
Effect of the Hematocrit and Storage Temperature of Dried Blood Samples in the Serological Study of Mumps, Measles and Rubella

 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
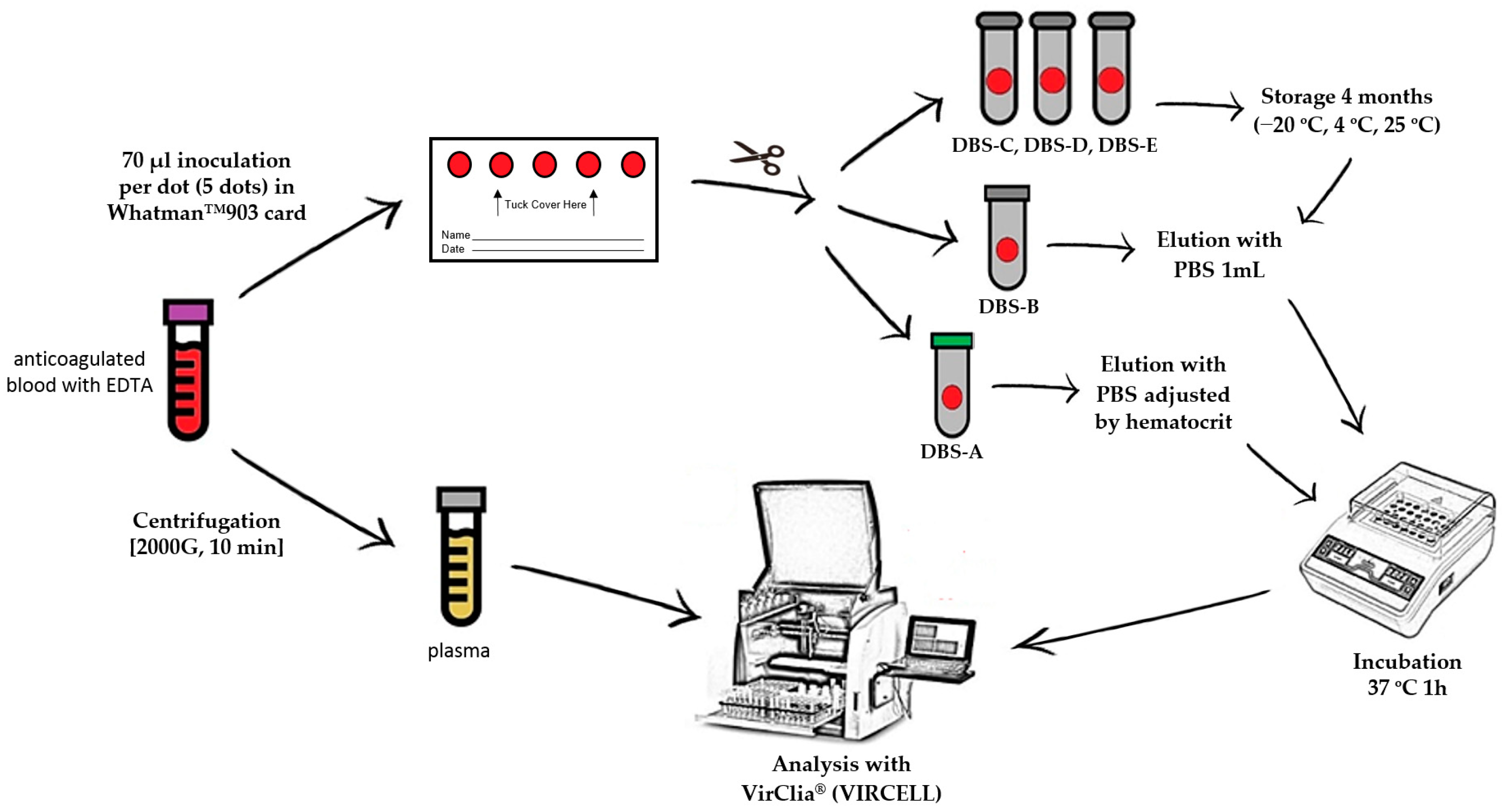
2.2. Sample Collection and Storage
2.3. DBS Elution
2.4. Serological Testing
2.5. Statistical Analysis
3. Results
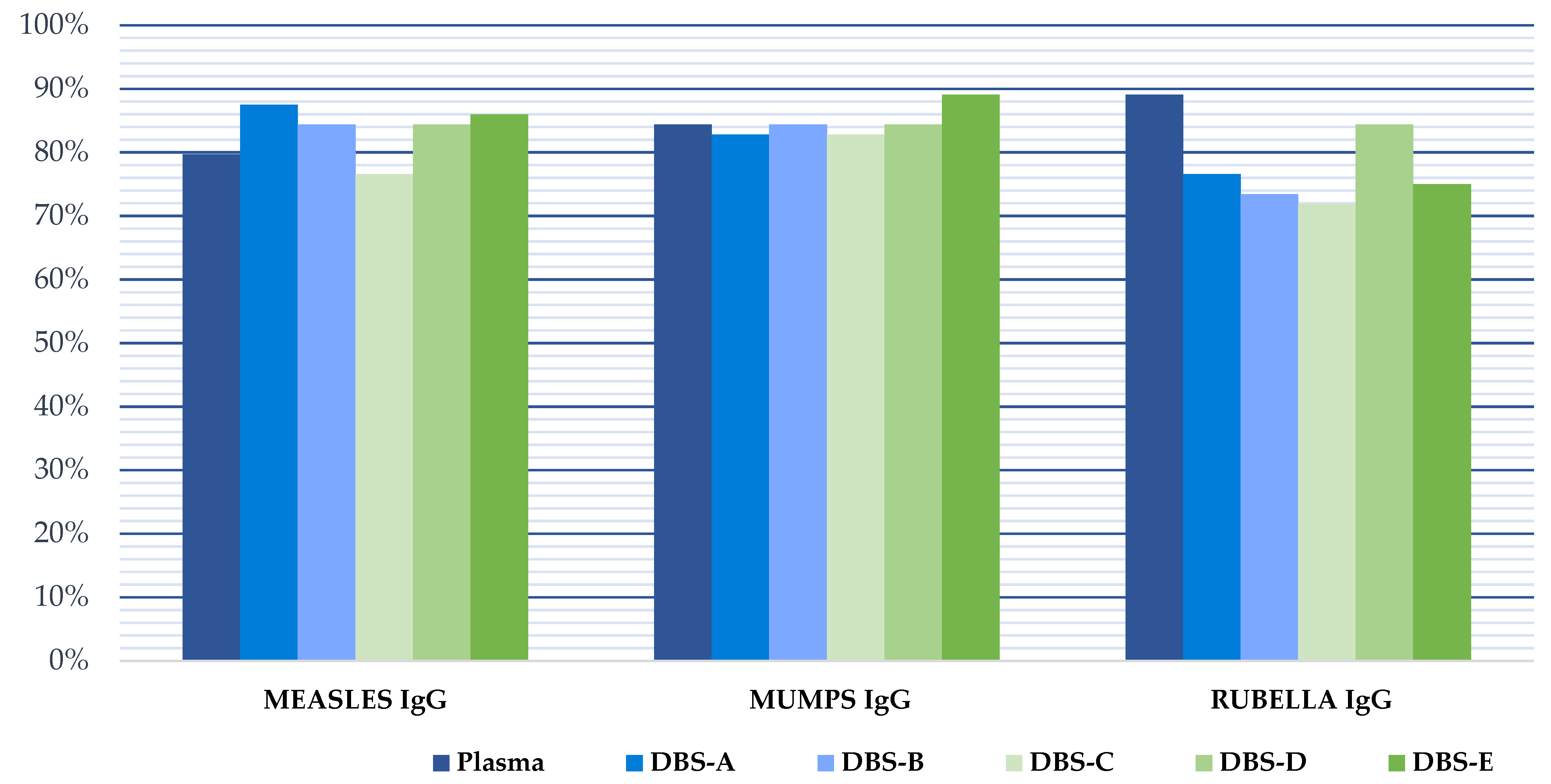
3.1. Immunization Levels in Plasma
3.2. Correlation between DBS and Plasma
3.2.1. Effect of the Hematocrit
3.2.2. DBS Stability
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schmidt, V. Ivar Christian Bang (1869–1918), founder of modern clinical microchemistry. Clin. Chem. 1986, 32, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, R. Blood Screening for Phenylketonuria. JAMA 1961, 178, 863. [Google Scholar] [CrossRef]
- Grüner, N.; Stambouli, O.; Ross, R.S. Dried blood spots--preparing and processing for use in immunoassays and in molecular techniques. J. Vis. Exp. 2015, 13, 52619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hannon, W.H.; Therell, B.L. Overview of the history and applications of dried blood spot samples. In Dried Blood Spots: Applications and Techniques; Li, W., Lee, M.S., Eds.; Wiley Hoboken: East Hanover, NJ, USA, 2014; Volume 3, pp. 3–15. [Google Scholar]
- Su, X.; Carlson, B.F.; Wang, X.; Li, X.; Zhang, Y.; Montgomery, J.P.; Ding, Y.; Wagner, A.L.; Gillespie, B.; Boulton, M.L. Dried blood spots: An evaluation of utility in the field. J. Infect. Public Health 2018, 11, 373–376. [Google Scholar] [CrossRef]
- Carrasco, T.; Barquín, D.; Ndarabu, A.; Fernández-Alonso, M.; Rubio-Garrido, M.; Carlos, S.; Makonda, B.; Holguín, Á.; Reina, G. HCV Diagnosis and Sequencing Using Dried Blood Spots from Patients in Kinshasa (DRC): A Tool to Achieve WHO 2030 Targets. Diagnostics 2021, 11, 522. [Google Scholar] [CrossRef] [PubMed]
- Catlett, B.; Hajarizadeh, B.; Cunningham, E.; Wolfson-Stofko, B.; Wheeler, A.; Khandaker-Hussain, B.; Feld, J.J.; Martró, E.; Chevaliez, S.; Pawlotsky, J.M.; et al. Diagnostic Accuracy of Assays Using Point-of-Care Testing or Dried Blood Spot Samples for the Determination of Hepatitis C Virus RNA: A Systematic Review. J. Infect. Dis. 2022, 226, 1005–1021. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Garrido, M.; Ndarabu, A.; Reina, G.; Barquín, D.; Fernández-Alonso, M.; Carlos, S.; Holguín, Á. Utility Of POC Xpert HIV-1 Tests For Detection-Quantification Of Complex HIV Recombinants Using Dried Blood Spots From Kinshasa, D. R. Congo. Sci. Rep. 2019, 9, 5679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barquín, D.; Ndarabu, A.; Carlos, S.; Fernández-Alonso, M.; Rubio-Garrido, M.; Makonda, B.; Holguín, Á.; Reina, G. HIV-1 diagnosis using dried blood spots from patients in Kinshasa, DRC: A tool to detect misdiagnosis and achieve World Health Organization 2030 targets. Int. J. Infect. Dis. 2021, 111, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Øverbø, J.; Aziz, A.; Zaman, K.; Julin, C.H.; Qadri, F.; Stene-Johansen, K.; Biswas, R.; Islam, S.; Bhuiyan, T.R.; Haque, W.; et al. Stability and Feasibility of Dried Blood Spots for Hepatitis E Virus Serology in a Rural Setting. Viruses 2022, 14, 2525. [Google Scholar] [CrossRef]
- Ryan, P.; Valencia, J.; Cuevas, G.; Troya, J.; Torres-Macho, J.; Muñoz-Gómez, M.J.; Muñoz-Rivas, N.; Canorea, I.; Vázquez-Morón, S.; Resino, S. HIV screening and retention in care in people who use drugs in Madrid, Spain: A prospective study. Infect. Dis. Poverty 2021, 10, 111. [Google Scholar] [CrossRef]
- Bajis, S.; Grebely, J.; Hajarizadeh, B.; Applegate, T.; Marshall, A.D.; Harrod, M.E.; Byrne, J.; Bath, N.; Read, P.; Edwards, M.; et al. Hepatitis C virus testing, liver disease assessment and treatment uptake among people who inject drugs pre- and post-universal access to direct-acting antiviral treatment in Australia: The LiveRLife study. J. Viral Hepat. 2020, 27, 281–293. [Google Scholar] [CrossRef] [PubMed]
- International Air Transport Association Dangerous (IATA) Goods Regulations (62nd Edition). Available online: https://www.iata.org/contentassets/b08040a138dc4442a4f066e6fb99fe2a/dgr-62-en-3.6.2.pdf (accessed on 21 November 2022).
- WHO Manual for HIV Drug Resistance Testing Using Dried Blood Spot Specimens. Available online: https://www.who.int/publications/i/item/9789240009424 (accessed on 24 November 2022).
- Amini, F.; Auma, E.; Hsia, Y.; Bilton, S.; Hall, T.; Ramkhelawon, L.; Heath, P.T.; Le Doare, K. Reliability of dried blood spot (DBS) cards in antibody measurement: A systematic review. PLoS ONE 2021, 16, e0248218. [Google Scholar] [CrossRef] [PubMed]
- Eick, G.; Urlacher, S.S.; McDade, T.W.; Kowal, P.; Snodgrass, J.J. Validation of an Optimized ELISA for Quantitative Assessment of Epstein-Barr Virus Antibodies from Dried Blood Spots. Biodemography Soc. Biol. 2016, 62, 222–233. [Google Scholar] [CrossRef] [Green Version]
- Sultana, R.; Bhuiyan, T.R.; Sathi, A.S.; Sharmin, S.; Yeasmin, S.; Uddin, M.I.; Bhuiyan, S.; Mannoor, K.; Karim, M.M.; Zaman, K.; et al. Developing and validating a modified enzyme linked immunosorbent assay method for detecting HEV IgG antibody from dried blood spot (DBS) samples in endemic settings. Microbes Infect. 2022, 24, 104890. [Google Scholar] [CrossRef] [PubMed]
- Palmer, O.M.P.; Dasgupta, A. Review of the Preanalytical Errors That Impact Therapeutic Drug Monitoring. Ther. Drug Monit. 2021, 43, 595–608. [Google Scholar] [CrossRef]
- Whittaker, K.; Mao, Y.-Q.; Lin, Y.; Zhang, H.; Zhu, S.; Peck, H.; Huang, R.-P. Dried blood sample analysis by antibody array across the total testing process. Sci. Rep. 2021, 11, 20549. [Google Scholar] [CrossRef]
- Rodríguez-Galet, A.; Rubio-Garrido, M.; Valadés-Alcaraz, A.; Rodríguez-Domínguez, M.; Galán, J.C.; Ndarabu, A.; Reina, G.; Holguín, A. Immune surveillance for six vaccinable pathogens using paired plasma and dried blood spots in HIV infected and uninfected children in Kinshasa. Sci. Rep. 2022, 12, 7920. [Google Scholar] [CrossRef]
- Eisenberg, A.L.; Patel, E.U.; Packman, Z.; Fernandez, R.; Piwowar-Manning, E.; Hamilton, E.L.; MacPhail, C.; Hughes, J.P.; Pettifor, A.; Kallas, E.; et al. Short Communication: Dried Blood Spots Stored at Room Temperature Should Not Be Used for HIV Incidence Testing. AIDS Res. Hum. Retroviruses 2018, 34, 1013–1016. [Google Scholar] [CrossRef]
- McAllister, G.; Shepherd, S.; Templeton, K.; Aitken, C.; Gunson, R. Long term stability of HBsAg, anti-HBc and anti-HCV in dried blood spot samples and eluates. J. Clin. Virol. 2015, 71, 10–17. [Google Scholar] [CrossRef]
- Singh, M.P.; Majumdar, M.; Budhathoki, B.; Goyal, K.; Chawla, Y.; Ratho, R.K. Assessment of dried blood samples as an alternative less invasive method for detection of Hepatitis E virus marker in an outbreak setting. J. Med. Virol. 2013, 86, 713–719. [Google Scholar] [CrossRef]
- Manak, M.M.; Hack, H.R.; Shutt, A.L.; Danboise, B.A.; Jagodzinski, L.L.; Peel, S.A. Stability of Human Immunodeficiency Virus Serological Markers in Samples Collected as HemaSpot and Whatman 903 Dried Blood Spots. J. Clin. Microbiol. 2018, 56, e00933-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moat, S.J.; Zelek, W.M.; Carne, E.; Ponsford, M.J.; Bramhall, K.; Jones, S.; El-Shanawany, T.; Wise, M.J.; Thomas, A.; George, C.; et al. Development of a high-throughput SARS-CoV-2 antibody testing pathway using dried blood spot specimens. Ann. Clin. Biochem. Int. J. Biochem. Lab. Med. 2021, 58, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, C.M.; Wagmann, L.; Meyer, M.R. Development, validation, and application of a quantitative volumetric absorptive microsampling–based method in finger prick blood by means of LC-HRMS/MS applicable for adherence monitoring of antipsychotics. Anal. Bioanal. Chem. 2021, 413, 1729–1737. [Google Scholar] [CrossRef] [PubMed]
- Martens-Lobenhoffer, J.; Hinderhofer, M.; Tröger, U.; Bode-Böger, S.M. Stability of ceftolozane in human plasma and dried blood spots: Implications for transport and storage. J. Pharmacol. Toxicol. Methods 2020, 103, 106692. [Google Scholar] [CrossRef]
- Crawshaw, A.F.; Farah, Y.; Deal, A.; Rustage, K.; E Hayward, S.; Carter, J.; Knights, F.; Goldsmith, L.P.; Campos-Matos, I.; Wurie, F.; et al. Defining the determinants of vaccine uptake and undervaccination in migrant populations in Europe to improve routine and COVID-19 vaccine uptake: A systematic review. Lancet Infect. Dis. 2022, 22, e254–e266. [Google Scholar] [CrossRef]
- Hinman, A.; Orenstein, W. Immunisation practice in developed countries. Lancet 1990, 335, 707–710. [Google Scholar] [CrossRef]
- Holroyd, T.A.; Schiaffino, F.; Chang, R.H.; Wanyiri, J.W.; Saldanha, I.J.; Gross, M.; Moss, W.J.; Hayford, K. Diagnostic accuracy of dried blood spots for serology of vaccine-preventable diseases: A systematic review. Expert Rev. Vaccines 2022, 21, 185–200. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Male | Female | Total | |
|---|---|---|---|
| n (%) | 31 (48%) | 33 (52%) | 64 |
| Median age at sampling [IQR] | 42.8 [37.6–58.3] | 41.8 [31.6–56.7] | 42.6 [36.5–58.1] |
| Age Groups, n (%) | |||
| <30 | 5 (16%) | 7 (21%) | 12 (18.8%) |
| 30–45 | 12 (39%) | 12 (36%) | 24 (37.5%) |
| 45–60 | 7 (23%) | 8 (24%) | 15 (23.4%) |
| >60 | 7 (23%) | 6 (18%) | 13 (20.3%) |
| Hematocrit, median [IQR] | 42.7 [38.9–45.7] | 39.8 [37.2–41.7] | 41.0 [37.8–43.6] |
| Age groups | |||
| <30 | 42.7% | 40.5% | 41.9% |
| 30–45 | 44.8% | 41.0% | 42.1% |
| 45–60 | 43.2% | 38.6% | 41.0% |
| >60 | 38.2% | 38.1% | 38.2% |
| Pathogen immunity (plasma) | |||
| Measles IgG (%) | 71.0% | 87.9% | 79.7% |
| Age groups | |||
| <30 | 40.0% | 85.7% | 66.7% |
| 30–45 | 58.3% | 91.7% | 75.0% |
| 45–60 | 100% | 87.5% | 93.3% |
| >60 | 85.7% | 83.3% | 84.6% |
| Mumps IgG (%) | 80.6% | 87.9% | 84.4% |
| Age groups | |||
| <30 | 100% | 85.7% | 91.7% |
| 30–45 | 75.0% | 91.7% | 83.3% |
| 45–60 | 71.4% | 87.5% | 80.0% |
| >60 | 85.7% | 83.3% | 84.6% |
| Rubella IgG (%) | 87.1% | 90.9% | 89.1% |
| Age groups | |||
| <30 | 80.0% | 85.7% | 83.3% |
| 30–45 | 91.7% | 91.7% | 91.7% |
| 45–60 | 71.4% | 100% | 86.7% |
| >60 | 100% | 83.3% | 92.3% |
| Plasma/DBS-A | Plasma/DBS-B | Plasma/DBS-C | Plasma/DBS-D | Plasma/DBS-E | |
|---|---|---|---|---|---|
| MEASLES | 0.939 | 0.948 | 0.878 | 0.889 | 0.762 |
| MUMPS | 0.914 | 0.928 | 0.905 | 0.917 | 0.882 |
| RUBELLA | 0.953 | 0.940 | 0.951 | 0.925 | 0.872 |
| MEASLES * | MUMPS ** | RUBELLA *** | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sen | Spe | PPV | NPV | Sen | Spe | PPV | NPV | Sen | Spe | PPV | NPV | ||
| DBS-A | Plasma cut-off | 100% | 57.1% | 94.4% | 100% | 100% | 87.5% | 98.2% | 100% | 100% | 60% | 96.6% | 100% |
| DBS cut-off ** | 100% | 87.5% | 98.1% | 100% | 98.1% | 100% | 100% | 90% | 84.2% | 80% | 98% | 30.8% | |
| DBS-B | Plasma cut-off | 100% | 60% | 96.2% | 100% | 100% | 88.9% | 98.2% | 100% | 100% | 60% | 96.6% | 100 |
| DBS cut-off | 100% | 87.5% | 98.1% | 100% | 100% | 100% | 100% | 100% | 82.5% | 100% | 100% | 33.3% | |
| DBS-C | Plasma cut-off | 96.1% | 50% | 94.2% | 60% | 100% | 87.5% | 98.2% | 100% | 98.2% | 60% | 96.6% | 75% |
| DBS cut-off | 92.2% | 87.5% | 97.9% | 63.3% | 98.1% | 100% | 100% | 90% | 80.7% | 100% | 100% | 31.3% | |
| DBS-D | Plasma cut-off | 98% | 42.9% | 92.6% | 75% | 100% | 62.5% | 94.7% | 100% | 100% | 60% | 96.6% | 100% |
| DBS cut-off | 94.1% | 62.5% | 94.1% | 62.5% | 98.1% | 88.9% | 98.1% | 88.9% | 84.2% | 100% | 100% | 35.7% | |
| DBS-E | Plasma cut-off | 96% | 0% | 88.9% | 0% | 100% | 28.6% | 91.5% | 100% | 100% | 40% | 95% | 100% |
| DBS cut-off | 94.1% | 50% | 92.3% | 57.1% | 98.1% | 55.6% | 93% | 83.3% | 80.7% | 80% | 97.9% | 26.7% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Mateos, M.; Jaso, J.; Martínez de Aguirre, P.; Carlos, S.; Fernández-Ciriza, L.; Holguín, Á.; Reina, G. Effect of the Hematocrit and Storage Temperature of Dried Blood Samples in the Serological Study of Mumps, Measles and Rubella. Diagnostics 2023, 13, 349. https://doi.org/10.3390/diagnostics13030349
Rodríguez-Mateos M, Jaso J, Martínez de Aguirre P, Carlos S, Fernández-Ciriza L, Holguín Á, Reina G. Effect of the Hematocrit and Storage Temperature of Dried Blood Samples in the Serological Study of Mumps, Measles and Rubella. Diagnostics. 2023; 13(3):349. https://doi.org/10.3390/diagnostics13030349
Chicago/Turabian StyleRodríguez-Mateos, Mariano, Javier Jaso, Paula Martínez de Aguirre, Silvia Carlos, Leire Fernández-Ciriza, África Holguín, and Gabriel Reina. 2023. "Effect of the Hematocrit and Storage Temperature of Dried Blood Samples in the Serological Study of Mumps, Measles and Rubella" Diagnostics 13, no. 3: 349. https://doi.org/10.3390/diagnostics13030349
APA StyleRodríguez-Mateos, M., Jaso, J., Martínez de Aguirre, P., Carlos, S., Fernández-Ciriza, L., Holguín, Á., & Reina, G. (2023). Effect of the Hematocrit and Storage Temperature of Dried Blood Samples in the Serological Study of Mumps, Measles and Rubella. Diagnostics, 13(3), 349. https://doi.org/10.3390/diagnostics13030349