
The Bidirectional Relationship between Periodontal Disease and Diabetes Mellitus—A Review

 , , ,
, , ,  ,
,  and
and 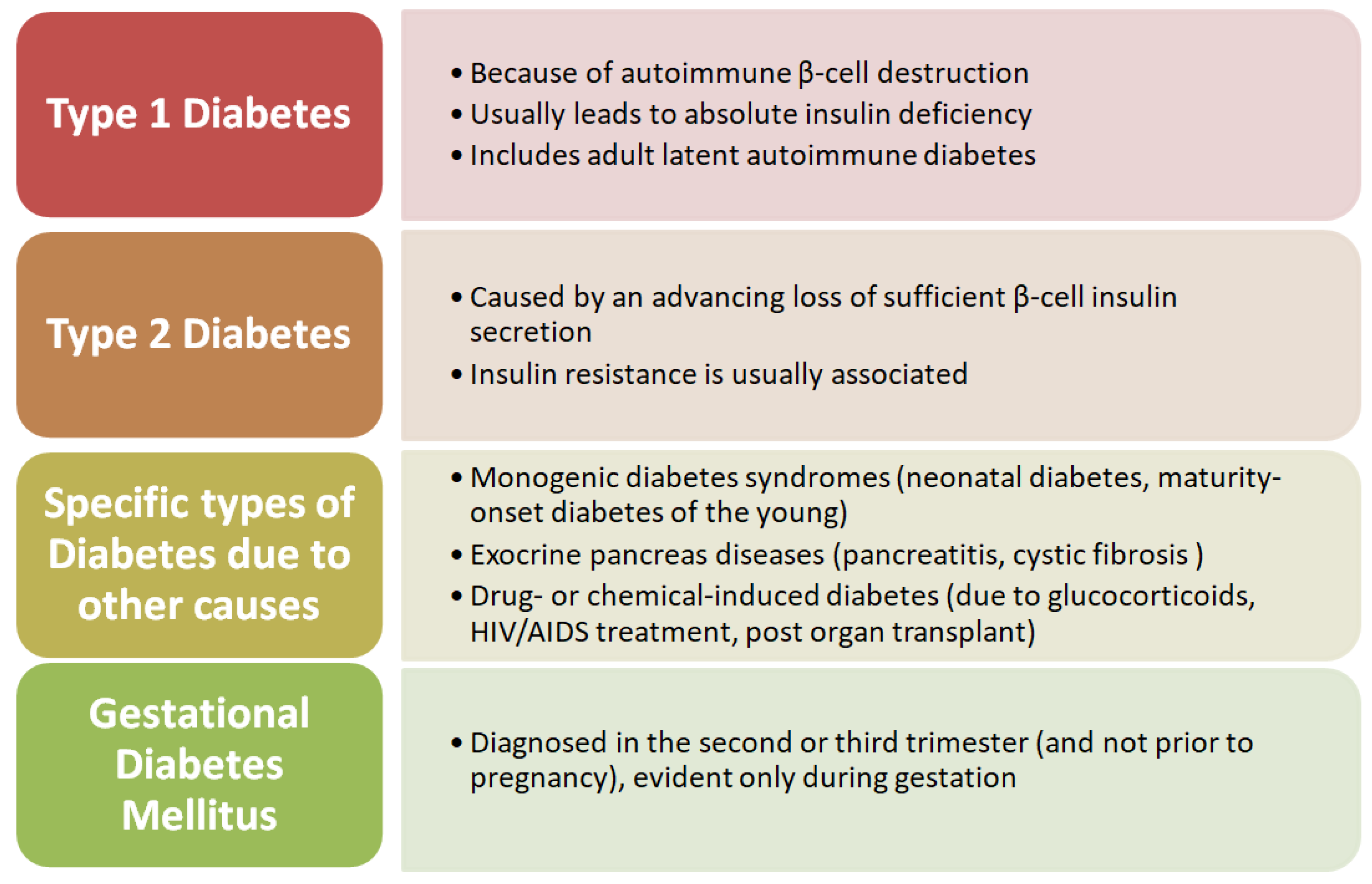{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Etiopathogenesis and Clinical Correlations between Diabetes Mellitus and Periodontal Disease
3. Diabetes Mellitus
4. Microvascular Complications
5. Periodontal Disease
6. Oral Microbiota
7. Smoking as a Predisposing Factor for Periodontal Disease and Diabetes
8. Pro and Anti-inflammatory Factors
9. Common Genes and Pathways in Periodontal Disease and Diabetes
10. Present Possibilities and Future Challenges
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72. [Google Scholar]
- Auerbacher, M.; Gebetsberger, L.; Kaisarly, D.; Schmidmaier, R.; Hickel, R.; Drey, M. Oral health in patients with neurodegenerative and cerebrovascular disease: A retrospective study. Disabil. Rehabil. 2022, 22, 1–9. [Google Scholar] [CrossRef]
- De Sire, A.; Invernizzi, M.; Ferrillo, M.; Gimigliano, F.; Baricich, A.; Cisari, C.; De Marchi, F.; Foglio Bonda, P.L.; Mazzini, L.; Migliario, M. Functional status and oral health in patients with amyotrophic lateral sclerosis: A cross-sectional study. NeuroRehabilitation 2021, 48, 49–57. [Google Scholar] [CrossRef]
- Ferrillo, M.; Migliario, M.; Marotta, N.; Lippi, L.; Antonelli, A.; Calafiore, D.; Ammendolia, V.; Fortunato, L.; Renò, F.; Giudice, A.; et al. Oral Health in Breast Cancer Women with Vitamin D Deficiency: A Machine Learning Study. J. Clin. Med. 2022, 11, 4662. [Google Scholar] [CrossRef] [PubMed]
- Covello, F.; Ruoppolo, G.; Carissimo, C.; Zumbo, G.; Ferrara, C.; Polimeni, A.; Vekeozza, I. Multiple Sclerosis: Impact on Oral Hygiene, Dysphagia, and Quality of Life. Int. J. Environ. Res. Public Health 2020, 17, 3979. [Google Scholar] [CrossRef] [PubMed]
- Martu, M.A.; Solomon, S.M.; Toma, V.; Maftei, G.A.; Iovan, A.; Gamen, A.; Hurjui, L.; Rezus, E.; Foia, L.; Forna, N.C. The importance of cytokines in periodontal disease and rheumatoid arthritis. Review. Rom. J. Oral Rehabil. 2019, 11, 220–240. [Google Scholar]
- Martu, M.A.; Maftei, G.A.; Sufaru, I.G.; Jelihovschi, I.; Luchian, I.; Hurjui, L.; Martu, I.; Pasarin, L. COVID-19 and Periodontal Disease-Ethiopathogenic and Clinical Implications. Rom. J. Oral Rehab. 2020, 12, 116–124. [Google Scholar]
- Zhou, X.; Zhang, W.; Liu, X.; Zhang, W.; Li, Y. Interrelationship between diabetes and periodontitis: Role of hyperlipidemia. Arch. Oral Biol. 2015, 60, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M.; Bissett, S.M. Periodontitis and diabetes. Br. Dent. J. 2019, 227, 577–584. [Google Scholar] [CrossRef]
- Zheng, M.; Wang, C.; Ali, A.; Shih, Y.A.; Xie, Q.; Guo, C. Prevalence of periodontitis in people clinically diagnosed with diabetes mellitus: A meta-analysis of epidemiologic studies. Acta Diabetol. 2021, 58, 1307–1327. [Google Scholar] [CrossRef]
- Polak, D.; Shapira, L. An update on the evidence for pathogenic mechanisms that may link periodontitis and diabetes. J. Clin. Periodontol. 2018, 45, 150–166. [Google Scholar] [CrossRef] [PubMed]
- Nibali, L.; Gkranias, N.; Mainas, G.; Di Pino, A. Periodontitis and implant complications in diabetes. Periodontol. 2000 2022, 90, 88–105. [Google Scholar] [CrossRef] [PubMed]
- Eke, P.I.; Borgnakke, W.S.; Genco, R.J. Recent epidemiologic trends in periodontitis in the USA. Periodontol. 2000 2020, 82, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Quadri, M.F.A.; Fageeh, H.I.; Ibraheem, W.; Jessani, A. A case–control study of type 2 diabetes mellitus and periodontitis in Saudi Arabian adults. J. Multidiscip. Healthc. 2020, 13, 1741–1748. [Google Scholar] [CrossRef]
- Sonnenschein, S.K. Generalized Severe Periodontitis and Periodontal Abscess in Type 2 Diabetes: A Case Report. Balk. J. Dent. Med. 2016, 20, 111–116. [Google Scholar] [CrossRef]
- Lovic, D.; Piperidou, A.; Zografou, I.; Grassos, H.; Pittaras, A.; Manolis, A. The growing epidemic of diabetes mellitus. Curr. Vasc. Pharmacol. 2020, 18, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef]
- Nazir, M.; Al-Ansari, A.; Al-Khalifa, K.; Alhareky, M.; Gaffar, B.; Almas, K. Global Prevalence of Periodontal Disease and Lack of Its Surveillance. Sci. World J. 2020, 2020, 2146160. [Google Scholar] [CrossRef]
- Genco, R.J.; Graziani, F.; Hasturk, H. Effects of periodontal disease on glycemic control, complications, and incidence of diabetes mellitus. Periodontol. 2000 2020, 83, 59–65. [Google Scholar] [CrossRef]
- Jepsen, S.; Suvan, J.; Deschner, J. The association of periodontal diseases with metabolic syndrome and obesity. Periodontol. 2000 2020, 83, 125–153. [Google Scholar] [CrossRef]
- Siddiqi, A.; Zafar, S.; Sharma, A.; Quaranta, A. Awareness of Diabetic Patients Regarding the Bidirectional Association between Periodontal Disease and Diabetes Mellitus: A Public Oral Health Concern. J. Contemp. Dent. Pract. 2020, 21, 1270–1274. [Google Scholar] [PubMed]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J. Clin. Periodontol. 2018, 45, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R.G.; Shlossman, M.; Budding, L.M.; Pettitt, D.J.; Saad, M.F.; Genco, R.J.; Knowler, W.C. Periodontal disease and NIDDM in Pima Indians. Diabetes Care 1990, 13, 36–40. [Google Scholar] [CrossRef]
- Altamash, M.; Klinge, B.; Engström, P.E. Periodontal treatment and HbA1c levels in subjects with diabetes mellitus. J. Oral Rehabil. 2016, 43, 31–38. [Google Scholar] [CrossRef]
- Liccardo, D.; Cannavo, A.; Spagnuolo, G.; Ferrara, N.; Cittadini, A.; Rengo, C.; Rengo, G. Periodontal disease: A risk factor for diabetes and cardiovascular disease. Int. J. Mol. Sci. 2019, 20, 1414. [Google Scholar] [CrossRef] [PubMed]
- Maftei, G.-A.; Martu, M.-A.; Martu, M.-C.; Popescu, D.; Surlin, P.; Tatarciuc, D.; Popa, C.; Foia, L.-G. Correlations between Salivary Immuno-Biochemical Markers and HbA1c in Type 2 Diabetes Subjects before and after Dental Extraction. Antioxidants 2021, 10, 1741. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A.; Ferrannini, E.; Zimmet, P.; Alberti, G. International Textbook of Diabetes Mellitus, 4th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2015. [Google Scholar]
- Tan, M.H. (Ed.) Diabetes Mellitus: Impact on Bone, Dental and Musculoskeletal Health; Academic Press: Cambridge, MA, USA, 2020. [Google Scholar]
- Penlioglou, T.; Stoian, A.P.; Papanas, N. Diabetes, Vascular Aging and Stroke: Old Dogs, New Tricks? J. Clin. Med. 2021, 10, 4620. [Google Scholar] [CrossRef]
- Cole, J.B.; Florez, J.C. Genetics of diabetes mellitus and diabetes complications. Nat. Rev. Nephrol. 2020, 16, 377–390. [Google Scholar] [CrossRef]
- Yi Shi, P.M.V. Macro- and Microvascular Endothelial Dysfunction in Diabetes. J. Diabetes 2017, 9, 434–449. [Google Scholar] [CrossRef]
- Schmidt, A.M. Highlighting Diabetes Mellitus. The Epidemic Continues. Arterioscler. Thromb. Vasc. Biol. 2018, 38, e1–e8. [Google Scholar] [CrossRef]
- Petersmann, A.; Müller-Wieland, D.; Müller, U.A.; Landgraf, R.; Nauck, M.; Freckmann, G.; Heinemann, L.S.E. Definition, Classification and Diagnosis of Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 2019, 127, s1–s7. [Google Scholar] [CrossRef]
- Harreiter, J.; Roden, M. Diabetes mellitus—Definition, classification, diagnosis, screening and prevention. Wien. Klin. Wochenschr. 2019, 131, 6–15. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37, S81–S90. [Google Scholar] [CrossRef] [Green Version]
- DiMeglio, L.A.; Evans-Molina, C.; Oram, R.A. Type 1 diabetes. Lancet 2018, 391, 2449–2462. [Google Scholar] [CrossRef]
- Engin, A.B. The Definition and Prevalence of Obesity and Metabolic Syndrome. Adv. Exp. Med. Biol. 2017, 960, 1–17. [Google Scholar] [PubMed]
- Fernandez, C.J.; George, A.S.; Subrahmanyan, N.A.; Pappachan, J.M. Epidemiological link between obesity, type 2 diabetes mellitus and cancer. World J. Methodol. 2021, 11, 23. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.N.; Tien, K.J. The Impact of Antidiabetic Agents on Sarcopenia in Type 2 Diabetes: A Literature Review. J. Diabetes Res. 2020, 2020, 9368583. [Google Scholar] [CrossRef]
- Kosiborod, M.; Gomes, M.B.; Nicolucci, A.; Pocock, S.; Rathmann, W.; Shestakova, M.V.; Watada, H.; Shimomura, I.; Chen, H.; Cid-Ruzafa, J.; et al. Vascular complications in patients with type 2 diabetes: Prevalence and associated factors in 38 countries. Cardiovasc. Diabetol. 2018, 17, 150–163. [Google Scholar] [CrossRef]
- Martu, M.A.; Maftei, G.A.; Luchian, I.; Popa, C.; Filioreanu, A.M.; Tatarciuc, D.; Nichitean, G.; Hurjui, L.L.; Foia, L.G. Wound healing of periodontal and oral tissues: Part II—Patho-phisiological conditions and metabolic diseases. Rom. J. Oral Rehab. 2020, 12, 30–40. [Google Scholar]
- Avogaro, A.; Fadini, G.P. Microvascular complications in diabetes: A growing concern for cardiologists. Int. J. Cardiol. 2019, 291, 29–35. [Google Scholar] [CrossRef]
- Lefever, E.; Vliebergh, J.; Chantal, M. Improving the treatment of patients with diabetes using insulin analogues: Current findings and future directions. Expert Opin. Drug Saf. 2020, 9, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.T.M.; Akhter, R.; Garde, S.; Scott, C.; Twigg, S.M.; Colagiuri, S.; Ajwani, S.; Eberhard, J. The association of periodontal disease with the complications of diabetes mellitus. A systematic review. Diabetes Res. Clin. Pract. 2020, 165, 108244. [Google Scholar] [CrossRef]
- Graves, D.T.; Ding, Z.; Yang, Y. The impact of diabetes on periodontal diseases. Periodontol. 2000 2020, 82, 214–224. [Google Scholar] [CrossRef]
- Verhulst, M.J.L.; Loos, B.G.; Gerdes, V.E.A.; Teeuw, W.J. Evaluating All Potential Oral Complications of Diabetes Mellitus. Front. Endocrinol. 2019, 10, 56. [Google Scholar] [CrossRef]
- Luc, K.; Schramm-Luc, A.; Guzik, T.J.; Mikolajczyk, T.P. Oxidative stress and inflammatory markers in prediabetes and diabetes. J. Physiololy Pharmacol. 2019, 70, 809–824. [Google Scholar]
- Rehman, K.; Akash, M.S.H. Mechanism of Generation of Oxidative Stress and Pathophysiology of Type 2 Diabetes Mellitus: How Are They Interlinked? J. Cell. Biochem. 2017, 118, 3577–3585. [Google Scholar] [CrossRef] [PubMed]
- Balci Yuce, H.; Karatas, Ö.; Tulu, F.; Altan, A.; Gevrek, F. Effect of diabetes on collagen metabolism and hypoxia in human gingival tissue: A stereological, histopathological, and immunohistochemical study. Biotech. Histochem. 2019, 94, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Poittevin, M.; Bonnin, P.; Pimpie, C.; Rivière, L.; Sebrié, C.; Dohan, A.; Pocard, M.; Charriaut-Marlangue, C.; Kubis, N. Diabetic microangiopathy: Impact of impaired cerebral vasoreactivity and delayed angiogenesis after permanent middle cerebral artery occlusion on stroke damage and cerebral repair in mice. Diabetes 2015, 64, 999–1010. [Google Scholar] [CrossRef]
- Faselis, C.; Katsimardou, A.; Imprialos, K.; Deligkaris, P.; Kallistratos, M.; Dimitriadis, K. Microvascular Complications of Type 2 Diabetes Mellitus. Curr. Vasc. Pharmacol. 2019, 18, 117–124. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, H.N.; Zhen, Z.; Yiu, K.H.; Tse, H.F.; Pelekos, G.; Tonetti, M.; Jin, L. Periodontal treatment modulates gene expression of endothelial progenitor cells in diabetic patients. J. Clin. Periodontol. 2017, 44, 1253–1263. [Google Scholar] [CrossRef]
- Nitta, H.; Katagiri, S.; Nagasawa, T.; Izumi, Y.; Ishikawa, I.; Izumiyama, H.; Uchimura, I.; Kanazawa, M.; Chiba, H.; Matsuo, A.; et al. The number of microvascular complications is associated with an increased risk for severity of periodontitis in type 2 diabetes patients: Results of a multicenter hospital-based cross-sectional study. J. Diabetes Investig. 2017, 8, 677–686. [Google Scholar] [CrossRef] [PubMed]
- De Miguel-Infante, A.; Martinez-Huedo, M.A.; Mora-Zamorano, E.; Hernández-Barrera, V.; Jiménez-Trujillo, I.; de Burgos-Lunar, C.; Cardenas Valladolid, J.; Jiménez-García, R.; Lopez-de-Andrés, A. Periodontal disease in adults with diabetes, prevalence and risk factors. Results of an observational study. Int. J. Clin. Pract. 2018, 73, e13294. [Google Scholar] [CrossRef]
- Tanaka, A.; Takeuchi, K.; Furuta, M.; Takeshita, T.; Suma, S.; Shinagawa, T.; Shimazaki, Y.; Yamashita, Y. Relationship of toothbrushing to metabolic syndrome in middle-aged adults. J. Clin. Periodontol. 2018, 45, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Resnik, R.; Misch, C.E. Misch’s Avoiding Complications. In Oral Implantology; Elsevier: Maryland Heights, MO, USA, 2018; pp. 771–826. [Google Scholar]
- CDC. Oral Health—Periodontal Disease. Available online: https://www.cdc.gov/oralhealth/conditions/periodontal-disease.html (accessed on 7 February 2023).
- Kikuchi, T.; Hayashi, J.-i.; Mitani, A. Next-Generation Examination, Diagnosis, and Personalized Medicine in Periodontal Disease. J. Pers. Med. 2022, 12, 1743. [Google Scholar] [CrossRef] [PubMed]
- Tegelberg, P.; Tervonen, T.; Knuuttila, M.; Jokelainen, J.; Keinänen-Kiukaanniemi, S.; Auvinen, J.; Ylöstalo, P. Long-term metabolic syndrome is associated with periodontal pockets and alveolar bone loss. J. Clin. Periodontol. 2019, 46, 799–808. [Google Scholar] [CrossRef]
- Sonnenschein, S.K.; Meyle, J. Local inflammatory reactions in patients with diabetes and periodontitis. Periodontol. 2000 2015, 69, 221–254. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions–Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89, S1–S8. [Google Scholar] [CrossRef]
- Glurich, I.; Acharya, A. Updates from the evidence base examining association between periodontal disease and type 2 diabetes mellitus: Current status and clinical relevance. Curr. Diabetes Rep. 2019, 19, 121. [Google Scholar] [CrossRef]
- Hsu, Y.T.; Nair, M.; Angelov, N.; Lalla, E.; Lee, C.T. Impact of diabetes on clinical periodontal outcomes following non-surgical periodontal therapy. J. Clin. Periodontol. 2019, 46, 206–217. [Google Scholar] [CrossRef]
- Sabharwal, A.; Gomes-Filho, I.S.; Stellrecht, E.; Scannapieco, F.A. Role of periodontal therapy in management of common complex systemic diseases and conditions: An update. Periodontol. 2000 2018, 78, 212–226. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Taylor, J.J.; Jaedicke, K.M.; De Jager, M.; Bikker, J.W.; Selten, W.; Bissett, S.M.; Whall, K.M.; van de Merwe, R.; Areibi, A.; et al. Treatment of periodontitis reduces systemic inflammation in type 2 diabetes. J. Clin. Periodontol. 2020, 47, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Sudhakara, P.; Gupta, A.; Bhardwaj, A.; Wilson, A. Oral dysbiotic communities and their implications in systemic diseases. Dent. J. 2018, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Mocanu, R.C.; Martu, M.-A.; Luchian, I.; Sufaru, I.G.; Maftei, G.A.; Ioanid, N.; Martu, S.; Tatarciuc, M. Microbiologic Profiles of Patients with Dental Prosthetic Treatment and Periodontitis before and after Photoactivation Therapy—Randomized Clinical Trial. Microorganisms 2021, 9, 713. [Google Scholar] [CrossRef]
- Sufaru, I.-G.; Martu, M.-A.; Solomon, S.M. Advances in Periodontal Pathogens. Microorganisms 2022, 10, 1439. [Google Scholar] [CrossRef] [PubMed]
- Longo, P.L.; Dabdoub, S.; Kumar, P.; Artese, H.P.C.; Dib, S.A.; Romito, G.A.; Mayer, M.P.A. Glycaemic status affects the subgingival microbiome of diabetic patients. J. Clin. Periodontol. 2018, 45, 932–940. [Google Scholar] [CrossRef] [PubMed]
- Graves, D.T.; Corrêa, J.D.; Silva, T.A. The Oral Microbiota Is Modified by Systemic Diseases. J. Dent. Res. 2019, 98, 148–156. [Google Scholar] [CrossRef]
- Popa, C.; Filioreanu, A.M.; Stelea, C.; Maftei, G.A.; Popescu, E. Prevalence of oral lesions modulated by patient’s age: The young versus the elderly. Rom. J. Oral Rehabil. 2018, 10, 50–56. [Google Scholar]
- Kilian, M. The oral microbiome—friend or foe? Eur. J. Oral Sci. 2018, 126, 5–12. [Google Scholar] [CrossRef]
- Ogawa, T.; Honda-Ogawa, M.; Ikebe, K.; Notomi, Y.; Iwamoto, Y.; Shirobayashi, I.; Hata, S.; Kibi, M.; Masayasu, S.; Sasaki, S.; et al. Characterizations of oral microbiota in elderly nursing home residents with diabetes. J. Oral Sci. 2017, 59, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Matsha, T.E.; Prince, Y.; Davids, S.; Chikte, U.; Erasmus, R.T.; Kengne, A.P.; Davison, G. Oral Microbiome Signatures in Diabetes Mellitus and Periodontal Disease. J. Dent. Res. 2020, 99, 658–665. [Google Scholar] [CrossRef]
- Radhakrishnan, P.; Anbalagan, R.; Barani, R.; Mani, M.; Seshadri, K.G.; Srikanth, P. Sequencing of Porphyromonas gingivalis from saliva in patients with periodontitis and type 2 diabetes mellitus. Indian J. Med. Microbiol. 2019, 37, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, N.; Suzuki, J.I.; Kobayashi, N.; Hanatani, T.; Ashigaki, N.; Yoshida, A.; Shiheido, Y.; Sato, H.; Izumi, Y.; Isobe, M. Increased oral porphyromonas gingivalis prevalence in cardiovascular patients with uncontrolled diabetes mellitus. Int. Heart J. 2018, 59, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Bao, J.; Chang, Y.; Wang, M.; Chen, B.; Yan, F. Gut microbiota may mediate the influence of periodontitis on prediabetes. J. Dent. Res. 2021, 100, 1387–1396. [Google Scholar] [CrossRef]
- Castrillon, C.A.; Hincapie, J.P.; Yepes, F.L.; Roldan, N.; Moreno, S.M.; Contreras, A.; Botero, J.E. Occurrence of red complex microorganisms and A ggregatibacter actinomycetemcomitans in patients with diabetes. J. Investig. Clin. Dent. 2015, 6, 25–31. [Google Scholar] [CrossRef]
- Liu, L.S.; Gkranias, N.; Farias, B.; Spratt, D.; Donos, N. Differences in the subgingival microbial population of chronic periodontitis in subjects with and without type 2 diabetes mellitus—A systematic review. Clin. Oral Investig. 2018, 22, 2743–2762. [Google Scholar] [CrossRef]
- Ganiger, K.; Sridharan, S.; Rahul, A.; Satyanarayana, A. Quantitative analysis of key periodontopathic bacteria in gestational diabetic and non-diabetic women. J. Diabetes Metab. Disord. 2019, 18, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Sabharwal, A.; Ganley, K.; Miecznikowski, J.C.; Haase, E.M.; Barnes, V.; Scannapieco, F.A. The salivary microbiome of diabetic and non-diabetic adults with periodontal disease. J. Periodontol. 2019, 90, 26–34. [Google Scholar] [CrossRef] [PubMed]
- de Araújo Silva, D.N.; Casarin, M.; Monajemzadeh, S.; de Brito Bezerra, B.; Lux, R.; Pirih, F.Q. The microbiome in periodontitis and diabetes. Front. Oral Health 2022, 3. [Google Scholar] [CrossRef]
- Lu, X.; Liu, T.; Zhou, J.; Liu, J.; Yuan, Z.; Guo, L. Subgingival microbiome in periodontitis and type 2 diabetes mellitus: An exploratory study using metagenomic sequencing. J. Periodontal Implant. Sci. 2021, 52, 282–297. [Google Scholar] [CrossRef]
- Shi, B.; Lux, R.; Klokkevold, P.; Chang, M.; Barnard, E.; Haake, S.; Li, H. The subgingival microbiome associated with periodontitis in type 2 diabetes mellitus. ISME J. 2020, 14, 519–530. [Google Scholar] [CrossRef]
- Balmasova, I.P.; Olekhnovich, E.I.; Klimina, K.M.; Korenkova, A.A.; Vakhitova, M.T.; Babaev, E.A.; Ovchinnikova, L.A.; Lomakin, Y.A.; Smirnov, I.V.; Tsarev, V.N.; et al. Drift of the Subgingival Periodontal Microbiome during Chronic Periodontitis in Type 2 Diabetes Mellitus Patients. Pathogens 2021, 10, 504. [Google Scholar] [CrossRef]
- Teles, F.; Wang, Y.; Hajishengallis, G.; Hasturk, H.; Marchesan, J.T. Impact of systemic factors in shaping the periodontal microbiome. Periodontol. 2000 2021, 85, 126–160. [Google Scholar] [CrossRef] [PubMed]
- Xiao, E.; Mattos, M.; Vieira, G.H.A.; Chen, S.; Corrêa, J.D.; Wu, Y.; Albiero, M.L.; Bittinger, K.; Graves, D.T. Diabetes enhances IL-17 expression and alters the oral microbiome to increase its pathogenicity. Cell Host Microbe 2017, 22, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the Global Burden of Periodontal Diseases on Health, Nutrition and Wellbeing of Mankind: A Call for Global Action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef]
- Vergnes, J.N.; Canceill, T.; Vinel, A.; Laurencin-Dalicieux, S.; Maupas-Schwalm, F.; Blasco-Baqué, V.; Hanaire, H.; Arrivé, E.; Rigalleau, V.; Nabet, C.; et al. The effects of periodontal treatment on diabetic patients: The DIAPERIO randomized controlled trial. J. Clin. Periodontol. 2018, 45, 1150–1163. [Google Scholar] [CrossRef]
- Gupta, S.; Maharjan, A.; Dhami, B.; Amgain, P.; Katwal, S.; Adhikari, B.; Shukla, A. Status of tobacco smoking and diabetes with periodontal disease. J. Nepal Med. Assoc. 2018, 56, 818–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, H. Tobacco use and periodontal disease—the role of microvascular dysfunction. Biology 2021, 10, 441. [Google Scholar] [CrossRef] [PubMed]
- Miranda, T.S.; Almeida, M.L.; Marins, L.M.; da Silva, H.D.P.; Feres, M.; Duarte, P.M. Might smoking assuage the pro-inflammatory effect of diabetes in periodontal sites? Oral Dis. 2020, 26, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, S.M.; Joshi, V.; Fellows, M.; Dabdoub, S.M.; Nagaraja, H.N.; O’Donnell, B.; Deshpande, N.R.; Kumar, P.S. A tale of two risks: Smoking, diabetes and the subgingival microbiome. ISME J. 2017, 11, 2075–2089. [Google Scholar] [CrossRef]
- Cheng, R.; Wu, Z.; Li, M.; Shao, M.; Hu, T. Interleukin-1β is a potential therapeutic target for periodontitis: A narrative review. Intern. J. Oral Sci. 2020, 12, 2. [Google Scholar] [CrossRef]
- Schett, G.; Dayer, J.M.; Manger, B. Interleukin-1 function and role in rheumatic disease. Nat. Rev. Rheumatol. 2016, 12, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou, E.; Conti, P.; Carinci, F.; Lauritano, D.; Theoharides, T.C. IL-1 superfamily members and periodontal diseases. J. Dent. Res. 2020, 99, 1425–1434. [Google Scholar] [CrossRef] [PubMed]
- Stolarczyk, E. Adipose tissue inflammation in obesity: A metabolic or immune response? Curr. Opin. Pharmacol. 2017, 37, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Kocher, T.; König, J.; Borgnakke, W.S.; Pink, C.; Meisel, P. Periodontal complications of hyperglycemia/diabetes mellitus: Epidemiologic complexity and clinical challenge. Periodontol. 2000 2018, 78, 59–97. [Google Scholar] [CrossRef] [PubMed]
- Duarte, P.M.; Bezerra, J.P.; Miranda, T.S.; Feres, M.; Chambrone, L.; Shaddox, L.M. Local levels of inflammatory mediators in uncontrolled type 2 diabetic subjects with chronic periodontitis. J. Clin. Periodontol. 2014, 41, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Herder, C.; Carstensen, M.; Ouwens, D.M. Anti-inflammatory cytokines and risk of type 2 diabetes. Diabetes Obes. Metab. 2013, 15, 39–50. [Google Scholar] [CrossRef]
- Wu, Y.Y.; Xiao, E.; Graves, D.T. Diabetes mellitus related bone metabolism and periodontal disease. Int. J. Oral Sci. 2015, 7, 63–72. [Google Scholar] [CrossRef]
- Taylor, J.J.; Preshaw, P.M.; Lalla, E. A review of the evidence for pathogenic mechanisms that may link periodontitis and diabetes. J. Clin. Periodontol. 2013, 40, s113–s134. [Google Scholar] [CrossRef]
- Salhi, L.; Reners, M. Update on the Bidirectional Link Between Diabetes and Periodontitis. Periodontitis 2022, 1373, 231–240. [Google Scholar]
- Camargo, G.A.; da Silva Rodrigues, J.M.; de Amorim, C.S.; de Farias Wenderoscky, L.; Pascoal, V.D.; Souza, A.C.; Duque, C. Gene expression of inflammatory immune factors and clinical parameters in diabetes and nondiabetes patients with periodontal disease. Res. Soc. Dev. 2022, 11, e17711124185. [Google Scholar] [CrossRef]
- Abdellatif, H.M.; Binshabaib, M.S.; Shawky, H.A.; ALHarthi, S.S. Association between Periodontitis and Genetic Polymorphisms in Interleukins among Patients with Diabetes Mellitus. Dent. J. 2021, 9, 45. [Google Scholar] [CrossRef]
- Tai, J.; Sun, D.; Wang, X.; Kang, Z. Matrix metalloproteinase-8 rs11225395 polymorphism correlates with colorectal cancer risk and survival in a Chinese Han population: A case-control study. Aging 2020, 12, 19618. [Google Scholar] [CrossRef] [PubMed]
- Forgo, B.; Medda, E.; Hernyes, A.; Szalontai, L.; Tarnoki, D.L.; Tarnoki, A.D. Carotid artery atherosclerosis: A review on heritability and genetics. Twin Res. Hum. Genet. 2018, 21, 333–346. [Google Scholar] [CrossRef]
- Singh, H.; Samani, D.; Nambiar, N.; Ghate, M.V.; Gangakhedkar, R.R. Prevalence of MMP-8 gene polymorphisms in HIV-infected individuals and its association with HIV-associated neurocognitive disorder. Gene 2018, 646, 83–90. [Google Scholar] [CrossRef]
- Brodzikowska, A.; Górski, B. Polymorphisms in Genes Involved in Inflammation and Periodontitis: A Narrative Review. Biomolecules 2022, 12, 552. [Google Scholar] [CrossRef] [PubMed]
- Kafa, F.; Abou Sulaiman, A.; Haddad, S. Association of matrix metalloproteinase-8 gene promoter polymorphisms with type II diabetes mellitus in Syrian population. Hum. Gene 2022, 23, 201061. [Google Scholar] [CrossRef]
- Sirniö, P.; Tuomisto, A.; Tervahartiala, T.; Sorsa, T.; Klintrup, K.; Karhu, T.; Herzig, K.H.; Mäkelä, J.; Karttunen, T.J.; Salo, T.; et al. High-serum MMP-8 levels are associated with decreased survival and systemic inflammation in colorectal cancer. Br. J. Cancer 2018, 119, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Cirelli, T.; Nepomuceno, R.; Goveia, J.M.; Orrico, S.R.; Cirelli, J.A.; Theodoro, L.H.; Barros, S.P.; Scarel-Caminaga, R.M. Association of type 2 diabetes mellitus and periodontal disease susceptibility with genome-wide association–identified risk variants in a Southeastern Brazilian population. Clin. Oral Investig. 2021, 25, 3873–3892. [Google Scholar] [CrossRef]
- Nepomuceno, R.; Villela, B.S.; Corbi, S.C.T.; Bastos, A.D.S.; Dos Santos, R.A.; Takahashi, C.S.; Orrico, S.R.P.; Scarel-Caminaga, R.M. Dyslipidemia rather than type 2 diabetes mellitus or chronic periodontitis affects the systemic expression of pro-and anti-inflammatory genes. Mediat. Inflamm. 2017, 2017, 1491405. [Google Scholar] [CrossRef]
- Nicchio, I.G.; Cirelli, T.; Nepomuceno, R.; Hidalgo, M.A.; Rossa, C.; Cirelli, J.A.; Orrico, S.R.P.; Barros, S.P.; Theodoro, L.H.; Scarel-Caminaga, R.M. Polymorphisms in Genes of Lipid Metabolism Are Associated with Type 2 Diabetes Mellitus and Periodontitis, as Comorbidities, and with the Subjects’ Periodontal, Glycemic, and Lipid Profiles. J. Diabetes Res. 2021, 2021, 1049307. [Google Scholar] [CrossRef]
- Kang, J.; Kwon, E.J.; Ha, M.; Lee, H.; Yu, Y.; Kang, J.W.; Kim, Y.; Lee, E.Y.; Joo, J.Y.; Heo, H.J.; et al. Identification of Shared Genes and Pathways in Periodontitis and Type 2 Diabetes by Bioinformatics Analysis. Front. Endocrinol. 2022, 12, 724278. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.; Huo, P.; Li, W.; Li, P.; He, L.; Meng, H. Interactions among moderate/severe periodontitis, ADIPOQ-rs1501299, and LEPR-rs1137100 polymorphisms on the risk of type 2 diabetes in a Chinese population. Arch. Oral Biol. 2019, 103, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.J.; France, J.; Crean, S.; Singhrao, S.K. The Porphyromonas gingivalis/host interactome shows enrichment in GWASdb genes related to Alzheimer’s disease, diabetes and cardiovascular diseases. Front. Aging Neurosci. 2017, 9, 408. [Google Scholar] [CrossRef]
- Shah, P.D.; Schooling, C.M.; Borrell, L.N. Impact of liability to periodontitis on glycemic control and type II diabetes risk: A Mendelian randomization study. Front. Genet. 2021, 12, 767577. [Google Scholar] [CrossRef]
- Wang, Y.B.; Yan, S.Y.; Li, X.H.; Huang, Q.; Luo, L.-S.; Wang, Y.-Y.; Jin, Y.-H.; Zeng, X.-T. Causal association between periodontitis and type 2 diabetes: A bidirectional two-sample mendelian randomization analysis. Front. Genet. 2022, 12, 2765. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Păunică, I.; Giurgiu, M.; Dumitriu, A.S.; Păunică, S.; Pantea Stoian, A.M.; Martu, M.-A.; Serafinceanu, C. The Bidirectional Relationship between Periodontal Disease and Diabetes Mellitus—A Review. Diagnostics 2023, 13, 681. https://doi.org/10.3390/diagnostics13040681
Păunică I, Giurgiu M, Dumitriu AS, Păunică S, Pantea Stoian AM, Martu M-A, Serafinceanu C. The Bidirectional Relationship between Periodontal Disease and Diabetes Mellitus—A Review. Diagnostics. 2023; 13(4):681. https://doi.org/10.3390/diagnostics13040681
Chicago/Turabian StylePăunică, Ioana, Marina Giurgiu, Anca Silvia Dumitriu, Stana Păunică, Anca Mihaela Pantea Stoian, Maria-Alexandra Martu, and Cristian Serafinceanu. 2023. "The Bidirectional Relationship between Periodontal Disease and Diabetes Mellitus—A Review" Diagnostics 13, no. 4: 681. https://doi.org/10.3390/diagnostics13040681
APA StylePăunică, I., Giurgiu, M., Dumitriu, A. S., Păunică, S., Pantea Stoian, A. M., Martu, M. -A., & Serafinceanu, C. (2023). The Bidirectional Relationship between Periodontal Disease and Diabetes Mellitus—A Review. Diagnostics, 13(4), 681. https://doi.org/10.3390/diagnostics13040681