

Prognosis and Nomogram Prediction for Patients with Oral Squamous Cell Carcinoma: A Cohort Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Collection
2.5. Nomogram Construction and Validation
3. Results
3.1. Patient Characteristics and Risk Factors of OSCC
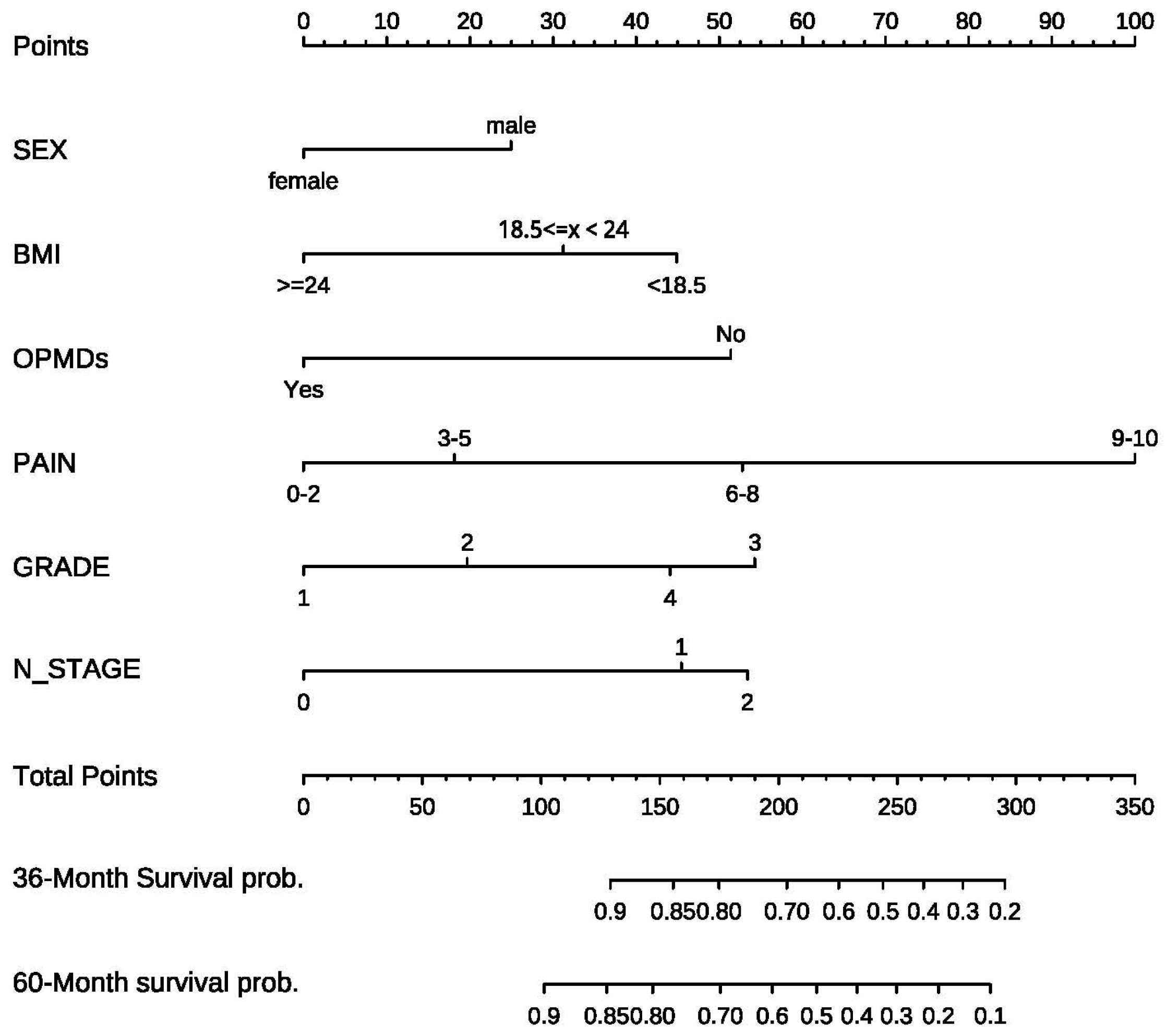
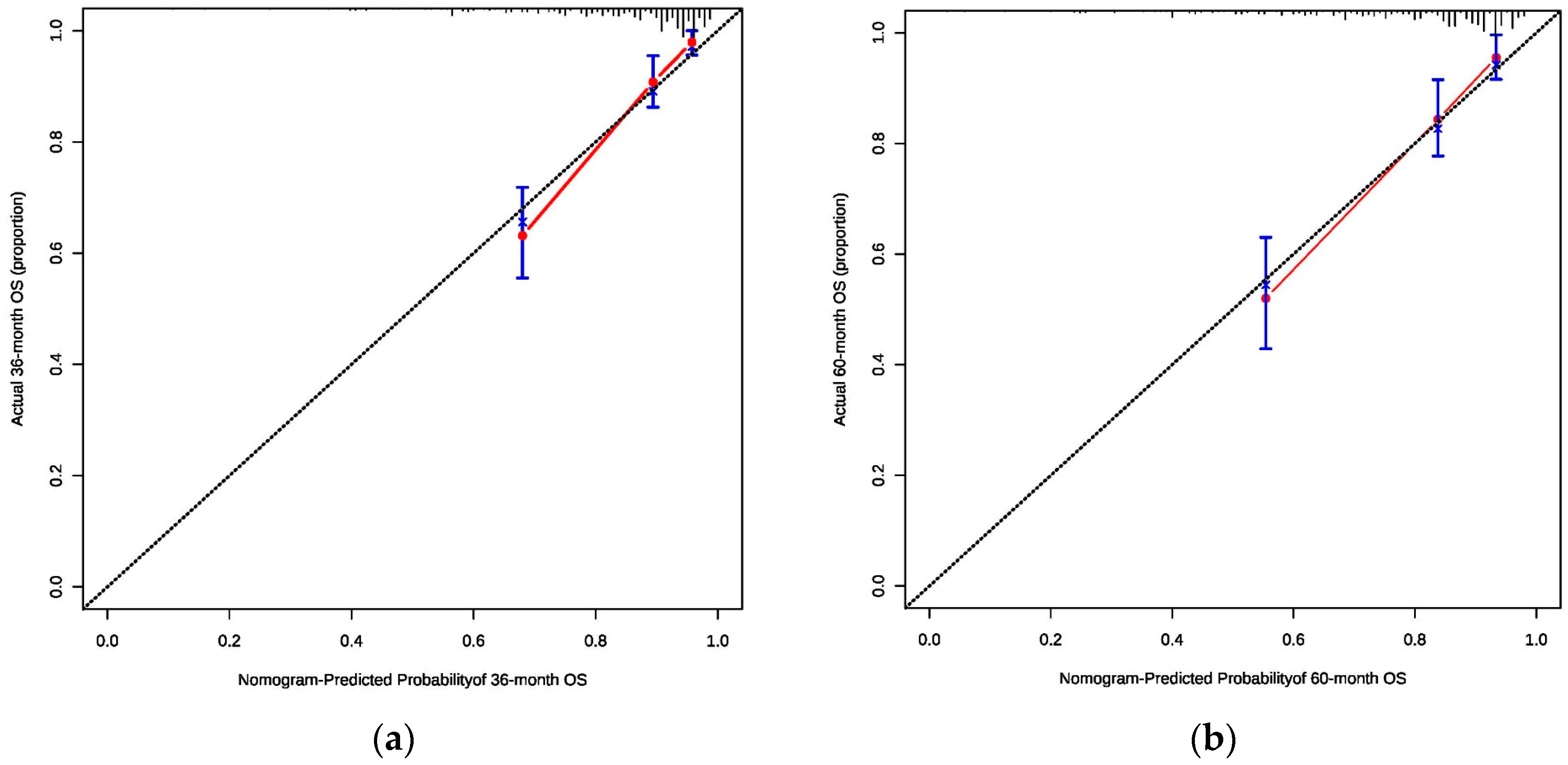
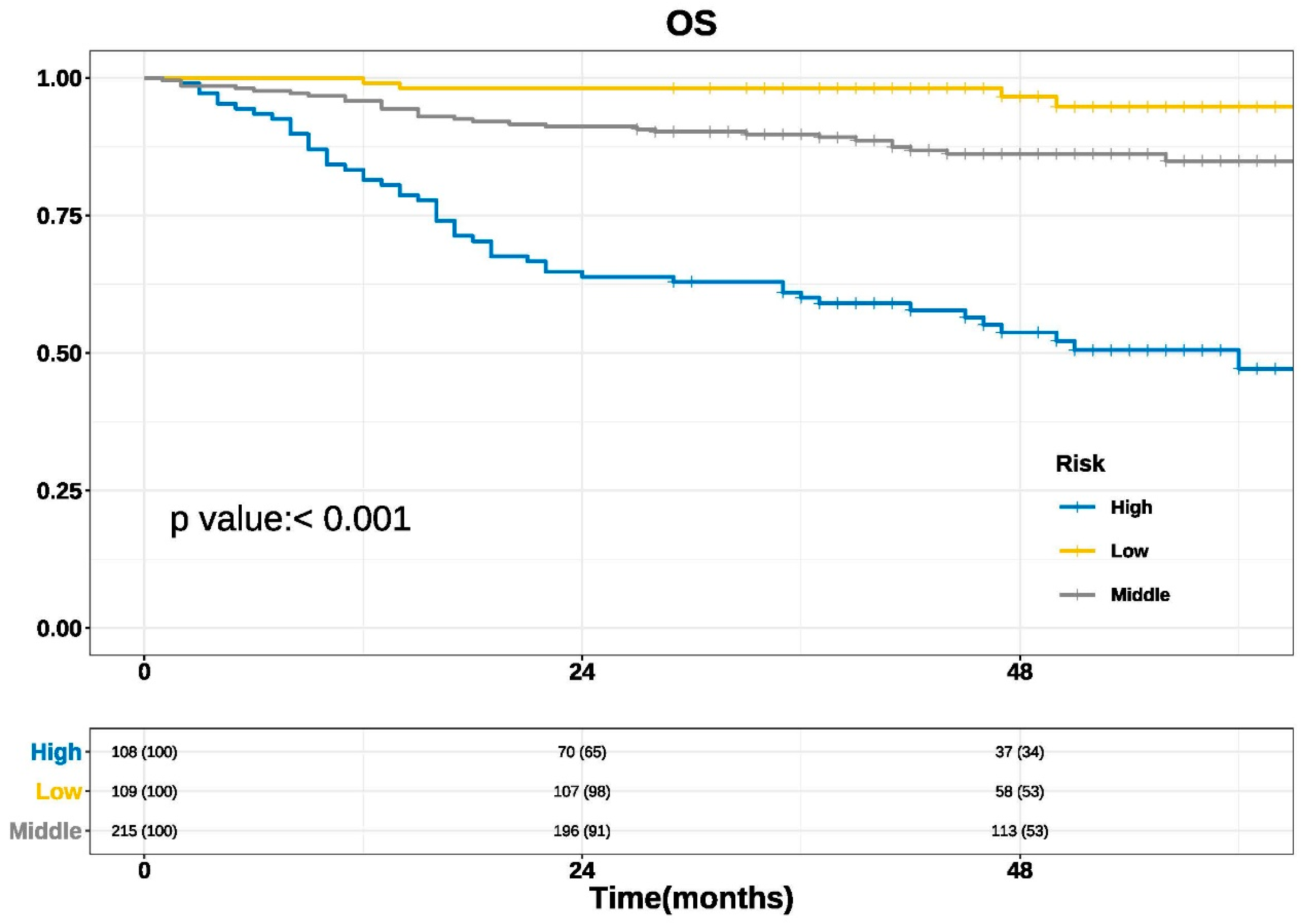
3.2. Nomogram Construction and Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cramer, J.D.; Burtness, B.; Le, Q.T.; Ferris, R.L. The changing therapeutic landscape of head and neck cancer. Nat. Rev. Clin. Oncol. 2019, 16, 669–683. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Sun, K.; Zheng, R.; Zeng, H.; Wang, S.; Chen, R.; Wei, W.; He, J. Cancer incidence and mortality in China, 2015. J. Natl. Cancer Cent. 2021, 1, 2–11. [Google Scholar] [CrossRef]
- Zheng, R.; Zhang, S.; Zeng, H.; Wang, S.; Sun, K.; Chen, R.; Li, L.; Wei, W.; He, J. Cancer incidence and mortality in China, 2016. J. Natl. Cancer Cent. 2022, 2, 1–9. [Google Scholar] [CrossRef]
- Jemal, A.; Murray, T.; Ward, E.; Samuels, A.; Tiwari, R.C.; Ghafoor, A.; Feuer, E.J.; Thun, M.J. Cancer statistics, 2005. CA Cancer J. Clin. 2005, 55, 10–30. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2015. CA Cancer J. Clin. 2015, 65, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.; Chen, W.; Zheng, R.; Zhang, S.; Ji, J.S.; Zou, X.; Xia, C.; Sun, K.; Yang, Z.; Li, H.; et al. Changing cancer survival in China during 2003-15: A pooled analysis of 17 population-based cancer registries. Lancet Glob. Health 2018, 6, e555–e567. [Google Scholar] [CrossRef] [PubMed]
- Moeckelmann, N.; Ebrahimi, A.; Tou, Y.K.; Gupta, R.; Low, T.H.; Ashford, B.; Ch’ng, S.; Palme, C.E.; Clark, J.R. Prognostic implications of the 8th edition American Joint Committee on Cancer (AJCC) staging system in oral cavity squamous cell carcinoma. Oral Oncol. 2018, 85, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Kattan, M.W.; Hess, K.R.; Amin, M.B.; Lu, Y.; Moons, K.G.; Gershenwald, J.E.; Gimotty, P.A.; Guinney, J.H.; Halabi, S.; Lazar, A.J.; et al. American Joint Committee on Cancer acceptance criteria for inclusion of risk models for individualized prognosis in the practice of precision medicine. CA Cancer J. Clin. 2016, 66, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W.; Moons, K.G.; van der Windt, D.A.; Hayden, J.A.; Perel, P.; Schroter, S.; Riley, R.D.; Hemingway, H.; Altman, D.G. Prognosis Research Strategy (PROGRESS) 3: Prognostic model research. PLoS Med. 2013, 10, e1001381. [Google Scholar] [CrossRef]
- Grimes, D.A. The nomogram epidemic: Resurgence of a medical relic. Ann. Intern. Med. 2008, 149, 273–275. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 2015, 16, e173–e180. [Google Scholar] [CrossRef] [PubMed]
- Weiser, M.R.; Gönen, M.; Chou, J.F.; Kattan, M.W.; Schrag, D. Predicting survival after curative colectomy for cancer: Individualizing colon cancer staging. J. Clin. Oncol. 2011, 29, 4796–4802. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Zhang, L.; Jiang, G.; Wang, Q.; Liu, L.; Liu, D.; Wang, Z.; Zhu, Z.; Deng, Q.; Xiong, X.; et al. Development and validation of a nomogram for predicting survival in patients with resected non-small-cell lung cancer. J. Clin. Oncol. 2015, 33, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Marks, R.; Zhang, M.; Jiang, G.; Jatoi, A.; Garces, Y.I.; Mansfield, A.; Molina, J.; Yang, P. Nomograms Predict Overall Survival for Patients with Small-Cell Lung Cancer Incorporating Pretreatment Peripheral Blood Markers. J. Thorac. Oncol. 2015, 10, 1213–1220. [Google Scholar] [CrossRef]
- Weiser, M.R.; Landmann, R.G.; Kattan, M.W.; Gonen, M.; Shia, J.; Chou, J.; Paty, P.B.; Guillem, J.G.; Temple, L.K.; Schrag, D.; et al. Individualized prediction of colon cancer recurrence using a nomogram. J. Clin. Oncol. 2008, 26, 380–385. [Google Scholar] [CrossRef]
- Zhang, J.X.; Song, W.; Chen, Z.H.; Wei, J.H.; Liao, Y.J.; Lei, J.; Hu, M.; Chen, G.Z.; Liao, B.; Lu, J.; et al. Prognostic and predictive value of a microRNA signature in stage II colon cancer: A microRNA expression analysis. Lancet Oncol. 2013, 14, 1295–1306. [Google Scholar] [CrossRef]
- Zhou, M.; Lv, S.; Hou, Y.; Zhang, R.; Wang, W.; Yan, Z.; Li, T.; Gan, W.; Zeng, Z.; Zhang, F.; et al. Characterization of sialylation-related long noncoding RNAs to develop a novel signature for predicting prognosis, immune landscape, and chemotherapy response in colorectal cancer. Front. Immunol. 2022, 13, 994874. [Google Scholar] [CrossRef]
- Ying, H.Q.; Deng, Q.W.; He, B.S.; Pan, Y.Q.; Wang, F.; Sun, H.L.; Chen, J.; Liu, X.; Wang, S.K. The prognostic value of preoperative NLR, d-NLR, PLR and LMR for predicting clinical outcome in surgical colorectal cancer patients. Med. Oncol. 2014, 31, 305. [Google Scholar] [CrossRef]
- Diao, J.D.; Ma, L.X.; Sun, M.Y.; Wu, C.J.; Wang, L.J.; Liu, Y.L.; Yang, Y.J. Construction and validation of a nomogram to predict overall survival in patients with inflammatory breast cancer. Cancer Med. 2019, 8, 5600–5608. [Google Scholar] [CrossRef]
- Roth, A.J.; Kornblith, A.B.; Batel-Copel, L.; Peabody, E.; Scher, H.I.; Holland, J.C. Rapid screening for psychologic distress in men with prostate carcinoma: A pilot study. Cancer 1998, 82, 1904–1908. [Google Scholar] [CrossRef]
- Gao, L.; Mao, C.; Yu, G.Y.; Peng, X. Authorization, translation, back translation and language modification of the simplified Chinese adult comorbidity-27 index. Zhonghua Kou Qiang Yi Xue Za Zhi 2016, 51, 623–627. [Google Scholar] [CrossRef]
- Greenlee, R.T.; Hill-Harmon, M.B.; Murray, T.; Thun, M. Cancer statistics, 2001. CA Cancer J. Clin. 2001, 51, 15–36. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Thomas, A.; Murray, T.; Thun, M. Cancer statistics, 2002. CA Cancer J. Clin. 2002, 52, 23–47. [Google Scholar] [CrossRef] [PubMed]
- Tham, T.; Machado, R.; Herman, S.W.; Kraus, D.; Costantino, P.; Roche, A. Personalized prognostication in head and neck cancer: A systematic review of nomograms according to the AJCC precision medicine core (PMC) criteria. Head Neck. 2019, 41, 2811–2822. [Google Scholar] [CrossRef]
- Russo, D.; Mariani, P.; Caponio, V.C.A.; Russo, L.L.; Fiorillo, L.; Zhurakivska, K.; Muzio, L.L.; Laino, L.; Troiano, G. Development and Validation of Prognostic Models for Oral Squamous Cell Carcinoma: A Systematic Review and Appraisal of the Literature. Cancers 2021, 13, 5755. [Google Scholar] [CrossRef] [PubMed]
- Bobdey, S.; Balasubramaniam, G.; Mishra, P. Nomogram prediction for survival of patients with oral cavity squamous cell carcinoma. Head Neck. 2016, 38, 1826–1831. [Google Scholar] [CrossRef]
- Montero, P.H.; Yu, C.; Palmer, F.L.; Patel, P.D.; Ganly, I.; Shah, J.P.; Shaha, A.R.; Boyle, J.O.; Kraus, D.H.; Singh, B.; et al. Nomograms for preoperative prediction of prognosis in patients with oral cavity squamous cell carcinoma. Cancer 2014, 120, 214–221. [Google Scholar] [CrossRef]
- Bobdey, S.; Mair, M.; Nair, S.; Nair, D.; Balasubramaniam, G.; Chaturvedi, P. A Nomogram based prognostic score that is superior to conventional TNM staging in predicting outcome of surgically treated T4 buccal mucosa cancer: Time to think beyond TNM. Oral Oncol. 2018, 81, 10–15. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, Z.; Liu, X.; Ju, J.; Chai, J.; Ni, Q.; Ma, C.; Gao, T.; Sun, M. Nomograms to estimate long-term overall survival and tongue cancer-specific survival of patients with tongue squamous cell carcinoma. Cancer Med. 2017, 6, 1002–1013. [Google Scholar] [CrossRef]
- Sun, W.; Cheng, M.; Zhuang, S.; Chen, H.; Yang, S.; Qiu, Z. Nomograms to predict survival of stage IV tongue squamous cell carcinoma after surgery. Medicine 2019, 98, e16206. [Google Scholar] [CrossRef] [PubMed]
- Chang, B.; He, W.; Ouyang, H.; Peng, J.; Shen, L.; Wang, A.; Wu, P. A Prognostic Nomogram Incorporating Depth of Tumor Invasion to Predict Long-term Overall Survival for Tongue Squamous Cell Carcinoma With R0 Resection. J. Cancer 2018, 9, 2107–2115. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | No. of Patients (%) | |
|---|---|---|
| Age | ||
| <30 | 6 | 1.39% |
| 30 ≤ x < 40 | 26 | 6.02% |
| 40 ≤ x < 50 | 63 | 14.58% |
| 50 ≤ x < 60 | 124 | 28.71% |
| 60 ≤ x < 70 | 140 | 32.41% |
| 70 ≤ x < 80 | 63 | 14.58% |
| ≥80 | 10 | 2.31% |
| Gender | ||
| Male | 291 | 67.36% |
| Female | 141 | 32.64% |
| Educational level | ||
| Higher | 114 | 26.39% |
| Medium | 108 | 25.00% |
| Lower | 210 | 48.61% |
| BMI | ||
| <18.5 | 25 | 5.79% |
| 18.5 ≤ x < 24 | 208 | 48.15% |
| ≥24 | 199 | 46.06% |
| Anxiety state score | ||
| 0–2 | 216 | 50.00% |
| 3–5 | 127 | 29.40% |
| 6–8 | 78 | 18.05% |
| 9–10 | 11 | 2.55% |
| Smoking | ||
| Yes | 226 | 52.31% |
| No | 206 | 47.69% |
| Drinking | ||
| Yes | 169 | 39.12% |
| No | 263 | 60.88% |
| Tumor history | ||
| Yes | 45 | 10.42% |
| No | 387 | 89.58% |
| Family history | ||
| Yes | 156 | 36.11% |
| No | 276 | 63.89% |
| Overall comorbidity grade | ||
| 0 | 216 | 50.00% |
| 1 | 173 | 40.05% |
| 2 | 33 | 7.64% |
| 3 | 10 | 2.31% |
| OPMDs history | ||
| Yes | 64 | 14.81% |
| No | 368 | 85.19% |
| Subsite | ||
| Lip | 19 | 4.40% |
| Buccal mucosa | 43 | 9.95% |
| Gingiva | 94 | 21.76% |
| Retromolar tissue | 15 | 3.47% |
| Palate | 7 | 1.62% |
| Mouth floor | 52 | 12.04% |
| Tongue | 179 | 41.44% |
| Oropharyngeal | 23 | 5.32% |
| Pain severity score | ||
| 0–2 | 191 | 44.22% |
| 3–5 | 149 | 34.49% |
| 6–8 | 70 | 16.20% |
| 9–10 | 22 | 5.09% |
| SCC grade | ||
| 1 | 181 | 41.90% |
| 2 | 154 | 35.65% |
| 3 | 76 | 17.59% |
| 4 | 21 | 4.86% |
| T stage | ||
| 1 | 136 | 31.48% |
| 2 | 161 | 37.27% |
| 3 | 49 | 11.34% |
| 4 | 86 | 19.91% |
| N stage | ||
| 0 | 285 | 65.98% |
| 1 | 63 | 14.58% |
| 2b | 70 | 16.20% |
| 2c | 13 | 3.01% |
| 3 | 1 | 0.23% |
| Radiation and chemotherapy | ||
| Yes | 118 | 27.31% |
| No | 314 | 72.69% |
| Variable | The Deceased Groups (n = 85, 19.68%) | The Survived Groups (n = 347, 80.32%) | p | ||
|---|---|---|---|---|---|
| Gender | |||||
| Male | 68 | 23.37% | 223 | 76.63% | 0.006 |
| Female | 17 | 12.06% | 124 | 87.94% | |
| BMI | |||||
| <18.5 | 8 | 32.00% | 17 | 68.00% | 0.008 |
| 18.5 ≤ x < 24 | 50 | 24.04% | 158 | 75.96% | |
| ≥24 | 27 | 13.57% | 172 | 86.43% | |
| Smoking | |||||
| Yes | 54 | 23.89% | 172 | 76.11% | 0.021 |
| No | 31 | 15.05% | 175 | 84.95% | |
| Drinking | |||||
| Yes | 44 | 26.04% | 125 | 73.96% | 0.008 |
| No | 41 | 15.59% | 222 | 84.41% | |
| OPMDs | |||||
| Yes | 4 | 6.25% | 60 | 93.75% | 0.003 |
| No | 81 | 22.01% | 287 | 77.99% | |
| Pain scores | |||||
| 0–2 | 22 | 11.52% | 169 | 88.48% | <0.0001 |
| 3–5 | 30 | 20.13% | 119 | 79.87% | |
| 6–8 | 22 | 31.43% | 48 | 68.57% | |
| 9–10 | 11 | 50.00% | 11 | 50.00% | |
| SCC grade | |||||
| 1 | 18 | 9.94% | 163 | 90.06% | <0.0001 |
| 2 | 29 | 18.83% | 125 | 81.17% | |
| 3 | 39 | 45.88% | 46 | 54.12% | |
| 4 | 8 | 38.10% | 13 | 61.90% | |
| T stage | |||||
| 1 | 13 | 9.56% | 123 | 90.44% | <0.0001 |
| 2 | 31 | 19.25% | 130 | 80.75% | |
| 3 | 14 | 28.57% | 35 | 71.43% | |
| 4 | 27 | 31.40% | 59 | 68.60% | |
| N stage | |||||
| 0 | 34 | 11.93% | 251 | 88.07% | <0.0001 |
| 1 | 18 | 28.57% | 45 | 71.43% | |
| 2b | 23 | 32.86% | 47 | 67.14% | |
| 2c | 9 | 69.23% | 4 | 30.77% | |
| 3 | 1 | 100.00% | 0 | 0.00% | |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p | Hazard Ratio (95% CI) | p | |
| Gender | ||||
| Male | 1 | 1 | ||
| Female | 0.487 (0.286–0.828) | 0.008 | 0.561 (0.280–1.125) | 0.103 |
| BMI | ||||
| <18.5 | 1 | 1 | ||
| 18.5 ≤ x < 24 | 0.767 (0.364–1.618) | 0.486 | 0.756 (0.352–1.623) | 0.472 |
| ≥24 | 0.418 (0.190–0.921) | 0.03 | 0.434 (0.192–0.978) | 0.044 |
| Smoking | ||||
| No | 1 | 1 | ||
| Yes | 1.632 (1.049–2.538) | 0.03 | 0.771 (0.396–1.502) | 0.444 |
| Drinking | ||||
| No | 1 | 1 | ||
| Yes | 1.735 (1.134–2.656) | 0.011 | 0.949 (0.529–1.703) | 0.861 |
| OPMDs | ||||
| No | 1 | 1 | ||
| Yes | 0.279 (0.102–0.761) | 0.013 | 0.413 (0.145–1.173) | 0.097 |
| Pain | ||||
| 0–2 | 1 | 1 | ||
| 3–5 | 1.786 (1.030–3.097) | 0.039 | 1.383 (0.771–2.479) | 0.277 |
| 6–8 | 3.223 (1.783–5.826) | <0.0001 | 2.301 (1.222–4.334) | 0.01 |
| 9–10 | 6.847 (3.307–14.177) | <0.0001 | 5.193 (2.269–11.885) | <0.0001 |
| Grade | ||||
| 1 | 1 | 1 | ||
| 2 | 2.009 (1.116–3.618) | 0.02 | 1.352 (0.735–2.485) | 0.332 |
| 3 | 4.635 (2.583–8.316) | <0.0001 | 2.393 (1.264–4.528) | 0.007 |
| 4 | 4.558 (1.980–10.491) | <0.0001 | 2.129 (0.842–5.386) | 0.111 |
| T stage | ||||
| 1 | 1 | 1 | ||
| 2 | 2.047 (1.071–3.913) | 0.03 | 1.508 (0.764–2.979) | 0.237 |
| 3 | 3.286 (1.544–6.993) | 0.002 | 1.864 (0.833–4.174) | 0.13 |
| 4 | 3.654 (1.885–7.083) | <0.0001 | 1.184 (0.560–2.502) | 0.659 |
| N stage | ||||
| 0 | 1 | 1 | ||
| 1 | 2.711 (1.530–4.803) | 0.001 | 2.164 (1.187–3.944) | 0.012 |
| 2b | 3.040 (1.790–5.162) | <0.0001 | 2.090 (1.158–3.771) | 0.014 |
| 2c | 8.624 (4.125–18.033) | <0.0001 | 3.134 (1.324–7.420) | 0.009 |
| 3 | 47.613 (6.197–365.834) | <0.0001 | 14.848 (1.523–144.762) | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.-Y.; Xie, S.; Wang, D.-C.; Shan, X.-F.; Cai, Z.-G. Prognosis and Nomogram Prediction for Patients with Oral Squamous Cell Carcinoma: A Cohort Study. Diagnostics 2023, 13, 1768. https://doi.org/10.3390/diagnostics13101768
Zhang X-Y, Xie S, Wang D-C, Shan X-F, Cai Z-G. Prognosis and Nomogram Prediction for Patients with Oral Squamous Cell Carcinoma: A Cohort Study. Diagnostics. 2023; 13(10):1768. https://doi.org/10.3390/diagnostics13101768
Chicago/Turabian StyleZhang, Xin-Yuan, Shang Xie, Dian-Can Wang, Xiao-Feng Shan, and Zhi-Gang Cai. 2023. "Prognosis and Nomogram Prediction for Patients with Oral Squamous Cell Carcinoma: A Cohort Study" Diagnostics 13, no. 10: 1768. https://doi.org/10.3390/diagnostics13101768
APA StyleZhang, X. -Y., Xie, S., Wang, D. -C., Shan, X. -F., & Cai, Z. -G. (2023). Prognosis and Nomogram Prediction for Patients with Oral Squamous Cell Carcinoma: A Cohort Study. Diagnostics, 13(10), 1768. https://doi.org/10.3390/diagnostics13101768