

Three-Dimensional Measurements of the Palate and Dental Arch Perimeter as Predictors for Maxillary Palatal Canine Impaction—A Cone-Beam Computed Tomography Image Analysis
 , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Methods
2.2. Sample Size Estimation
2.3. Inclusion Criteria
- Radiographs of patients 15–25 years of age with complete permanent teeth, excluding wisdom teeth.
- Cases with unilateral or bilateral impacted maxillary canine.
- No previous orthodontic treatment.
- No developmental anomalies, no history of trauma or craniofacial malformations.
- No intensive restorations or crowns.
- Class I molars dental relationship.
- Cases with high-quality CBCT images and volumetric data.
2.4. CBCT Imaging
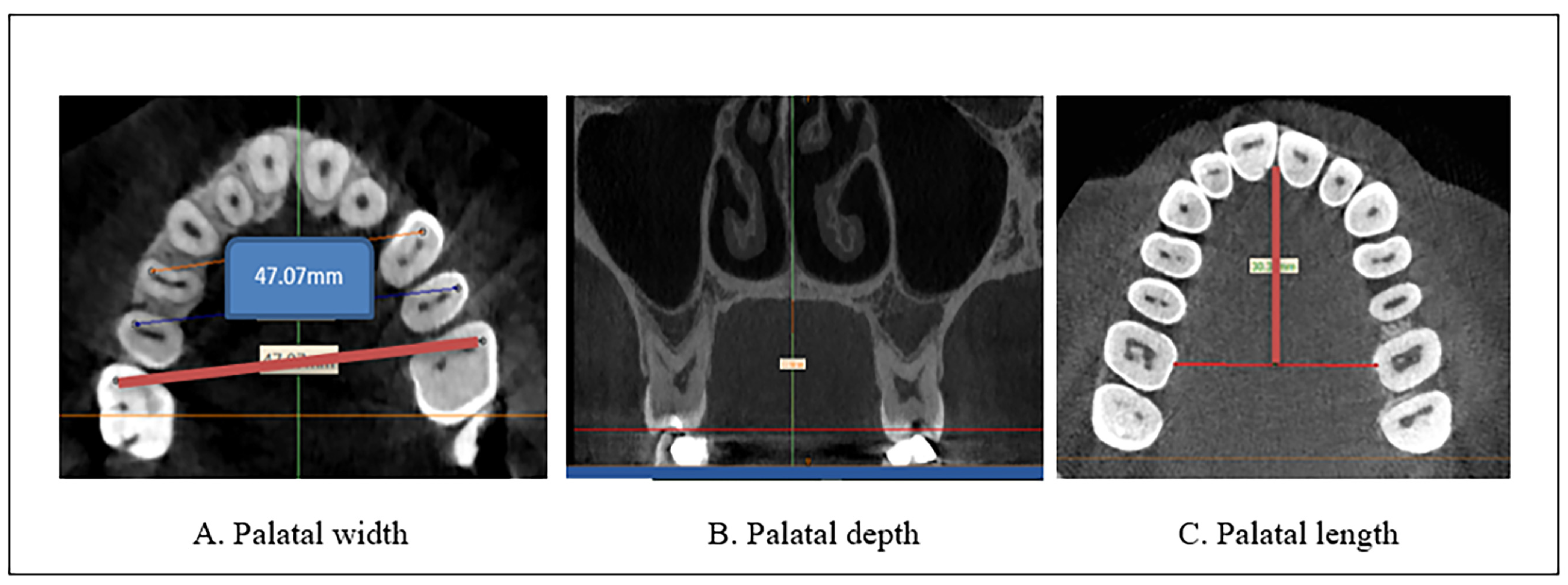
2.4.1. Palatal Measurement
- -
- Palatal width was measured by drawing lines from the mesiobuccal cusp tip of the maxillary first molar from one side to the other [19]. The exact location of the buccal cusp tips of the upper first molar was identified and checked in all the planes from the coronal plane [20] and even from the reference plane. Then, the palatal width was measured from the axial view. Using the axial plane for the evaluation allowed the accurate designation of the selected landmark without superimposing different landmarks [20]. The coronal and axial levels at which the position of the mesiobuccal cusp of the upper molar was identified differ from one case to another due to anatomical variations, but in most of the cases, they are between (66–73 and 45–50) slices, respectively.The measurements were performed on an axial view of the radiographs derived from the CBCT images (Figure 1A).
- -
- -
- The palatal length was determined by measuring the linear distance from the mesial contact point of the upper central incisors to the midpoint of the linear distance between the two upper first molars, obtained from the axial view of the radiographs derived from the CBCT images (Figure 1C).
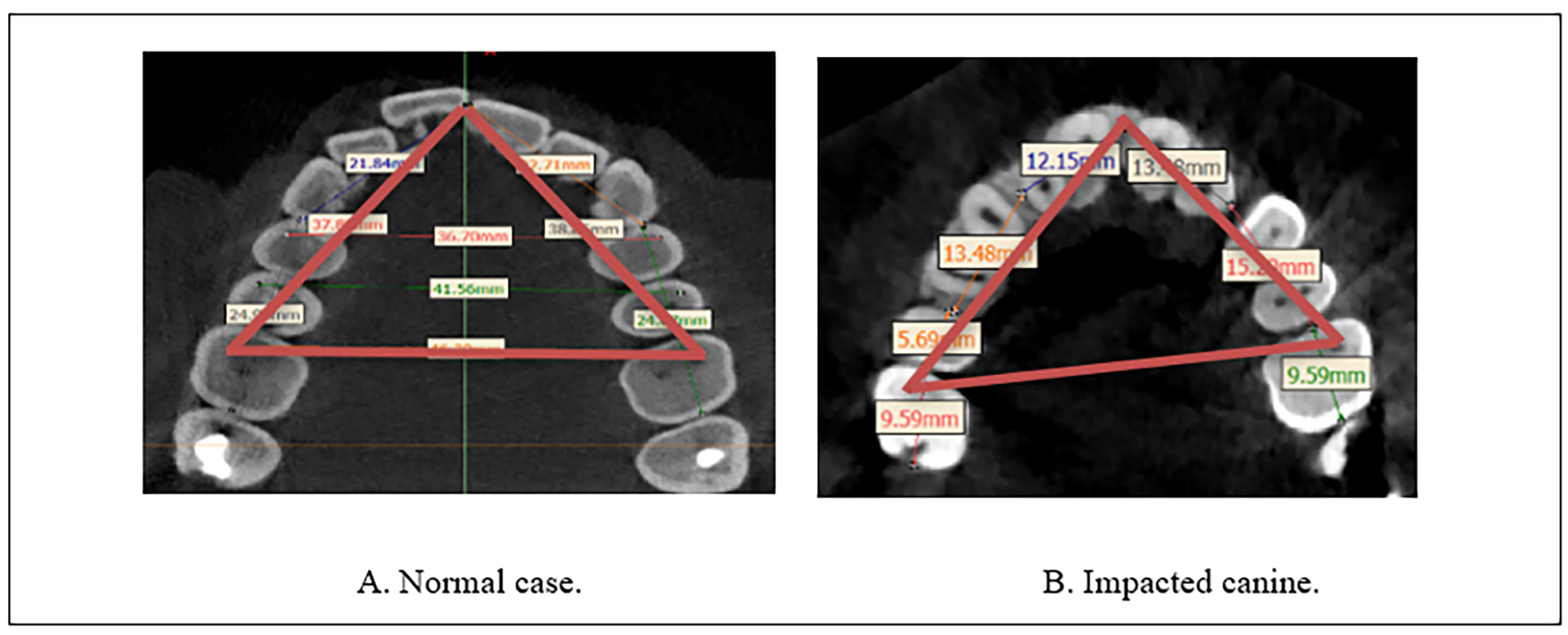
2.4.2. Maxillary Arch Perimeter
2.5. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Inferential Statistics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raghoebar, G.M.; Boering, G.; Vissink, A.; Stegenga, B. Eruption disturbances of permanent molars: A review. J. Oral Pathol. Med. 1991, 20, 159–166. [Google Scholar] [CrossRef]
- Quadras, D.D.; Nayak, U.S.; Ravi, M.S.; Pujari, P. Early prediction of maxillary canine impaction using sectors and angular measurement—A radiographic study. MJDS 2017, 2, 7–11. [Google Scholar]
- Bjerklin, K. Orthodontic management of impacted maxillary canines. APOS Trends Orthod. 2020, 10, 64–71. [Google Scholar] [CrossRef]
- Aziz, Z.H. Problems Related to Permanent Maxillary Canine in Skeletal Class I Jaw Relationship in Sulaimani Kurd Students Aged 18–22 Years. Master’s Thesis, College of Dentistry, University of Sulaimani, Sulaymaniyah, Iraq, 2008. [Google Scholar]
- Al-Atabi, H.; Mohammed-Salih, H.; Nahidh, M. Buccally malposed maxillary canines in intermediate schools’ students of sammawa city. Iraqi Dent. J. 2016, 38, 21–27. [Google Scholar] [CrossRef]
- Bondemark, L.; Tsiopa, J. Prevalence of ectopic eruption, impaction, retention and agenesis of the permanent second molar. Angle Orthod. 2007, 77, 773–778. [Google Scholar] [CrossRef]
- Aslan, B.I.; Üçüncü, N. Clinical consideration and management of impacted maxillary canine teeth. In Emerging Trends in Oral Health Sciences and Dentistry; InTech: Rang-Du-Fliers, France, 2015; Chapter 21; pp. 465–501. [Google Scholar]
- Coulter, J.; Richardson, A. Normal eruption of the maxillary canine quantified in three dimensions. Eur. J. Orthod. 1997, 19, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Siotou, K.; Kouskouki, M.P.; Christopoulou, I.; Tsolakis, A.I.; Tsolakis, I.A. Frequency and Local Etiological Factors of Impaction of Permanent Teeth among 1400 Patients in a Greek Population. Dent. J. 2022, 10, 150. [Google Scholar] [CrossRef]
- Litsas, G.A. Review of early displaced maxillary canines Etiology, diagnosis and interceptive treatment. Open Dent. J. 2011, 5, 39–47. [Google Scholar] [CrossRef]
- Janakiraman, E.N.; Alexander, M.; Sanjay, P. Prospective analysis of frequency and contributing factors of nerve injuries following third-molar surgery. J. Craniofac. Surg. 2010, 2, 784–786. [Google Scholar] [CrossRef]
- Mohanty, P.; Acharya, S.S.; Dany, S.S.; Mohanty, D. Maxillary canine impaction and its management—A review. Int. J. Contemp. Med. Res. 2015, 2, 949–955. [Google Scholar]
- Gupta, A.; Makhija, P.; Bhatia, V.; Navlani, M.; Virang, B. Impacted Canine- Diagnosis and Prevention. Web Med. Cent. Dent. 2012, 3, WMC003011. [Google Scholar]
- Mohammad, O.F.; Mahmood, A.D. Investigating the correlation between palatal depth and width measurements in impacted maxillary canine patients by using cone-beam computed tomography. JODR 2018, 5, 32–39. [Google Scholar]
- Hong, W.H.; Radfar, R.; Chung, C.H. Relationship between the maxillary transverse dimension and palatally displaced canines: A cone-beam computed tomographic study. Angle Orthod. 2015, 85, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Shalini, S.; Ravindra, K.J. Prevelence of maxillary canine impaction and associated factors in class I and class II malocclusion—A retrospective study. Eur. J. Mol. Clin. Med. 2020, 7, 2515–8260. [Google Scholar]
- Di Carlo, G.; Saccucci, M.; Luzzi, V.; Ierardo, G.; Vozza, I.; Sfasciotti, G.L.; Polimeni, A. Prevalence of maxillary canine impaction in skeletal Class III malocclusions compared to Class I malocclusions. J. Clin. Exp. Dent. 2019, 11, e264–e268. [Google Scholar] [CrossRef]
- Dağsuyu, İ.M.; Okşayan, R.; Kahraman, F.; Aydın, M.; Bayrakdar, İ.Ş.; Uğurlu, M. The Relationship between Dental Follicle Width and Maxillary Impacted Canines’ Descriptive and Resorptive Features Using Cone-Beam Computed Tomography. BioMed Res. Int. 2017, 2017, 2938691. [Google Scholar] [CrossRef]
- Ala, M.; Shahid, F.; Purmal, K.; Ahmad, B.; Khamis, M. Tooth size and dental arch dimension measurement through cone-beam computed tomography: Effect of age and gender. Res. J. Recent Sci. 2014, 3, 85–94. [Google Scholar]
- Azim, A.A.; Azim, K.A.; Deutsch, A.S.; Huang, G.T. Acquisition of anatomic parameters concerning molar pulp chamber landmarks using cone-beam computed tomography. J. Endod. 2014, 40, 1298–1302. [Google Scholar] [CrossRef]
- El Nahass, H.; Naiem, S.N. Palatal bone dimensions on cone-beam computed tomography. Implications for the palate as autogenous donor site: An observational study. Int. J. Oral Maxillofac. Surg. 2016, 45, 99–103. [Google Scholar] [CrossRef]
- Ahmad, Z.M. Palatal dimensions and its correlation with the circumference of upper anterior teeth. RDENTJ 2009, 9, 259–267. [Google Scholar] [CrossRef]
- Arboleda-Ariza, N.; Schilling, J.; Arriola-Guillén, L.E.; Ruíz-Mora, G.A.; Rodríguez-Cárdenas, Y.A.; Aliaga-Del Castillo, A. Maxillary transverse dimensions in subjects with and without impacted canines: A comparative cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Hyun, H.K.; Jang, K.T. Interrelationship between the position of impacted maxillary canines and the morphology of the maxilla. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 556–562. [Google Scholar] [CrossRef]
- Al-Nimri, K.; Gharaibeh, T. Space conditions and dental and occlusal features in patients with palatally impacted maxillary canines: An aetiological study. Eur. J. Orthod. 2005, 27, 461–465. [Google Scholar] [CrossRef]
- Nisha, S.; Shashikumar, P.; Chandra, S. Maxillary canine impaction to treat or not. Indian J. Multidiscip. Dent. 2017, 7, 124–128. [Google Scholar] [CrossRef]
- Margot, R.; Maria, C.D.; Ali, A.; Annouschka, L.; Anna, V.; Guy, W. Prediction of maxillary canine impaction based on pano-ramic radiographs. Clin. Exp. Dent. Res. 2020, 6, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, P.M.; Tabbaa, S.; Flores-Mir, C.; Al-Jewair, T. A CBCT investigation of the association between sella-turcica bridging and maxillary palatal canine impaction. BioMed Res. Int. 2018, 2018, 4329050. [Google Scholar] [CrossRef]
- Al-Zubair, N.M.; Al-Labani, M.A.; Al-Motareb, F.L. Yemeni palatal morphology. Saudi J. Health Sci. 2015, 4, 88–91. [Google Scholar] [CrossRef]
- Haney, E.; Gansky, S.A.; Lee, J.S.; Johnson, E.; Maki, K.; Miller, A.J.; Huang, J.C. Comparative analysis of traditional radiographs and cone-beam computed tomography volumetric images in the diagnosis and treatment planning of maxillary impacted canines. Am. J. Orthod. Dentofacial. Orthop. 2010, 137, 590–597. [Google Scholar] [CrossRef]
- Richardson, G.; Russell, K.A. A review of impacted permanent maxillary cuspids–diagnosis and prevention. J. Can. Dent. Assoc. 2000, 66, 497–501. [Google Scholar]
- Al-Khateeb, S.; Abu Alhaija, E.S.; Rwaite, A.; Burqan, B.A. Dental arch parameters of the displacement and non-displacement sides in subjects with unilateral palatal canine ectopia. Angle Orthod. 2013, 83, 259–265. [Google Scholar] [CrossRef]
- Genc, E.; Karaman, A. Investigation of the relationship between maxillary dimensions and labial and palatal maxillary impacted canines using cone beam computed tomography. J. Stomatol. Oral Maxillofac. Surg. 2023, 124 (Suppl. S1), 101282. [Google Scholar] [CrossRef] [PubMed]
- Elmarhoumy, S. Cone-beam computed tomography evaluation of the relationship between maxillary transvere dimensions and impacted maxillary canine. Egypt. Dent. J. 2021, 67, 1767–1775. [Google Scholar] [CrossRef]
- Fattahi, H.; Ghaeed, F.; Alipour, A. Association between maxillary canine impaction and arch dimensions. Aust. Orthod. J. 2012, 28, 57–62. [Google Scholar] [PubMed]
- Stanaitytė, R.; Smailienė, D.; Kaduševičius, I. Tooth size discrepancies and dental arch width in patients with palatally and labially impacted maxillary canines. Sveik. Moksl./Health Sci. 2014, 24, 69–74. [Google Scholar] [CrossRef]
- Yan, B.; Sun, Z.; Fields, H.; Wang, L.; Luo, L. Etiologic factors for buccal and palatal maxillary canine impaction: A perspective based on cone-beam computed tomography analyses. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 527–534. [Google Scholar] [CrossRef]
- Cacciatore, G.; Poletti, L.; Sforza, C. Early diagnosed impacted maxillary canines and the morphology of the maxilla: A three-dimensional study. Prog. Orthod. 2018, 19, 20. [Google Scholar] [CrossRef]
- Ali Rizvi, S.A.; Shaheed, M.; Ayub, A.; Ziareen, S.; Masood, O. Association of maxillary transverse discrepancy and impacted maxillary canines. Pak. Oral Dent. J. 2012, 32, 439–443. [Google Scholar]
- Bizzarro, M.; Generali, C.; Maietta, S.; Martorelli, M.; Ferrillo, M.; Flores-Mir, C.; Perillo, L. Association between 3D palatal morphology and upper arch dimensions in buccally displaced maxillary canines early in mixed dentition. Eur. J. Orthod. 2018, 40, 592–596. [Google Scholar] [CrossRef]
- Yassaei, S.; Safi, Y.; Valian, F.; Mohammadi, A. Evaluation of maxillary arch width and palatal volume and depth in patients with maxillary impacted canine by CBCT. Heliyon 2022, 8, 10854. [Google Scholar] [CrossRef]
- Lombardo, L.; Coppola, P.; Siciliani, G. Comparison of dental and alveolar arch forms between different ethnic groups. Int. Orthod. 2015, 13, 462–488. [Google Scholar] [CrossRef]
- D’Oleo-Aracena, M.F.; Arriola-Guillén, L.E.; Rodríguez-Cárdenas, Y.A.; Ruíz-Mora, G.A. Skeletal and dentoalveolar bilateral dimensions in unilateral palatally impacted canine using cone beam computed tomography. Prog. Orthod. 2017, 18, 1–7. [Google Scholar]
- Dager, M.M.; McNamara, J.A.; Baccetti, T.; Franchi, L. Aging in the craniofacial complex: Longitudinal dental arch changes through the sixth decade. Angle Orthod. 2008, 78, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Pasini, M.; Giuca, M.R.; Ligori, S.; Mummolo, S.; Fiasca, F.; Marzo, G.; Quinzi, V. Association between Anatomical Variations and Maxillary Canine Impaction: A Retrospective Study in Orthodontics. Appl. Sci. 2020, 10, 5638. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | No | Mean | SD |
|---|---|---|---|
| Palatal width | 90 | 40.72 | 2.50 |
| Palatal depth | 90 | 20.68 | 2.44 |
| Palatal length | 90 | 29.64 | 3.35 |
| Arch Perimeter | 90 | 60.27 | 3.39 |
| Parameters | Canine Condition | No | Mean | SD | F-Test | p-Value |
|---|---|---|---|---|---|---|
| Palatal width | Control/erupted | 30 | 40.35 | 2.15 | 0.523 | 0.595 |
| Unilateral impacted | 30 | 40.99 | 2.94 | |||
| Bilateral impaction | 30 | 40.84 | 2.38 | |||
| Palatal depth | Control/erupted | 30 | 21.74 | 2.13 | 6.08 | 0.003 * |
| Unilateral impacted | 30 | 20.65 | 3.09 | |||
| Bilateral impaction | 30 | 19.65 | 1.40 | |||
| Palatal length | Control/erupted | 30 | 30.82 | 1.33 | 30.06 | 0.000 * |
| Unilateral impacted | 30 | 26.64 | 3.54 | |||
| Bilateral impaction | 30 | 31.45 | 2.46 | |||
| Arch Perimeter | Control/erupted | 30 | 62.01 | 3.21 | 11.09 | 0.000 * |
| Unilateral impacted | 30 | 58.31 | 3.20 | |||
| Bilateral impaction | 30 | 60.50 | 2.72 |
| Canine Condition | Palatal Width | Palatal Depth | Palatal Length | Arch Perimeter | |
|---|---|---|---|---|---|
| Erupted or Impacted | Pearson correlation | 0.106 | −0.308 ** | −0.251 * | −0.364 ** |
| R2 | 0.011 | 0.122 | 0.005 | 0.132 | |
| Sig. | 0.319 | 0.003 | 0.094 | 0.000 | |
| N | 90 | 90 | 90 | 90 | |
| Model | Unstandardized Coefficients | Standardized Coefficients | t-Test | p-Value | |
|---|---|---|---|---|---|
| B | Std. Error | Beta | |||
| (Constant) | 5.129 | 2.036 | 2.520 | 0.014 | |
| Palatal width | 0.026 | 0.032 | 0.080 | 0.817 | 0.416 |
| Palatal depth | −0.130 | 0.033 | −0.386 | −3.922 | 0.000 |
| Palatal length | 0.046 | 0.025 | 0.187 | 1.859 | 0.067 |
| Perimeter | −0.064 | 0.024 | −0.265 | −2.633 | 0.010 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kareem, F.A.; Rasheed, T.A.; Rauf, A.M.; Jalal, R.A.; Faraj, B.M. Three-Dimensional Measurements of the Palate and Dental Arch Perimeter as Predictors for Maxillary Palatal Canine Impaction—A Cone-Beam Computed Tomography Image Analysis. Diagnostics 2023, 13, 1808. https://doi.org/10.3390/diagnostics13101808
Kareem FA, Rasheed TA, Rauf AM, Jalal RA, Faraj BM. Three-Dimensional Measurements of the Palate and Dental Arch Perimeter as Predictors for Maxillary Palatal Canine Impaction—A Cone-Beam Computed Tomography Image Analysis. Diagnostics. 2023; 13(10):1808. https://doi.org/10.3390/diagnostics13101808
Chicago/Turabian StyleKareem, Fadil Abdullah, Tara Ali Rasheed, Aras Maruf Rauf, Ranj Adil Jalal, and Bestoon Mohammed Faraj. 2023. "Three-Dimensional Measurements of the Palate and Dental Arch Perimeter as Predictors for Maxillary Palatal Canine Impaction—A Cone-Beam Computed Tomography Image Analysis" Diagnostics 13, no. 10: 1808. https://doi.org/10.3390/diagnostics13101808
APA StyleKareem, F. A., Rasheed, T. A., Rauf, A. M., Jalal, R. A., & Faraj, B. M. (2023). Three-Dimensional Measurements of the Palate and Dental Arch Perimeter as Predictors for Maxillary Palatal Canine Impaction—A Cone-Beam Computed Tomography Image Analysis. Diagnostics, 13(10), 1808. https://doi.org/10.3390/diagnostics13101808