
Availability of Third Molars as Donor Teeth for Autotransplantation to Replace Congenitally Absent Second Premolars in Children and Young Adults

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Methods
3. Results
3.1. Distribution of the Congenital Absence of PM2
3.2. Distribution of the Presence of M3
3.3. Development of M3 Related to Age
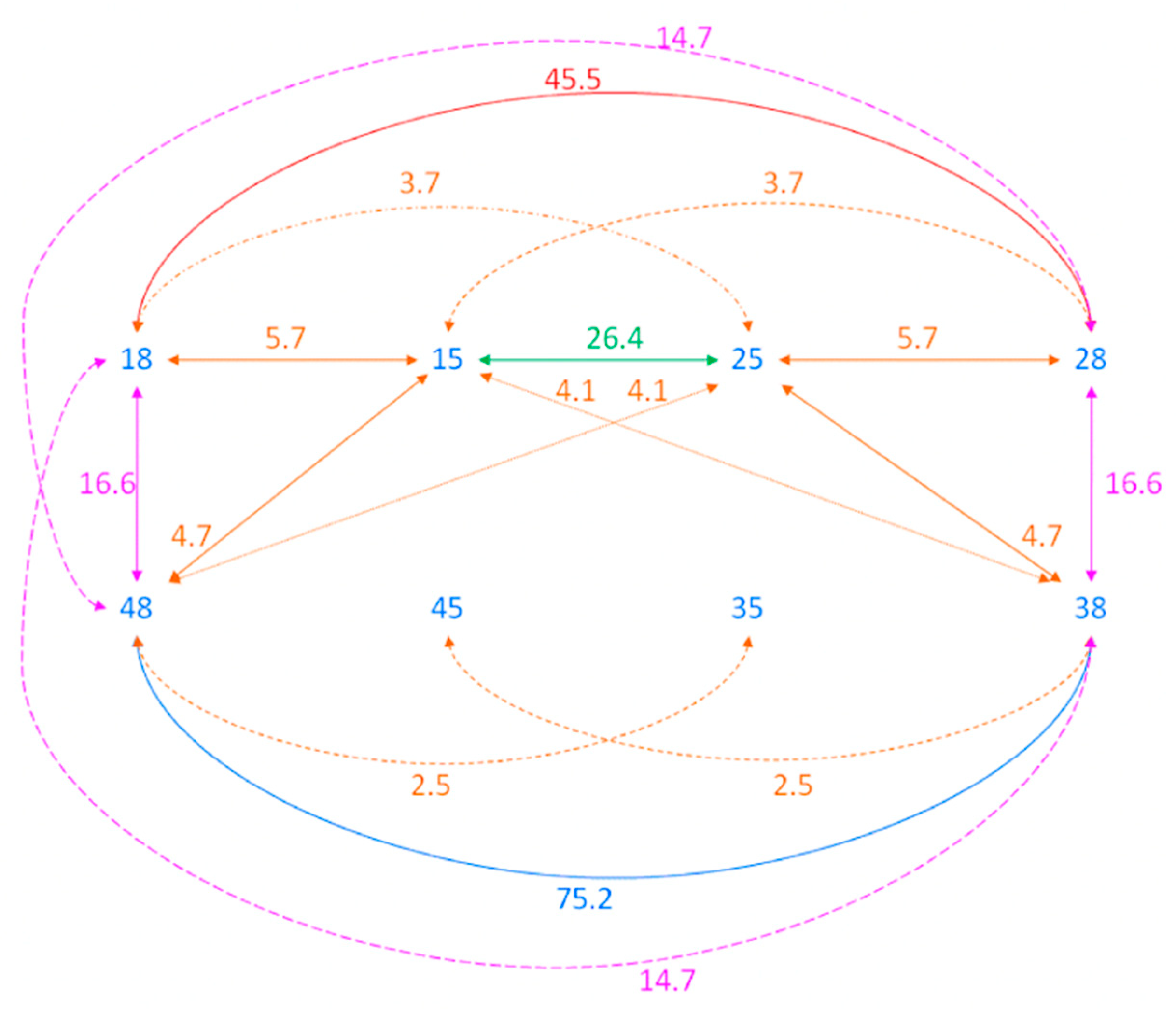
3.4. Association between Congenital Absence of PM2 and M3
4. Discussion
Limitations
5. Conclusions
- In the majority of patients with a congenital absence of PM2, at least one M3 was present and, therefore, it could be considered as an autotransplantation donor. Mostly, one or two PM2s were absent.
- The prevalence of a congenital absence of M3 was statistically significantly increased in relation to the increasing number of congenitally absent PM2.
- The congenital absence of maxillary PM2 was statistically significantly associated with PM2 and M3 absence, while the congenital absence of mandibular PM2 occurred independently from PM2 and M3 absence.
- The best age to perform autotransplantation of immature M3 in relation to their development (1/4 to ¾ of their final root length) is usually between 14 to 17 years.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Medina, A.C. Radiographic study of prevalence and distribution of hypodontia in a pediatric orthodontic population in Venezuela. Pediatr. Dent. 2012, 34, 113–116. [Google Scholar] [PubMed]
- Nordgarden, H.; Jensen, J.L.; Storhaug, K. Reported prevalence of congenitally missing teeth in two Norwegian counties. Community Dent. Health 2002, 19, 258–261. [Google Scholar] [PubMed]
- Rakhshan, V.; Rakhshan, A. Systematic review and meta–analysis of congenitally missing permanent dentition: Sex dimorphism, occurrence patterns, associated factors and biasing factors. Int. Orthod. 2016, 14, 273–294. [Google Scholar] [CrossRef] [PubMed]
- Polder, B.J.; van’t Hof, M.A.; Van der Linden, F.P.; Kuijpers–Jagtman, A.M. A meta–analysis of the prevalence of dental agenesis of permanent teeth. Community Dent. Oral. Epidemiol. 2004, 32, 217–226. [Google Scholar] [CrossRef]
- Endo, T.; Ozoe, R.; Kubota, M.; Akiyama, M.; Shimooka, S. A survey of hypodontia in Japanese orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 29–35. [Google Scholar] [CrossRef]
- Endo, T.; Sanpei, S.; Komatsuzaki, A.; Endo, S.; Takakuwa, A.; Oka, K. Patterns of tooth agenesis in Japanese subjects with bilateral agenesis of mandibular second premolars. Odontology 2013, 101, 216–221. [Google Scholar] [CrossRef]
- Bilińska, M.; Laursen, M.; Plakwicz, P.; Zadurska, M.; Czochrowska, E. Methods of treatment of premolar agenesis—A literature review. Orthod. Forum. 2020, 16, 210–228. [Google Scholar] [CrossRef]
- Sletten, D.W.; Smith, B.M.; Southard, K.A.; Casco, J.S.; Southard, T.E. Retained deciduous mandibular molars in adults: A radiographic study of long–term changes. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 625–630. [Google Scholar] [CrossRef]
- Bjerklin, K.; Al–Najjar, M.; Kårestedt, H.; Andrén, A. Agenesis of mandibular second premolars with retained primary molars: A longitudinal radiographic study of 99 subjects from 12 years of age to adulthood. Eur. J. Orthod. 2008, 30, 254–261. [Google Scholar] [CrossRef]
- Hvaring, C.L.; Øgaard, B.; Stenvik, A.; Birkeland, K. The prognosis of retained primary molars without successors: Infraocclusion, root resorption and restorations in 111 patients. Eur. J. Orthod. 2014, 36, 26–30. [Google Scholar] [CrossRef]
- Ödman, J.; Gröndahl, K.; Lekholm, U.; Thilander, B. The effect of osseointegrated implants on the dento–alveolar development. A clinical and radiographic study in growing pigs. Eur. J. Orthod. 1991, 13, 279–286. [Google Scholar] [CrossRef]
- Thilander, B.; Ödman, J.; Jemt, T. Single implants in the upper incisor region and their relationship to the adjacent teeth. An 8–year follow–up study. Clin. Oral. Impl. Res. 1999, 10, 346–355. [Google Scholar] [CrossRef]
- Farret, M.M.; Farret, M.M. Absence of multiple premolars and ankylosis of deciduous molar with cant of the occlusal plane treated using skeletal anchorage. Angle Orthod. 2015, 85, 134–141. [Google Scholar] [CrossRef]
- Northway, W. Hemisection: One large step toward management of congenitally missing mandibular premolars. Angle Orthod. 2004, 74, 792–799. [Google Scholar]
- Czochrowska, E.M.; Stenvik, A.; Bjercke, B.; Zachrisson, B.U. Outcome of tooth transplantation: Survival and success rates 17–41 years posttreatment. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 110–119. [Google Scholar] [CrossRef]
- Plakwicz, P.; Wojtowicz, A.; Czochrowska, E.M. Survival and success rates of autotransplanted premolars: A prospective study of the protocol for developing teeth. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 229–237. [Google Scholar] [CrossRef]
- Kristerson, L. Autotransplantation of human premolars. A clinical and radiographic study of 100 teeth. Int. J. Oral. Surg. 1985, 14, 200–213. [Google Scholar] [CrossRef]
- Watanabe, Y.; Mohri, T.; Takeyama, M.; Yamaki, M.; Okiji, T.; Saito, C.; Saito, I. Long–term observation of autotransplanted teeth with complete root formation in orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 720–726. [Google Scholar] [CrossRef]
- Chung, C.J.; Han, J.H.; Kim, K.H. The pattern and prevalence of hypodontia in Koreans. Oral. Dis. 2008, 14, 620–625. [Google Scholar] [CrossRef]
- Matalova, E.; Fleischmannova, J.; Sharpe, P.T.; Tucker, A.S. Tooth agenesis: From molecular genetics to molecular dentistry. J. Dent. Res. 2008, 87, 617–623. [Google Scholar] [CrossRef]
- Bhutta, N.; Khan, S.; Saima, R.; Chatha, M.R. Correlation of third molar agenesis with hypodontia in an orthodontic population. Pak. Oral. Dental. J. 2014, 34, 656–659. [Google Scholar]
- Hirakata, C.; Sanpei, S.; Sanpei, S.; Tanaka, S.; Endo, T.; Sekimoto, T. Symmetrical agenesis of the mandibular third molars and agenesis of other teeth in a Japanese orthodontic population. J. Oral. Sci. 2016, 58, 171–176. [Google Scholar] [CrossRef]
- Sanpei, S.; Ishida, R.; Sanpei, S.; Endo, S.; Tanaka, S.; Endo, T.; Sekimoto, T. Patterns of bilateral agenesis of maxillary third molars and agenesis of other teeth. Odontology 2016, 104, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Garib, D.G.; Peck, S.; Gomes, S.C. Increased occurrence of dental anomalies associated with second–premolar agenesis. Angle Orthod. 2009, 79, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Moorrees, C.F.; Fanning, E.A.; Hunt, E.E., Jr. Age variation of formation stages for ten permanent teeth. J. Dent. Res. 1963, 42, 1490–1502. [Google Scholar] [CrossRef]
- Carey, V.; Zeger, S.L.; Diggle, P.J. Modelling multivariate binary data with alternating logistic regressions. Biometrika 1993, 80, 517–526. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, H.C.; Lyu, X.; Shen, G.H.; Deng, X.X.; Li, W.R.; Zhang, X.X.; Feng, H.L. Prevalence of tooth agenesis in adolescent Chinese populations with or without orthodontics. Chin. J. Dent. Res. 2015, 18, 59–65. [Google Scholar]
- Endo, S.; Sanpei, S.; Ishida, R.; Sanpei, S.; Abe, R.; Endo, T. Association between third molar agenesis patterns and agenesis of other teeth in a Japanese orthodontic population. Odontology 2015, 103, 89–96. [Google Scholar] [CrossRef]
- Hashim, H.A.; Al–Said, S. The prevalence and distribution of hypodontia in a sample of Qatari patients. J. Orthod. Sci. 2016, 5, 1–6. [Google Scholar] [CrossRef]
- Dhamo, B.; Vucic, S.; Kuijpers, M.A.; Jaddoe, V.W.; Hofman, A.; Wolvius, E.B.; Ongkosuwito, E.M. The association between hypodontia and dental development. Clin. Oral. Investig. 2016, 20, 1347–1354. [Google Scholar] [CrossRef]
- Al–Abdallah, M.; AlHadidi, A.; Hammad, M.; Al–Ahmad, H.; Saleh, R. Prevalence and distribution of dental anomalies: A comparison between maxillary and mandibular tooth agenesis. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 793–798. [Google Scholar] [CrossRef]
- Mani, S.A.; Mohsin, W.S.; John, J. Prevalence and patterns of tooth agenesis among Malay children. Southeast Asian J. Trop. Med. Public Health 2014, 45, 490–498. [Google Scholar]
- Gelbrich, B.; Hirsch, A.; Dannhauer, K.H.; Gelbrich, G. Agenesis of second premolars and delayed dental maturation. J. Orofac. Orthop. 2015, 76, 338–350. [Google Scholar] [CrossRef]
- Lebbe, A.; Cadenas de Llano–Pérula, M.; Thevissen, P.; Verdonck, A.; Fieuws, S.; Willems, G. Dental development in patients with agenesis. Int. J. Legal. Med. 2017, 131, 537–546. [Google Scholar] [CrossRef]
- Lee, S.H.; Lee, J.Y.; Park, H.K.; Kim, Y.K. Development of third molars in Korean juveniles and adolescents. Forensic. Sci. Int. 2009, 188, 107–111. [Google Scholar] [CrossRef]


{kind=link}
| Gender/Age | 10–13 Years Old | 14–17 Years Old | 18–22 Years Old | Total |
|---|---|---|---|---|
| Females | 47 (57.3%) | 27 (32.9%) | 8 (9.8%) | 82 (100%) |
| Males | 26 (53.1%) | 18 (36.7%) | 5 (10.2%) | 49 (100%) |
| Total | 73 (55.7%) | 45 (34.3%) | 13 (9.9%) | 131 (100%) |
| Gender/Tooth | 15 | 25 | 35 | 45 |
|---|---|---|---|---|
| Females (N = 82) | 22 (26.8%) | 21 (25.6%) | 58 (70.7%) | 66 (80.5%) |
| Males (N = 49) | 6 (12.2%) | 6 (12.2%) | 36 (73.5%) | 36 (73.5%) |
| Total (N = 131) | 28 (21.4%) | 27 (20.7%) | 94 (71.8%) | 102 (77.9%) |
| Absent Tooth | 15 | 25 | 35 | 45 | 15 & 25 | 15 & 35 | 25 & 45 | 35 & 45 | 15 & 25 & 35 | 15 & 35 & 45 | 25 & 35 & 45 | All Absent |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Females 82/63% | 1/1.2% | 1/1.2% | 8/9.8% | 20/24.4% | 2/2.4% | 3/3.7% | 0/0% | 26/31.7% | 1/1.2% | 3/3.7% | 5/6.1% | 12/14.3% |
| Males 49/37% | 1/2% | 0/0% | 12/24.5% | 10/20.4% | 0/0% | 0/0% | 2/4.1% | 19/38.8% | 0/0% | 1/0.8% | 0/0% | 4/8.2% |
| Total 131/100% | 2/1.5% | 1/0.8% | 20/15.3% | 30/22.9% | 2/1.5% | 3/2.3% | 2/1.5% | 45/34.5% | 1/0.8% | 4/2% | 5/3.8% | 16/12.2% |
| Gender/Tooth | 18 | 28 | 38 | 48 |
|---|---|---|---|---|
| Females (N = 82) | 49 (59.7%) | 53 (64.6%) | 39 (47.5%) | 42 (51.2%) |
| Males (N = 49) | 32 (66.3%) | 33 (67.3%) | 31 (63.3%) | 32 (66.3%) |
| Total (N = 131) | 81 (61.8%) | 86 (65.7%) | 70 (53.4%) | 74 (56.5%) |
| Missing Tooth | All Absent | 18 | 28 | 38 | 48 | 18 & 28 | 28 & 38 | 38 & 48 | 18 & 28 & 38 | 18 & 28 & 48 | 18 & 38 & 48 | 28 & 38 & 48 | All Present |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Females 82/ 63% | 23/28% | 2/2.4% | 4/4.9% | 0/ 0% | 2/2.4% | 9/ 11% | 1/ 1.2% | 1/1.2% | 1/0.8% | 3/3.7% | 1/1.2% | 2/2.4% | 33/ 40.2% |
| Males 49/ 37% | 9/ 18.4% | 1/ 2% | 3/6.1% | 1/ 2% | 1/ 2% | 1/ 2% | 0/ 0% | 2/ 4.1% | 2/4.1% | 3/6.1% | 2/ 4.1% | 1/ 2% | 23/46.9% |
| Total 131/100% | 32/ 24.4% | 3/2.3% | 7/5.3% | 1/0.8% | 3/2.3% | 10/7.6% | 1/0.8% | 3/2.3% | 3/2.3% | 6/4.6% | 3/2.3% | 3/2.3% | 56/42.7% |
| Number of Absent PM2 | Number of Absent M3 | |||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | Total | |
| 1 | 31 (58.5%) | 6 (11.3%) | 3 (5.7%) | 5 (9.4%) | 8 (15.1%) | 53 (100%) |
| 2 | 23 (44.2%) | 6 (11.5%) | 7 (13.5%) | 5 (9.6%) | 11 (21.1%) | 52 (100%) |
| 3 | 2 (20%) | 1 (10%) | 2 (20%) | 2 (20%) | 3 (30%) | 10 (100%) |
| 4 | 0 (0%) | 2 (12.5%) | 2 ( 12.5%) | 2 (12.5%) | 10 (62.5%) | 16 (100%) |
| Total | 56 | 15 | 14 | 14 | 32 | |
| Stage of M3 Development According to Moorreess et al [25]. | 10–13 years | 14–17 years | 18–22 years | ||||||
|---|---|---|---|---|---|---|---|---|---|
| All (100%) | Females (100%) | Males (100%) | All (100%) | Females (100%) | Males (100%) | All (100%) | Females (100%) | Males (100%) | |
| Crown development (Ci, Cco, Coc, Cr1/2, Cr3/4) | 74 (49.3%) | 41 (44%) | 33 (57.9%) | 22 (18%) | 8 (10.7%) | 14 (29.8%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Final crown and initial root development (Crc, Ri, Cli) | 59 (39.3%) | 41 (44%) | 18 (31.6%) | 32 (26.2%) | 23 (30.7%) | 9 (19.1%) | 10 (30.3%) | 9 (52.9%) | 1 (6.2%) |
| Root length quarter (R ¼) | 13 (8.7%) | 8 (8.6%) | 5 (8.8%) | 16 (13.1%) | 12 (16%) | 4 (8.5%) | 0 (0%) | 0 (0%) | 0 |
| Root length half (R ½) | 4 (2.7%) | 3 (0.4%) | 1 (1.7%) | 22 (18%) | 16 (21.3%) | 6 (12.8%) | 7 (21.2%) | 4 (23.5%) | 3 (18.7%) |
| Root length three-quarters (R ¾) | 0 (0%) | 0 (0%) | 0 (0%) | 24 (19.7%) | 16 (21.3%) | 8 (17%) | 7 (21.2%) | 3 (17.6%) | 4 (25%) |
| Final root development and apex closure (Rc, A½, Ac) | 0 (0%) | 0 (0%) | 0 (0%) | 6 (4.9%) | 0 (0%) | 6 (12.8%) | 9 (27.2%) | 1 (5.9%) | 8 (50%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bilińska, M.; Burzykowski, T.; Plakwicz, P.; Zadurska, M.; Czochrowska, E.M. Availability of Third Molars as Donor Teeth for Autotransplantation to Replace Congenitally Absent Second Premolars in Children and Young Adults. Diagnostics 2023, 13, 1874. https://doi.org/10.3390/diagnostics13111874
Bilińska M, Burzykowski T, Plakwicz P, Zadurska M, Czochrowska EM. Availability of Third Molars as Donor Teeth for Autotransplantation to Replace Congenitally Absent Second Premolars in Children and Young Adults. Diagnostics. 2023; 13(11):1874. https://doi.org/10.3390/diagnostics13111874
Chicago/Turabian StyleBilińska, Małgorzata, Tomasz Burzykowski, Paweł Plakwicz, Małgorzata Zadurska, and Ewa Monika Czochrowska. 2023. "Availability of Third Molars as Donor Teeth for Autotransplantation to Replace Congenitally Absent Second Premolars in Children and Young Adults" Diagnostics 13, no. 11: 1874. https://doi.org/10.3390/diagnostics13111874
APA StyleBilińska, M., Burzykowski, T., Plakwicz, P., Zadurska, M., & Czochrowska, E. M. (2023). Availability of Third Molars as Donor Teeth for Autotransplantation to Replace Congenitally Absent Second Premolars in Children and Young Adults. Diagnostics, 13(11), 1874. https://doi.org/10.3390/diagnostics13111874