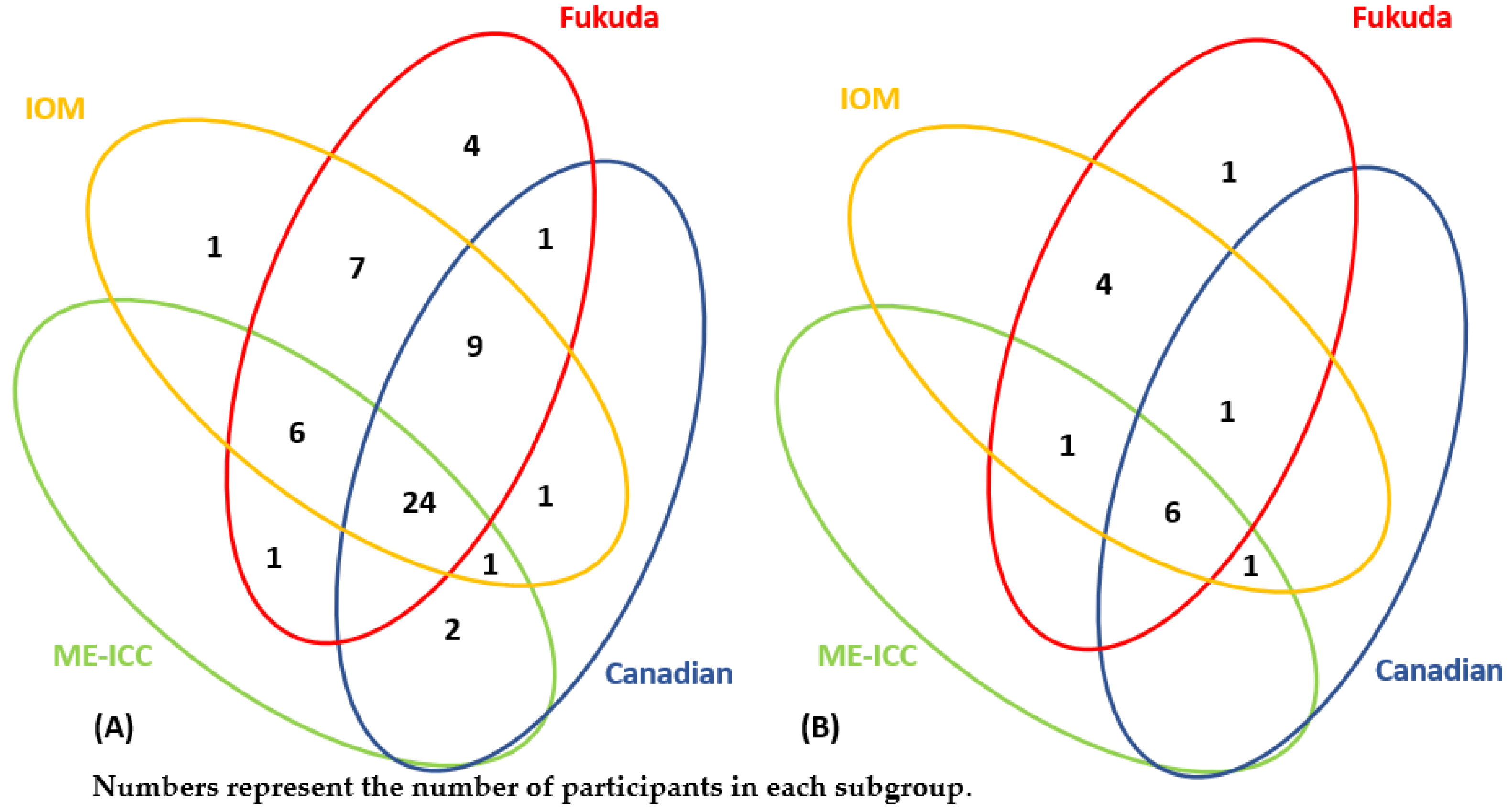
- A cohort of patients from 18 to 75 years old who met ≥1 of the 4 most commonly used ME/CFS case definitions (the Fukuda et al. (1994) CFS criteria [13], the Canadian ME/CFS criteria [14], the Myalgic Encephalomyelitis International Consensus Criteria (ME-ICC) [15], and the Institute of Medicine criteria), in whom the onset of the disease was not associated with COVID-19;
- A cohort of patients from 18 to 75 years old who met ≥1 of the 4 most commonly used ME/CFS case definitions and those symptoms developed following COVID-19;
- Control group (healthy volunteers from 18 to 75 years old).
- The presence of any symptoms (including chronic fatigue) before COVID-19.
- Complaints of chronic fatigue
- In cases of previous viral infections, including COVID-19 <4 weeks after recovery to the moment of enrollment in the study.
2.2. Symptom Assessment Tools
The ME/CFS Symptom Questionnaire DePaul Symptoms Qustionnaire-2
2.3. Patient Recruitment
2.4. Active Orthostatic Test
2.5. Assessment of Microcirculation
2.6. Statistical Analyses
3. Results
3.1. Participants
3.2. Clinical and Anamnestic Characteristics of ME/CFS as Neuroimmune Disorder
3.3. Mental Health Screening in Patients with ME/CFS and Assessment of the Relationship between Mental Health and Severity of Fatigue
3.4. Assessment of the Immune Status in Patients with ME/CFS
3.5. Identification of Autonomic Dysfunction during an Active Orthostatic Test
3.6. Assessment of the Dynamic Characteristics of Microcirculation with Laser Doppler Flowmetry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bested, A.C.; Marshall, L.M. Review of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: An evidence-based approach to diagnosis and management by clinicians. Rev. Environ. Health 2015, 30, 223–249. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.J.; Ahn, Y.C.; Jang, E.S.; Lee, S.W.; Lee, S.H.; Son, C.G. Systematic review and meta-analysis of the prevalence of chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). J. Transl. Med. 2020, 18, 100. [Google Scholar] [CrossRef] [PubMed]
- Bakken, I.; Tveito, K.; Gunnes, N.; Ghaderi, S.; Stoltenberg, C.; Trogstad, L.; Åberg, S.E.H.; Magnus, P. Two age peaks in the incidence of chronic fatigue syndrome/myalgic encephalomyelitis: A population-based registry study from Norway 2008-2012. BMC Med. 2014, 12, 167. [Google Scholar] [CrossRef] [Green Version]
- Słomko, J.; Newton, J.L.; Kujawski, S.; Tafil-Klawe, M.; Klawe, J.; Staines, D.; Marshall-Gradisnik, S.; Zalewski, P. Prevalence and characteristics of chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) in Poland: A cross-sectional study. BMJ Open 2019, 9, e023955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cullinan, J.; Pheby, D.F.H.; Araja, D.; Berkis, U.; Brenna, E.; de Korwin, J.-D.; Gitto, L.; Hughes, D.A.; Hunter, R.M.; Trepel, D.; et al. Perceptions of European ME/CFS Experts Concerning Knowledge and Understanding of ME/CFS among Primary Care Physicians in Europe: A Report from the European ME/CFS Research Network (EUROMENE). Medicina 2021, 57, 208. [Google Scholar] [CrossRef] [PubMed]
- Poenaru, S.; Abdallah, S.J.; Corrales-Medina, V.; Cowan, J. COVID-19 and post-infectious myalgic encephalomyelitis/chronic fatigue syndrome: A narrative review. Ther, Adv. Infect. Dis. 2021, 8, 20499361211009385. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.L.; Weitzer, D.J. Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)-A Systemic Review and Comparison of Clinical Presentation and Symptomatology. Medicina 2021, 57, 418. [Google Scholar] [CrossRef]
- Mackay, A. A Paradigm for Post-COVID-19 Fatigue Syndrome Analogous to ME/CFS. Front. Neurol. 2021, 12, 1334. [Google Scholar] [CrossRef]
- Bornstein, S.R.; Voit-Bak, K.; Donate, T.; Rodionov, R.N.; Gainetdinov, R.R.; Tselmin, S.; Kanczkowski, W.; Müller, G.M.; Achleitner, M.; Wang, J.; et al. Chronic post-COVID-19 syndrome and chronic fatigue syndrome: Is there a role for extracorporeal apheresis? Mol. Psychiatry 2021, 27, 34–37. [Google Scholar] [CrossRef]
- Komaroff, A.L.; Lipkin, W.I. Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of postacute COVID-19 syndrome. Trends Mol. Med. 2021, in press. [Google Scholar] [CrossRef]
- Lawn, T.; Kumar, P.; Knight, B.; Sharpe, M.; White, P.D. Psychiatric misdiagnoses in patients with chronic fatigue syndrome. JRSM Short Rep. 2010, 1, 28. [Google Scholar] [CrossRef] [Green Version]
- NICE. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19 (NG188); National Institute for Health and Care Excellence: London, UK, 2020. [Google Scholar]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, B.M.; Jain, A.K.; De Meirleir, K.L.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor-Henry, P.; Joshi, P.; Powles, A.C.P.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Chronic Fatigue Syndr. 2003, 11, 7–115. [Google Scholar] [CrossRef]
- Carruthers, B.M.; Van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bateman, L.; Dowell, T.; Komaroff, A.; Klimas, N.; Natelson, B.; Podell, R.; Ruhoy, I.; Dempsey, T.; Natelson, B.; Vera-Nunez, M.; et al. Diagnosing and Treating Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS); USA ME/CFS Clinician Coalition: Salt Lake City, UT, USA, 2019. [Google Scholar]
- Bedree, H.; Sunnquist, M.; Jason, L.A. The DePaul Symptom Questionnaire-2: A validation study. Fatigue Biomed. Health Behav. 2019, 7, 166–179. [Google Scholar] [CrossRef]
- Jason, L.A.; Sunnquist, M. The development of the DePaul Symptom Questionnaire: Original, expanded, brief, and pediatric versions. Front. Pediatr. 2018, 6, 330. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Bateman, L.; Bested, A.C.; Bonilla, H.F.; Chheda, B.V.; Chu, L.; Curtin, J.M.; Dempsey, T.T.; Dimmock, M.E.; Dowell, T.G.; Felsenstein, D.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management. Mayo Clin. Proc. 2021, 96, 2861–2878. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Fanciulli, A.; Campese, N.; Wenning, G.K. The Schellong test: Detecting orthostatic blood pressure and heart rate changes in German-speaking countries. Clin. Auton. Res. 2019, 29, 363–366. [Google Scholar] [CrossRef]
- Raj, S.R.; Guzman, J.C.; Harvey, P.; Richer, L.; Schondorf, R.; Seifer, C.; Thibodeau-Jarry, N.; Sheldon, R.S. Canadian Cardiovascular Society Position Statement on Postural Orthostatic Tachycardia Syndrome (POTS) and Related Disorders of Chronic Orthostatic Intolerance. Can. J. Cardiol. 2020, 36, 357–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goltsov, A.; Sidorov, V.V.; Sokolovski, S.G.; Rafailov, E.U. Editorial: Advanced Non-invasive Photonic Methods for Functional Monitoring of Haemodynamics and Vasomotor Regulation in Health and Diseases. Front. Physiol. 2020, 11, 325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozlov, V.; Azizov, G.; Gurova, O.; Kozlov, V.I.; Azizov, G.A.; Gurova, O.A. Laser Doppler Flowmetry for Assessment of Microcirculation and Microcirculatory Blood Flow Disorders (Manual); RUDN GNC Lazer Med.: Moscow, Russia, 2012. [Google Scholar]
- Borunova, A.A.; Zabotina, T.N.; Shoua, E.K.; Chkadua, G.Z.; Chertkova, A.I.; Tabakov, D.V.; Zakharova, E.N.; Ogorodnikova, E.V.; Kadagidze, Z.G. Subpopulation structure of peripheral blood lymphocytes of donors. Russ. J. Biother. 2020, 19, 54–64. [Google Scholar] [CrossRef]
- Garg, M.; Maralakunte, M.; Garg, S.; Dhooria, S.; Sehgal, I.; Bhalla, A.S.; Vijayvergiya, R.; Grover, S.; Bhatia, V.; Jagia, P.; et al. The Conundrum of ’Long-COVID-19ʹ: A Narrative Review. Int. J. Gen. Med. 2021, 14, 2491–2506. [Google Scholar] [CrossRef]
- Blomberg, J.; Gottfries, C.-G.; Elfaitouri, A.; Rizwan, M.; Rosén, A. Infection elicited autoimmunity and myalgic encephalomyelitis/chronic fatigue syndrome: An explanatory model. Front. Immunol. 2018, 9, 229–249. [Google Scholar] [CrossRef] [Green Version]
- Lim, E.-J.; Kang, E.-B.; Jang, E.-S.; Son, C.-G. The Prospects of the Two-Day Cardiopulmonary Exercise Test (CPET) in ME/CFS Patients: A Meta-Analysis. J. Clin. Med. 2020, 9, 4040. [Google Scholar] [CrossRef]
- Nacul, L.; Jérôme Authier, F.; Scheibenbogen, C.; Lorusso, L.; Bergliot Helland, I.; Alegre Martin, J. European Network on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (EUROMENE): Expert Consensus on the Diagnosis, Service Provision, and Care of People with ME/CFS in Europe. Medicina 2021, 57, 510. [Google Scholar] [CrossRef]
- Geraghty, K.; Jason, L.; Sunnquist, M.; Tuller, D.; Blease, C.; Adeniji, C. The ‘cognitive behavioural model’ of chronic fatigue syndrome: Critique of a flawed model. Health Psychol. Open 2019, 6, 2055102919838907. [Google Scholar] [CrossRef]
- Daniels, J.; Brigden, A.; Kacorova, A. Anxiety and depression in chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME): Examining the incidence of health anxiety in CFS/ME. Psychol. Psychother. Theory Res. Pract. 2017, 90, 502–509. [Google Scholar] [CrossRef]
- Loades, M.E.; Rimes, K.A.; Ali, S.; Lievesley, K.; Chalder, T. The presence of co-morbid mental health problems in a cohort of adolescents with chronic fatigue syndrome. Clin. Child Psychol. Psychiatry 2018, 23, 398–408. [Google Scholar] [CrossRef]
- Luty, J. Medically unexplained syndromes: Irritable bowel syndrome, fibromyalgia and chronic fatigue. BJPsych Adv. 2018, 24, 252–263. [Google Scholar] [CrossRef] [Green Version]
- Fedorowski, A. Postural orthostatic tachycardia syndrome: Clinical presentation, aaetiology and management. J. Intern. Med. 2019, 285, 352–366. [Google Scholar] [CrossRef] [PubMed]
- Kozlov, I.O.; Zherebtsov, E.A.; Podmasteryev, K.V.; Dunaev, A.V. Digital Laser Doppler Flowmetry: Device, Signal Processing Technique, and Clinical Testing. Biomed. Eng. 2021, 55, 12–16. [Google Scholar] [CrossRef]
- Barhatov, I.V. Laser doppler flowmetry for human blood microcirculation assessment. Kazan Med. J. 2014, 95, 63–69. [Google Scholar] [CrossRef]
- Zaichik, A.; Churilov, L. Fundamentals of General Pathology. In Fundamentals of General Pathophysiology; ELBI Publishers: Saint Petersburg, Russia, 1999; Volume 1. [Google Scholar]
- Bond, J.; Nielsen, T.; Hodges, L. Effects of post-exertional malaise on markers of arterial stiffness in individuals with myalgic encephalomyelitis/chronic fatigue syndrome. Int. J. Environ. Res. Public Health 2021, 18, 2366. [Google Scholar] [CrossRef]
- Dregan, A. Arterial stiffness association with chronic inflammatory disorders in the UK Biobank study. Heart 2018, 104, 1257–1262. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| -Endocrine diseases/metabolic disorders: primary adrenal cortex insufficiency, Cushing’s syndrome, hyper- and hypothyroidism, diabetes mellitus, hypercalcemia; |
| -Rheumatological diseases: systemic lupus erythematosus, rheumatoid arthritis, polymyositis; |
| -Hematological diseases: iron deficiency anemia, hemochromatosis, idiopathic thrombocytopenic purpura; |
| -Infectious diseases: HIV infection, hepatitis B, hepatitis C, tuberculosis, Lyme disease, giardiasis, helminthiasis, syphilis; |
| -Neurological diseases: multiple sclerosis, narcolepsy, obstructive sleep apnea, restless legs syndrome, Parkinson’s disease, myasthenia gravis, vitamin B12 deficiency, cervical spine injuries, epilepsy; |
| -Psychiatric illnesses: bipolar disorder, substance dependence, generalized anxiety disorder, schizophrenia, major depressive disorder; |
| -Gastrointestinal diseases: celiac disease, Crohn’s disease, ulcerative colitis |
| -Cardiovascular diseases with congestive heart failure; |
| -Chronic intoxication with heavy metals (lead, mercury); |
| -The development of the patient’s symptoms as side effects of any drugs; |
| -Respiratory diseases (chronic obstructive pulmonary disease, bronchial asthma) with the development of chronic respiratory failure; |
| -Overwork (work more than 50 h a week), overtraining syndrome; |
| -Body mass index over 40; |
| Parameters | 1st Cohort (ME/CFS) | 2nd Cohort (Post-COVID ME/CFS) | 3rd Cohort (Healthy Controls) | p Value |
|---|---|---|---|---|
| Number of participants | n = 56 | n = 14 | n = 9 | |
| Age, median [interquartile range] | 39.3 [31.4; 45.9] | 34.9 [29.8; 40.2] | 31.7 [22.2; 45.1] | 0.28 |
| Sex, male/female. | 18/38 | 4/10 | 4/5 | 0.71 |
| Question from DSQ-2, (Number of Question in DSQ-2) | Symptom’s Domain | r; p Value |
|---|---|---|
| Dead, heavy feeling after starting to exercise (14) 1 | PEM | 0.62; <0.0001 |
| Next-day soreness or fatigue after non-strenuous, everyday activities (15) | PEM | 0.63; <0.0001 |
| Mentally tired after the slightest effort (16) | PEM | 0.31; 0.02 |
| Minimum exercise makes you physically tired (17) | PEM | 0.60; <0.0001 |
| Physically drained or sick after mild activity (18) | PEM | 0.71; <0.0001 |
| Feeling unrefreshed after you wake up in the morning (19) | Sleep disorder | 0.47; 0.0003 |
| Needing to nap daily (20) | Sleep disorder | 0.29; 0.03 |
| Sleeping all day and staying awake all night (24) | Sleep disorder | 0.37; 0.01 |
| Pain or aching in your muscles (25) | Pain syndromes | 0.38; 0.004 |
| Muscle weakness (33) | Neurological sensory/motor symptoms | 0.44; 0.0007 |
| Nausea (48) | Dysautonomia | 0.31; 0.02 |
| Feeling unsteady on your feet, like you might fall (49) | Neurological sensory/motor symptoms | 0.26; 0.05 |
| Sore throat (64) | Immune dysfunction | 0.28; 0.04 |
| Tender/Sore lymph nodes (65) | Immune dysfunction | 0.27; 0.045 |
| Flu-like symptoms 2 (67) | Immune dysfunction | 0.30; 0.02 |
| Muscle fatigue after mild physical activity (75) | PEM | 0.31; 0.02 |
| Worsening of symptoms after mild mental activity (77) | PEM | 0.32; 0.01 |
| Daytime drowsiness (84) | Sleep disorder | 0.32; 0.02 |
| Sinus infections 3 (87) | Immune dysfunction | 0.27; 0.04 |
| Urinary urgency (88) | Dysautonomia | 0.39; 0.01 |
| 1st Cohort (ME/CFS) | 2nd Cohort (Post-COVID ME/CFS) | 3rd Cohort (Healthy Controls) | p Value, (r) | ||
|---|---|---|---|---|---|
| 1st vs. 3rd | 1st vs. 3rd | ||||
| Severity of depressive symptoms, HADS-D score | 8.0 [6.0; 11.0] | 8.5 [4.75; 12.0] | 3.0 [1.0; 8.0] | 0.01. (0.120) | 0.01. (0.120) |
| 1st Cohort (ME/CFS) | 2nd Cohort (Post-COVID ME/CFS) | 3rd Cohort (Healthy Controls) | p Value, (r) | ||
|---|---|---|---|---|---|
| 1st vs. 3rd | 2nd vs. 3rd | ||||
| Severity of anxiety symptoms, HADS-A score | 8.0 [5.8; 10.0] | 9.5 [5.3; 15.3] | 4.0 [1.0; 8.5] | 0.04, (0.088) | 0.06, (0.216) |
| r; p | ||
|---|---|---|
| Severity of fatigue (the composite score of the 13th question of the DSQ-2 questionnaire) | Severity of depressive symptoms (HADS-D score) | 0.11; 0.44 |
| Severity of fatigue (the composite score of the 13th question of the DSQ-2 questionnaire) | Severity of anxiety (HADS-A score) | −0.18; 0.22 |
| 1st Cohort (ME/ CFS) | 2nd Cohort (Post-COVID ME/CFS) | 3rd Cohort (Healthy Controls) | p Value, (OR) | ||
|---|---|---|---|---|---|
| 1st vs. 3rd | 2nd vs. 3rd | ||||
| Prevalence of POTS | 6 (37.5%) | 6 (75.0%) | 1 (11.1%) | 0.35 | 0.02, (24.00) |
| Parameters | 1st Cohort (ME/CFS) | 2nd Cohort (Post-COVID ME/CFS) | 3rd Cohort (Healthy Controls) | p Value, (r) | ||
|---|---|---|---|---|---|---|
| 1st vs. 3rd | 2nd vs. 3rd | 2nd vs. 3rd | ||||
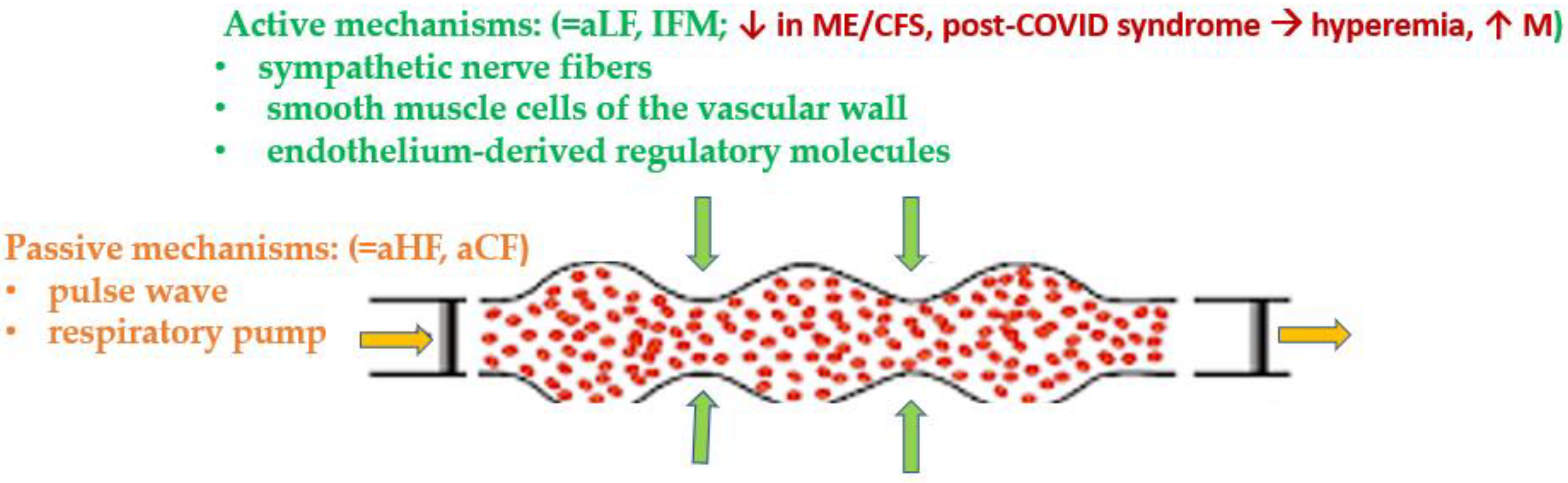
| M, perfusion units | 4.86 [4.55; 6.88] | 5.84 [4.13; 6.74] | 3.08 [2.19; 4.71] | 0.02, (0.432) | 0.01, (0.655) | 0.72 |
| σ, perfusion units | 0.59 [0.46; 0.91] | 0.70 [0.51; 0.83] | 0.69 [0.52; 0.95] | 0.65 | 0.95 | 0.52 |
| vALF, perfusion units | 16.96 [8.43; 24.36] | 15.94 [10.17; 21.57] | 38.08 [22.28; 43.82] | 0.05, (0.318) | 0.02, (0.580) | 0.98 |
| vAHF, perfusion units | 16.97 [5.42; 27.31] | 4.11 [3.35; 29.88] | 5.42 [2.81; 14.65] | 0.25 | 0.94 | 0.32 |
| vACF, perfusion units | 68.09 [48.26; 76.42] | 76.52 [59.96; 81.22] | 54.87 [45.20; 67.23] | 0.35 | 0.30 | 0.35 |
| IFM, | 0.33 [0.23; 0.47] | 0.36 [0.24; 0.42] | 0.60 [0.41; 0.70] | 0.04, (0.354) | 0.04, (0.510) | 0.94 |
| R | 1.01 [0.86; 1.16] | 0.82 [0.66; 0.96] | 0.83 [0.70; 0.92] | 0.09 | 0.94 | 0.04 (0.350) |
| CT | 2.77 [2.28; 3.71] | 3.32 [3.00; 6.20] | 2.77 [2.14; 3.80] | 0.94 | 0.18 | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryabkova, V.A.; Gavrilova, N.Y.; Fedotkina, T.V.; Churilov, L.P.; Shoenfeld, Y. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Post-COVID Syndrome: A Common Neuroimmune Ground? Diagnostics 2023, 13, 66. https://doi.org/10.3390/diagnostics13010066
Ryabkova VA, Gavrilova NY, Fedotkina TV, Churilov LP, Shoenfeld Y. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Post-COVID Syndrome: A Common Neuroimmune Ground? Diagnostics. 2023; 13(1):66. https://doi.org/10.3390/diagnostics13010066
Chicago/Turabian StyleRyabkova, Varvara A., Natalia Y. Gavrilova, Tamara V. Fedotkina, Leonid P. Churilov, and Yehuda Shoenfeld. 2023. "Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Post-COVID Syndrome: A Common Neuroimmune Ground?" Diagnostics 13, no. 1: 66. https://doi.org/10.3390/diagnostics13010066
APA StyleRyabkova, V. A., Gavrilova, N. Y., Fedotkina, T. V., Churilov, L. P., & Shoenfeld, Y. (2023). Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Post-COVID Syndrome: A Common Neuroimmune Ground? Diagnostics, 13(1), 66. https://doi.org/10.3390/diagnostics13010066